
You searched for:"Péricles Almeida Delfino Duarte"
We found (7) results for your search.-
Original Article
Functional independence and spirometry in adult post-intensive care unit patients
- Lilian Regina Lengler Abentroth
 ,
, - Erica Fernanda Osaku,
- Mayara Manzoni Marques da Silva,
- Jaiane Luiza Jaskowiak,
- Renata de Souza Zaponi, [ … ],
- Péricles Almeida Delfino Duarte
Abstract
Original ArticleFunctional independence and spirometry in adult post-intensive care unit patients
Rev Bras Ter Intensiva. 2021;33(2):243-250
DOI 10.5935/0103-507X.20210031
- Lilian Regina Lengler Abentroth ,
- Erica Fernanda Osaku,
- Mayara Manzoni Marques da Silva,
- Jaiane Luiza Jaskowiak,
- Renata de Souza Zaponi,
- Suely Mariko Ogasawara,
- Marcela Aparecida Leite,
- Cláudia Rejane Lima de Macedo Costa,
- Itamar Regazzo Pedreschi Porto,
- Amaury Cezar Jorge,
- Péricles Almeida Delfino Duarte
Views0ABSTRACT
Objective:
To relate functional independence to the degree of pulmonary impairment in adult patients 3 months after discharge from the intensive care unit.
Methods:
This was a retrospective cohort study conducted in one adult intensive care unit and a multi-professional post-intensive care unit outpatient clinic of a single center. Patients admitted to the intensive care unit from January 2012 to December 2013 who underwent (3 months later) spirometry and answered the Functional Independence Measure Questionnaire were included.
Results:
Patients were divided into groups according to the classification of functional independence and spirometry. The study included 197 patients who were divided into greater dependence (n = 4), lower dependence (n = 12) and independent (n = 181) groups. Comparing the three groups, regarding the classification of the Functional Independence Measure, patients with greater dependence had higher Acute Physiology and Chronic Health Evaluation II and Sequential Organ Failure Assessment values at intensive care unit admission with more advanced age, more days on mechanical ventilation, and longer stay in the intensive care unit and hospital. The majority of patients presented with pulmonary impairment, which was the obstructive pattern observed most frequently. When comparing functional independence with pulmonary function, it was observed that the lower the functional status, the worse the pulmonary function, with a significant difference being observed in peak expiratory flow (p = 0.030).
Conclusion:
The majority of patients who returned to the outpatient clinic 3 months after discharge had good functional status but did present with pulmonary impairment, which is related to the degree of functional dependence.
Keywords:Ambulatory care facilities, hospitalCritical careIntensive care unitsMobility limitationPeak expiratory flow rateRespiration, artificialSpirometrySee moreViews0

Abstract
Original ArticleFunctional independence and spirometry in adult post-intensive care unit patients
Rev Bras Ter Intensiva. 2021;33(2):243-250
DOI 10.5935/0103-507X.20210031
- Lilian Regina Lengler Abentroth ,
- Erica Fernanda Osaku,
- Mayara Manzoni Marques da Silva,
- Jaiane Luiza Jaskowiak,
- Renata de Souza Zaponi,
- Suely Mariko Ogasawara,
- Marcela Aparecida Leite,
- Cláudia Rejane Lima de Macedo Costa,
- Itamar Regazzo Pedreschi Porto,
- Amaury Cezar Jorge,
- Péricles Almeida Delfino Duarte
Views0ABSTRACT
Objective:
To relate functional independence to the degree of pulmonary impairment in adult patients 3 months after discharge from the intensive care unit.
Methods:
This was a retrospective cohort study conducted in one adult intensive care unit and a multi-professional post-intensive care unit outpatient clinic of a single center. Patients admitted to the intensive care unit from January 2012 to December 2013 who underwent (3 months later) spirometry and answered the Functional Independence Measure Questionnaire were included.
Results:
Patients were divided into groups according to the classification of functional independence and spirometry. The study included 197 patients who were divided into greater dependence (n = 4), lower dependence (n = 12) and independent (n = 181) groups. Comparing the three groups, regarding the classification of the Functional Independence Measure, patients with greater dependence had higher Acute Physiology and Chronic Health Evaluation II and Sequential Organ Failure Assessment values at intensive care unit admission with more advanced age, more days on mechanical ventilation, and longer stay in the intensive care unit and hospital. The majority of patients presented with pulmonary impairment, which was the obstructive pattern observed most frequently. When comparing functional independence with pulmonary function, it was observed that the lower the functional status, the worse the pulmonary function, with a significant difference being observed in peak expiratory flow (p = 0.030).
Conclusion:
The majority of patients who returned to the outpatient clinic 3 months after discharge had good functional status but did present with pulmonary impairment, which is related to the degree of functional dependence.
