Diagnostic techniques and procedures Archives - Critical Care Science (CCS)

Abstract
Crit Care Sci. 2023;35(1):37-43
DOI 10.5935/2965-2774.20230275-pt
To compare the diagnostic performance of maximal expiratory pressure with maximal expiratory pressure during induced cough for predicting extubation failure within 72 hours in patients who completed a spontaneous breathing trial (SBT).
The study was conducted between October 2018 and September 2019. All patients aged over 18 years admitted to the intensive care unit who required invasive mechanical ventilation for over 48 hours and successfully completed a spontaneous breathing trial were included. The maximal expiratory pressure was assessed with a unidirectional valve for 40 seconds, and verbal encouragement was given. The maximal expiratory pressure during induced cough was measured with slow instillation of 2mL of a 0.9% saline solution. The primary outcome variable was extubation failure.
Eighty patients were included, of which 43 (54%) were male. Twenty-two patients [27.5% (95%CI 18.9 - 38.1)] failed extubation within 72 hours. Differences were observed in the maximal expiratory pressure during induced cough between the group who failed extubation, with a median of 0cmH2O (P25-75: 0 - 90), and the group without extubation failure, with a median of 120cmH2O (P25-75: 73 - 120); p < 0.001.
In patients who completed a spontaneous breathing trial, the maximal expiratory pressure during induced cough had a higher diagnostic performance for predicting extubation failure within 72 hours.
Abstract
Crit Care Sci. 2023;35(1):37-43
DOI 10.5935/2965-2774.20230275-pt
To compare the diagnostic performance of maximal expiratory pressure with maximal expiratory pressure during induced cough for predicting extubation failure within 72 hours in patients who completed a spontaneous breathing trial (SBT).
The study was conducted between October 2018 and September 2019. All patients aged over 18 years admitted to the intensive care unit who required invasive mechanical ventilation for over 48 hours and successfully completed a spontaneous breathing trial were included. The maximal expiratory pressure was assessed with a unidirectional valve for 40 seconds, and verbal encouragement was given. The maximal expiratory pressure during induced cough was measured with slow instillation of 2mL of a 0.9% saline solution. The primary outcome variable was extubation failure.
