Original Articles - Basic Research Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2012;24(2):130-136
DOI 10.1590/S0103-507X2012000200006
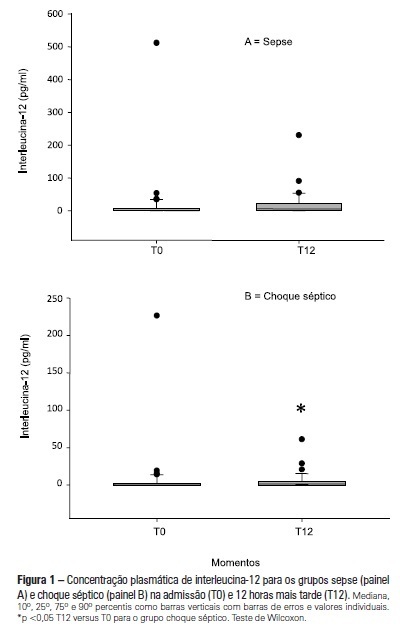
OBJECTIVE: To examine the behavior of interleukin-12 and verify whether it can be used to differentiate septic conditions in children. METHODS: Septic children aged between 28 days and 14 years, prospectively enrolled from 01/2004 to 12/2005, were divided into sepsis (SG; n=47) and septic shock (SSG; n=43) groups. Interleukin-12 levels were measured at admission (T0) and 12 hours later (T12). Disease severity was assessed by the PRISM score. RESULTS: Interleukin-12 levels did not differentiate children with sepsis from those with septic shock at admission [SSG: 0.24 (0-226.4)=SG: 1.23 (0-511.6); p=0.135)] and T12 [SG: 6.11 (0-230.5)=SSG: 1.32 (0-61.0); p=0.1239)]. Comparing time points, no significant difference was observed in the SG [SG, T0: 1.23 (0-511.6)=T12: 6.11 (0-230.5); p=0.075]. In SSG however, interleukin-12 increased from T0 to T12 (SSG, T0: 0.24 (0-226.4)
Abstract
Rev Bras Ter Intensiva. 2012;24(2):130-136
DOI 10.1590/S0103-507X2012000200006
OBJECTIVE: To examine the behavior of interleukin-12 and verify whether it can be used to differentiate septic conditions in children. METHODS: Septic children aged between 28 days and 14 years, prospectively enrolled from 01/2004 to 12/2005, were divided into sepsis (SG; n=47) and septic shock (SSG; n=43) groups. Interleukin-12 levels were measured at admission (T0) and 12 hours later (T12). Disease severity was assessed by the PRISM score. RESULTS: Interleukin-12 levels did not differentiate children with sepsis from those with septic shock at admission [SSG: 0.24 (0-226.4)=SG: 1.23 (0-511.6); p=0.135)] and T12 [SG: 6.11 (0-230.5)=SSG: 1.32 (0-61.0); p=0.1239)]. Comparing time points, no significant difference was observed in the SG [SG, T0: 1.23 (0-511.6)=T12: 6.11 (0-230.5); p=0.075]. In SSG however, interleukin-12 increased from T0 to T12 (SSG, T0: 0.24 (0-226.4)
Abstract
Rev Bras Ter Intensiva. 2012;24(2):137-142
DOI 10.1590/S0103-507X2012000200007
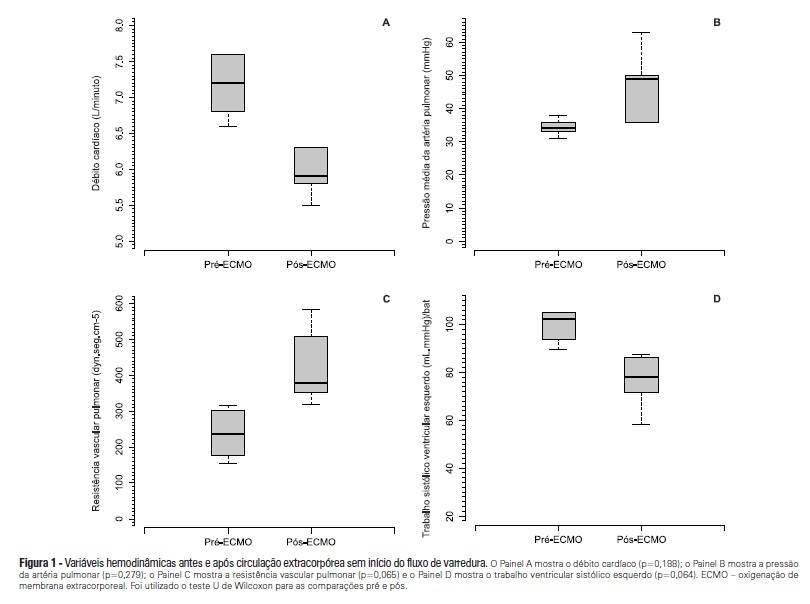
OBJECTIVE: To investigate the hemodynamic, respiratory and metabolic impact of blood contact with a priming volume and extracorporeal membrane oxygenation circuit, before the initiation of oxygenation and ventilation METHODS: Five animals were instrumented and submitted to extracorporeal membrane oxygenation. Data were collected at the baseline and 30 minutes after starting extracorporeal circulation, without membrane ventilatory (sweeper) flow. RESULTS: After starting extracorporeal membrane oxygenation, there was a non-significant elevation in pulmonary vascular resistance from 235 (178,303) to 379 (353,508) dyn.seg.(cm5)-1 (P=0.065), associated with an elevation in the alveolar arterial oxygen gradient from 235 (178,303) to 379 (353,508) mmHg (P=0.063). We also observed a reduction in the left ventricle stroke work from 102 (94,105) to 78 (71,87) (mL.mmHg)/beat (P=0.064), in addition to a reduction in cardiac output from 7.2 (6.8,7.6) to 5.9 (5.8,6.3) L/min (P=0.188). The right ventricle stroke work was counterbalanced between the pulmonary vascular resistance increment and the cardiac output reduction, maintaining a similar value. CONCLUSIONS: We presented an experimental model that is feasible and safe. Blood contact with the priming volume and extracorporeal membrane oxygenation circuit resulted in non-significant systemic or metabolic changes.