Keywords:Ambulatory care facilities, hospitalCritical careIntensive care unitsMobility limitationPeak expiratory flow rateRespiration, artificialSpirometrySee more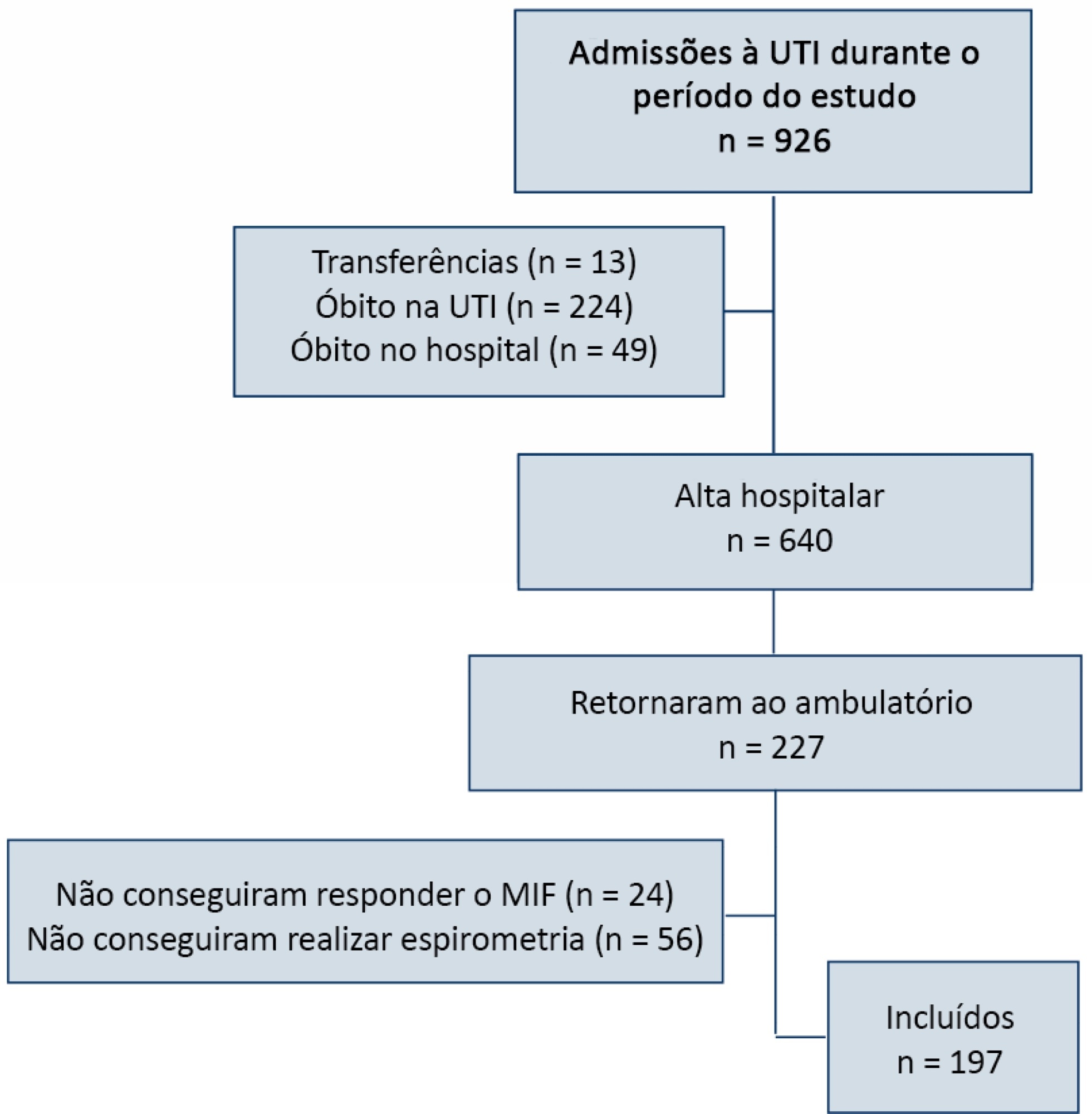
- Lilian Regina Lengler Abentroth
-
Original Article
Sedation and memories of patients subjected to mechanical ventilation in an intensive care unit
Rev Bras Ter Intensiva. 2014;26(2):122-129
Abstract
Original ArticleSedation and memories of patients subjected to mechanical ventilation in an intensive care unit
Rev Bras Ter Intensiva. 2014;26(2):122-129
DOI 10.5935/0103-507X.20140018
Views0See moreObjective:
To investigate the relationship between sedation and the memories reported by patients subjected to mechanical ventilation following discharge from the intensive care unit.
Methods:
This prospective, observational, cohort study was conducted with individuals subjected to mechanical ventilation who remained in the intensive care unit for more than 24 hours. Clinical statistics and sedation records were extracted from the participants’ clinical records; the data relative to the participants’ memories were collected using a specific validated instrument. Assessment was performed three months after discharge from the intensive care unit.
Results:
A total of 128 individuals were assessed, most of whom (84.4%) reported recollections from their stay in the intensive care unit as predominantly a combination of real and illusory events. The participants subjected to sedation (67.2%) at deep levels (Richmond Agitation-Sedation Scale [RASS] -4 and -5) for more than two days and those with psychomotor agitation (33.6%) exhibited greater susceptibility to occurrence of illusory memories (p>0.001).