Eighty patients were included, of which 43 (54%) were male. Twenty-two patients [27.5% (95%CI 18.9 - 38.1)] failed extubation within 72 hours. Differences were observed in the maximal expiratory pressure during induced cough between the group who failed extubation, with a median of 0cmH2O (P25-75: 0 - 90), and the group without extubation failure, with a median of 120cmH2O (P25-75: 73 - 120); p < 0.001.
In patients who completed a spontaneous breathing trial, the maximal expiratory pressure during induced cough had a higher diagnostic performance for predicting extubation failure within 72 hours.

Abstract
Rev Bras Ter Intensiva. 2019;31(4):464-473
DOI 10.5935/0103-507X.20190072
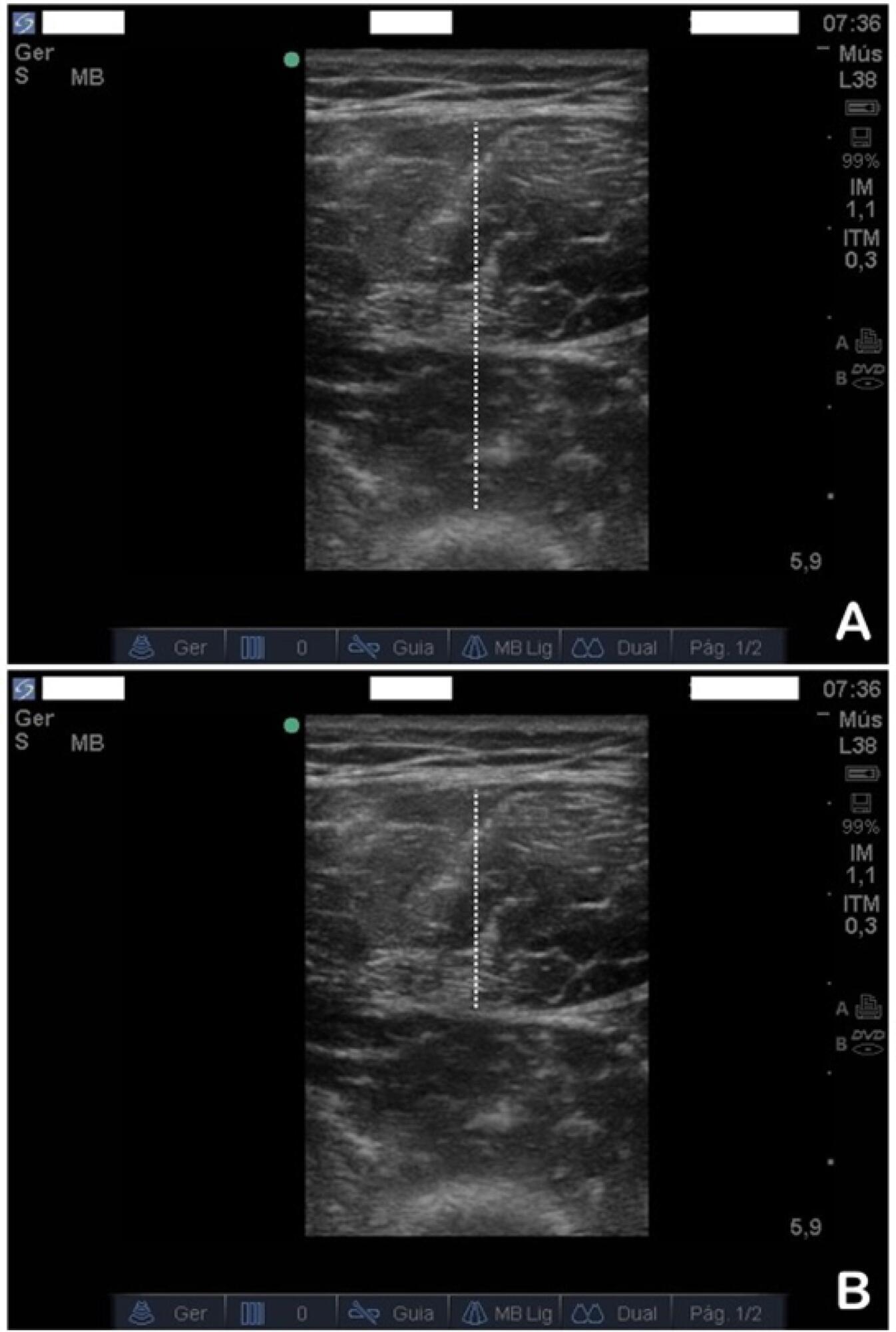
To evaluate the safety and feasibility of the ultrasound assessment of quadriceps in the emergency setting. To assess the intra- and interrater reliability for the acquisition and analysis of ultrasound images of muscle thickness and echogenicity in critically ill trauma patients between health professionals with different levels of expertise.
Diagnostic accuracy study. Two examiners (expert and novice) acquired ultrasound images from ten patients; an experienced, blinded analyst quantified the images. In a separate group of ten patients, two analysts (expert and novice) quantified quadriceps muscle thickness and echogenicity (square or trace method) from images acquired by one examiner.
Excellent reliability was found for image acquisition and analysis (intraclass correlation coefficients > 0.987; p < 0.001). The standard error of the measurement values ranged from 0.01 - 0.06cm for muscle thickness and from 0.75 - 2.04 arbitrary units for muscle echogenicity. The coefficients of variation were < 6% for thickness and echogenicity. The echogenicity values were higher when using the square technique than when using the tracing technique (p = 0.003).
Ultrasound is safe, feasible, and reliable for muscle assessment in critically ill trauma patients, regardless of the assessor's level of expertise.
Abstract
Rev Bras Ter Intensiva. 2019;31(4):464-473
DOI 10.5935/0103-507X.20190072
To evaluate the safety and feasibility of the ultrasound assessment of quadriceps in the emergency setting. To assess the intra- and interrater reliability for the acquisition and analysis of ultrasound images of muscle thickness and echogenicity in critically ill trauma patients between health professionals with different levels of expertise.
