Brain injuries Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2008;20(4):411-421
DOI 10.1590/S0103-507X2008000400015
Trauma is the leading cause of death of people from 1 to 44 years of age. Traumatic brain injury is the main determinant for mortality and morbidity caused by trauma. Outcome prediction is one of the major problems related to severe traumatic brain injury because clinical evaluation has an unreliable predictive value and complicates identification of patients with higher risk of developing secondary lesions and fatal outcome. That is why, there is considerable interest in development of biomarkers that reflect the severity of brain injury and correlate with mortality and functional outcome. Proteins S100B and neuron specific enolases are among the markers most studied for this purpose, however some studies are investigating glial fibrillary acidic protein, creatinine phospokinase, isoenzime B, myelin basic protein, plasma desoxiribonucleic acid, heat shock protein 70, von Willebrand factor, metalloproteinases and brain-derived neurotrophic factor, among others. Evidence suggests that inflammation, oxidative stress, excitotoxicity, neuroendocrine responses and apoptosis play an important role in the development of secondary lesions. Markers involved in these processes are being studied in traumatic brain injury. We reviewed these biomarkers, some of which present promising results for future clinical application.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):411-421
DOI 10.1590/S0103-507X2008000400015
Trauma is the leading cause of death of people from 1 to 44 years of age. Traumatic brain injury is the main determinant for mortality and morbidity caused by trauma. Outcome prediction is one of the major problems related to severe traumatic brain injury because clinical evaluation has an unreliable predictive value and complicates identification of patients with higher risk of developing secondary lesions and fatal outcome. That is why, there is considerable interest in development of biomarkers that reflect the severity of brain injury and correlate with mortality and functional outcome. Proteins S100B and neuron specific enolases are among the markers most studied for this purpose, however some studies are investigating glial fibrillary acidic protein, creatinine phospokinase, isoenzime B, myelin basic protein, plasma desoxiribonucleic acid, heat shock protein 70, von Willebrand factor, metalloproteinases and brain-derived neurotrophic factor, among others. Evidence suggests that inflammation, oxidative stress, excitotoxicity, neuroendocrine responses and apoptosis play an important role in the development of secondary lesions. Markers involved in these processes are being studied in traumatic brain injury. We reviewed these biomarkers, some of which present promising results for future clinical application.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):339-343
DOI 10.1590/S0103-507X2008000400004
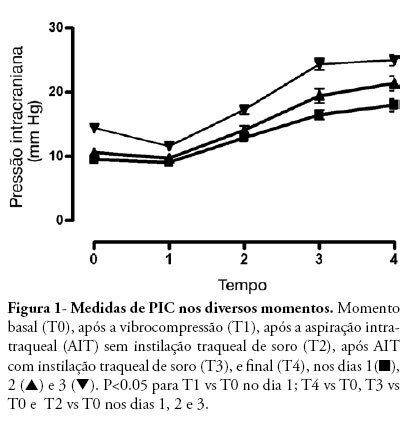
OBJECTIVE: After brain injury intracranial hypertension is the major cause of mortality, in addition to the possibility of functional, behavioral and cognitive sequels. Scarcity of studies on the effects of respiratory physiotherapy on these patients may lead to contradictory performances. This study aimed to assess the effects of customary respiratory physiotherapy maneuvers on intracranial and cerebral perfusion pressures in patients with severe brain injury. METHODS: Clinical, prospective trial with patients with severe traumatic brain injury, mechanically ventilated and with a continued measurement of intracranial pressure. The effects of manual vibrocompression maneuvers and intratracheal aspiration with or without saline infusion on the measurements of intracranial and cerebral perfusion pressures, between the first and third day after cerebral injury were evaluated. RESULTS: Data were collected from 11 patients, 41 years of age (median) and APACHE II of 19.5 ± 5. The manual vibrocompression maneuver did not cause an increase of intracranial pressure on any of the days assessed. Intracranial pressure significantly increased after intratracheal aspiration maneuvers in relation to the basal measurement (day1, 9.5 ± 0.9 mm Hg vs 18.0 ± 3.2 mm Hg; day 2, 10.6 ± 1.7 mm Hg vs 21.4 ± 3.8 mm Hg; day 3, 14.4 ± 1.0 vs 24.9 ± 2.7 mm Hg; p<0.05 for all). However, these elevations were transient (about 27 seconds) and accompanied by compensatory increases of the cerebral perfusion pressure. CONCLUSION: The manual vibrocompression maneuver did not increase intracranial pressure or cerebral perfusion pressure in patients with severe brain injury. Intratracheal aspiration induced a significant and transient increase of the intracranial and cerebral perfusion pressures.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):339-343
DOI 10.1590/S0103-507X2008000400004
OBJECTIVE: After brain injury intracranial hypertension is the major cause of mortality, in addition to the possibility of functional, behavioral and cognitive sequels. Scarcity of studies on the effects of respiratory physiotherapy on these patients may lead to contradictory performances. This study aimed to assess the effects of customary respiratory physiotherapy maneuvers on intracranial and cerebral perfusion pressures in patients with severe brain injury. METHODS: Clinical, prospective trial with patients with severe traumatic brain injury, mechanically ventilated and with a continued measurement of intracranial pressure. The effects of manual vibrocompression maneuvers and intratracheal aspiration with or without saline infusion on the measurements of intracranial and cerebral perfusion pressures, between the first and third day after cerebral injury were evaluated. RESULTS: Data were collected from 11 patients, 41 years of age (median) and APACHE II of 19.5 ± 5. The manual vibrocompression maneuver did not cause an increase of intracranial pressure on any of the days assessed. Intracranial pressure significantly increased after intratracheal aspiration maneuvers in relation to the basal measurement (day1, 9.5 ± 0.9 mm Hg vs 18.0 ± 3.2 mm Hg; day 2, 10.6 ± 1.7 mm Hg vs 21.4 ± 3.8 mm Hg; day 3, 14.4 ± 1.0 vs 24.9 ± 2.7 mm Hg; p<0.05 for all). However, these elevations were transient (about 27 seconds) and accompanied by compensatory increases of the cerebral perfusion pressure. CONCLUSION: The manual vibrocompression maneuver did not increase intracranial pressure or cerebral perfusion pressure in patients with severe brain injury. Intratracheal aspiration induced a significant and transient increase of the intracranial and cerebral perfusion pressures.