
You searched for:"Luiz Monteiro da Cruz Neto"
We found (4) results for your search.-
Original Article
Resuscitation fluid practices in Brazilian intensive care units: a secondary analysis of Fluid-TRIPS
- Flavio Geraldo Rezende de Freitas
 ,
, - Naomi Hammond,
- Yang Li,
- Luciano Cesar Pontes de Azevedo,
- Alexandre Biasi Cavalcanti , [ … ],
- Flavia Ribeiro Machado
Abstract
Original ArticleResuscitation fluid practices in Brazilian intensive care units: a secondary analysis of Fluid-TRIPS
Rev Bras Ter Intensiva. 2021;33(2):206-218
DOI 10.5935/0103-507X.20210028
- Flavio Geraldo Rezende de Freitas ,
- Naomi Hammond,
- Yang Li,
- Luciano Cesar Pontes de Azevedo,
- Alexandre Biasi Cavalcanti ,
- Leandro Taniguchi ,
- André Gobatto,
- André Miguel Japiassú ,
- Antonio Tonete Bafi,
- Bruno Franco Mazza,
- Danilo Teixeira Noritomi,
- Felipe Dal-Pizzol ,
- Fernando Bozza ,
- Jorge Ibrahin Figueira Salluh ,
- Glauco Adrieno Westphal ,
- Márcio Soares ,
- Murillo Santucci César de Assunção ,
- Thiago Lisboa,
- Suzana Margarete Ajeje Lobo,
- Achilles Rohlfs Barbosa,
- Adriana Fonseca Ventura,
- Ailson Faria de Souza,
- Alexandre Francisco Silva,
- Alexandre Toledo,
- Aline Reis,
- Allan Cembranel,
- Alvaro Rea Neto,
- Ana Lúcia Gut,
- Ana Patricia Pierre Justo,
- Ana Paula Santos,
- André Campos D. de Albuquerque,
- André Scazufka,
- Antonio Babo Rodrigues,
- Bruno Bonaccorsi Fernandino,
- Bruno Goncalves Silva,
- Bruno Sarno Vidal,
- Bruno Valle Pinheiro,
- Bruno Vilela Costa Pinto,
- Carlos Augusto Ramos Feijo,
- Carlos de Abreu Filho,
- Carlos Eduardo da Costa Nunes Bosso,
- Carlos Eduardo Nassif Moreira,
- Carlos Henrique Ferreira Ramos,
- Carmen Tavares,
- Cidamaiá Arantes,
- Cintia Grion,
- Ciro Leite Mendes,
- Claudio Kmohan,
- Claudio Piras,
- Cristine Pilati Pileggi Castro,
- Cyntia Lins,
- Daniel Beraldo,
- Daniel Fontes,
- Daniela Boni,
- Débora Castiglioni,
- Denise de Moraes Paisani,
- Durval Ferreira Fonseca Pedroso,
- Ederson Roberto Mattos,
- Edgar de Brito Sobrinho,
- Edgar M. V. Troncoso,
- Edison Moraes Rodrigues Filho,
- Eduardo Enrico Ferrari Nogueira,
- Eduardo Leme Ferreira,
- Eduardo Souza Pacheco,
- Euzebio Jodar,
- Evandro L. A. Ferreira,
- Fabiana Fernandes de Araujo,
- Fabiana Schuelter Trevisol,
- Fábio Ferreira Amorim,
- Fabio Poianas Giannini,
- Fabrício Primitivo Matos Santos,
- Fátima Buarque,
- Felipe Gallego Lima,
- Fernando Antonio Alvares da Costa,
- Fernando Cesar dos Anjos Sad,
- Fernando G. Aranha,
- Fernando Ganem,
- Flavio Callil,
- Francisco Flávio Costa Filho,
- Frederico Toledo Campo Dall´Arto,
- Geovani Moreno,
- Gilberto Friedman,
- Giulliana Martines Moralez,
- Guilherme Abdalla da Silva,
- Guilherme Costa,
- Guilherme Silva Cavalcanti,
- Guilherme Silva Cavalcanti,
- Gustavo Navarro Betônico,
- Gustavo Navarro Betônico,
- Hélder Reis,
- Helia Beatriz N. Araujo,
- Helio Anjos Hortiz Júnior,
- Helio Penna Guimaraes,
- Hugo Urbano,
- Israel Maia,
- Ivan Lopes Santiago Filho,
- Jamil Farhat Júnior,
- Janu Rangel Alvarez,
- Joel Tavares Passos,
- Jorge Eduardo da Rocha Paranhos,
- José Aurelio Marques,
