Brain injuries Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2022;34(4):410-417
DOI 10.5935/0103-507X.20220261-en
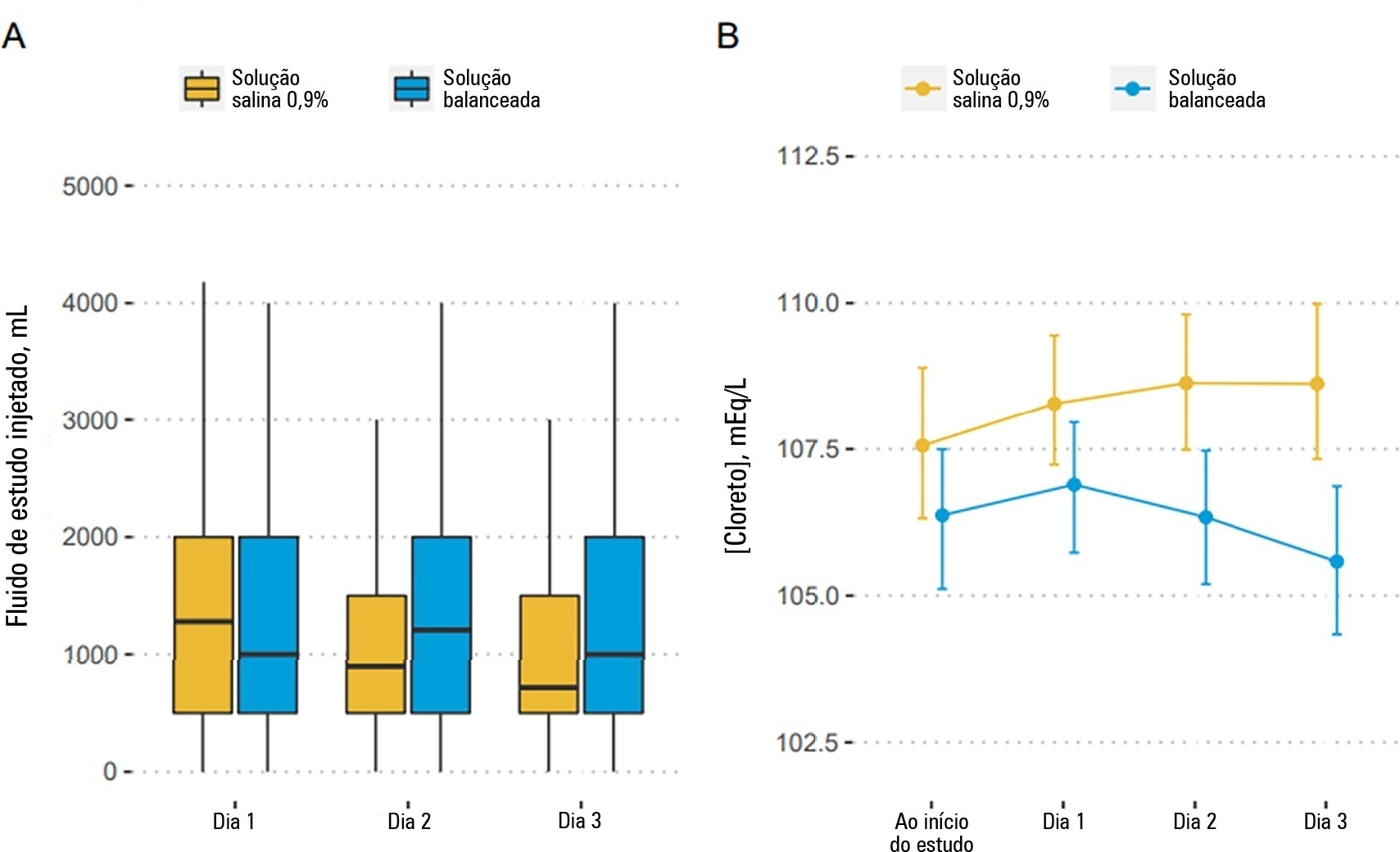
To describe the effects of balanced solution use on the short-term outcomes of patients with traumatic brain injury enrolled in BaSICS trial.
Patients were randomized to receive either 0.9% saline or balanced solution during their intensive care unit stay. The primary endpoint was 90-day mortality, and the secondary outcomes were days alive and free of intensive care unit stay at 28 days. The primary endpoint was assessed using Bayesian logistic regression. The secondary endpoint was assessed using a Bayesian zero-inflated beta binomial regression.
We included 483 patients (236 in the 0.9% saline arm and 247 in the balanced solution arm). A total of 338 patients (70%) with a Glasgow coma scale score ≤ 12 were enrolled. The overall probability that balanced solutions were associated with higher 90-day mortality was 0.98 (OR 1.48; 95%CrI 1.04 - 2.09); this mortality increment was particularly noticeable in patients with a Glasgow coma scale score below 6 at enrollment (probability of harm of 0.99). Balanced solutions were associated with -1.64 days alive and free of intensive care unit at 28 days (95%CrI -3.32 - 0.00) with a probability of harm of 0.97.
