brain death Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2021;33(4):557-564
DOI 10.5935/0103-507X.20210072
To describe health care providers’ knowledge about lung donation and donor lung management.
A descriptive, cross-sectional study based on an anonymous survey was conducted between March and September 2018 among health care professionals registered to Sociedad Argentina de Terapia Intensiva.
Of the 736 respondents, the mean age was 40.5 years (standard deviation 8.9), and 61.3% were female. Sixty percent were physicians, 21.5% were nurses, and 17.9% were physiotherapists. Seventy-eight percent considered themselves appropriately informed about organ procurement, and 79.8% stated that they knew potential organ donor critical care management. The lung donor criteria were answered correctly by 71.3% of the respondents. However, after the donor’s brain death, 51% made no changes to ventilator parameters, 22.9% were not aware of which parameters to reprogram, and 44.5% selected tidal volume of 6 - 8mL/kg and positive end expiratory pressure of 5cmH2O. For 85% of the health care providers, the type of apnea test chosen was disconnection from the ventilator, and only 18.5% used a lung management protocol. The most frequent interventions used in the case of arterial oxygen partial pressure/fractional inspired oxygen < 300 were positive end expiratory pressure titration, closed-circuit endotracheal suctioning, and recruitment maneuvers.
Health care professionals surveyed in Argentina correctly answered most of the questions related to lung donor criteria. However, they lacked detailed knowledge about ventilatory settings, ventilatory strategies, and protocols for lung donors. Educational programs are key to optimizing multiorgan donation and should be focused on protecting the donor lungs to increase the numbers of organs available for transplantation.
Abstract
Rev Bras Ter Intensiva. 2021;33(4):557-564
DOI 10.5935/0103-507X.20210072
To describe health care providers’ knowledge about lung donation and donor lung management.
A descriptive, cross-sectional study based on an anonymous survey was conducted between March and September 2018 among health care professionals registered to Sociedad Argentina de Terapia Intensiva.
Of the 736 respondents, the mean age was 40.5 years (standard deviation 8.9), and 61.3% were female. Sixty percent were physicians, 21.5% were nurses, and 17.9% were physiotherapists. Seventy-eight percent considered themselves appropriately informed about organ procurement, and 79.8% stated that they knew potential organ donor critical care management. The lung donor criteria were answered correctly by 71.3% of the respondents. However, after the donor’s brain death, 51% made no changes to ventilator parameters, 22.9% were not aware of which parameters to reprogram, and 44.5% selected tidal volume of 6 - 8mL/kg and positive end expiratory pressure of 5cmH2O. For 85% of the health care providers, the type of apnea test chosen was disconnection from the ventilator, and only 18.5% used a lung management protocol. The most frequent interventions used in the case of arterial oxygen partial pressure/fractional inspired oxygen < 300 were positive end expiratory pressure titration, closed-circuit endotracheal suctioning, and recruitment maneuvers.
Health care professionals surveyed in Argentina correctly answered most of the questions related to lung donor criteria. However, they lacked detailed knowledge about ventilatory settings, ventilatory strategies, and protocols for lung donors. Educational programs are key to optimizing multiorgan donation and should be focused on protecting the donor lungs to increase the numbers of organs available for transplantation.
Abstract
Rev Bras Ter Intensiva. 2021;33(2):290-297
DOI 10.5935/0103-507X.20210037
To analyze the impact of Resolution 2.173/2017 of the Federal Council of Medicine on results from the Central Estadual de Transplantes de Santa Catarina.
This was a cross-sectional observational study of medical records of all patients (1,605) with suspected brain death notified to the Central Estadual de Transplantes de Santa Catarina; for this study, procedures to confirm this diagnosis were initiated between July 2016 and December 2017 and between January 2018 and June 2019. The median duration of the protocol in each period was considered for the comparison between the intervals. The collected data were transformed into rates (per million population). The mean rates for the periods before and after the implementation of the protocol were analyzed by Student’s t-test, and qualitative variables were analyzed by Pearson’s chi-squared test.
The mean duration of brain death confirmation procedures decreased more than 1 hour in the second period compared to the first period, with statistical significance (p = 0.001). The rates of harvested livers and transplanted pancreas, the number of notifications by hospital size and the rate of cardiac arrest in the macro-region of the Itajaí Valley were significantly different between the two periods.