Conclusion:
The probability of the occurrence of illusory memories was greater among the participants who were subjected to deep sedation. Sedation seems to be an additional factor that contributed to the occurrence of illusory memories in severely ill individuals subjected to mechanical ventilation.
Views0Abstract
Original ArticleSedation and memories of patients subjected to mechanical ventilation in an intensive care unit
Rev Bras Ter Intensiva. 2014;26(2):122-129
DOI 10.5935/0103-507X.20140018
Views0See moreObjective:
To investigate the relationship between sedation and the memories reported by patients subjected to mechanical ventilation following discharge from the intensive care unit.
Methods:
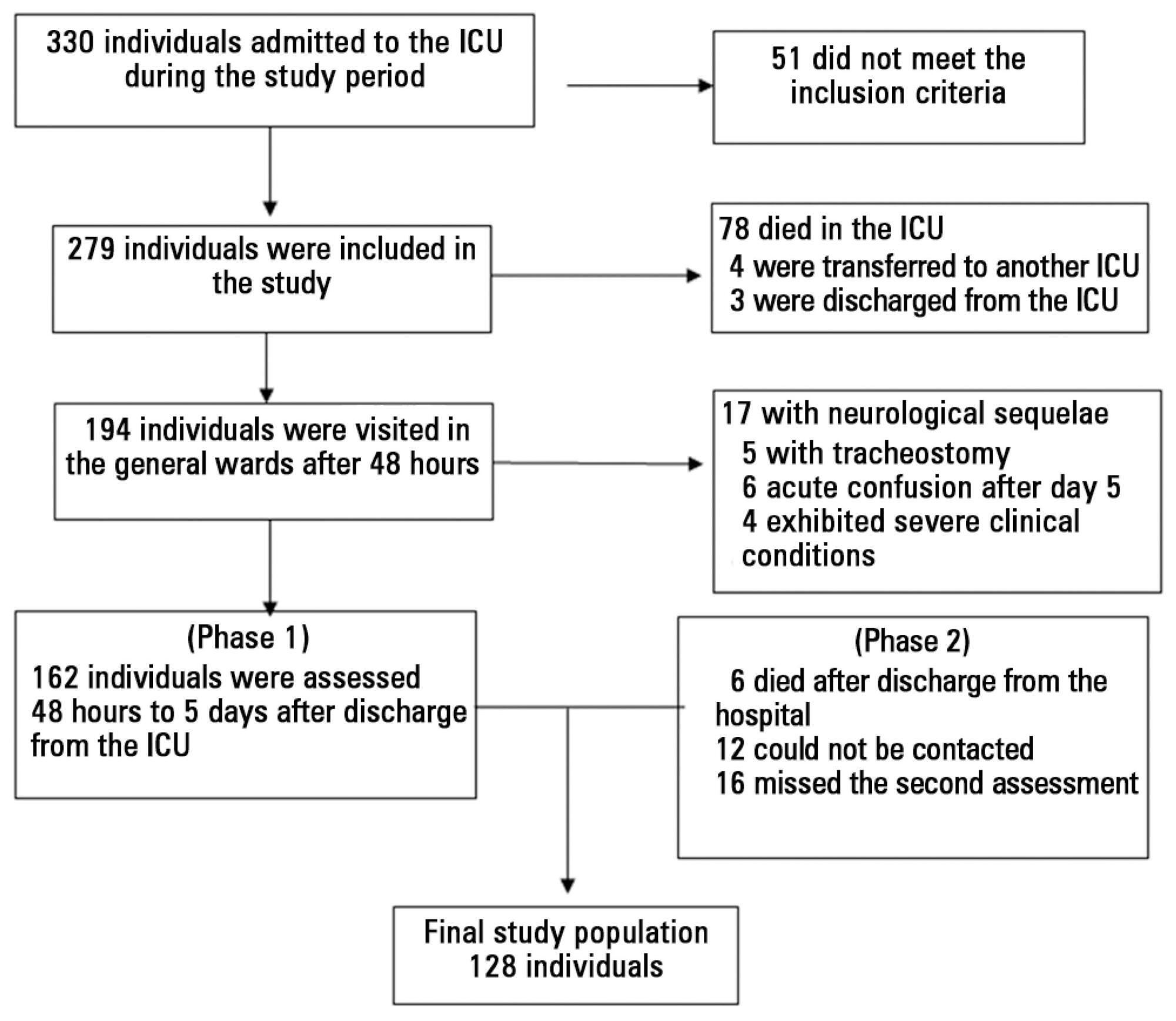
This prospective, observational, cohort study was conducted with individuals subjected to mechanical ventilation who remained in the intensive care unit for more than 24 hours. Clinical statistics and sedation records were extracted from the participants’ clinical records; the data relative to the participants’ memories were collected using a specific validated instrument. Assessment was performed three months after discharge from the intensive care unit.
Results:
A total of 128 individuals were assessed, most of whom (84.4%) reported recollections from their stay in the intensive care unit as predominantly a combination of real and illusory events. The participants subjected to sedation (67.2%) at deep levels (Richmond Agitation-Sedation Scale [RASS] -4 and -5) for more than two days and those with psychomotor agitation (33.6%) exhibited greater susceptibility to occurrence of illusory memories (p>0.001).