There was a high probability that balanced solutions were associated with high 90-day mortality and fewer days alive and free of intensive care units at 28 days.
Abstract
Rev Bras Ter Intensiva. 2022;34(4):410-417
DOI 10.5935/0103-507X.20220261-en
To describe the effects of balanced solution use on the short-term outcomes of patients with traumatic brain injury enrolled in BaSICS trial.
Patients were randomized to receive either 0.9% saline or balanced solution during their intensive care unit stay. The primary endpoint was 90-day mortality, and the secondary outcomes were days alive and free of intensive care unit stay at 28 days. The primary endpoint was assessed using Bayesian logistic regression. The secondary endpoint was assessed using a Bayesian zero-inflated beta binomial regression.
We included 483 patients (236 in the 0.9% saline arm and 247 in the balanced solution arm). A total of 338 patients (70%) with a Glasgow coma scale score ≤ 12 were enrolled. The overall probability that balanced solutions were associated with higher 90-day mortality was 0.98 (OR 1.48; 95%CrI 1.04 - 2.09); this mortality increment was particularly noticeable in patients with a Glasgow coma scale score below 6 at enrollment (probability of harm of 0.99). Balanced solutions were associated with -1.64 days alive and free of intensive care unit at 28 days (95%CrI -3.32 - 0.00) with a probability of harm of 0.97.