In the period after the new resolution on brain death, there was a reduction in the duration for diagnosis. However, other indicators did not change significantly, providing evidence for the multidimensional nature of the organ transplantation process in Santa Catarina and the need for further studies to better understand and optimize the process.
Abstract
Rev Bras Ter Intensiva. 2021;33(2):290-297
DOI 10.5935/0103-507X.20210037
To analyze the impact of Resolution 2.173/2017 of the Federal Council of Medicine on results from the Central Estadual de Transplantes de Santa Catarina.
This was a cross-sectional observational study of medical records of all patients (1,605) with suspected brain death notified to the Central Estadual de Transplantes de Santa Catarina; for this study, procedures to confirm this diagnosis were initiated between July 2016 and December 2017 and between January 2018 and June 2019. The median duration of the protocol in each period was considered for the comparison between the intervals. The collected data were transformed into rates (per million population). The mean rates for the periods before and after the implementation of the protocol were analyzed by Student’s t-test, and qualitative variables were analyzed by Pearson’s chi-squared test.
The mean duration of brain death confirmation procedures decreased more than 1 hour in the second period compared to the first period, with statistical significance (p = 0.001). The rates of harvested livers and transplanted pancreas, the number of notifications by hospital size and the rate of cardiac arrest in the macro-region of the Itajaí Valley were significantly different between the two periods.
In the period after the new resolution on brain death, there was a reduction in the duration for diagnosis. However, other indicators did not change significantly, providing evidence for the multidimensional nature of the organ transplantation process in Santa Catarina and the need for further studies to better understand and optimize the process.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):1-11
DOI 10.5935/0103-507X.20210001
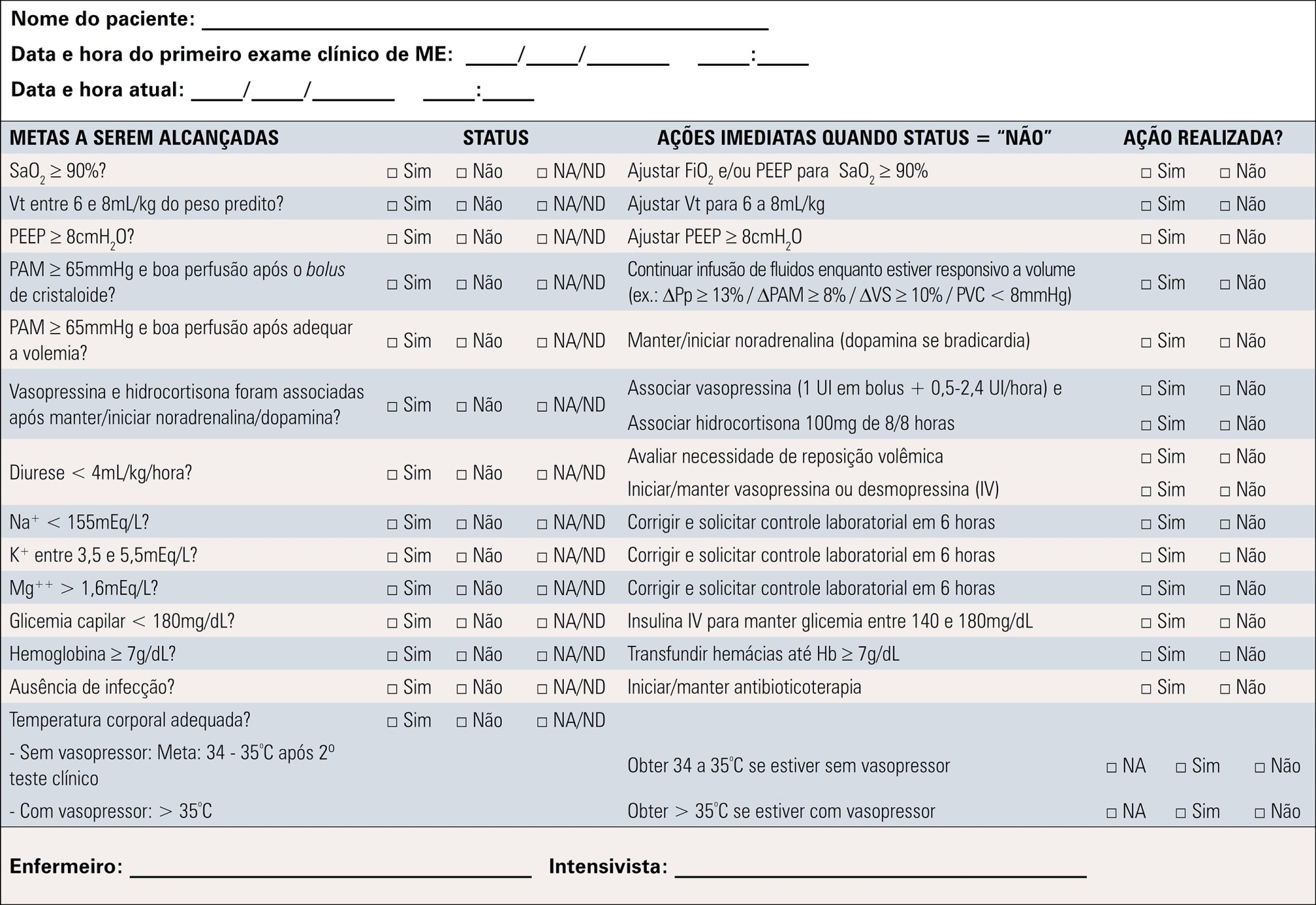
To contribute to updating the recommendations for brain-dead potential organ donor management.