Abstract
Rev Bras Ter Intensiva. 2012;24(2):137-142
DOI 10.1590/S0103-507X2012000200007
OBJECTIVE: To investigate the hemodynamic, respiratory and metabolic impact of blood contact with a priming volume and extracorporeal membrane oxygenation circuit, before the initiation of oxygenation and ventilation METHODS: Five animals were instrumented and submitted to extracorporeal membrane oxygenation. Data were collected at the baseline and 30 minutes after starting extracorporeal circulation, without membrane ventilatory (sweeper) flow. RESULTS: After starting extracorporeal membrane oxygenation, there was a non-significant elevation in pulmonary vascular resistance from 235 (178,303) to 379 (353,508) dyn.seg.(cm5)-1 (P=0.065), associated with an elevation in the alveolar arterial oxygen gradient from 235 (178,303) to 379 (353,508) mmHg (P=0.063). We also observed a reduction in the left ventricle stroke work from 102 (94,105) to 78 (71,87) (mL.mmHg)/beat (P=0.064), in addition to a reduction in cardiac output from 7.2 (6.8,7.6) to 5.9 (5.8,6.3) L/min (P=0.188). The right ventricle stroke work was counterbalanced between the pulmonary vascular resistance increment and the cardiac output reduction, maintaining a similar value. CONCLUSIONS: We presented an experimental model that is feasible and safe. Blood contact with the priming volume and extracorporeal membrane oxygenation circuit resulted in non-significant systemic or metabolic changes.
Abstract
Rev Bras Ter Intensiva. 2012;24(1):23-29
DOI 10.1590/S0103-507X2012000100004
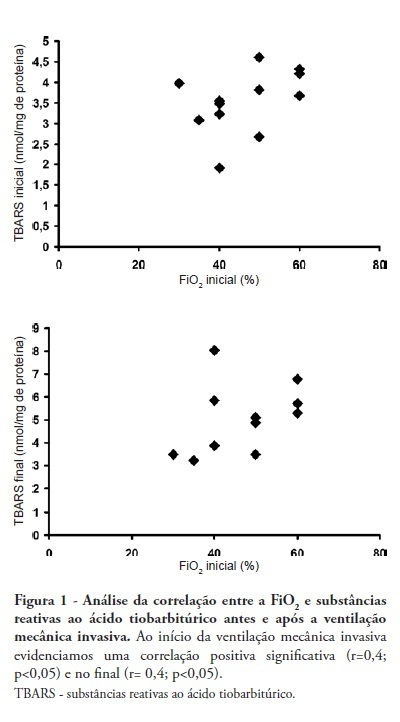
OBJECTIVE: Mechanical ventilation is a mainstay of therapy in intensive care units; however, its deleterious effects need to be assessed. Therefore, we aimed to assess oxidative stress in patients admitted to an intensive care unit undergoing invasive mechanical ventilation. METHODS: This cross-sectional study included 12 invasive mechanical ventilation patients. Blood samples (3 mL) were collected on the first and last days on invasive mechanical ventilation. Thiobarbituric acid-reacting substances (TBARS) were assessed in plasma, and superoxide dismutase (SOD) and catalase (CAT) were assessed in erythrocytes. RESULTS: The mean age was 64.8 ± 17.6 years, the tidal volume (VT) 382 ± 44.5 mL, and the APACHE II score 15 ± 7. When initial and final TBARS were compared, a significant difference was identified (3.54 ± 0.74 vs. 4.96 ± 1.47, p = 0.04). Antioxidant enzymes showed no significant differences. Correlations between PaO2/FiO2 and TBARS (r = 0.4), SOD and PaO2/FiO2 (r = 0.51) and APACHE II and SOD (r = 0.56) were identified. Six patients died. CONCLUSION: Patients undergoing invasive mechanical ventilation can develop redox state changes, showing increased TBARS and reduced antioxidant enzymes.