There was a high probability that balanced solutions were associated with high 90-day mortality and fewer days alive and free of intensive care units at 28 days.
Abstract
Rev Bras Ter Intensiva. 2022;34(1):197-201
Abstract
Rev Bras Ter Intensiva. 2022;34(1):197-201
Abstract
Rev Bras Ter Intensiva. 2021;33(3):469-476
DOI 10.5935/0103-507X.20210066
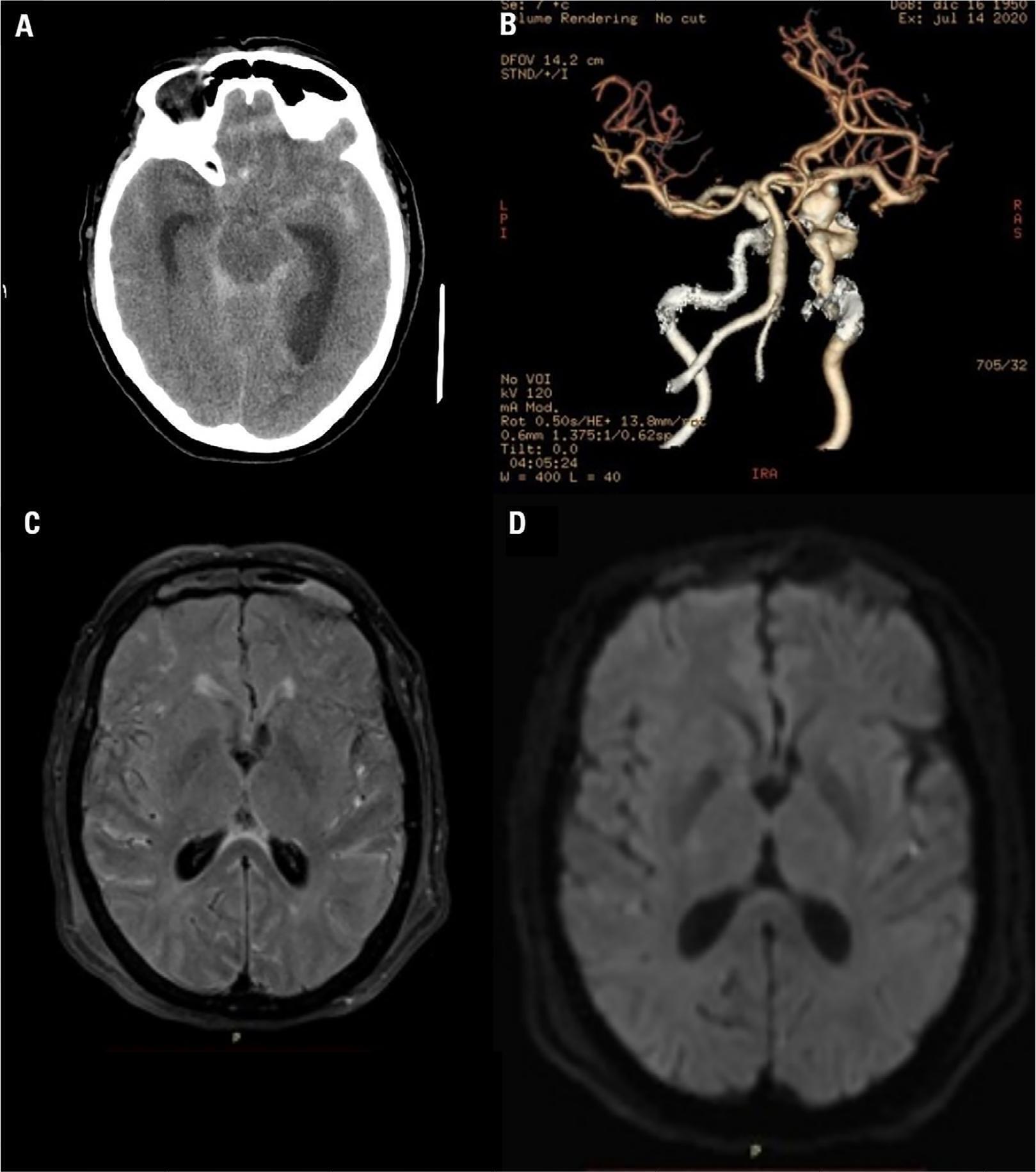
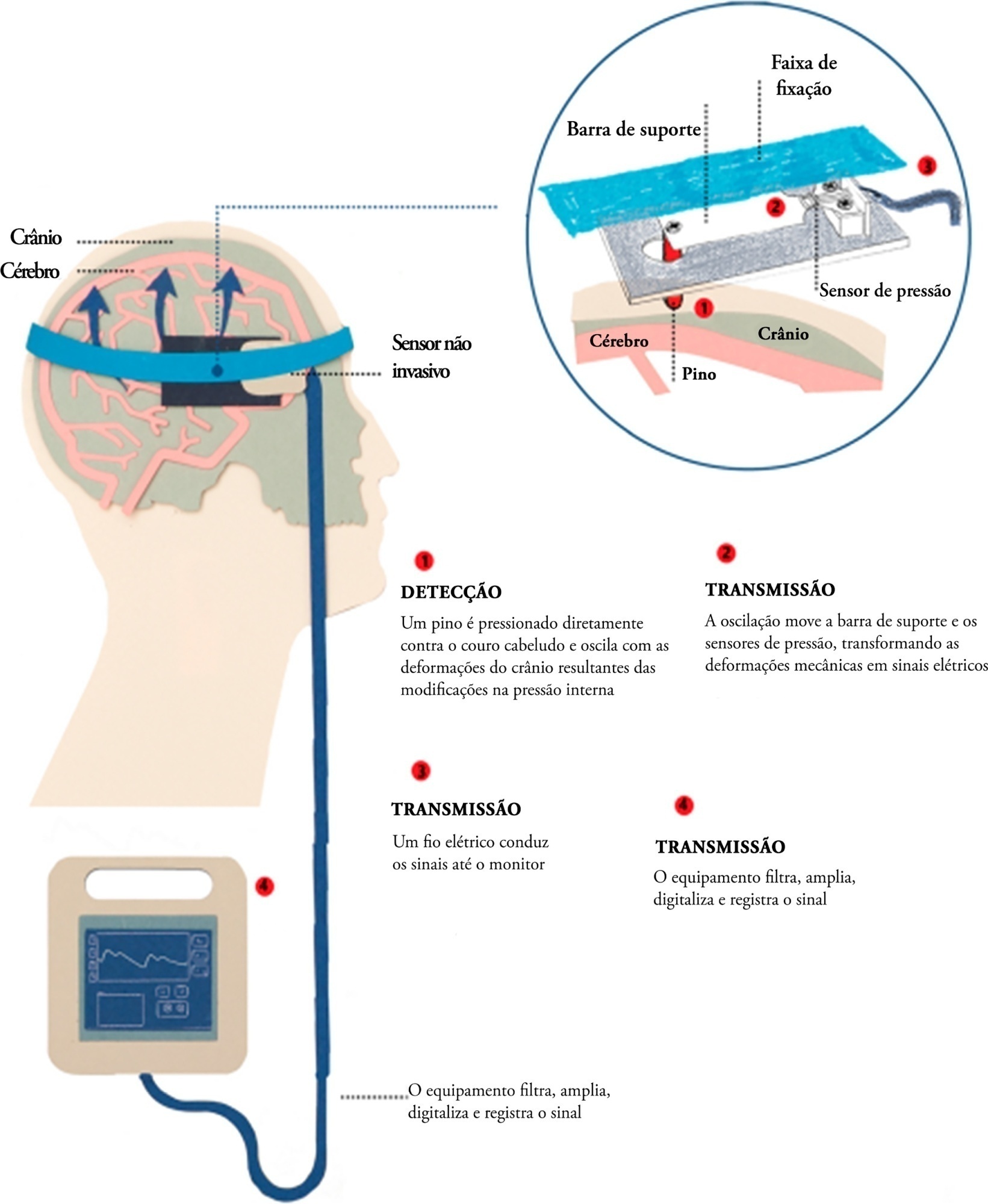
Brain injury caused by extracorporeal circulation during cardiovascular surgical procedures has been a recurring complication since the implementation of extracorporeal circulation five decades ago. There is no unique cause of brain injury due to the use of extracorporeal circulation, but it is known that brain injury affects about 70% of patients who undergo this procedure. Intracranial pressure assessment is one method that can guide the management of patients undergoing procedures associated with neurological disturbances. This study describes two cases of patients who underwent cardiovascular surgery with extracorporeal circulation in whom clinical protocols for neuroprotection in the postoperative phase were guided by intracranial pressure waveform findings obtained with a novel noninvasive intracranial pressure monitoring method.