A group of 27 experts, including intensivists, transplant coordinators, transplant surgeons, and epidemiologists, answered questions related to the following topics were divided into mechanical ventilation, hemodynamics, endocrine-metabolic management, infection, body temperature, blood transfusion, and checklists use. The outcomes considered were cardiac arrests, number of organs removed or transplanted as well as function / survival of transplanted organs. The quality of evidence of the recommendations was assessed using the Grading of Recommendations Assessment, Development, and Evaluation system to classify the recommendations.
A total of 19 recommendations were drawn from the expert panel. Of these, 7 were classified as strong, 11 as weak and 1 was considered a good clinical practice.
Despite the agreement among panel members on most recommendations, the grade of recommendation was mostly weak.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):1-11
DOI 10.5935/0103-507X.20210001
To contribute to updating the recommendations for brain-dead potential organ donor management.
A group of 27 experts, including intensivists, transplant coordinators, transplant surgeons, and epidemiologists, answered questions related to the following topics were divided into mechanical ventilation, hemodynamics, endocrine-metabolic management, infection, body temperature, blood transfusion, and checklists use. The outcomes considered were cardiac arrests, number of organs removed or transplanted as well as function / survival of transplanted organs. The quality of evidence of the recommendations was assessed using the Grading of Recommendations Assessment, Development, and Evaluation system to classify the recommendations.
A total of 19 recommendations were drawn from the expert panel. Of these, 7 were classified as strong, 11 as weak and 1 was considered a good clinical practice.
Despite the agreement among panel members on most recommendations, the grade of recommendation was mostly weak.
Abstract
Rev Bras Ter Intensiva. 2020;32(4):571-577
DOI 10.5935/0103-507X.20200095
To describe the results from the implementation of a respiratory care and mechanical ventilation protocol on potential lung donors who met the conditions for procurement. The secondary objective is to compare the results with historical data.
This was a retrospective, observational study. It included potential donors suitable for procurement of organs who had brain death and were hospitalized in critical care units of the Autonomous City of Buenos Aires from April 2017 to March 2018. Main variables: number of potential lung donors that reached the objective of procurement, rate of lungs procured, and rate of implanted lungs. Values of p < 0.05 were considered significant.
Thirty potential lung donors were included, and 23 (88.5%; 95%CI 69.8 - 97.6) met the oxygenation objective. Twenty potential lung donors donated organs, of whom eight donated lungs, with which four double lung transplants and eight single lung transplants were performed. Seven of 12 lungs were procured and implanted in the preprotocol period, while all 12 were under the protocol (p = 0.38). The implantation rate was 58.3% (7/12) in the historical control period and 100% (12/12) (p = 0.04) in the study period.
Abstract
Rev Bras Ter Intensiva. 2020;32(4):571-577
DOI 10.5935/0103-507X.20200095
To describe the results from the implementation of a respiratory care and mechanical ventilation protocol on potential lung donors who met the conditions for procurement. The secondary objective is to compare the results with historical data.
This was a retrospective, observational study. It included potential donors suitable for procurement of organs who had brain death and were hospitalized in critical care units of the Autonomous City of Buenos Aires from April 2017 to March 2018. Main variables: number of potential lung donors that reached the objective of procurement, rate of lungs procured, and rate of implanted lungs. Values of p < 0.05 were considered significant.