Conclusion:
The probability of the occurrence of illusory memories was greater among the participants who were subjected to deep sedation. Sedation seems to be an additional factor that contributed to the occurrence of illusory memories in severely ill individuals subjected to mechanical ventilation.
-
Special Article
Brazilian recommendations of mechanical ventilation 2013. Part 2
Rev Bras Ter Intensiva. 2014;26(3):215-239
Abstract
Special ArticleBrazilian recommendations of mechanical ventilation 2013. Part 2
Rev Bras Ter Intensiva. 2014;26(3):215-239
DOI 10.5935/0103-507X.20140034
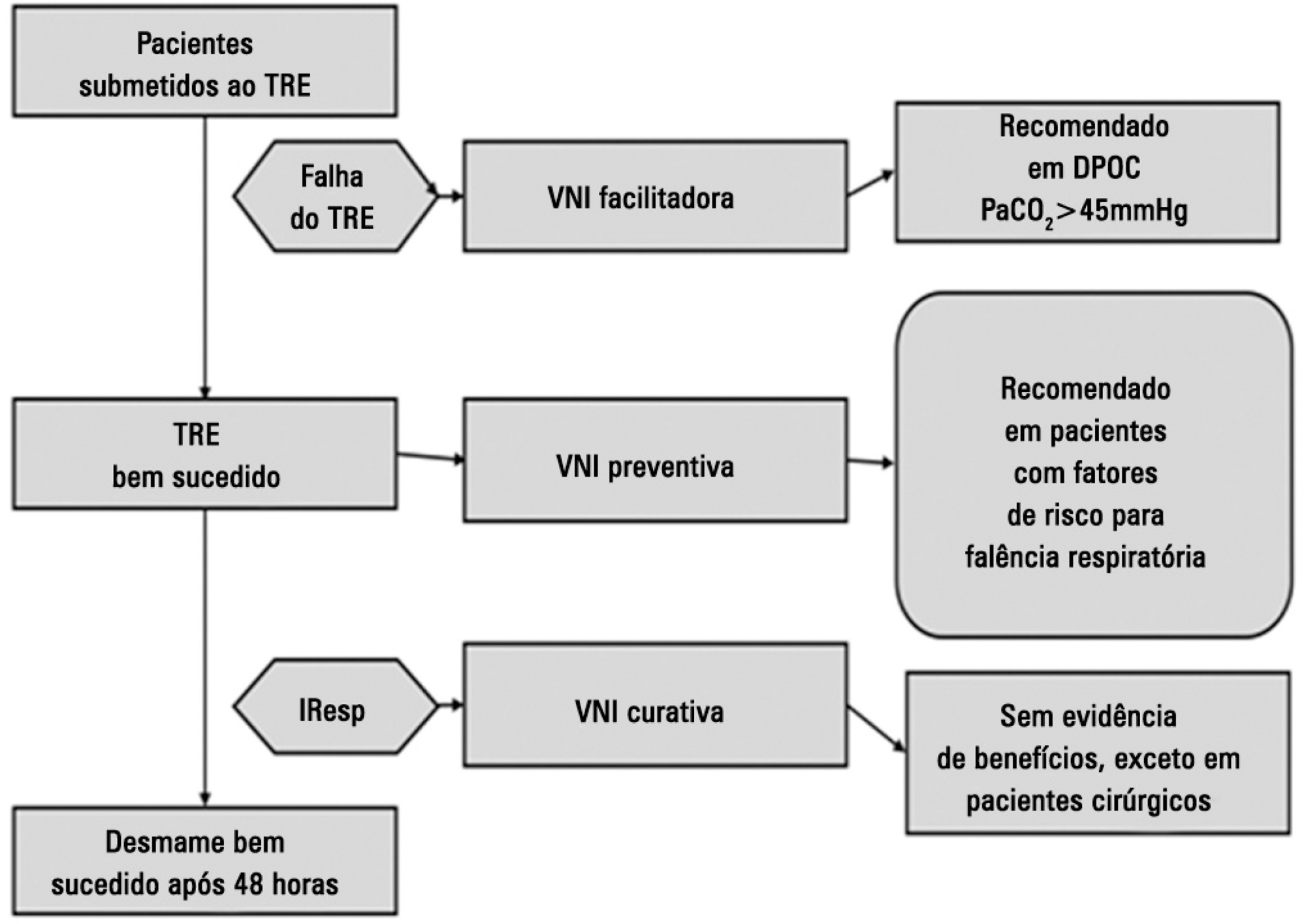
Views1See morePerspectives on invasive and noninvasive ventilatory support for critically ill patients are evolving, as much evidence indicates that ventilation may have positive effects on patient survival and the quality of the care provided in intensive care units in Brazil. For those reasons, the Brazilian Association of Intensive Care Medicine (Associação de Medicina Intensiva Brasileira – AMIB) and the Brazilian Thoracic Society (Sociedade Brasileira de Pneumologia e Tisiologia – SBPT), represented by the Mechanical Ventilation Committee and the Commission of Intensive Therapy, respectively, decided to review the literature and draft recommendations for mechanical ventilation with the goal of creating a document for bedside guidance as to the best practices on mechanical ventilation available to their members. The document was based on the available evidence regarding 29 subtopics selected as the most relevant for the subject of interest. The project was developed in several stages, during which the selected topics were distributed among experts recommended by both societies with recent publications on the subject of interest and/or significant teaching and research activity in the field of mechanical ventilation in Brazil. The experts were divided into pairs that were charged with performing a thorough review of the international literature on each topic. All the experts met at the Forum on Mechanical Ventilation, which was held at the headquarters of AMIB in São Paulo on August 3 and 4, 2013, to collaboratively draft the final text corresponding to each sub-topic, which was presented to, appraised, discussed and approved in a plenary session that included all 58 participants and aimed to create the final document.
