
You searched for:"Diego Silva Leite Nunes"
We found (5) results for your search.-
Original Article
SAPS 3 in the modified NUTrition RIsk in the Critically ill score has comparable predictive accuracy to APACHE II as a severity marker
- Valeska Fernandes Pasinato
 ,
, - Oellen Stuani Franzosi ,
- Sérgio Henrique Loss ,
- Diego Silva Leite Nunes,
- Kelly Carraro Foletto, [ … ],
- Silvia Regina Rios Vieira
Abstract
Original ArticleSAPS 3 in the modified NUTrition RIsk in the Critically ill score has comparable predictive accuracy to APACHE II as a severity marker
Rev Bras Ter Intensiva. 2021;33(3):394-400
DOI 10.5935/0103-507X.20210064
- Valeska Fernandes Pasinato ,
- Oellen Stuani Franzosi ,
- Sérgio Henrique Loss ,
- Diego Silva Leite Nunes,
- Kelly Carraro Foletto,
- Gabriela Soranço Salazar,
- Silvia Regina Rios Vieira
Views2ABSTRACT
Objective:
To evaluate the substitution of Acute Physiology and Chronic Health Evaluation II (APACHE II) by Simplified Acute Physiology Score 3 (SAPS 3) as a severity marker in the modified version of the NUTrition RIsk in the Critically ill score (mNUTRIC); without interleukin 6) based on an analysis of its discriminative ability for in-hospital mortality prediction.
Methods:
This retrospective cohort study evaluated 1,516 adult patients admitted to an intensive care unit of a private general hospital from April 2017 to January 2018. Performance evaluation included Fleiss’ Kappa and Pearson correlation analysis. The discriminative ability for estimating in-hospital mortality was assessed with the Receiver Operating Characteristic curve.
Results:
The sample was randomly divided into two-thirds for model development (n = 1,025; age 72 [57 – 83]; 52.4% male) and one-third for performance evaluation (n = 490; age 72 [57 – 83]; 50.8% male). The agreement with mNUTRIC was Kappa of 0.563 (p < 0.001), and the correlation between the instruments was Pearson correlation of 0.804 (p < 0.001). The tool showed good performance in predicting in-hospital mortality (area under the curve 0.825 [0.787 - 0.863] p < 0.001).
Conclusion:
The substitution of APACHE II by SAPS 3 as a severity marker in the mNUTRIC score showed good performance in predicting in-hospital mortality. These data provide the first evidence regarding the validity of the substitution of APACHE II by SAPS 3 in the mNUTRIC as a marker of severity. Multicentric studies and additional analyses of nutritional adequacy parameters are required.
Keywords:APACHECritical careMortalitynutritional assessmentSeverity of illness indexSimplified acute physiology scoreSee moreViews2

Abstract
Original ArticleSAPS 3 in the modified NUTrition RIsk in the Critically ill score has comparable predictive accuracy to APACHE II as a severity marker
Rev Bras Ter Intensiva. 2021;33(3):394-400
DOI 10.5935/0103-507X.20210064
- Valeska Fernandes Pasinato ,
- Oellen Stuani Franzosi ,
- Sérgio Henrique Loss ,
- Diego Silva Leite Nunes,
- Kelly Carraro Foletto,
- Gabriela Soranço Salazar,
- Silvia Regina Rios Vieira
Views2ABSTRACT
Objective:
To evaluate the substitution of Acute Physiology and Chronic Health Evaluation II (APACHE II) by Simplified Acute Physiology Score 3 (SAPS 3) as a severity marker in the modified version of the NUTrition RIsk in the Critically ill score (mNUTRIC); without interleukin 6) based on an analysis of its discriminative ability for in-hospital mortality prediction.
Methods:
This retrospective cohort study evaluated 1,516 adult patients admitted to an intensive care unit of a private general hospital from April 2017 to January 2018. Performance evaluation included Fleiss’ Kappa and Pearson correlation analysis. The discriminative ability for estimating in-hospital mortality was assessed with the Receiver Operating Characteristic curve.
Results:
The sample was randomly divided into two-thirds for model development (n = 1,025; age 72 [57 – 83]; 52.4% male) and one-third for performance evaluation (n = 490; age 72 [57 – 83]; 50.8% male). The agreement with mNUTRIC was Kappa of 0.563 (p < 0.001), and the correlation between the instruments was Pearson correlation of 0.804 (p < 0.001). The tool showed good performance in predicting in-hospital mortality (area under the curve 0.825 [0.787 - 0.863] p < 0.001).