Abstract
Rev Bras Ter Intensiva. 2012;24(1):23-29
DOI 10.1590/S0103-507X2012000100004
OBJECTIVE: Mechanical ventilation is a mainstay of therapy in intensive care units; however, its deleterious effects need to be assessed. Therefore, we aimed to assess oxidative stress in patients admitted to an intensive care unit undergoing invasive mechanical ventilation. METHODS: This cross-sectional study included 12 invasive mechanical ventilation patients. Blood samples (3 mL) were collected on the first and last days on invasive mechanical ventilation. Thiobarbituric acid-reacting substances (TBARS) were assessed in plasma, and superoxide dismutase (SOD) and catalase (CAT) were assessed in erythrocytes. RESULTS: The mean age was 64.8 ± 17.6 years, the tidal volume (VT) 382 ± 44.5 mL, and the APACHE II score 15 ± 7. When initial and final TBARS were compared, a significant difference was identified (3.54 ± 0.74 vs. 4.96 ± 1.47, p = 0.04). Antioxidant enzymes showed no significant differences. Correlations between PaO2/FiO2 and TBARS (r = 0.4), SOD and PaO2/FiO2 (r = 0.51) and APACHE II and SOD (r = 0.56) were identified. Six patients died. CONCLUSION: Patients undergoing invasive mechanical ventilation can develop redox state changes, showing increased TBARS and reduced antioxidant enzymes.
Abstract
Rev Bras Ter Intensiva. 2012;24(1):30-34
DOI 10.1590/S0103-507X2012000100005
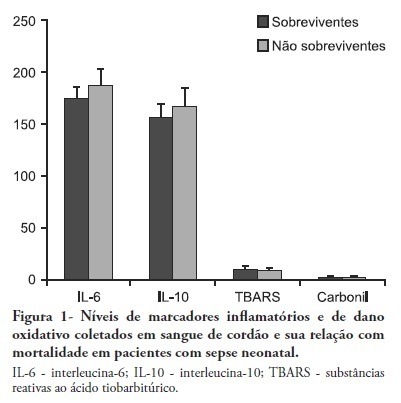
OBJECTIVES: Neonatal sepsis is a complex syndrome involving an uncontrolled systemic inflammatory response associated with an infection. It may result in the dysfunction or failure of one or more organs or even death. Given its high incidence in premature neonates, the identification of prognostic factors to optimize the early diagnosis and therapeutic interventions are highly desirable. This objective study determine the relationship between inflammatory markers and oxidative parameters as prognostic factors in early neonatal sepsis. METHODS: We conducted a prospective observational study by collecting data from 120 patients in the maternity unit of a university hospital. Preterm (<37 weeks of pregnancy) infants with at least one additional risk factor for neonatal sepsis were included. The levels of interleukin (IL)-6, IL-10, thiobarbituric acid reactive species (TBARS) and protein carbonyls and their association with sepsis severity were determined in the cord blood. RESULTS: Levels of IL-6 and TBARS, but not IL-10 and protein carbonyls, demonstrated a mild to moderate correlation with the SNAPPE-II severity score (r=0.435, p=0.02 and r = 0.385, p = 0.017, respectively). No correlations were found between these markers and mortality. CONCLUSION: TBARS and IL-6 have a mild to moderate correlation with SNAPPE-II, but none of the studied markers were able to predict mortality in our sample.