Views1Abstract
Special ArticleBrazilian recommendations of mechanical ventilation 2013. Part 2
Rev Bras Ter Intensiva. 2014;26(3):215-239
DOI 10.5935/0103-507X.20140034
Views1See morePerspectives on invasive and noninvasive ventilatory support for critically ill patients are evolving, as much evidence indicates that ventilation may have positive effects on patient survival and the quality of the care provided in intensive care units in Brazil. For those reasons, the Brazilian Association of Intensive Care Medicine (Associação de Medicina Intensiva Brasileira – AMIB) and the Brazilian Thoracic Society (Sociedade Brasileira de Pneumologia e Tisiologia – SBPT), represented by the Mechanical Ventilation Committee and the Commission of Intensive Therapy, respectively, decided to review the literature and draft recommendations for mechanical ventilation with the goal of creating a document for bedside guidance as to the best practices on mechanical ventilation available to their members. The document was based on the available evidence regarding 29 subtopics selected as the most relevant for the subject of interest. The project was developed in several stages, during which the selected topics were distributed among experts recommended by both societies with recent publications on the subject of interest and/or significant teaching and research activity in the field of mechanical ventilation in Brazil. The experts were divided into pairs that were charged with performing a thorough review of the international literature on each topic. All the experts met at the Forum on Mechanical Ventilation, which was held at the headquarters of AMIB in São Paulo on August 3 and 4, 2013, to collaboratively draft the final text corresponding to each sub-topic, which was presented to, appraised, discussed and approved in a plenary session that included all 58 participants and aimed to create the final document.
-
Original Article
The knowledge of intensive care professionals about diarrhea
Rev Bras Ter Intensiva. 2014;26(3):299-304
Abstract
Original ArticleThe knowledge of intensive care professionals about diarrhea
Rev Bras Ter Intensiva. 2014;26(3):299-304
DOI 10.5935/0103-507X.20140042
Views0See moreObjective:
To assess the opinions and practices of intensive care professionals with regard to diarrhea in critically ill patients.
Methods:
A multicenter cross-sectional study was conducted among health care professionals working at three adult intensive care units. Participants responded individually to a self-administered questionnaire about their length of work experience in intensive care; the definition, characterization, and causes of diarrhea; types of records in the patient’s medical record; and training received.
Results:
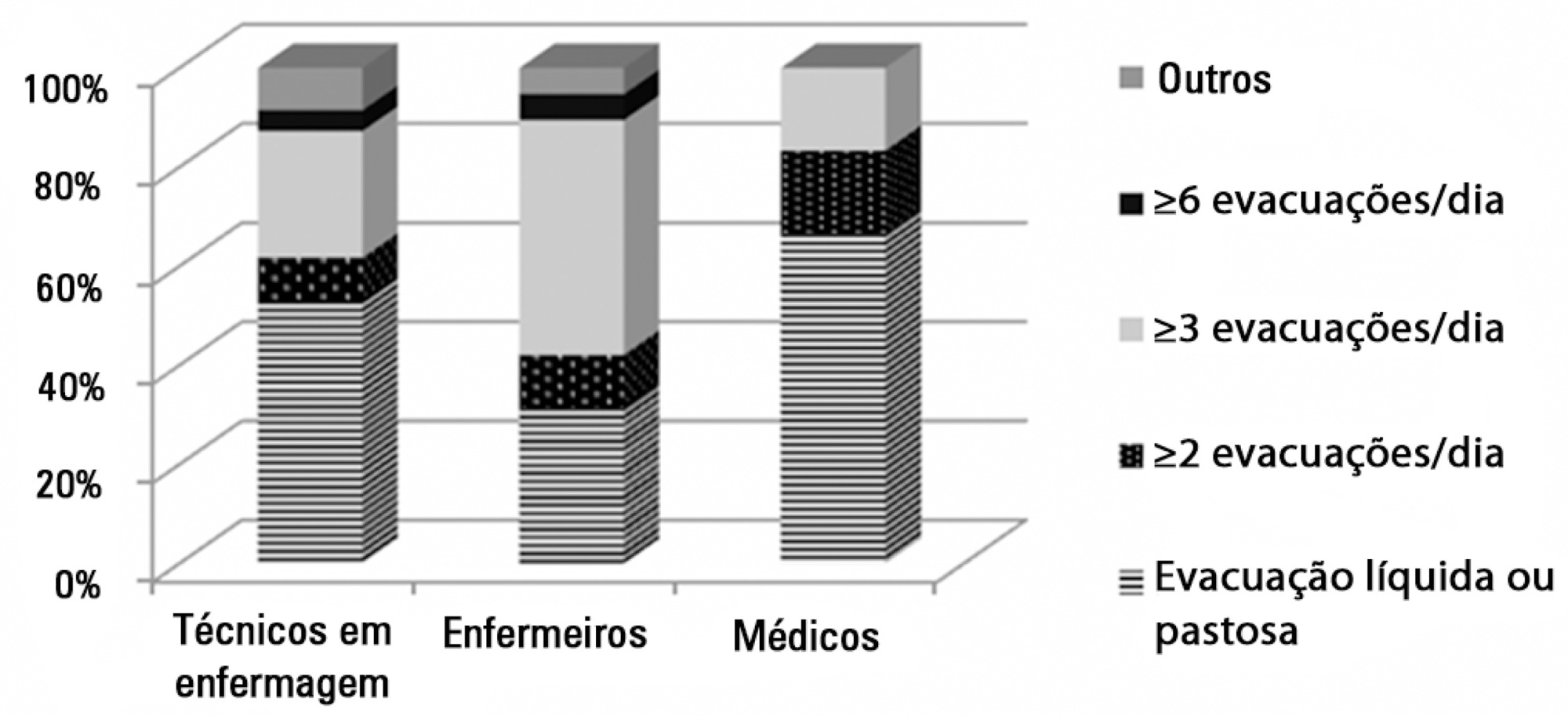
A total of 78 professionals participated in this study, of whom 59.0% were nurse technicians, 25.7% were nurses, and 15.3% were physicians; 77.0% of them had worked in intensive care for over 1 year. Only 37.2% had received training on this topic. Half of the interviewees defined diarrhea as “liquid and/or pasty stools” regardless of frequency, while the other 50.0% defined diarrhea based on the increased number of daily bowel movements. The majority of them mentioned diet as the main cause of diarrhea, followed by “use of medications” (p<0.001). Distinct nutritional practices were observed among the analyzed professionals regarding episodes of diarrhea, such as discontinuing, maintaining, or reducing the volume of enteral nutrition; physicians reported that they do not routinely communicate the problem to other professionals (for example, to a nutritionist) and do not routinely record and quantify diarrhea events in patients' medical records.
Conclusion:
Different opinions and practices were observed in intensive care professionals with regard to diarrhea.