Diagnostic accuracy study. Two examiners (expert and novice) acquired ultrasound images from ten patients; an experienced, blinded analyst quantified the images. In a separate group of ten patients, two analysts (expert and novice) quantified quadriceps muscle thickness and echogenicity (square or trace method) from images acquired by one examiner.
Excellent reliability was found for image acquisition and analysis (intraclass correlation coefficients > 0.987; p < 0.001). The standard error of the measurement values ranged from 0.01 - 0.06cm for muscle thickness and from 0.75 - 2.04 arbitrary units for muscle echogenicity. The coefficients of variation were < 6% for thickness and echogenicity. The echogenicity values were higher when using the square technique than when using the tracing technique (p = 0.003).
Ultrasound is safe, feasible, and reliable for muscle assessment in critically ill trauma patients, regardless of the assessor's level of expertise.
Abstract
Rev Bras Ter Intensiva. 2016;28(1):62-69
DOI 10.5935/0103-507X.20160014
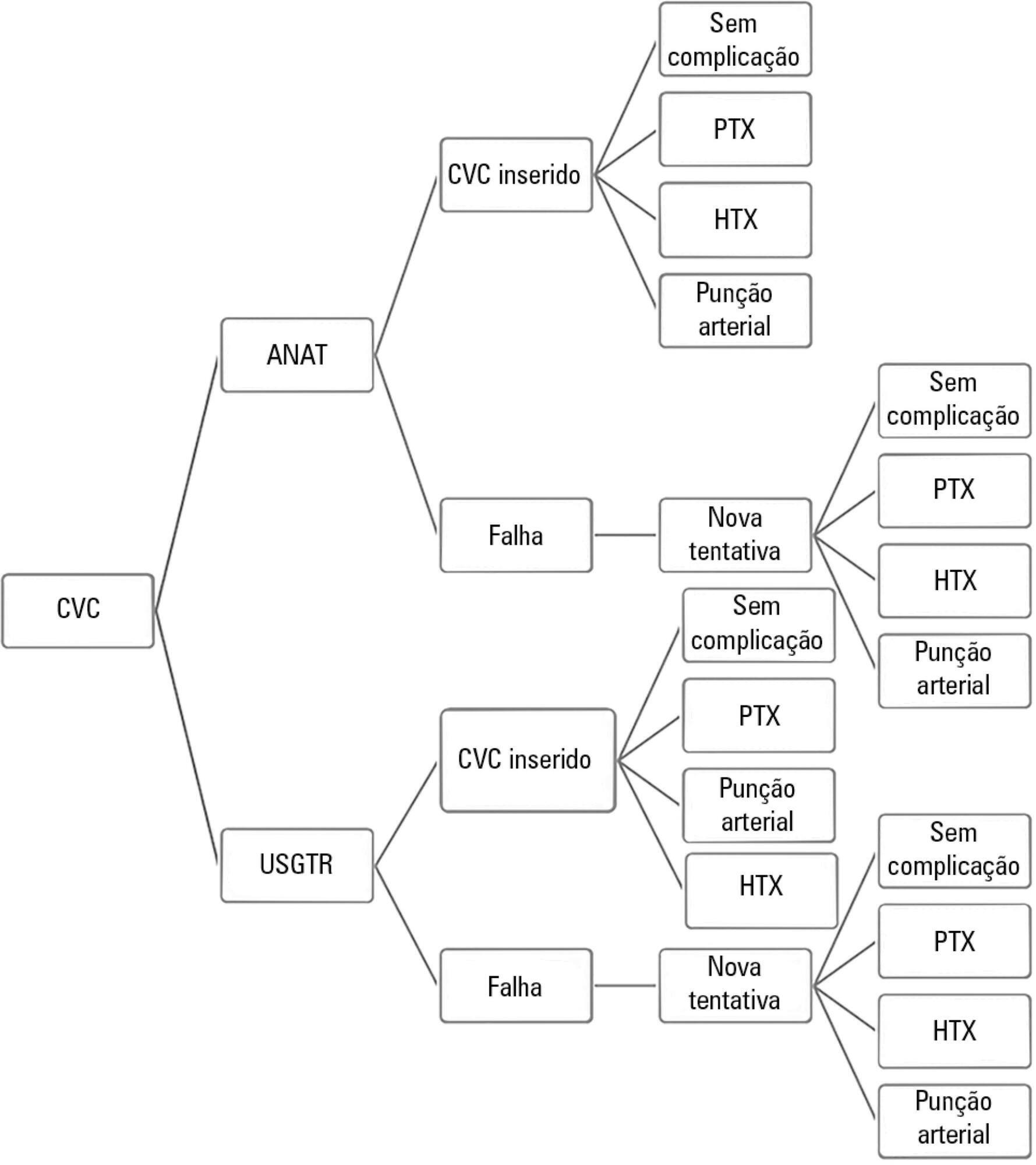
To evaluate the cost-effectiveness, from the funding body's point of view, of real-time ultrasound-guided central venous catheter insertion compared to the traditional method, which is based on the external anatomical landmark technique.