Conclusion:
The substitution of APACHE II by SAPS 3 as a severity marker in the mNUTRIC score showed good performance in predicting in-hospital mortality. These data provide the first evidence regarding the validity of the substitution of APACHE II by SAPS 3 in the mNUTRIC as a marker of severity. Multicentric studies and additional analyses of nutritional adequacy parameters are required.
Keywords:APACHECritical careMortalitynutritional assessmentSeverity of illness indexSimplified acute physiology scoreSee more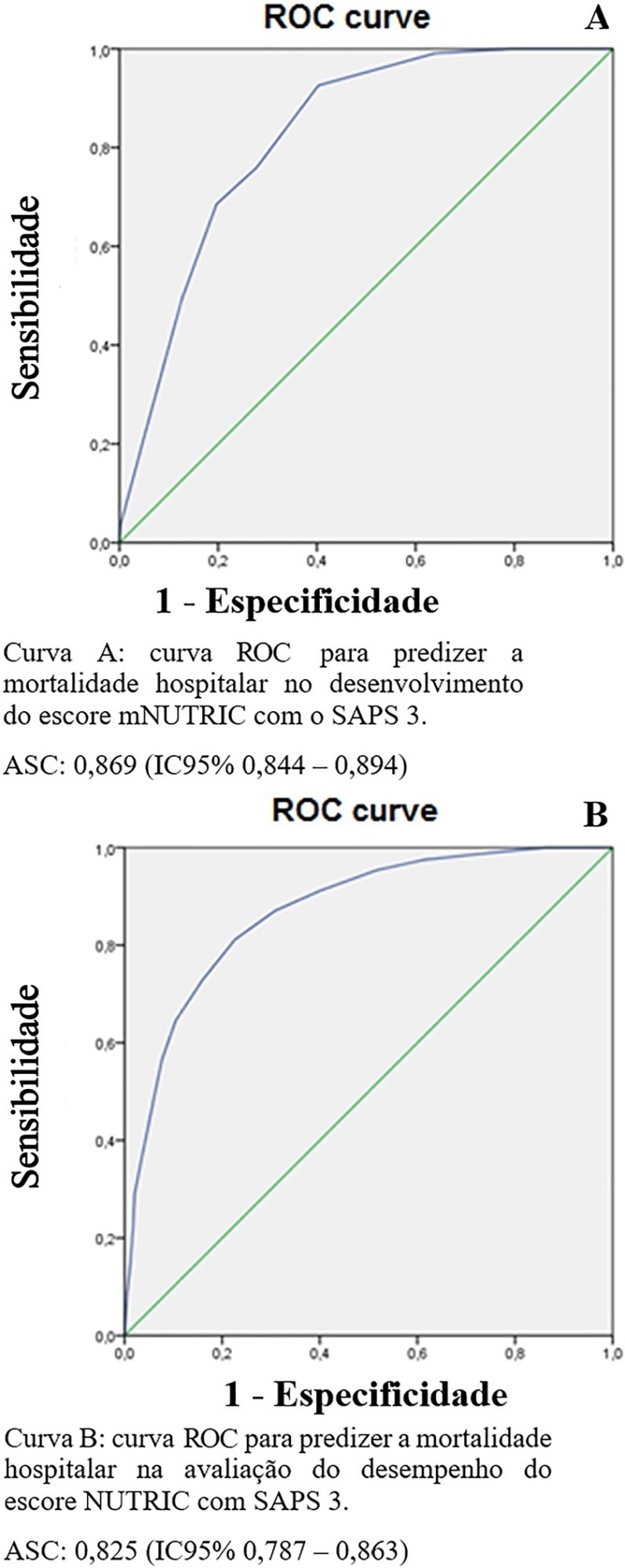
- Valeska Fernandes Pasinato
-
Original Article
Changes in cardiac arrest profiles after the implementation of a Rapid Response Team
- Marina Verçoza Viana ,
- Diego Silva Leite Nunes,
- Cassiano Teixeira ,
- Silvia Regina Rios Vieira,
- Grazziela Torres, [ … ],
- Marcio Manozzo Boniatti
Abstract
Original ArticleChanges in cardiac arrest profiles after the implementation of a Rapid Response Team
Rev Bras Ter Intensiva. 2021;33(1):96-101
DOI 10.5935/0103-507X.20210010
- Marina Verçoza Viana ,
- Diego Silva Leite Nunes,
- Cassiano Teixeira ,
- Silvia Regina Rios Vieira,
- Grazziela Torres,
- Janete Salles Brauner,
- Helena Müller,
- Thais Crivellaro Dutra Butelli,
- Marcio Manozzo Boniatti
Views1See moreABSTRACT
Objective:
To evaluate changes in the characteristics of in-hospital cardiac arrest after the implementation of a Rapid Response Team.
