Costs and cost analysis Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2016;28(1):62-69
DOI 10.5935/0103-507X.20160014
To evaluate the cost-effectiveness, from the funding body's point of view, of real-time ultrasound-guided central venous catheter insertion compared to the traditional method, which is based on the external anatomical landmark technique.
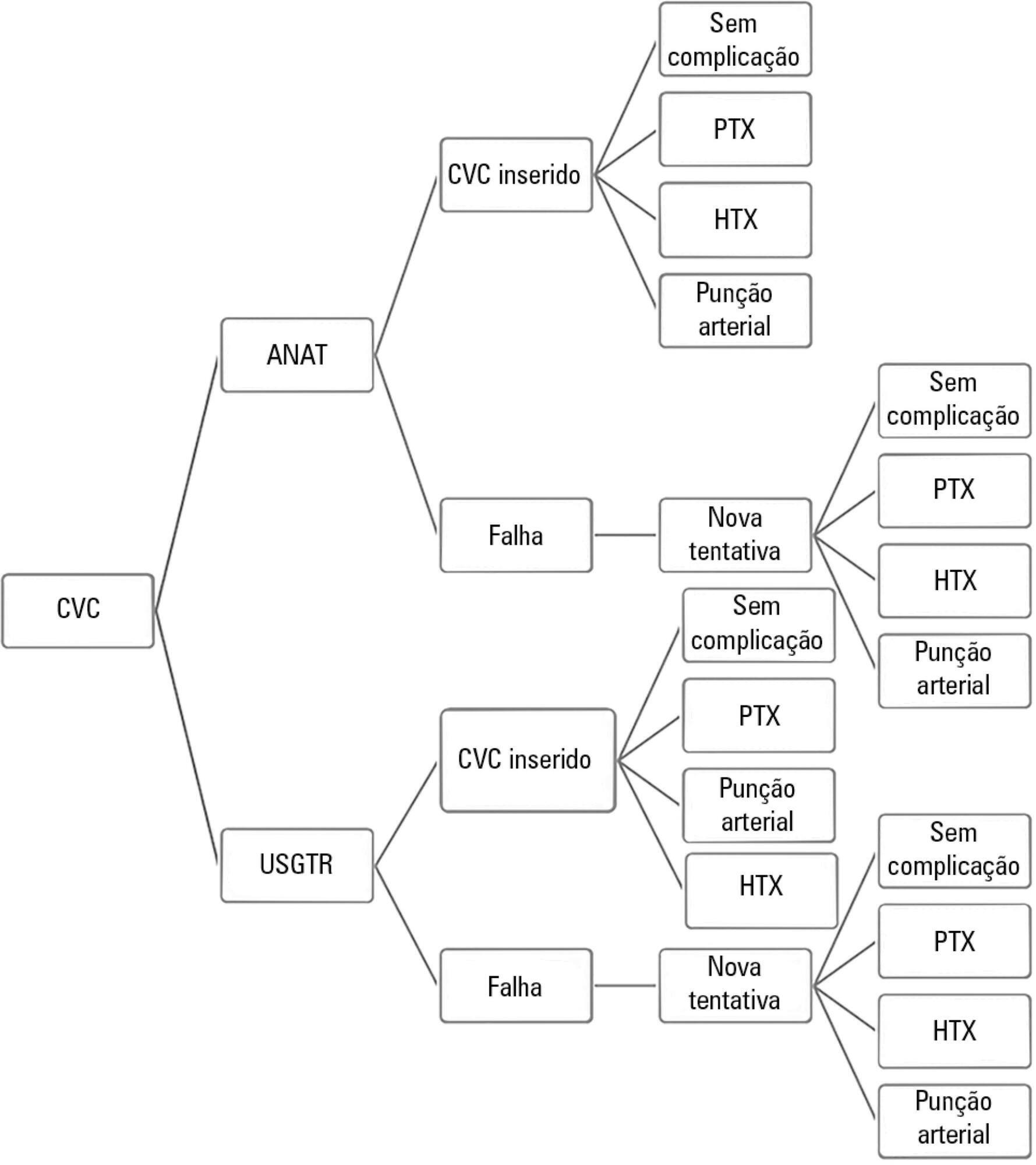
A theoretical simulation based on international literature data was applied to the Brazilian context, i.e., the Unified Health System (Sistema Único de Saúde - SUS). A decision tree was constructed that showed the two central venous catheter insertion techniques: real-time ultrasonography versus external anatomical landmarks. The probabilities of failure and complications were extracted from a search on the PubMed and Embase databases, and values associated with the procedure and with complications were taken from market research and the Department of Information Technology of the Unified Health System (DATASUS). Each central venous catheter insertion alternative had a cost that could be calculated by following each of the possible paths on the decision tree. The incremental cost-effectiveness ratio was calculated by dividing the mean incremental cost of real-time ultrasound compared to the external anatomical landmark technique by the mean incremental benefit, in terms of avoided complications.