- José Gonçalves Moreira Filho,
- Jose Neto Andrade,
- José Onofre de C Sobrinho,
- Jose Terceiro de Paiva Bezerra,
- Juliana Apolônio Alves,
- Juliana Ferreira,
- Jussara Gomes,
- Karina Midori Sato,
- Karine Gerent,
- Kathia Margarida Costa Teixeira,
- Katia Aparecida Pessoa Conde,
- Laércia Ferreira Martins,
- Lanese Figueirêdo,
- Leila Rezegue,
- Leonardo Tcherniacovsk,
- Leone Oliveira Ferraz,
- Liane Cavalcante,
- Ligia Rabelo,
- Lilian Miilher,
- Lisiane Garcia,
- Luana Tannous,
- Ludhmila Abrahão Hajjar,
- Luís Eduardo Miranda Paciência,
- Luiz Monteiro da Cruz Neto,
- Macia Valeria Bley,
- Marcelo Ferreira Sousa,
- Marcelo Lourencini Puga,
- Marcelo Luz Pereira Romano,
- Marciano Nobrega,
- Marcio Arbex,
- Márcio Leite Rodrigues,
- Márcio Osório Guerreiro,
- Marcone Rocha,
- Maria Angela Pangoni Alves,
- Maria Angela Pangoni Alves,
- Maria Doroti Rosa,
- Mariza D’Agostino Dias,
- Miquéias Martins,
- Mirella de Oliveira,
- Miriane Melo Silveira Moretti,
- Mirna Matsui,
- Octavio Messender,
- Orlando Luís de Andrade Santarém,
- Patricio Júnior Henrique da Silveira,
- Paula Frizera Vassallo,
- Paulo Antoniazzi,
- Paulo César Gottardo,
- Paulo Correia,
- Paulo Ferreira,
- Paulo Torres,
- Pedro Gabrile M. de Barros e Silva,
- Rafael Foernges,
- Rafael Gomes,
- Rafael Moraes,
- Raimundo Nonato filho,
- Renato Luis Borba,
- Renato V Gomes,
- Ricardo Cordioli,
- Ricardo Lima,
- Ricardo Pérez López,
- Ricardo Rath de Oliveira Gargioni,
- Richard Rosenblat,
- Roberta Machado de Souza,
- Roberto Almeida,
- Roberto Camargo Narciso,
- Roberto Marco,
- Roberto waltrick,
- Rodrigo Biondi,
- Rodrigo Figueiredo,
- Rodrigo Santana Dutra,
- Roseane Batista,
- Rouge Felipe,
- Rubens Sergio da Silva Franco,
- Sandra Houly,
- Sara Socorro Faria,
- Sergio Felix Pinto,
- Sergio Luzzi,
- Sergio Sant’ana,
- Sergio Sonego Fernandes,
- Sérgio Yamada,
- Sérgio Zajac,
- Sidiner Mesquita Vaz,
- Silvia Aparecida Bezerra Bezerra,
- Tatiana Bueno Tardivo Farhat,
- Thiago Martins Santos,
- Tiago Smith,
- Ulysses V. A. Silva,
- Valnei Bento Damasceno,
- Vandack Nobre,
- Vicente Cés de Souza Dantas,
- Vivian Menezes Irineu,
- Viviane Bogado,
- Wagner Nedel,
- Walther Campos Filho,
- Weidson Dantas,
- William Viana,
- Wilson de Oliveira Filho,
- Wilson Martins Delgadinho,
- Simon Finfer,
- Flavia Ribeiro Machado
Views1See moreAbstract
Objective:
To describe fluid resuscitation practices in Brazilian intensive care units and to compare them with those of other countries participating in the Fluid-TRIPS.
Methods:
This was a prospective, international, cross-sectional, observational study in a convenience sample of intensive care units in 27 countries (including Brazil) using the Fluid-TRIPS database compiled in 2014. We described the patterns of fluid resuscitation use in Brazil compared with those in other countries and identified the factors associated with fluid choice.
Results:
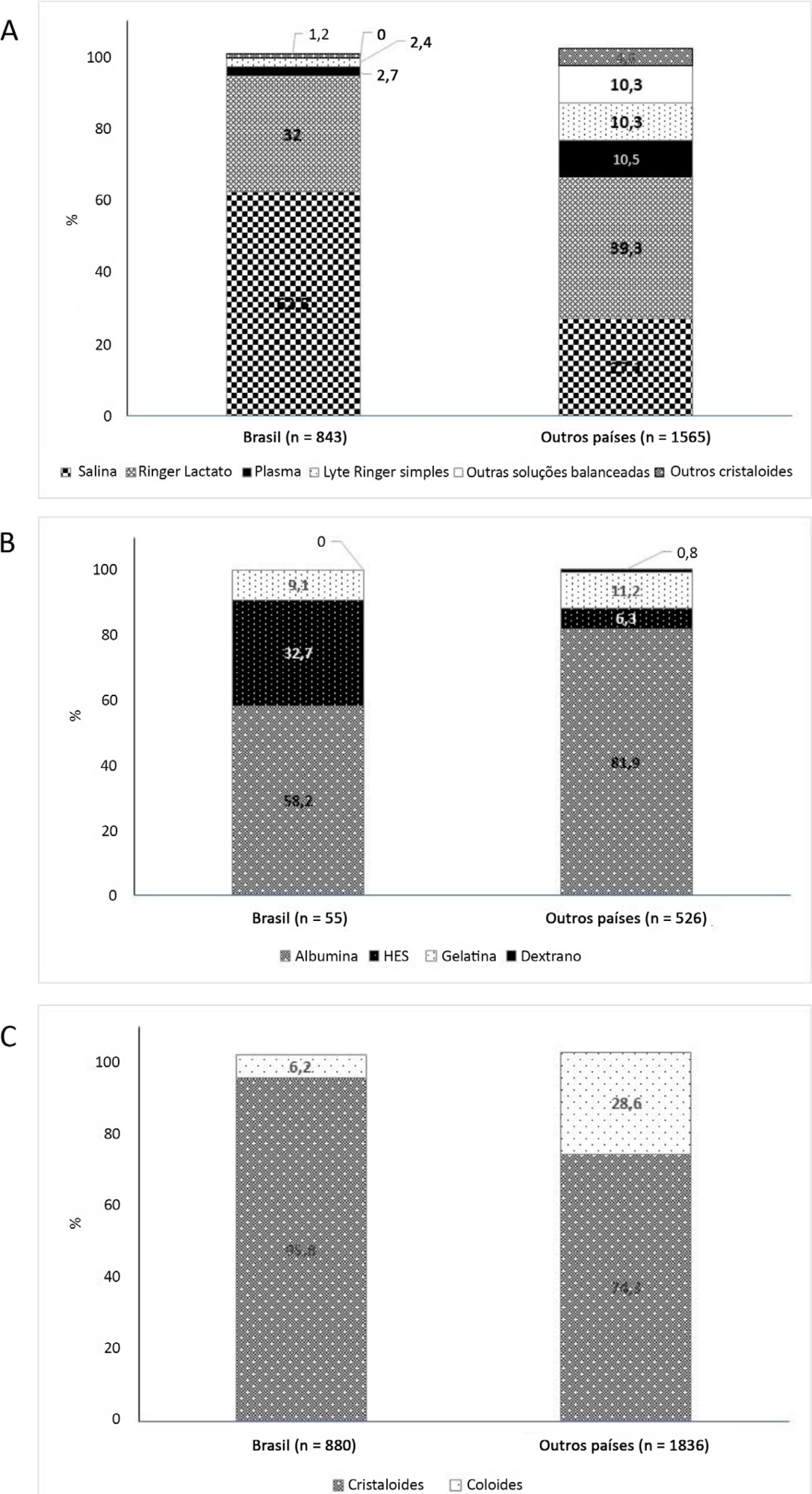