Abstract
Rev Bras Ter Intensiva. 2021;33(3):469-476
DOI 10.5935/0103-507X.20210066
Brain injury caused by extracorporeal circulation during cardiovascular surgical procedures has been a recurring complication since the implementation of extracorporeal circulation five decades ago. There is no unique cause of brain injury due to the use of extracorporeal circulation, but it is known that brain injury affects about 70% of patients who undergo this procedure. Intracranial pressure assessment is one method that can guide the management of patients undergoing procedures associated with neurological disturbances. This study describes two cases of patients who underwent cardiovascular surgery with extracorporeal circulation in whom clinical protocols for neuroprotection in the postoperative phase were guided by intracranial pressure waveform findings obtained with a novel noninvasive intracranial pressure monitoring method.
Abstract
Rev Bras Ter Intensiva. 2018;30(2):237-243
DOI 10.5935/0103-507X.20180035
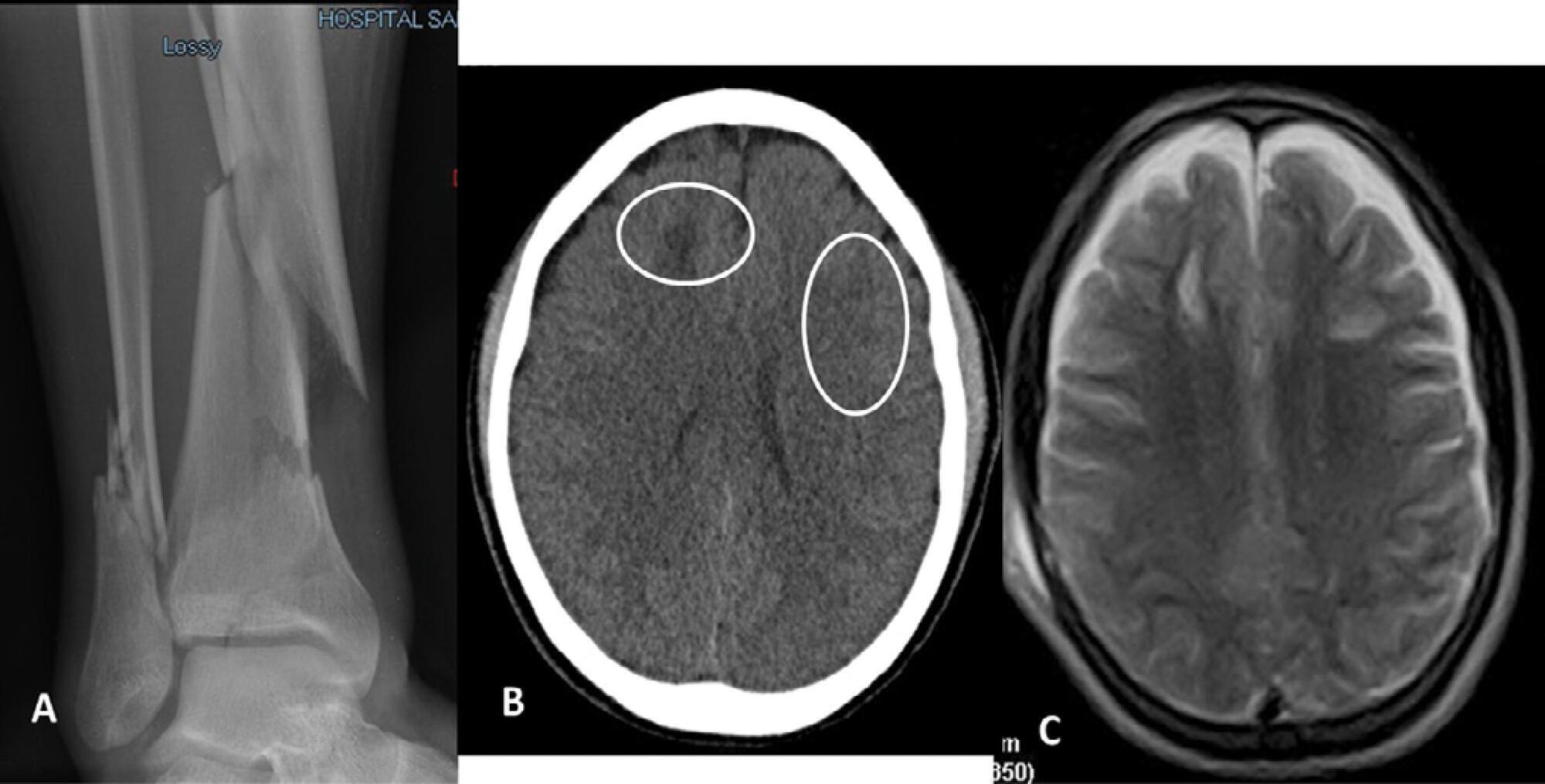
Paroxysmal sympathetic hyperactivity represents an uncommon and potentially life-threatening complication of severe brain injuries, which are most commonly traumatic. This syndrome is a clinical diagnosis based on the recurrent occurrence of tachycardia, hypertension, diaphoresis, tachypnea, and occasionally high fever and dystonic postures. The episodes may be induced by stimulation or may occur spontaneously. Underdiagnosis is common, and delayed recognition may increase morbidity and long-term disability. Trigger avoidance and pharmacological therapy can be very successful in controlling this complication. Fat embolism syndrome is a rare but serious complication of long bone fractures. Neurologic signs, petechial hemorrhages and acute respiratory failure constitute the characteristic presenting triad. The term cerebral fat embolism is used when the neurological involvement predominates. The diagnosis is clinical, but specific neuroimaging findings can be supportive. The neurologic manifestations include different degrees of alteration of consciousness, focal deficits or seizures. Management is supportive, but good outcomes are possible even in cases with very severe presentation. We report two cases of paroxysmal sympathetic hyperactivity after cerebral fat embolism, which is a very uncommon association.