When considering the incorporation of real-time ultrasound and the concomitant lower cost due to the reduced number of complications, the decision tree revealed a final mean cost for the external anatomical landmark technique of 262.27 Brazilian reals (R$) and for real-time ultrasound of R$187.94. The final incremental cost of the real-time ultrasound-guided technique was -R$74.33 per central venous catheter. The incremental cost-effectiveness ratio was -R$2,494.34 due to the pneumothorax avoided.
Real-time ultrasound-guided central venous catheter insertion was associated with decreased failure and complication rates and hypothetically reduced costs from the view of the funding body, which in this case was the SUS.
Abstract
Rev Bras Ter Intensiva. 2016;28(1):62-69
DOI 10.5935/0103-507X.20160014
To evaluate the cost-effectiveness, from the funding body's point of view, of real-time ultrasound-guided central venous catheter insertion compared to the traditional method, which is based on the external anatomical landmark technique.
A theoretical simulation based on international literature data was applied to the Brazilian context, i.e., the Unified Health System (Sistema Único de Saúde - SUS). A decision tree was constructed that showed the two central venous catheter insertion techniques: real-time ultrasonography versus external anatomical landmarks. The probabilities of failure and complications were extracted from a search on the PubMed and Embase databases, and values associated with the procedure and with complications were taken from market research and the Department of Information Technology of the Unified Health System (DATASUS). Each central venous catheter insertion alternative had a cost that could be calculated by following each of the possible paths on the decision tree. The incremental cost-effectiveness ratio was calculated by dividing the mean incremental cost of real-time ultrasound compared to the external anatomical landmark technique by the mean incremental benefit, in terms of avoided complications.
When considering the incorporation of real-time ultrasound and the concomitant lower cost due to the reduced number of complications, the decision tree revealed a final mean cost for the external anatomical landmark technique of 262.27 Brazilian reals (R$) and for real-time ultrasound of R$187.94. The final incremental cost of the real-time ultrasound-guided technique was -R$74.33 per central venous catheter. The incremental cost-effectiveness ratio was -R$2,494.34 due to the pneumothorax avoided.
Real-time ultrasound-guided central venous catheter insertion was associated with decreased failure and complication rates and hypothetically reduced costs from the view of the funding body, which in this case was the SUS.
Abstract
Rev Bras Ter Intensiva. 2014;26(3):253-262
DOI 10.5935/0103-507X.20140036
To analyze the cost-utility of using extracorporeal oxygenation for patients with severe acute respiratory distress syndrome in Brazil.
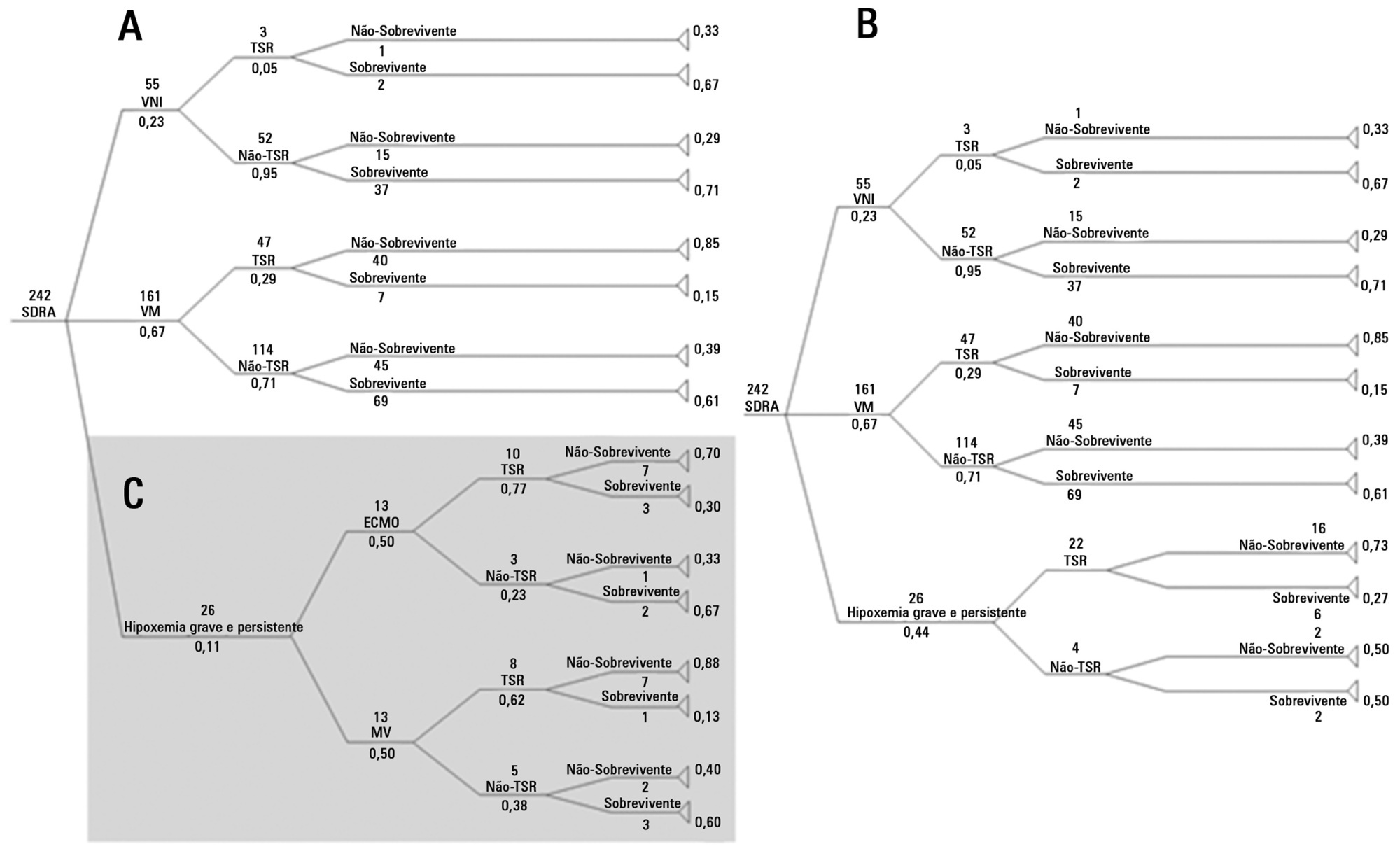