Views0Abstract
Original ArticleThe knowledge of intensive care professionals about diarrhea
Rev Bras Ter Intensiva. 2014;26(3):299-304
DOI 10.5935/0103-507X.20140042
Views0See moreObjective:
To assess the opinions and practices of intensive care professionals with regard to diarrhea in critically ill patients.
Methods:
A multicenter cross-sectional study was conducted among health care professionals working at three adult intensive care units. Participants responded individually to a self-administered questionnaire about their length of work experience in intensive care; the definition, characterization, and causes of diarrhea; types of records in the patient’s medical record; and training received.
Results:
A total of 78 professionals participated in this study, of whom 59.0% were nurse technicians, 25.7% were nurses, and 15.3% were physicians; 77.0% of them had worked in intensive care for over 1 year. Only 37.2% had received training on this topic. Half of the interviewees defined diarrhea as “liquid and/or pasty stools” regardless of frequency, while the other 50.0% defined diarrhea based on the increased number of daily bowel movements. The majority of them mentioned diet as the main cause of diarrhea, followed by “use of medications” (p<0.001). Distinct nutritional practices were observed among the analyzed professionals regarding episodes of diarrhea, such as discontinuing, maintaining, or reducing the volume of enteral nutrition; physicians reported that they do not routinely communicate the problem to other professionals (for example, to a nutritionist) and do not routinely record and quantify diarrhea events in patients' medical records.
Conclusion:
Different opinions and practices were observed in intensive care professionals with regard to diarrhea.
-
Special Article
Brazilian recommendations of mechanical ventilation 2013. Part I
Rev Bras Ter Intensiva. 2014;26(2):89-121
Abstract
Special ArticleBrazilian recommendations of mechanical ventilation 2013. Part I
Rev Bras Ter Intensiva. 2014;26(2):89-121
DOI 10.5935/0103-507X.20140017
Views5See morePerspectives on invasive and noninvasive ventilatory support for critically ill patients are evolving, as much evidence indicates that ventilation may have positive effects on patient survival and the quality of the care provided in intensive care units in Brazil. For those reasons, the Brazilian Association of Intensive Care Medicine (Associação de Medicina Intensiva Brasileira – AMIB) and the Brazilian Thoracic Society (Sociedade Brasileira de Pneumologia e Tisiologia – SBPT), represented by the Mechanical Ventilation Committee and the Commission of Intensive Therapy, respectively, decided to review the literature and draft recommendations for mechanical ventilation with the goal of creating a document for bedside guidance as to the best practices on mechanical ventilation available to their members. The document was based on the available evidence regarding 29 subtopics selected as the most relevant for the subject of interest. The project was developed in several stages, during which the selected topics were distributed among experts recommended by both societies with recent publications on the subject of interest and/or significant teaching and research activity in the field of mechanical ventilation in Brazil. The experts were divided into pairs that were charged with performing a thorough review of the international literature on each topic. All the experts met at the Forum on Mechanical Ventilation, which was held at the headquarters of AMIB in São Paulo on August 3 and 4, 2013, to collaboratively draft the final text corresponding to each sub-topic, which was presented to, appraised, discussed and approved in a plenary session that included all 58 participants and aimed to create the final document.