Abstract
Rev Bras Ter Intensiva. 2012;24(1):30-34
DOI 10.1590/S0103-507X2012000100005
OBJECTIVES: Neonatal sepsis is a complex syndrome involving an uncontrolled systemic inflammatory response associated with an infection. It may result in the dysfunction or failure of one or more organs or even death. Given its high incidence in premature neonates, the identification of prognostic factors to optimize the early diagnosis and therapeutic interventions are highly desirable. This objective study determine the relationship between inflammatory markers and oxidative parameters as prognostic factors in early neonatal sepsis. METHODS: We conducted a prospective observational study by collecting data from 120 patients in the maternity unit of a university hospital. Preterm (<37 weeks of pregnancy) infants with at least one additional risk factor for neonatal sepsis were included. The levels of interleukin (IL)-6, IL-10, thiobarbituric acid reactive species (TBARS) and protein carbonyls and their association with sepsis severity were determined in the cord blood. RESULTS: Levels of IL-6 and TBARS, but not IL-10 and protein carbonyls, demonstrated a mild to moderate correlation with the SNAPPE-II severity score (r=0.435, p=0.02 and r = 0.385, p = 0.017, respectively). No correlations were found between these markers and mortality. CONCLUSION: TBARS and IL-6 have a mild to moderate correlation with SNAPPE-II, but none of the studied markers were able to predict mortality in our sample.
Abstract
Rev Bras Ter Intensiva. 2011;23(4):426-433
DOI 10.1590/S0103-507X2011000400006
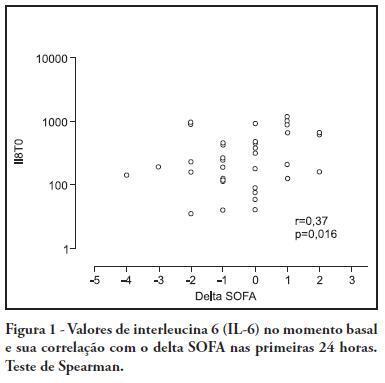
OBJECTIVE: To investigate the correlation of organ dysfunction and its progression with inflammatory response during the early phases of septic shock by assessing baseline cytokine concentrations. METHODS: This study included patients over 18 years old with septic shock within the first 48 hours after the onset of organ dysfunction. Interleukin 6 (IL-6), interleukin 8 (IL-8), interleukin 10 (IL-10) and C-reactive protein levels were assessed at inclusion and after 24 hours, and the differences between these values were calculated. The progression of organ dysfunction was assessed using the Sequential Organ Failure Assessment (SOFA) score upon admission and 24 hours later for a delta-SOFA determination and were categorized as either worsened or improved. The results were expressed as means + standard deviation or median (25-75% percentiles). Values with descriptive p values of 0.05 or less were considered significant. RESULTS: Overall, we included 41 patients with median SOFA scores of 8.0 (6.5-10.0) upon admission (T0) and 8.0 (6.0-10.0) 24 hours later (T1). Worsened, improved or unchanged SOFA scores were observed in 11 (Group 1), 17 (Group 2) and 13 (Group 3) patients, respectively. For Group 1, the baseline IL-6, IL-8 and IL-10 values were higher, and a significant increase of IL-8 levels was found after 24 hours. The change in the SOFA score after 24 hours was significantly, although weakly, correlated with baseline IL-6 and IL-8 concentrations. CONCLUSIONS: Higher baseline IL-6, IL-8 and IL-10 levels are associated with unfavorable organ dysfunction outcomes. Increased IL-8 levels within the first 24 hours are correlated with a worsening dysfunction.
Abstract
Rev Bras Ter Intensiva. 2011;23(4):426-433
DOI 10.1590/S0103-507X2011000400006
OBJECTIVE: To investigate the correlation of organ dysfunction and its progression with inflammatory response during the early phases of septic shock by assessing baseline cytokine concentrations. METHODS: This study included patients over 18 years old with septic shock within the first 48 hours after the onset of organ dysfunction. Interleukin 6 (IL-6), interleukin 8 (IL-8), interleukin 10 (IL-10) and C-reactive protein levels were assessed at inclusion and after 24 hours, and the differences between these values were calculated. The progression of organ dysfunction was assessed using the Sequential Organ Failure Assessment (SOFA) score upon admission and 24 hours later for a delta-SOFA determination and were categorized as either worsened or improved. The results were expressed as means + standard deviation or median (25-75% percentiles). Values with descriptive p values of 0.05 or less were considered significant. RESULTS: Overall, we included 41 patients with median SOFA scores of 8.0 (6.5-10.0) upon admission (T0) and 8.0 (6.0-10.0) 24 hours later (T1). Worsened, improved or unchanged SOFA scores were observed in 11 (Group 1), 17 (Group 2) and 13 (Group 3) patients, respectively. For Group 1, the baseline IL-6, IL-8 and IL-10 values were higher, and a significant increase of IL-8 levels was found after 24 hours. The change in the SOFA score after 24 hours was significantly, although weakly, correlated with baseline IL-6 and IL-8 concentrations. CONCLUSIONS: Higher baseline IL-6, IL-8 and IL-10 levels are associated with unfavorable organ dysfunction outcomes. Increased IL-8 levels within the first 24 hours are correlated with a worsening dysfunction.