Methods:
This was a prospective observational study of in-hospital cardiac arrest that occurred from January 2013 to December 2017. The exclusion criterion was in-hospital cardiac arrest in the intensive care unit, emergency room or operating room. The Rapid Response Team was implemented in July 2014 in the study hospital. Patients were classified into two groups: a Pre-Rapid Response Team (in-hospital cardiac arrest before Rapid Response Team implementation) and a Post-Rapid Response Team (in-hospital cardiac arrest after Rapid Response Team implementation). Patients were followed until hospital discharge or death.
Results:
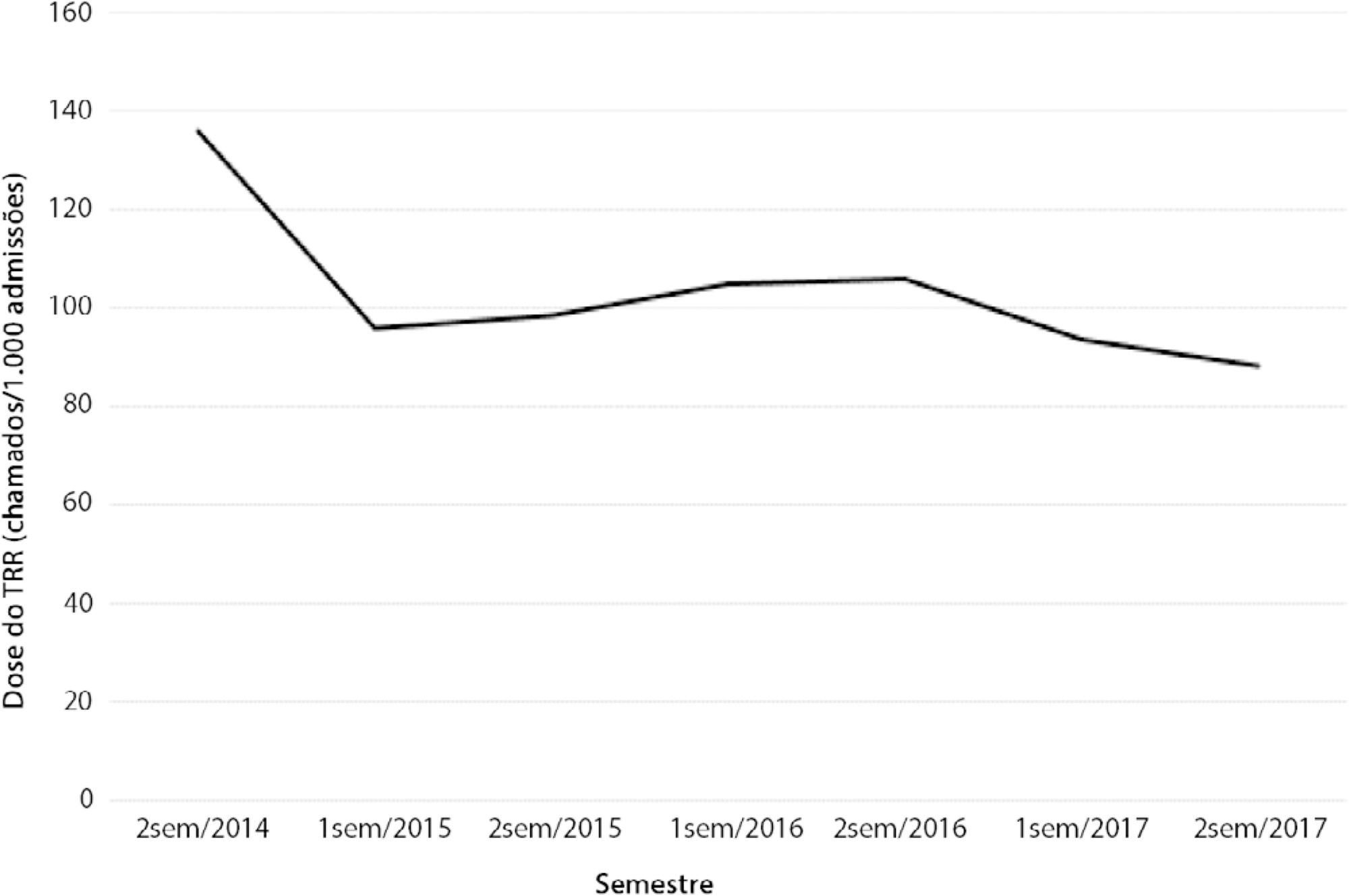
We had a total of 308 cardiac arrests (64.6 ± 15.2 years, 60.3% men, 13.9% with initial shockable rhythm). There was a decrease from 4.2 to 2.5 in-hospital cardiac arrest/1000 admissions after implementation of the Rapid Response Team, and we had approximately 124 calls/1000 admissions. Pre-Rapid Response Team cardiac arrest was associated with more hypoxia (29.4 versus 14.3%; p = 0.006) and an altered respiratory rate (14.7 versus 4.2%; p = 0.004) compared with post-Rapid Response Team cardiac arrest. Cardiac arrest due to hypoxia was more common before Rapid Response Team implementation (61.2 versus 38.1%, p < 0.001). In multivariate analysis, return of spontaneous circulation was associated with shockable rhythm (OR 2.97; IC95% 1.04 - 8.43) and witnessed cardiac arrest (OR 2.52; IC95% 1.39 - 4.59) but not with Rapid Response Team implementation (OR 1.40; IC95% 0.70 - 2.81) or premonitory signs (OR 0.71; IC95% 0.39 - 1.28). In multivariate analysis, in-hospital mortality was associated with non-shockable rhythm (OR 5.34; IC95% 2.28 - 12.53) and age (OR 1.03; IC95% 1.01 - 1.05) but not with Rapid Response Team implementation (OR 0.89; IC95% 0.40 - 2.02).
Conclusion:
Even though Rapid Response Team implementation is associated with a reduction in in-hospital cardiac arrest, it was not associated with the mortality of in-hospital cardiac arrest victims. A significant decrease in cardiac arrests due to respiratory causes was noted after Rapid Response Team implementation.
Views1Abstract