Views5Abstract
Special ArticleBrazilian recommendations of mechanical ventilation 2013. Part I
Rev Bras Ter Intensiva. 2014;26(2):89-121
DOI 10.5935/0103-507X.20140017
Views5See morePerspectives on invasive and noninvasive ventilatory support for critically ill patients are evolving, as much evidence indicates that ventilation may have positive effects on patient survival and the quality of the care provided in intensive care units in Brazil. For those reasons, the Brazilian Association of Intensive Care Medicine (Associação de Medicina Intensiva Brasileira – AMIB) and the Brazilian Thoracic Society (Sociedade Brasileira de Pneumologia e Tisiologia – SBPT), represented by the Mechanical Ventilation Committee and the Commission of Intensive Therapy, respectively, decided to review the literature and draft recommendations for mechanical ventilation with the goal of creating a document for bedside guidance as to the best practices on mechanical ventilation available to their members. The document was based on the available evidence regarding 29 subtopics selected as the most relevant for the subject of interest. The project was developed in several stages, during which the selected topics were distributed among experts recommended by both societies with recent publications on the subject of interest and/or significant teaching and research activity in the field of mechanical ventilation in Brazil. The experts were divided into pairs that were charged with performing a thorough review of the international literature on each topic. All the experts met at the Forum on Mechanical Ventilation, which was held at the headquarters of AMIB in São Paulo on August 3 and 4, 2013, to collaboratively draft the final text corresponding to each sub-topic, which was presented to, appraised, discussed and approved in a plenary session that included all 58 participants and aimed to create the final document.
-
Outcome of influenza A (H1N1) patients admitted to intensive care units in the Paraná state, Brazil
Rev Bras Ter Intensiva. 2009;21(3):231-236
Abstract
Outcome of influenza A (H1N1) patients admitted to intensive care units in the Paraná state, Brazil
Rev Bras Ter Intensiva. 2009;21(3):231-236
DOI 10.1590/S0103-507X2009000300001
Views3See moreOBJECTIVE: This study aimed to analyze outcome, clinical and epidemiological characteristics and severity factors in adult patients admitted with a diagnosis of infection by virus A (H1N1) to public and private intensive care units, in Paraná, Brazil. METHODS: Cohort study of medical charts of patients older than 12 years admitted to 11 intensive care units in 6 cities in the state of Parana, Brazil, during a period of 45 days, with diagnosis of swine influenza. The diagnosis of infection with A (H1N1) was made by real time polymerase chain reaction (RT-PCR) of nasopharyngeal secretion, or strong clinical suspicion when other causes had been ruled out (even with negative RT-PCR). Descriptive statistics were performed, analysis by the Chi square test was used to compare percentages and the Student’s t test for continuous variables with univariate analysis, assuming a significance level of p <0.05. RESULTS: There were 63 adult patients admitted with a diagnosis of H1N1, 37 (58.7%) being RT-PCR positive. Most patients were young adults (65% under 40 years of age) with no gender predominance and high incidence of obesity (27.0% with Body Mass Index > 30). Mean of the Acute Physiologic Chronic Health Evaluation II (APACHE II) score was 15.0 + 8.1. Mortality in the intensive care unit was 39.7%. The main factors associated with mortality were: positive RT-PCR, low levels of initial PaO2/FiO2, high initial levels of urea and lactate dehydrogenase, required level of positive end expiratory pressure, need for the prone position and vasopressors. CONCLUSIONS: Adult patients with A (H1N1) virus infection admitted to intensive care units had a high risk of death, particularly due to respiratory impairment. Positive RT-PCR, urea and lactic dehydrogenase, low initial PaO2/FiO2 and high levels of PEEP were correlated with higher mortality.