Thirty potential lung donors were included, and 23 (88.5%; 95%CI 69.8 - 97.6) met the oxygenation objective. Twenty potential lung donors donated organs, of whom eight donated lungs, with which four double lung transplants and eight single lung transplants were performed. Seven of 12 lungs were procured and implanted in the preprotocol period, while all 12 were under the protocol (p = 0.38). The implantation rate was 58.3% (7/12) in the historical control period and 100% (12/12) (p = 0.04) in the study period.

Abstract
Rev Bras Ter Intensiva. 2020;32(3):468-473
DOI 10.5935/0103-507X.20200077
Extracorporeal membrane oxygenation is used as extracirculatory support for the care of patients with severe and reversible cardiac and/or respiratory failure. Neurological complications may be related to the procedure. Given the unfavorable neurological evolution and the need to perform a brain death protocol, the performance of an apnea test in this context remains a challenge. We report the use of an apnea test for the diagnosis of brain death post-cardiac surgery in a patient receiving venoarterial extracorporeal membrane oxygenation.
Abstract
Rev Bras Ter Intensiva. 2020;32(3):468-473
DOI 10.5935/0103-507X.20200077
Extracorporeal membrane oxygenation is used as extracirculatory support for the care of patients with severe and reversible cardiac and/or respiratory failure. Neurological complications may be related to the procedure. Given the unfavorable neurological evolution and the need to perform a brain death protocol, the performance of an apnea test in this context remains a challenge. We report the use of an apnea test for the diagnosis of brain death post-cardiac surgery in a patient receiving venoarterial extracorporeal membrane oxygenation.
Abstract
Rev Bras Ter Intensiva. 2020;32(2):319-325
DOI 10.5935/0103-507X.20200032
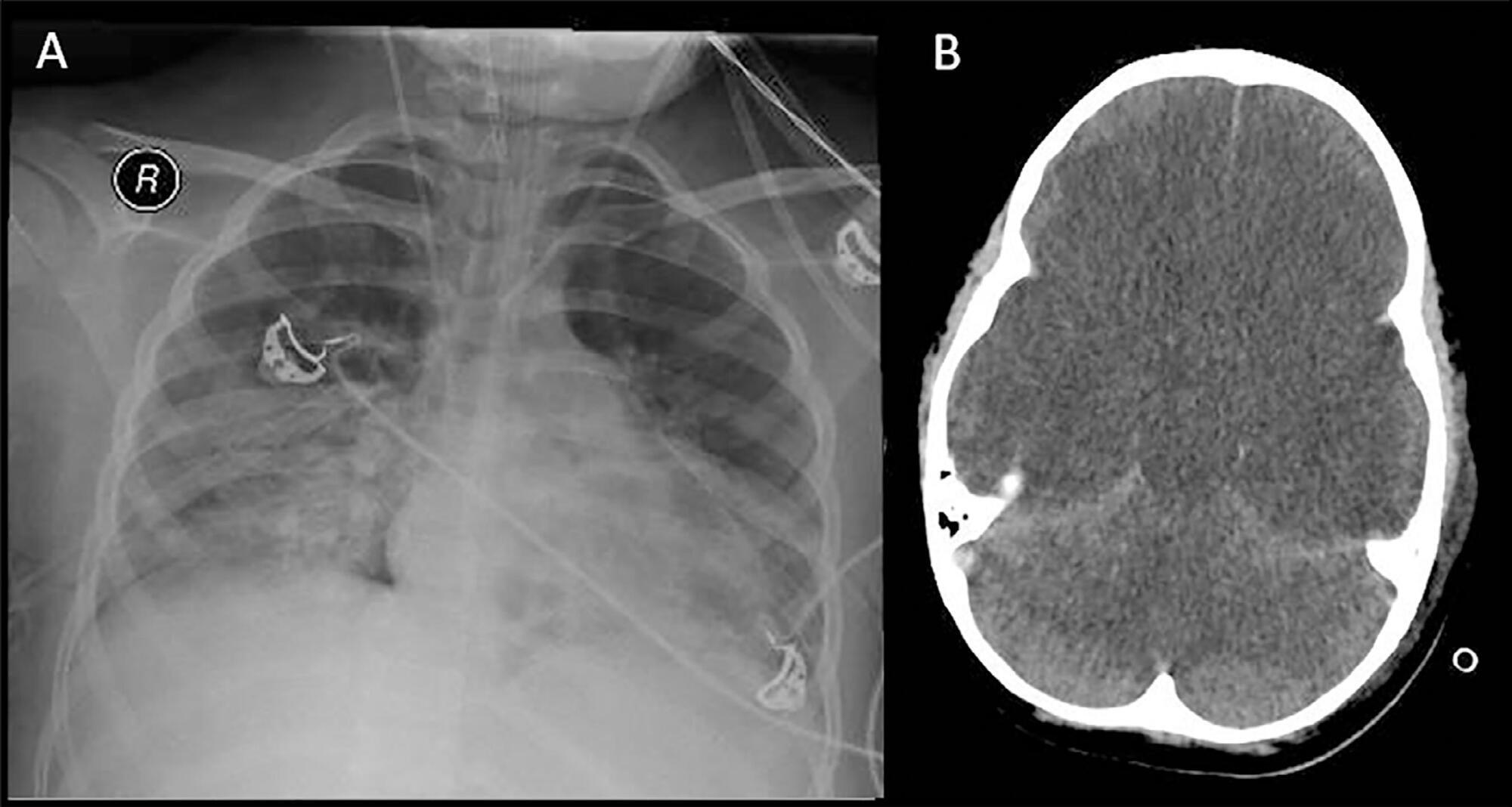