Abstract
Rev Bras Ter Intensiva. 2018;30(2):237-243
DOI 10.5935/0103-507X.20180035
Paroxysmal sympathetic hyperactivity represents an uncommon and potentially life-threatening complication of severe brain injuries, which are most commonly traumatic. This syndrome is a clinical diagnosis based on the recurrent occurrence of tachycardia, hypertension, diaphoresis, tachypnea, and occasionally high fever and dystonic postures. The episodes may be induced by stimulation or may occur spontaneously. Underdiagnosis is common, and delayed recognition may increase morbidity and long-term disability. Trigger avoidance and pharmacological therapy can be very successful in controlling this complication. Fat embolism syndrome is a rare but serious complication of long bone fractures. Neurologic signs, petechial hemorrhages and acute respiratory failure constitute the characteristic presenting triad. The term cerebral fat embolism is used when the neurological involvement predominates. The diagnosis is clinical, but specific neuroimaging findings can be supportive. The neurologic manifestations include different degrees of alteration of consciousness, focal deficits or seizures. Management is supportive, but good outcomes are possible even in cases with very severe presentation. We report two cases of paroxysmal sympathetic hyperactivity after cerebral fat embolism, which is a very uncommon association.
Abstract
Rev Bras Ter Intensiva. 2015;27(2):113-118
DOI 10.5935/0103-507X.20150021
To analyze the clinical characteristics, complications and factors associated with the prognosis of severe traumatic brain injury among patients who undergo a decompressive craniectomy.
Retrospective study of patients seen in an intensive care unit with severe traumatic brain injury in whom a decompressive craniectomy was performed between the years 2003 and 2012. Patients were followed until their discharge from the intensive care unit. Their clinical-tomographic characteristics, complications, and factors associated with prognosis (univariate and multivariate analysis) were analyzed.
A total of 64 patients were studied. Primary and lateral decompressive craniectomies were performed for the majority of patients. A high incidence of complications was found (78% neurological and 52% nonneurological). A total of 42 patients (66%) presented poor outcomes, and 22 (34%) had good neurological outcomes. Of the patients who survived, 61% had good neurological outcomes. In the univariate analysis, the factors significantly associated with poor neurological outcome were postdecompressive craniectomy intracranial hypertension, greater severity and worse neurological state at admission. In the multivariate analysis, only postcraniectomy intracranial hypertension was significantly associated with a poor outcome.
This study involved a very severe and difficult to manage group of patients with high morbimortality. Intracranial hypertension was a main factor of poor outcome in this population.
Abstract
Rev Bras Ter Intensiva. 2015;27(2):113-118
DOI 10.5935/0103-507X.20150021
To analyze the clinical characteristics, complications and factors associated with the prognosis of severe traumatic brain injury among patients who undergo a decompressive craniectomy.
Retrospective study of patients seen in an intensive care unit with severe traumatic brain injury in whom a decompressive craniectomy was performed between the years 2003 and 2012. Patients were followed until their discharge from the intensive care unit. Their clinical-tomographic characteristics, complications, and factors associated with prognosis (univariate and multivariate analysis) were analyzed.
A total of 64 patients were studied. Primary and lateral decompressive craniectomies were performed for the majority of patients. A high incidence of complications was found (78% neurological and 52% nonneurological). A total of 42 patients (66%) presented poor outcomes, and 22 (34%) had good neurological outcomes. Of the patients who survived, 61% had good neurological outcomes. In the univariate analysis, the factors significantly associated with poor neurological outcome were postdecompressive craniectomy intracranial hypertension, greater severity and worse neurological state at admission. In the multivariate analysis, only postcraniectomy intracranial hypertension was significantly associated with a poor outcome.
This study involved a very severe and difficult to manage group of patients with high morbimortality. Intracranial hypertension was a main factor of poor outcome in this population.