On the study day, 3,214 patients in Brazil and 3,493 patients in other countries were included, of whom 16.1% and 26.8% (p < 0.001) received fluids, respectively. The main indication for fluid resuscitation was impaired perfusion and/or low cardiac output (Brazil: 71.7% versus other countries: 56.4%, p < 0.001). In Brazil, the percentage of patients receiving crystalloid solutions was higher (97.7% versus 76.8%, p < 0.001), and 0.9% sodium chloride was the most commonly used crystalloid (62.5% versus 27.1%, p < 0.001). The multivariable analysis suggested that the albumin levels were associated with the use of both crystalloids and colloids, whereas the type of fluid prescriber was associated with crystalloid use only.
Conclusion:
Our results suggest that crystalloids are more frequently used than colloids for fluid resuscitation in Brazil, and this discrepancy in frequencies is higher than that in other countries. Sodium chloride (0.9%) was the crystalloid most commonly prescribed. Serum albumin levels and the type of fluid prescriber were the factors associated with the choice of crystalloids or colloids for fluid resuscitation.
Views1

Abstract
Original ArticleResuscitation fluid practices in Brazilian intensive care units: a secondary analysis of Fluid-TRIPS
Rev Bras Ter Intensiva. 2021;33(2):206-218
DOI 10.5935/0103-507X.20210028
- Flavio Geraldo Rezende de Freitas ,
- Naomi Hammond,
- Yang Li,
- Luciano Cesar Pontes de Azevedo,
- Alexandre Biasi Cavalcanti ,
- Leandro Taniguchi ,
- André Gobatto,
- André Miguel Japiassú ,
- Antonio Tonete Bafi,
- Bruno Franco Mazza,
- Danilo Teixeira Noritomi,
- Felipe Dal-Pizzol ,
- Fernando Bozza ,
- Jorge Ibrahin Figueira Salluh ,
- Glauco Adrieno Westphal ,
- Márcio Soares ,
- Murillo Santucci César de Assunção ,
- Thiago Lisboa,
- Suzana Margarete Ajeje Lobo,
- Achilles Rohlfs Barbosa,
- Adriana Fonseca Ventura,
- Ailson Faria de Souza,
- Alexandre Francisco Silva,
- Alexandre Toledo,
- Aline Reis,
- Allan Cembranel,
- Alvaro Rea Neto,
- Ana Lúcia Gut,
- Ana Patricia Pierre Justo,
- Ana Paula Santos,
- André Campos D. de Albuquerque,
- André Scazufka,
- Antonio Babo Rodrigues,
- Bruno Bonaccorsi Fernandino,
- Bruno Goncalves Silva,
- Bruno Sarno Vidal,
- Bruno Valle Pinheiro,
- Bruno Vilela Costa Pinto,
- Carlos Augusto Ramos Feijo,
- Carlos de Abreu Filho,
- Carlos Eduardo da Costa Nunes Bosso,
- Carlos Eduardo Nassif Moreira,
- Carlos Henrique Ferreira Ramos,
- Carmen Tavares,
- Cidamaiá Arantes,
- Cintia Grion,
- Ciro Leite Mendes,
- Claudio Kmohan,
- Claudio Piras,
- Cristine Pilati Pileggi Castro,
- Cyntia Lins,
- Daniel Beraldo,
- Daniel Fontes,
- Daniela Boni,
- Débora Castiglioni,
- Denise de Moraes Paisani,
- Durval Ferreira Fonseca Pedroso,
- Ederson Roberto Mattos,
- Edgar de Brito Sobrinho,
- Edgar M. V. Troncoso,
- Edison Moraes Rodrigues Filho,
- Eduardo Enrico Ferrari Nogueira,
- Eduardo Leme Ferreira,
- Eduardo Souza Pacheco,
- Euzebio Jodar,
- Evandro L. A. Ferreira,
- Fabiana Fernandes de Araujo,
- Fabiana Schuelter Trevisol,
- Fábio Ferreira Amorim,
- Fabio Poianas Giannini,
- Fabrício Primitivo Matos Santos,
- Fátima Buarque,
- Felipe Gallego Lima,
- Fernando Antonio Alvares da Costa,
- Fernando Cesar dos Anjos Sad,
- Fernando G. Aranha,
- Fernando Ganem,
- Flavio Callil,