The apnea test, which involves disconnection from the mechanical ventilator, presents risks during the determination of brain death, especially in hypoxemic patients. We describe the performance of the apnea test without disconnection from the mechanical ventilator in two patients. The first case involved an 8-year-old boy admitted with severe hypoxemia due to pneumonia. He presented with cardiorespiratory arrest, followed by unresponsive coma due to hypoxic-ischemic encephalopathy. Two clinical exams revealed the absence of brainstem reflexes, and transcranial Doppler ultrasound revealed brain circulatory arrest. Three attempts were made to perform the apnea test, which were interrupted by hypoxemia; therefore, the apnea test was performed without disconnection from the mechanical ventilator, adjusting the continuous airway pressure to 10cmH2O and the inspired fraction of oxygen to 100%. The oxygen saturation was maintained at 100% for 10 minutes. Posttest blood gas analysis results were as follows: pH, 6.90; partial pressure of oxygen, 284.0mmHg; partial pressure of carbon dioxide, 94.0mmHg; and oxygen saturation, 100%. The second case involved a 43-year-old woman admitted with subarachnoid hemorrhage (Hunt-Hess V and Fisher IV). Two clinical exams revealed unresponsive coma and absence of all brainstem reflexes. Brain scintigraphy showed no radioisotope uptake into the brain parenchyma. The first attempt at the apnea test was stopped after 5 minutes due to hypothermia (34.9°C). After rewarming, the apnea test was repeated without disconnection from the mechanical ventilator, showing maintenance of the functional residual volume with electrical bioimpedance. Posttest blood gas analysis results were as follows: pH, 7.01; partial pressure of oxygen, 232.0mmHg; partial pressure of carbon dioxide, 66.9mmHg; and oxygen saturation, 99.0%. The apnea test without disconnection from the mechanical ventilator allowed the preservation of oxygenation in both cases. The use of continuous airway pressure during the apnea test seems to be a safe alternative in order to maintain alveolar recruitment and oxygenation during brain death determination.