Abstract
Rev Bras Ter Intensiva. 2015;27(4):315-321
DOI 10.5935/0103-507X.20150055
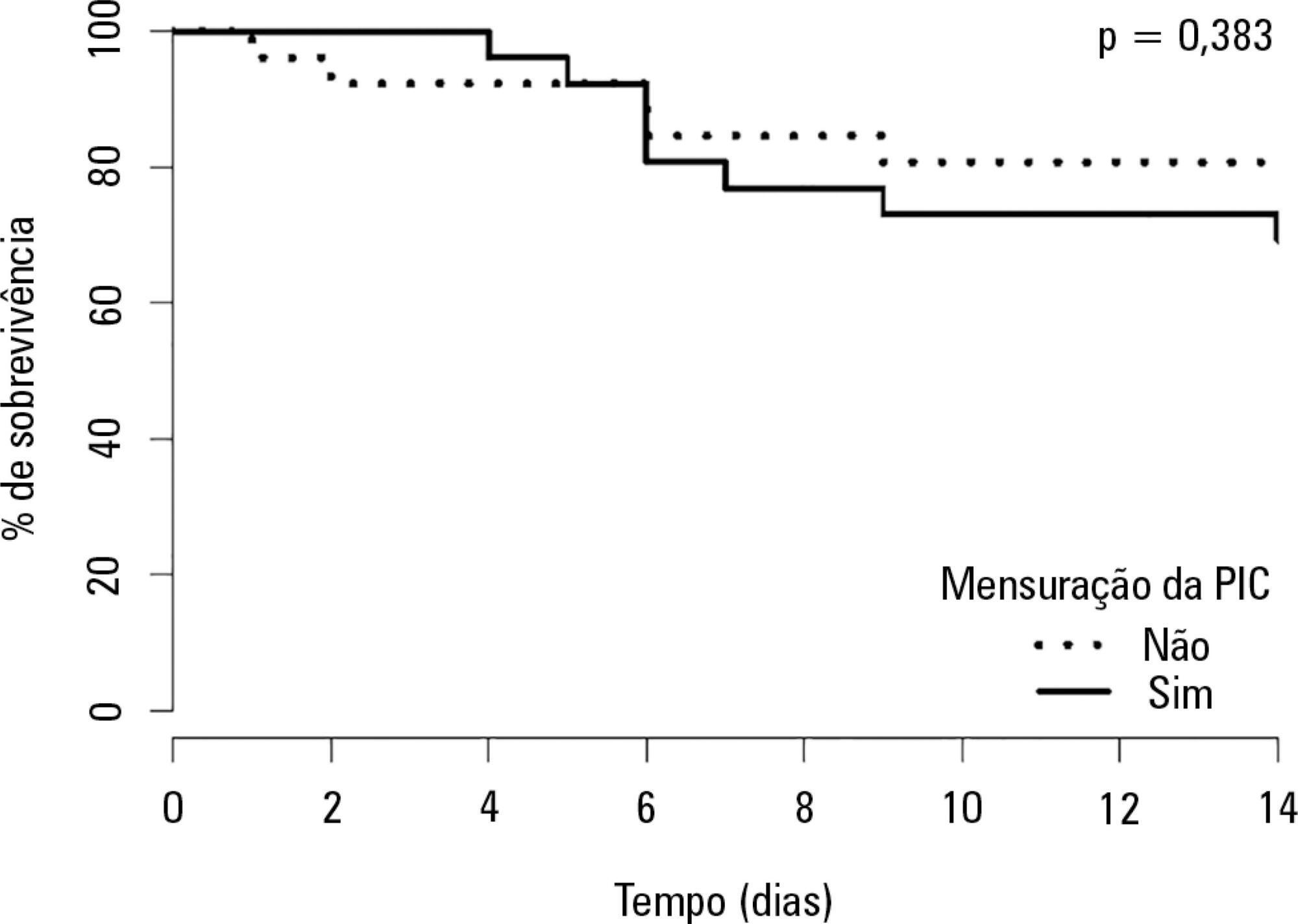
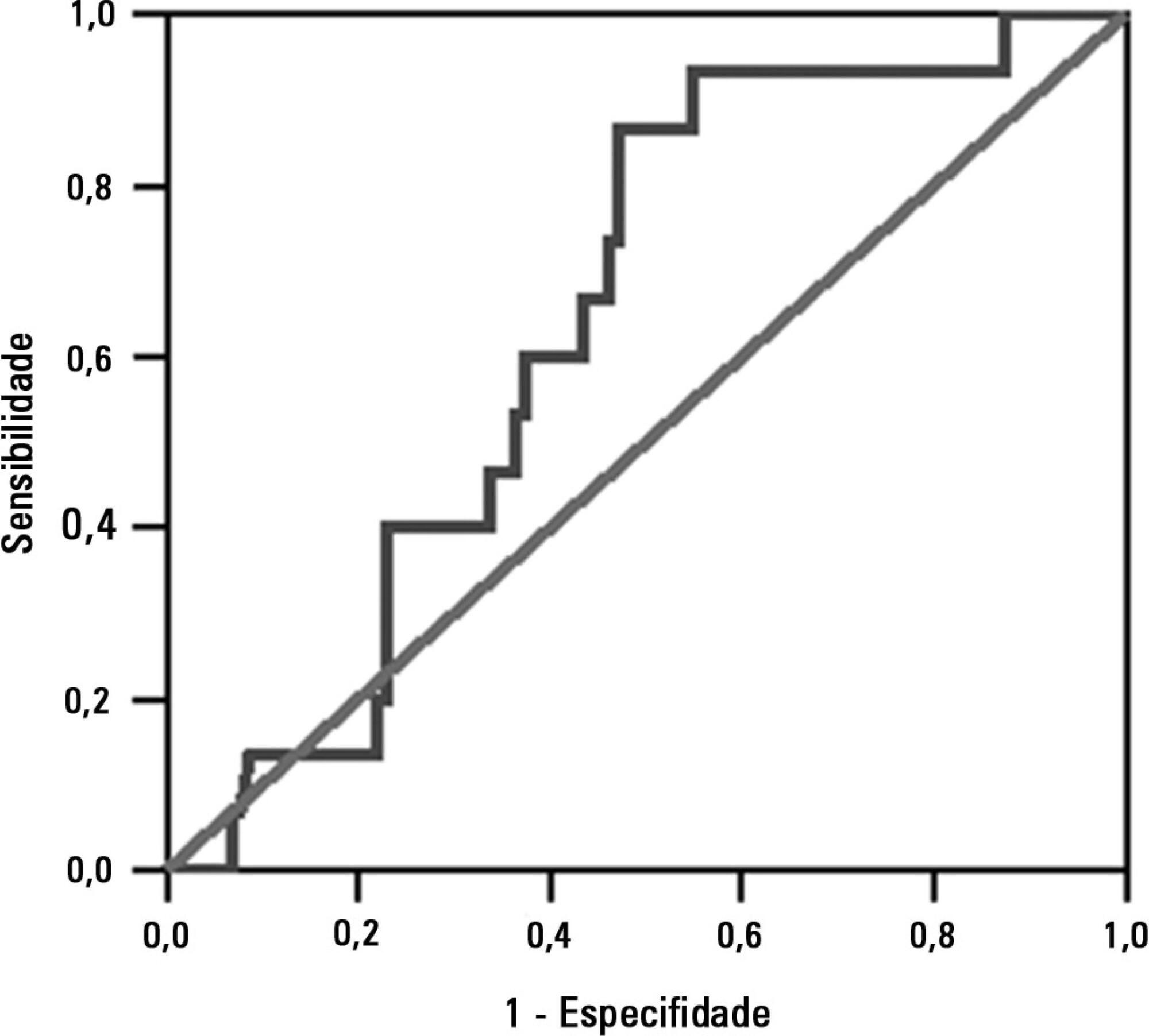
To assess the impact of intracranial pressure monitoring on the short-term outcomes of traumatic brain injury patients.
Retrospective observational study including 299 consecutive patients admitted due to traumatic brain injury from January 2011 through July 2012 at a Level 1 trauma center in São Paulo, Brazil. Patients were categorized in two groups according to the measurement of intracranial pressure (measured intracranial pressure and non-measured intracranial pressure groups). We applied a propensity-matched analysis to adjust for possible confounders (variables contained in the Crash Score prognostic algorithm).
Global mortality at 14 days (16%) was equal to that observed in high-income countries in the CRASH Study and was better than expected based on the CRASH calculator score (20.6%), with a standardized mortality ratio of 0.77. A total of 28 patients received intracranial pressure monitoring (measured intracranial pressure group), of whom 26 were paired in a 1:1 fashion with patients from the non-measured intracranial pressure group. There was no improvement in the measured intracranial pressure group compared to the non-measured intracranial pressure group regarding hospital mortality, 14-day mortality, or combined hospital and chronic care facility mortality. Survival up to 14 days was also similar between groups.
Patients receiving intracranial pressure monitoring tend to have more severe traumatic brain injuries. However, after adjusting for multiple confounders using propensity scoring, no benefits in terms of survival were observed among intracranial pressure-monitored patients and those managed with a systematic clinical protocol.
Abstract
Rev Bras Ter Intensiva. 2015;27(4):315-321
DOI 10.5935/0103-507X.20150055
To assess the impact of intracranial pressure monitoring on the short-term outcomes of traumatic brain injury patients.
Retrospective observational study including 299 consecutive patients admitted due to traumatic brain injury from January 2011 through July 2012 at a Level 1 trauma center in São Paulo, Brazil. Patients were categorized in two groups according to the measurement of intracranial pressure (measured intracranial pressure and non-measured intracranial pressure groups). We applied a propensity-matched analysis to adjust for possible confounders (variables contained in the Crash Score prognostic algorithm).