- Francisco Flávio Costa Filho,
- Frederico Toledo Campo Dall´Arto,
- Geovani Moreno,
- Gilberto Friedman,
- Giulliana Martines Moralez,
- Guilherme Abdalla da Silva,
- Guilherme Costa,
- Guilherme Silva Cavalcanti,
- Guilherme Silva Cavalcanti,
- Gustavo Navarro Betônico,
- Gustavo Navarro Betônico,
- Hélder Reis,
- Helia Beatriz N. Araujo,
- Helio Anjos Hortiz Júnior,
- Helio Penna Guimaraes,
- Hugo Urbano,
- Israel Maia,
- Ivan Lopes Santiago Filho,
- Jamil Farhat Júnior,
- Janu Rangel Alvarez,
- Joel Tavares Passos,
- Jorge Eduardo da Rocha Paranhos,
- José Aurelio Marques,
- José Gonçalves Moreira Filho,
- Jose Neto Andrade,
- José Onofre de C Sobrinho,
- Jose Terceiro de Paiva Bezerra,
- Juliana Apolônio Alves,
- Juliana Ferreira,
- Jussara Gomes,
- Karina Midori Sato,
- Karine Gerent,
- Kathia Margarida Costa Teixeira,
- Katia Aparecida Pessoa Conde,
- Laércia Ferreira Martins,
- Lanese Figueirêdo,
- Leila Rezegue,
- Leonardo Tcherniacovsk,
- Leone Oliveira Ferraz,
- Liane Cavalcante,
- Ligia Rabelo,
- Lilian Miilher,
- Lisiane Garcia,
- Luana Tannous,
- Ludhmila Abrahão Hajjar,
- Luís Eduardo Miranda Paciência,
- Luiz Monteiro da Cruz Neto,
- Macia Valeria Bley,
- Marcelo Ferreira Sousa,
- Marcelo Lourencini Puga,
- Marcelo Luz Pereira Romano,
- Marciano Nobrega,
- Marcio Arbex,
- Márcio Leite Rodrigues,
- Márcio Osório Guerreiro,
- Marcone Rocha,
- Maria Angela Pangoni Alves,
- Maria Angela Pangoni Alves,
- Maria Doroti Rosa,
- Mariza D’Agostino Dias,
- Miquéias Martins,
- Mirella de Oliveira,
- Miriane Melo Silveira Moretti,
- Mirna Matsui,
- Octavio Messender,
- Orlando Luís de Andrade Santarém,
- Patricio Júnior Henrique da Silveira,
- Paula Frizera Vassallo,
- Paulo Antoniazzi,
- Paulo César Gottardo,
- Paulo Correia,
- Paulo Ferreira,
- Paulo Torres,
- Pedro Gabrile M. de Barros e Silva,
- Rafael Foernges,
- Rafael Gomes,
- Rafael Moraes,
- Raimundo Nonato filho,
- Renato Luis Borba,
- Renato V Gomes,
- Ricardo Cordioli,
- Ricardo Lima,
- Ricardo Pérez López,
- Ricardo Rath de Oliveira Gargioni,
- Richard Rosenblat,
- Roberta Machado de Souza,
- Roberto Almeida,
- Roberto Camargo Narciso,
- Roberto Marco,
- Roberto waltrick,
- Rodrigo Biondi,
- Rodrigo Figueiredo,
- Rodrigo Santana Dutra,
- Roseane Batista,
- Rouge Felipe,
- Rubens Sergio da Silva Franco,
- Sandra Houly,
- Sara Socorro Faria,
- Sergio Felix Pinto,
- Sergio Luzzi,
- Sergio Sant’ana,
- Sergio Sonego Fernandes,
- Sérgio Yamada,
- Sérgio Zajac,
- Sidiner Mesquita Vaz,
- Silvia Aparecida Bezerra Bezerra,
- Tatiana Bueno Tardivo Farhat,
- Thiago Martins Santos,
- Tiago Smith,
- Ulysses V. A. Silva,
- Valnei Bento Damasceno,
- Vandack Nobre,
- Vicente Cés de Souza Dantas,
- Vivian Menezes Irineu,
- Viviane Bogado,
- Wagner Nedel,
- Walther Campos Filho,
- Weidson Dantas,
- William Viana,
- Wilson de Oliveira Filho,
- Wilson Martins Delgadinho,
- Simon Finfer,
- Flavia Ribeiro Machado
Views1See moreAbstract
Objective:
To describe fluid resuscitation practices in Brazilian intensive care units and to compare them with those of other countries participating in the Fluid-TRIPS.