Abstract
Rev Bras Ter Intensiva. 2020;32(2):319-325
DOI 10.5935/0103-507X.20200032
The apnea test, which involves disconnection from the mechanical ventilator, presents risks during the determination of brain death, especially in hypoxemic patients. We describe the performance of the apnea test without disconnection from the mechanical ventilator in two patients. The first case involved an 8-year-old boy admitted with severe hypoxemia due to pneumonia. He presented with cardiorespiratory arrest, followed by unresponsive coma due to hypoxic-ischemic encephalopathy. Two clinical exams revealed the absence of brainstem reflexes, and transcranial Doppler ultrasound revealed brain circulatory arrest. Three attempts were made to perform the apnea test, which were interrupted by hypoxemia; therefore, the apnea test was performed without disconnection from the mechanical ventilator, adjusting the continuous airway pressure to 10cmH2O and the inspired fraction of oxygen to 100%. The oxygen saturation was maintained at 100% for 10 minutes. Posttest blood gas analysis results were as follows: pH, 6.90; partial pressure of oxygen, 284.0mmHg; partial pressure of carbon dioxide, 94.0mmHg; and oxygen saturation, 100%. The second case involved a 43-year-old woman admitted with subarachnoid hemorrhage (Hunt-Hess V and Fisher IV). Two clinical exams revealed unresponsive coma and absence of all brainstem reflexes. Brain scintigraphy showed no radioisotope uptake into the brain parenchyma. The first attempt at the apnea test was stopped after 5 minutes due to hypothermia (34.9°C). After rewarming, the apnea test was repeated without disconnection from the mechanical ventilator, showing maintenance of the functional residual volume with electrical bioimpedance. Posttest blood gas analysis results were as follows: pH, 7.01; partial pressure of oxygen, 232.0mmHg; partial pressure of carbon dioxide, 66.9mmHg; and oxygen saturation, 99.0%. The apnea test without disconnection from the mechanical ventilator allowed the preservation of oxygenation in both cases. The use of continuous airway pressure during the apnea test seems to be a safe alternative in order to maintain alveolar recruitment and oxygenation during brain death determination.
Abstract
Rev Bras Ter Intensiva. 2019;31(1):86-92
DOI 10.5935/0103-507X.20190009
To examine the association between donor plasma cytokine levels and the development of primary graft dysfunction of organs transplanted from deceased donors.