Global mortality at 14 days (16%) was equal to that observed in high-income countries in the CRASH Study and was better than expected based on the CRASH calculator score (20.6%), with a standardized mortality ratio of 0.77. A total of 28 patients received intracranial pressure monitoring (measured intracranial pressure group), of whom 26 were paired in a 1:1 fashion with patients from the non-measured intracranial pressure group. There was no improvement in the measured intracranial pressure group compared to the non-measured intracranial pressure group regarding hospital mortality, 14-day mortality, or combined hospital and chronic care facility mortality. Survival up to 14 days was also similar between groups.
Patients receiving intracranial pressure monitoring tend to have more severe traumatic brain injuries. However, after adjusting for multiple confounders using propensity scoring, no benefits in terms of survival were observed among intracranial pressure-monitored patients and those managed with a systematic clinical protocol.
Abstract
Rev Bras Ter Intensiva. 2013;25(3):212-217
DOI 10.5935/0103-507X.20130037
To investigate the association between the rapid shallow breathing index and successful extubation in patients with traumatic brain injury.
This study was a prospective study conducted in patients with traumatic brain injury of both genders who underwent mechanical ventilation for at least two days and who passed a spontaneous breathing trial. The minute volume and respiratory rate were measured using a ventilometer, and the data were used to calculate the rapid shallow breathing index (respiratory rate/tidal volume). The dependent variable was the extubation outcome: reintubation after up to 48 hours (extubation failure) or not (extubation success). The independent variable was the rapid shallow breathing index measured after a successful spontaneous breathing trial.
The sample comprised 119 individuals, including 111 (93.3%) males. The average age of the sample was 35.0±12.9 years old. The average duration of mechanical ventilation was 8.1±3.6 days. A total of 104 (87.4%) participants achieved successful extubation. No association was found between the rapid shallow breathing index and extubation success.
The rapid shallow breathing index was not associated with successful extubation in patients with traumatic brain injury.
Abstract
Rev Bras Ter Intensiva. 2013;25(3):212-217
DOI 10.5935/0103-507X.20130037
To investigate the association between the rapid shallow breathing index and successful extubation in patients with traumatic brain injury.
This study was a prospective study conducted in patients with traumatic brain injury of both genders who underwent mechanical ventilation for at least two days and who passed a spontaneous breathing trial. The minute volume and respiratory rate were measured using a ventilometer, and the data were used to calculate the rapid shallow breathing index (respiratory rate/tidal volume). The dependent variable was the extubation outcome: reintubation after up to 48 hours (extubation failure) or not (extubation success). The independent variable was the rapid shallow breathing index measured after a successful spontaneous breathing trial.
The sample comprised 119 individuals, including 111 (93.3%) males. The average age of the sample was 35.0±12.9 years old. The average duration of mechanical ventilation was 8.1±3.6 days. A total of 104 (87.4%) participants achieved successful extubation. No association was found between the rapid shallow breathing index and extubation success.
The rapid shallow breathing index was not associated with successful extubation in patients with traumatic brain injury.
Abstract
Rev Bras Ter Intensiva. 2012;24(1):97-105
DOI 10.1590/S0103-507X2012000100015
This article reviews the literature, organizes the major findings, and generates the best evidence-based recommendations on nutrition therapy for head trauma patients. Despite recent advances in head trauma diagnosis and therapy, the mortality associated with this condition remains high. Few therapeutic interventions have been proven to effectively improve this condition. Head trauma causes multiple metabolic and electrolytic disorders; it is characterized by a hypermetabolic state that is associated with intensive catabolism, leading to specific nutritional needs. The current literature lacks specific guidelines for nutrition therapy in severe head trauma patients, although a substantial amount of data has been reported and relevant issues are currently being studied; these data may allow better nutrition therapy guidelines for these patients. In addition to a well-trained multi-disciplinary team, the following recommendations appear to improve outcomes: introducing nutrition therapy early; preferred enteral administration; appropriate energy intake; formulations that are tailored to specific patients, including appropriate nutrients; and strict electrolytic and metabolic monitoring. Understanding the pathophysiology and the consequences of therapy is fundamental.
Abstract
Rev Bras Ter Intensiva. 2012;24(1):97-105
DOI 10.1590/S0103-507X2012000100015
This article reviews the literature, organizes the major findings, and generates the best evidence-based recommendations on nutrition therapy for head trauma patients. Despite recent advances in head trauma diagnosis and therapy, the mortality associated with this condition remains high. Few therapeutic interventions have been proven to effectively improve this condition. Head trauma causes multiple metabolic and electrolytic disorders; it is characterized by a hypermetabolic state that is associated with intensive catabolism, leading to specific nutritional needs. The current literature lacks specific guidelines for nutrition therapy in severe head trauma patients, although a substantial amount of data has been reported and relevant issues are currently being studied; these data may allow better nutrition therapy guidelines for these patients. In addition to a well-trained multi-disciplinary team, the following recommendations appear to improve outcomes: introducing nutrition therapy early; preferred enteral administration; appropriate energy intake; formulations that are tailored to specific patients, including appropriate nutrients; and strict electrolytic and metabolic monitoring. Understanding the pathophysiology and the consequences of therapy is fundamental.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (116) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)