Methods:
This was a prospective, international, cross-sectional, observational study in a convenience sample of intensive care units in 27 countries (including Brazil) using the Fluid-TRIPS database compiled in 2014. We described the patterns of fluid resuscitation use in Brazil compared with those in other countries and identified the factors associated with fluid choice.
Results:
On the study day, 3,214 patients in Brazil and 3,493 patients in other countries were included, of whom 16.1% and 26.8% (p < 0.001) received fluids, respectively. The main indication for fluid resuscitation was impaired perfusion and/or low cardiac output (Brazil: 71.7% versus other countries: 56.4%, p < 0.001). In Brazil, the percentage of patients receiving crystalloid solutions was higher (97.7% versus 76.8%, p < 0.001), and 0.9% sodium chloride was the most commonly used crystalloid (62.5% versus 27.1%, p < 0.001). The multivariable analysis suggested that the albumin levels were associated with the use of both crystalloids and colloids, whereas the type of fluid prescriber was associated with crystalloid use only.
Conclusion:
Our results suggest that crystalloids are more frequently used than colloids for fluid resuscitation in Brazil, and this discrepancy in frequencies is higher than that in other countries. Sodium chloride (0.9%) was the crystalloid most commonly prescribed. Serum albumin levels and the type of fluid prescriber were the factors associated with the choice of crystalloids or colloids for fluid resuscitation.
- Flavio Geraldo Rezende de Freitas
-
Original Article
The economic effect of extracorporeal membrane oxygenation to support adults with severe respiratory failure in Brazil: a hypothetical analysis
Rev Bras Ter Intensiva. 2014;26(3):253-262
Abstract
Original ArticleThe economic effect of extracorporeal membrane oxygenation to support adults with severe respiratory failure in Brazil: a hypothetical analysis
Rev Bras Ter Intensiva. 2014;26(3):253-262
DOI 10.5935/0103-507X.20140036
Views0Objective:
To analyze the cost-utility of using extracorporeal oxygenation for patients with severe acute respiratory distress syndrome in Brazil.
Methods:
A decision tree was constructed using databases from previously published studies. Costs were taken from the average price paid by the Brazilian Unified Health System (Sistema Único de Saúde; SUS) over three months in 2011. Using the data of 10,000,000 simulated patients with predetermined outcomes and costs, an analysis was performed of the ratio between cost increase and years of life gained, adjusted for quality (cost-utility), with survival rates of 40 and 60% for patients using extracorporeal membrane oxygenation.
Results:
The decision tree resulted in 16 outcomes with different life support techniques. With survival rates of 40 and 60%, respectively, the increased costs were R$=-301.00/-14.00, with a cost of R$=-30,913.00/-1,752.00 paid per six-month quality-adjusted life-year gained and R$=-2,386.00/-90.00 per quality-adjusted life-year gained until the end of life, when all patients with severe ARDS were analyzed. Analyzing only patients with severe hypoxemia (i.e., a ratio of partial oxygen pressure in the blood to the fraction of inspired oxygen <100mmHg), the increased cost was R$=-5,714.00/272.00, with a cost per six-month quality-adjusted life-year gained of R$=-9,521.00/293.00 and a cost of R$=-280.00/7.00 per quality-adjusted life-year gained.
Conclusion:
The cost-utility ratio associated with the use of extracorporeal membrane oxygenation in Brazil is potentially acceptable according to this hypothetical study.
Keywords:Costs and cost analysisExtracorporeal membrane oxygenation/economyIntensive care unitsRespiration, artificialRespiratory insufficiencySee moreViews0Abstract
Original ArticleThe economic effect of extracorporeal membrane oxygenation to support adults with severe respiratory failure in Brazil: a hypothetical analysis
Rev Bras Ter Intensiva. 2014;26(3):253-262
DOI 10.5935/0103-507X.20140036
Views0Objective:
To analyze the cost-utility of using extracorporeal oxygenation for patients with severe acute respiratory distress syndrome in Brazil.
Methods:
A decision tree was constructed using databases from previously published studies. Costs were taken from the average price paid by the Brazilian Unified Health System (Sistema Único de Saúde; SUS) over three months in 2011. Using the data of 10,000,000 simulated patients with predetermined outcomes and costs, an analysis was performed of the ratio between cost increase and years of life gained, adjusted for quality (cost-utility), with survival rates of 40 and 60% for patients using extracorporeal membrane oxygenation.
Results:
The decision tree resulted in 16 outcomes with different life support techniques. With survival rates of 40 and 60%, respectively, the increased costs were R$=-301.00/-14.00, with a cost of R$=-30,913.00/-1,752.00 paid per six-month quality-adjusted life-year gained and R$=-2,386.00/-90.00 per quality-adjusted life-year gained until the end of life, when all patients with severe ARDS were analyzed. Analyzing only patients with severe hypoxemia (i.e., a ratio of partial oxygen pressure in the blood to the fraction of inspired oxygen <100mmHg), the increased cost was R$=-5,714.00/272.00, with a cost per six-month quality-adjusted life-year gained of R$=-9,521.00/293.00 and a cost of R$=-280.00/7.00 per quality-adjusted life-year gained.