Views3Abstract
Outcome of influenza A (H1N1) patients admitted to intensive care units in the Paraná state, Brazil
Rev Bras Ter Intensiva. 2009;21(3):231-236
DOI 10.1590/S0103-507X2009000300001
Views3See moreOBJECTIVE: This study aimed to analyze outcome, clinical and epidemiological characteristics and severity factors in adult patients admitted with a diagnosis of infection by virus A (H1N1) to public and private intensive care units, in Paraná, Brazil. METHODS: Cohort study of medical charts of patients older than 12 years admitted to 11 intensive care units in 6 cities in the state of Parana, Brazil, during a period of 45 days, with diagnosis of swine influenza. The diagnosis of infection with A (H1N1) was made by real time polymerase chain reaction (RT-PCR) of nasopharyngeal secretion, or strong clinical suspicion when other causes had been ruled out (even with negative RT-PCR). Descriptive statistics were performed, analysis by the Chi square test was used to compare percentages and the Student’s t test for continuous variables with univariate analysis, assuming a significance level of p <0.05. RESULTS: There were 63 adult patients admitted with a diagnosis of H1N1, 37 (58.7%) being RT-PCR positive. Most patients were young adults (65% under 40 years of age) with no gender predominance and high incidence of obesity (27.0% with Body Mass Index > 30). Mean of the Acute Physiologic Chronic Health Evaluation II (APACHE II) score was 15.0 + 8.1. Mortality in the intensive care unit was 39.7%. The main factors associated with mortality were: positive RT-PCR, low levels of initial PaO2/FiO2, high initial levels of urea and lactate dehydrogenase, required level of positive end expiratory pressure, need for the prone position and vasopressors. CONCLUSIONS: Adult patients with A (H1N1) virus infection admitted to intensive care units had a high risk of death, particularly due to respiratory impairment. Positive RT-PCR, urea and lactic dehydrogenase, low initial PaO2/FiO2 and high levels of PEEP were correlated with higher mortality.
-
Original Articles
Epidemiology and outcomes of non-cardiac surgical patients in Brazilian intensive care units
Rev Bras Ter Intensiva. 2008;20(4):376-384
Abstract
Original ArticlesEpidemiology and outcomes of non-cardiac surgical patients in Brazilian intensive care units
Rev Bras Ter Intensiva. 2008;20(4):376-384
DOI 10.1590/S0103-507X2008000400010
Views0See moreOBJECTIVES: Due to the dramatic medical breakthroughs and an increasingly ageing population, the proportion of patients who are at risk of dying following surgery is increasing over time. The aim of this study was to evaluate the outcomes and the epidemiology of non-cardiac surgical patients admitted to the intensive care unit. METHODS: A multicenter, prospective, observational, cohort study was carried out in 21 intensive care units. A total of 885 adult surgical patients admitted to a participating intensive care unit from April to June 2006 were evaluated and 587 patients were enrolled. Exclusion criteria were trauma, cardiac, neurological, gynecologic, obstetric and palliative surgeries. The main outcome measures were postoperative complications and intensive care unit and 90-day mortality rates. RESULTS: Major and urgent surgeries were performed in 66.4% and 31.7% of the patients, respectively. The intensive care unit mortality rate was 15%, and 38% of the patients had postoperative complications. The most common complication was infection or sepsis (24.7%). Myocardial ischemia was diagnosed in only 1.9% of the patients. A total of 94 % of the patients who died after surgery had co-morbidities at the time of surgery (3.4 ± 2.2). Multiple organ failure was the main cause of death (53%). CONCLUSION: Sepsis is the predominant cause of morbidity in patients undergoing non-cardiac surgery. In this patient population, multiple organ failure prevailed as the most frequent cause of death in the hospital.
Views0Abstract
Original ArticlesEpidemiology and outcomes of non-cardiac surgical patients in Brazilian intensive care units
Rev Bras Ter Intensiva. 2008;20(4):376-384
DOI 10.1590/S0103-507X2008000400010
Views0See moreOBJECTIVES: Due to the dramatic medical breakthroughs and an increasingly ageing population, the proportion of patients who are at risk of dying following surgery is increasing over time. The aim of this study was to evaluate the outcomes and the epidemiology of non-cardiac surgical patients admitted to the intensive care unit. METHODS: A multicenter, prospective, observational, cohort study was carried out in 21 intensive care units. A total of 885 adult surgical patients admitted to a participating intensive care unit from April to June 2006 were evaluated and 587 patients were enrolled. Exclusion criteria were trauma, cardiac, neurological, gynecologic, obstetric and palliative surgeries. The main outcome measures were postoperative complications and intensive care unit and 90-day mortality rates. RESULTS: Major and urgent surgeries were performed in 66.4% and 31.7% of the patients, respectively. The intensive care unit mortality rate was 15%, and 38% of the patients had postoperative complications. The most common complication was infection or sepsis (24.7%). Myocardial ischemia was diagnosed in only 1.9% of the patients. A total of 94 % of the patients who died after surgery had co-morbidities at the time of surgery (3.4 ± 2.2). Multiple organ failure was the main cause of death (53%). CONCLUSION: Sepsis is the predominant cause of morbidity in patients undergoing non-cardiac surgery. In this patient population, multiple organ failure prevailed as the most frequent cause of death in the hospital.
Search
Search in:
KEY WORDS
Case reports Child Coronavirus infections COVID-19 Critical care Critical illness ICU Infant, newborn Intensive care Intensive care units Intensive care units, pediatric mechanical ventilation Mortality Physical therapy modalities Prognosis Respiration, artificial Respiratory insufficiency risk factors SARS-CoV-2 Sepsis