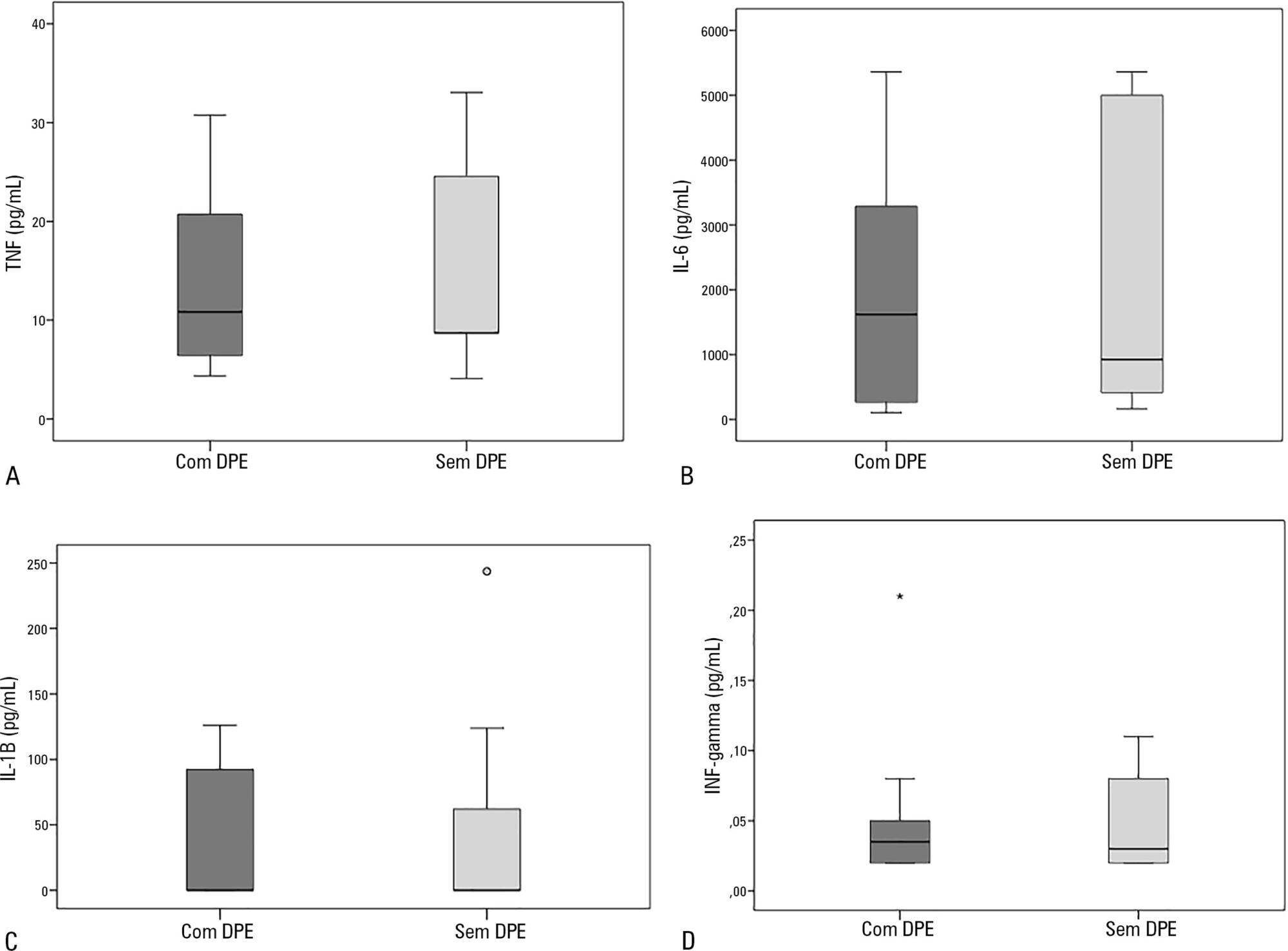
Seventeen deceased donors and the respective 47 transplant recipients were prospectively included in the study. Recipients were divided into two groups: group 1, patients who developed primary graft dysfunction; and group 2, patients who did not develop primary graft dysfunction. Donor plasma levels of TNF, IL-6, IL-1β, and IFN-γ assessed by ELISA were compared between groups.
Sixty-nine organs were retrieved, and 48 transplants were performed. Donor plasma cytokine levels did not differ between groups (in pg/mL): TNF, group 1: 10.8 (4.3 - 30.8) versus group 2: 8.7 (4.1 - 33.1), p = 0.63; IL-6, group 1: 1617.8 (106.7 - 5361.7) versus group 2: 922.9 (161.7 - 5361.7), p = 0.56; IL-1β, group 1: 0.1 (0.1 - 126.1) versus group 2: 0.1 (0.1 - 243.6), p = 0.60; and IFN-γ, group 1: 0.03 (0.02 - 0.2) versus group 2: 0.03 (0.02 - 0.1), p = 0.93). Similar findings were obtained when kidney transplants were analyzed separately.
In this sample of transplant recipients, deceased donor plasma cytokines TNF, IL-6, IL-1β, and IFN-γ were not associated with the development of primary graft dysfunction.
Abstract
Rev Bras Ter Intensiva. 2019;31(1):86-92
DOI 10.5935/0103-507X.20190009
To examine the association between donor plasma cytokine levels and the development of primary graft dysfunction of organs transplanted from deceased donors.
Seventeen deceased donors and the respective 47 transplant recipients were prospectively included in the study. Recipients were divided into two groups: group 1, patients who developed primary graft dysfunction; and group 2, patients who did not develop primary graft dysfunction. Donor plasma levels of TNF, IL-6, IL-1β, and IFN-γ assessed by ELISA were compared between groups.
Sixty-nine organs were retrieved, and 48 transplants were performed. Donor plasma cytokine levels did not differ between groups (in pg/mL): TNF, group 1: 10.8 (4.3 - 30.8) versus group 2: 8.7 (4.1 - 33.1), p = 0.63; IL-6, group 1: 1617.8 (106.7 - 5361.7) versus group 2: 922.9 (161.7 - 5361.7), p = 0.56; IL-1β, group 1: 0.1 (0.1 - 126.1) versus group 2: 0.1 (0.1 - 243.6), p = 0.60; and IFN-γ, group 1: 0.03 (0.02 - 0.2) versus group 2: 0.03 (0.02 - 0.1), p = 0.93). Similar findings were obtained when kidney transplants were analyzed separately.
In this sample of transplant recipients, deceased donor plasma cytokines TNF, IL-6, IL-1β, and IFN-γ were not associated with the development of primary graft dysfunction.