Conclusion:
The cost-utility ratio associated with the use of extracorporeal membrane oxygenation in Brazil is potentially acceptable according to this hypothetical study.
Keywords:Costs and cost analysisExtracorporeal membrane oxygenation/economyIntensive care unitsRespiration, artificialRespiratory insufficiencySee more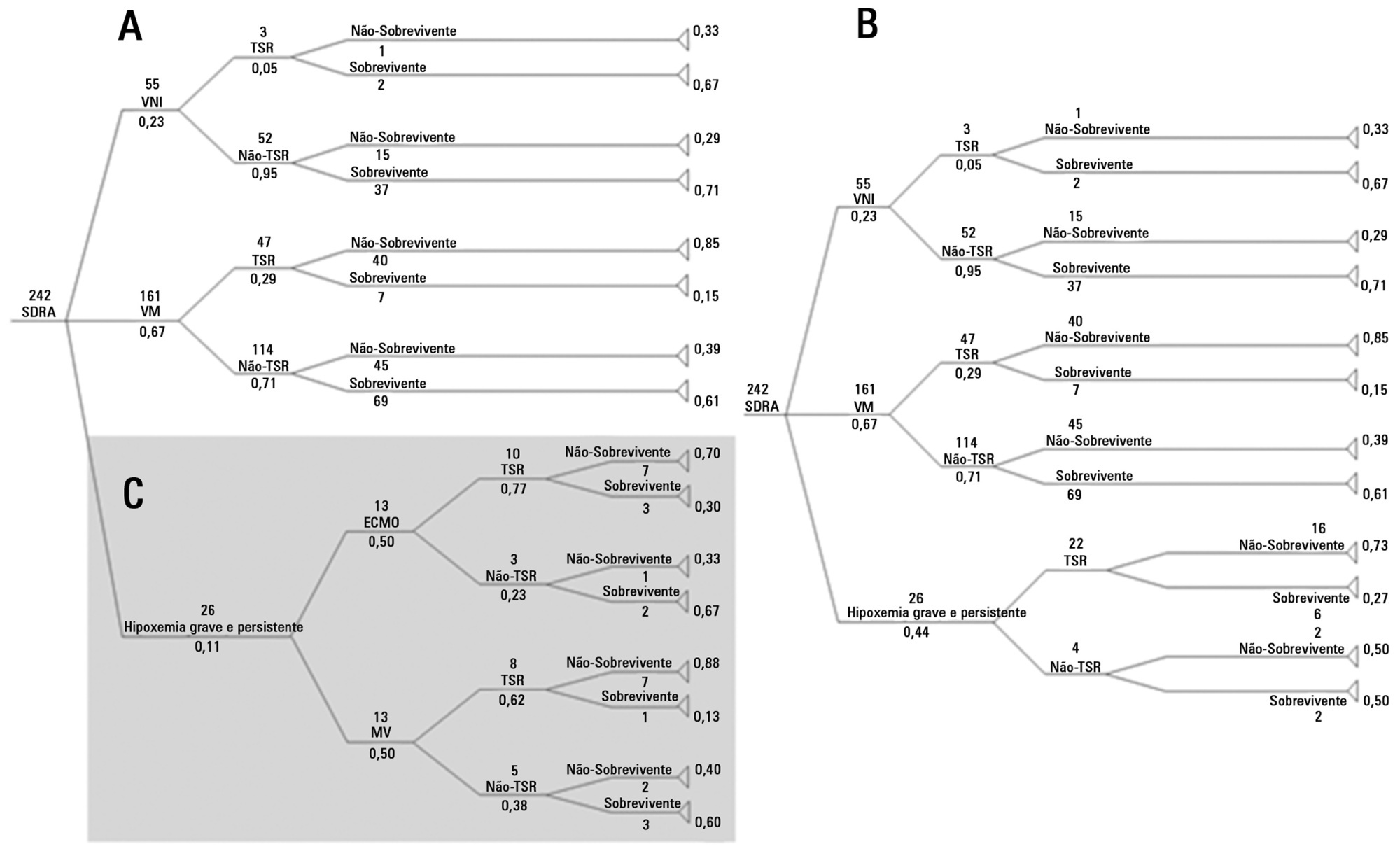
-
Original Articles
Anion gap corrected for albumin, phosphate and lactate is a good predictor of strong ion gap in critically ill patients: a nested cohort study
Rev Bras Ter Intensiva. 2013;25(3):205-211
Abstract
Original ArticlesAnion gap corrected for albumin, phosphate and lactate is a good predictor of strong ion gap in critically ill patients: a nested cohort study
Rev Bras Ter Intensiva. 2013;25(3):205-211
DOI 10.5935/0103-507X.20130036
Views1OBJECTIVE:
Corrected anion gap and strong ion gap are commonly used to estimate unmeasured anions. We evaluated the performance of the anion gap corrected for albumin, phosphate and lactate in predicting strong ion gap in a mixed population of critically ill patients. We hypothesized that anion gap corrected for albumin, phosphate and lactate would be a good predictor of strong ion gap, independent of the presence of metabolic acidosis. In addition, we evaluated the impact of strong ion gap at admission on hospital mortality.