A decision tree was constructed using databases from previously published studies. Costs were taken from the average price paid by the Brazilian Unified Health System (Sistema Único de Saúde; SUS) over three months in 2011. Using the data of 10,000,000 simulated patients with predetermined outcomes and costs, an analysis was performed of the ratio between cost increase and years of life gained, adjusted for quality (cost-utility), with survival rates of 40 and 60% for patients using extracorporeal membrane oxygenation.
The decision tree resulted in 16 outcomes with different life support techniques. With survival rates of 40 and 60%, respectively, the increased costs were R$=-301.00/-14.00, with a cost of R$=-30,913.00/-1,752.00 paid per six-month quality-adjusted life-year gained and R$=-2,386.00/-90.00 per quality-adjusted life-year gained until the end of life, when all patients with severe ARDS were analyzed. Analyzing only patients with severe hypoxemia (i.e., a ratio of partial oxygen pressure in the blood to the fraction of inspired oxygen <100mmHg), the increased cost was R$=-5,714.00/272.00, with a cost per six-month quality-adjusted life-year gained of R$=-9,521.00/293.00 and a cost of R$=-280.00/7.00 per quality-adjusted life-year gained.
The cost-utility ratio associated with the use of extracorporeal membrane oxygenation in Brazil is potentially acceptable according to this hypothetical study.
Abstract
Rev Bras Ter Intensiva. 2014;26(3):253-262
DOI 10.5935/0103-507X.20140036
To analyze the cost-utility of using extracorporeal oxygenation for patients with severe acute respiratory distress syndrome in Brazil.
A decision tree was constructed using databases from previously published studies. Costs were taken from the average price paid by the Brazilian Unified Health System (Sistema Único de Saúde; SUS) over three months in 2011. Using the data of 10,000,000 simulated patients with predetermined outcomes and costs, an analysis was performed of the ratio between cost increase and years of life gained, adjusted for quality (cost-utility), with survival rates of 40 and 60% for patients using extracorporeal membrane oxygenation.
The decision tree resulted in 16 outcomes with different life support techniques. With survival rates of 40 and 60%, respectively, the increased costs were R$=-301.00/-14.00, with a cost of R$=-30,913.00/-1,752.00 paid per six-month quality-adjusted life-year gained and R$=-2,386.00/-90.00 per quality-adjusted life-year gained until the end of life, when all patients with severe ARDS were analyzed. Analyzing only patients with severe hypoxemia (i.e., a ratio of partial oxygen pressure in the blood to the fraction of inspired oxygen <100mmHg), the increased cost was R$=-5,714.00/272.00, with a cost per six-month quality-adjusted life-year gained of R$=-9,521.00/293.00 and a cost of R$=-280.00/7.00 per quality-adjusted life-year gained.
The cost-utility ratio associated with the use of extracorporeal membrane oxygenation in Brazil is potentially acceptable according to this hypothetical study.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (116) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)