A theoretical simulation based on international literature data was applied to the Brazilian context, i.e., the Unified Health System (Sistema Único de Saúde - SUS). A decision tree was constructed that showed the two central venous catheter insertion techniques: real-time ultrasonography versus external anatomical landmarks. The probabilities of failure and complications were extracted from a search on the PubMed and Embase databases, and values associated with the procedure and with complications were taken from market research and the Department of Information Technology of the Unified Health System (DATASUS). Each central venous catheter insertion alternative had a cost that could be calculated by following each of the possible paths on the decision tree. The incremental cost-effectiveness ratio was calculated by dividing the mean incremental cost of real-time ultrasound compared to the external anatomical landmark technique by the mean incremental benefit, in terms of avoided complications.
When considering the incorporation of real-time ultrasound and the concomitant lower cost due to the reduced number of complications, the decision tree revealed a final mean cost for the external anatomical landmark technique of 262.27 Brazilian reals (R$) and for real-time ultrasound of R$187.94. The final incremental cost of the real-time ultrasound-guided technique was -R$74.33 per central venous catheter. The incremental cost-effectiveness ratio was -R$2,494.34 due to the pneumothorax avoided.
Real-time ultrasound-guided central venous catheter insertion was associated with decreased failure and complication rates and hypothetically reduced costs from the view of the funding body, which in this case was the SUS.
Abstract
Rev Bras Ter Intensiva. 2016;28(1):62-69
DOI 10.5935/0103-507X.20160014
To evaluate the cost-effectiveness, from the funding body's point of view, of real-time ultrasound-guided central venous catheter insertion compared to the traditional method, which is based on the external anatomical landmark technique.
A theoretical simulation based on international literature data was applied to the Brazilian context, i.e., the Unified Health System (Sistema Único de Saúde - SUS). A decision tree was constructed that showed the two central venous catheter insertion techniques: real-time ultrasonography versus external anatomical landmarks. The probabilities of failure and complications were extracted from a search on the PubMed and Embase databases, and values associated with the procedure and with complications were taken from market research and the Department of Information Technology of the Unified Health System (DATASUS). Each central venous catheter insertion alternative had a cost that could be calculated by following each of the possible paths on the decision tree. The incremental cost-effectiveness ratio was calculated by dividing the mean incremental cost of real-time ultrasound compared to the external anatomical landmark technique by the mean incremental benefit, in terms of avoided complications.
When considering the incorporation of real-time ultrasound and the concomitant lower cost due to the reduced number of complications, the decision tree revealed a final mean cost for the external anatomical landmark technique of 262.27 Brazilian reals (R$) and for real-time ultrasound of R$187.94. The final incremental cost of the real-time ultrasound-guided technique was -R$74.33 per central venous catheter. The incremental cost-effectiveness ratio was -R$2,494.34 due to the pneumothorax avoided.
Real-time ultrasound-guided central venous catheter insertion was associated with decreased failure and complication rates and hypothetically reduced costs from the view of the funding body, which in this case was the SUS.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (115) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)