METHODS:
We included 84 critically ill patients. Correlation and agreement between the anion gap corrected for albumin, phosphate and lactate and strong ion gap was evaluated by the Pearson correlation test, linear regression, a Bland-Altman plot and calculating interclass correlation coefficient. Two subgroup analyses were performed: one in patients with base-excess <-2mEq/L (low BE group - lBE) and the other in patients with base-excess >-2mEq/L (high BE group – hBE). A logistic regression was performed to evaluate the association between admission strong ion gap levels and hospital mortality.
RESULTS:
There was a very strong correlation and a good agreement between anion gap corrected for albumin, phosphate and lactate and strong ion gap in the general population (r2=0.94; bias 1.40; limits of agreement -0.75 to 3.57). Correlation was also high in the lBE group (r2=0.94) and in the hBE group (r2=0.92). High levels of strong ion gap were present in 66% of the whole population and 42% of the cases in the hBE group. Strong ion gap was not associated with hospital mortality by logistic regression.
CONCLUSION:
Anion gap corrected for albumin, phosphate and lactate and strong ion gap have an excellent correlation. Unmeasured anions are frequently elevated in critically ill patients with normal base-excess. However, there was no association between unmeasured anions and hospital mortality.
Keywords:Acid-base equilibrium/ physiologyBlood chemical analysisCritical illnessLactate/bloodPhosphate/ bloodPrognosisSerum albumin/bloodSee moreViews1Abstract
Original ArticlesAnion gap corrected for albumin, phosphate and lactate is a good predictor of strong ion gap in critically ill patients: a nested cohort study
Rev Bras Ter Intensiva. 2013;25(3):205-211
DOI 10.5935/0103-507X.20130036
Views1OBJECTIVE:
Corrected anion gap and strong ion gap are commonly used to estimate unmeasured anions. We evaluated the performance of the anion gap corrected for albumin, phosphate and lactate in predicting strong ion gap in a mixed population of critically ill patients. We hypothesized that anion gap corrected for albumin, phosphate and lactate would be a good predictor of strong ion gap, independent of the presence of metabolic acidosis. In addition, we evaluated the impact of strong ion gap at admission on hospital mortality.
METHODS:
We included 84 critically ill patients. Correlation and agreement between the anion gap corrected for albumin, phosphate and lactate and strong ion gap was evaluated by the Pearson correlation test, linear regression, a Bland-Altman plot and calculating interclass correlation coefficient. Two subgroup analyses were performed: one in patients with base-excess <-2mEq/L (low BE group - lBE) and the other in patients with base-excess >-2mEq/L (high BE group – hBE). A logistic regression was performed to evaluate the association between admission strong ion gap levels and hospital mortality.
RESULTS:
There was a very strong correlation and a good agreement between anion gap corrected for albumin, phosphate and lactate and strong ion gap in the general population (r2=0.94; bias 1.40; limits of agreement -0.75 to 3.57). Correlation was also high in the lBE group (r2=0.94) and in the hBE group (r2=0.92). High levels of strong ion gap were present in 66% of the whole population and 42% of the cases in the hBE group. Strong ion gap was not associated with hospital mortality by logistic regression.
CONCLUSION:
Anion gap corrected for albumin, phosphate and lactate and strong ion gap have an excellent correlation. Unmeasured anions are frequently elevated in critically ill patients with normal base-excess. However, there was no association between unmeasured anions and hospital mortality.
Keywords:Acid-base equilibrium/ physiologyBlood chemical analysisCritical illnessLactate/bloodPhosphate/ bloodPrognosisSerum albumin/bloodSee more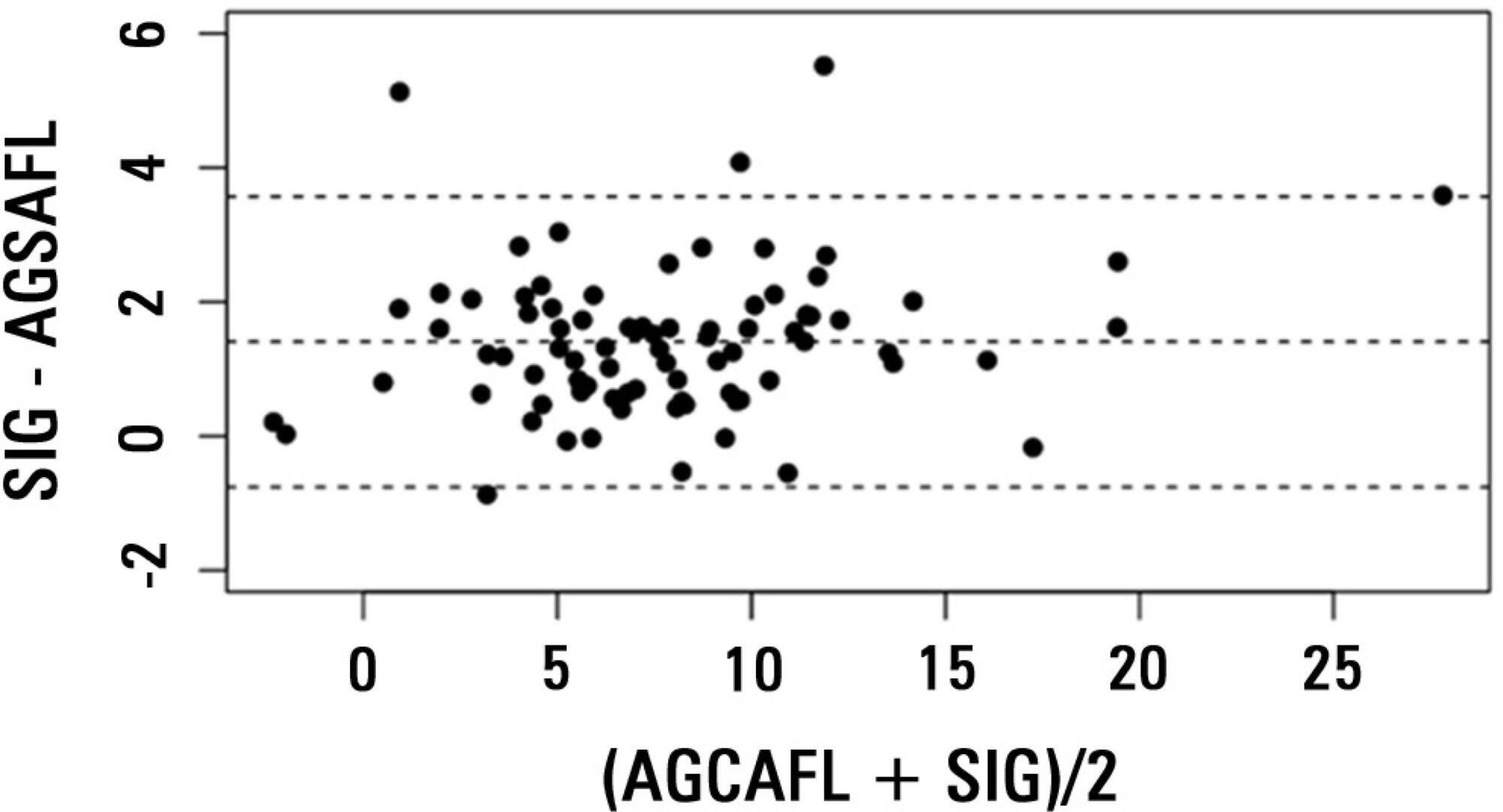
-
Original Articles
HLA-A*31 as a marker of genetic susceptibility to sepsis
Rev Bras Ter Intensiva. 2013;25(4):284-289
Abstract
Original ArticlesHLA-A*31 as a marker of genetic susceptibility to sepsis
Rev Bras Ter Intensiva. 2013;25(4):284-289
DOI 10.5935/0103-507X.20130049
Views0See moreObjective:
The HLA haplotype has been associated with many autoimmune diseases, but no associations have been described in sepsis. This study aims to investigate the HLA system as a possible marker of genetic sepsis susceptibility.
Methods:
This is a prospective cohort study including patients admitted to an intensive care unit and healthy controls from a list of renal transplant donors. Patients with less 18 years of age; pregnant or HIV positive patients; those with metastatic malignancies or receiving chemotherapy; or with advanced liver disease; or with end-of-life conditions were excluded. The DNA was extracted from the whole blood and HLA haplotypes determined using MiliPlex® technology.
Results:
From October 2010 to October 2012, 1,121 patients were included (1,078 kidney donors, 20 patients admitted with severe sepsis and 23 with septic shock). HLA-A*31 positive subjects had increased risk of developing sepsis (OR 2.36, 95%CI 1.26-5.35). Considering a p value <0.01, no other significant association was identified.
Conclusion:
HLA-A*31 expression is associated to risk of developing sepsis.
Views0Abstract
Original ArticlesHLA-A*31 as a marker of genetic susceptibility to sepsis
Rev Bras Ter Intensiva. 2013;25(4):284-289
DOI 10.5935/0103-507X.20130049
Views0See moreObjective:
The HLA haplotype has been associated with many autoimmune diseases, but no associations have been described in sepsis. This study aims to investigate the HLA system as a possible marker of genetic sepsis susceptibility.
Methods:
This is a prospective cohort study including patients admitted to an intensive care unit and healthy controls from a list of renal transplant donors. Patients with less 18 years of age; pregnant or HIV positive patients; those with metastatic malignancies or receiving chemotherapy; or with advanced liver disease; or with end-of-life conditions were excluded. The DNA was extracted from the whole blood and HLA haplotypes determined using MiliPlex® technology.
Results:
From October 2010 to October 2012, 1,121 patients were included (1,078 kidney donors, 20 patients admitted with severe sepsis and 23 with septic shock). HLA-A*31 positive subjects had increased risk of developing sepsis (OR 2.36, 95%CI 1.26-5.35). Considering a p value <0.01, no other significant association was identified.
Conclusion:
HLA-A*31 expression is associated to risk of developing sepsis.
Search
Search in:
KEY WORDS
Case reports Child Coronavirus infections COVID-19 Critical care Critical illness Extracorporeal membrane oxygenation Infant, newborn Intensive care Intensive care units Intensive care units, pediatric mechanical ventilation Mortality Physical therapy modalities Prognosis Respiration, artificial Respiratory insufficiency risk factors SARS-CoV-2 Sepsis