Abstract
Rev Bras Ter Intensiva. 2019;31(1):106-110
DOI 10.5935/0103-507X.20190015
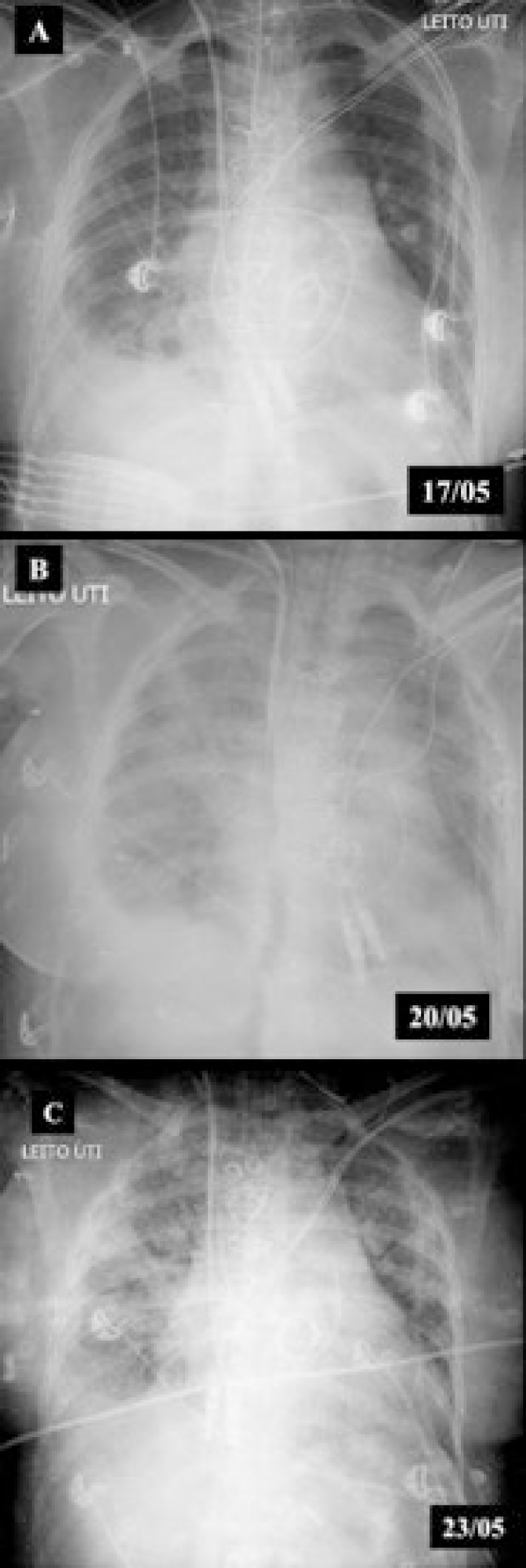
We report the case of a patient in whom brain death was suspected and associated with atelectasis and moderate to severe hypoxemia even though the patient was subjected to protective ventilation, a closed tracheal suction system, positive end-expiratory pressure, and recruitment maneuvers. Faced with the failure to obtain an adequate partial pressure of oxygen for the apnea test, we elected to place the patient in a prone position, use higher positive end-expiratory pressure, perform a new recruitment maneuver, and ventilate with a higher tidal volume (8mL/kg) without exceeding the plateau pressure of 30cmH2O. The apnea test was performed with the patient in a prone position, with continuous positive airway pressure coupled with a T-piece. The delay in diagnosis was 10 hours, and organ donation was not possible due to circulatory arrest. This report demonstrates the difficulties in obtaining higher levels of the partial pressure of oxygen for the apnea test. The delays in the diagnosis of brain death and in the organ donation process are discussed, as well as potential strategies to optimize the partial pressure of oxygen to perform the apnea test according to the current recommendations.
Abstract
Rev Bras Ter Intensiva. 2019;31(1):106-110
DOI 10.5935/0103-507X.20190015
We report the case of a patient in whom brain death was suspected and associated with atelectasis and moderate to severe hypoxemia even though the patient was subjected to protective ventilation, a closed tracheal suction system, positive end-expiratory pressure, and recruitment maneuvers. Faced with the failure to obtain an adequate partial pressure of oxygen for the apnea test, we elected to place the patient in a prone position, use higher positive end-expiratory pressure, perform a new recruitment maneuver, and ventilate with a higher tidal volume (8mL/kg) without exceeding the plateau pressure of 30cmH2O. The apnea test was performed with the patient in a prone position, with continuous positive airway pressure coupled with a T-piece. The delay in diagnosis was 10 hours, and organ donation was not possible due to circulatory arrest. This report demonstrates the difficulties in obtaining higher levels of the partial pressure of oxygen for the apnea test. The delays in the diagnosis of brain death and in the organ donation process are discussed, as well as potential strategies to optimize the partial pressure of oxygen to perform the apnea test according to the current recommendations.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (116) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)