Original ArticleChanges in cardiac arrest profiles after the implementation of a Rapid Response Team
Rev Bras Ter Intensiva. 2021;33(1):96-101
DOI 10.5935/0103-507X.20210010
- Marina Verçoza Viana ,
- Diego Silva Leite Nunes,
- Cassiano Teixeira ,
- Silvia Regina Rios Vieira,
- Grazziela Torres,
- Janete Salles Brauner,
- Helena Müller,
- Thais Crivellaro Dutra Butelli,
- Marcio Manozzo Boniatti
Views1See moreABSTRACT
Objective:
To evaluate changes in the characteristics of in-hospital cardiac arrest after the implementation of a Rapid Response Team.
Methods:
This was a prospective observational study of in-hospital cardiac arrest that occurred from January 2013 to December 2017. The exclusion criterion was in-hospital cardiac arrest in the intensive care unit, emergency room or operating room. The Rapid Response Team was implemented in July 2014 in the study hospital. Patients were classified into two groups: a Pre-Rapid Response Team (in-hospital cardiac arrest before Rapid Response Team implementation) and a Post-Rapid Response Team (in-hospital cardiac arrest after Rapid Response Team implementation). Patients were followed until hospital discharge or death.
Results:
We had a total of 308 cardiac arrests (64.6 ± 15.2 years, 60.3% men, 13.9% with initial shockable rhythm). There was a decrease from 4.2 to 2.5 in-hospital cardiac arrest/1000 admissions after implementation of the Rapid Response Team, and we had approximately 124 calls/1000 admissions. Pre-Rapid Response Team cardiac arrest was associated with more hypoxia (29.4 versus 14.3%; p = 0.006) and an altered respiratory rate (14.7 versus 4.2%; p = 0.004) compared with post-Rapid Response Team cardiac arrest. Cardiac arrest due to hypoxia was more common before Rapid Response Team implementation (61.2 versus 38.1%, p < 0.001). In multivariate analysis, return of spontaneous circulation was associated with shockable rhythm (OR 2.97; IC95% 1.04 - 8.43) and witnessed cardiac arrest (OR 2.52; IC95% 1.39 - 4.59) but not with Rapid Response Team implementation (OR 1.40; IC95% 0.70 - 2.81) or premonitory signs (OR 0.71; IC95% 0.39 - 1.28). In multivariate analysis, in-hospital mortality was associated with non-shockable rhythm (OR 5.34; IC95% 2.28 - 12.53) and age (OR 1.03; IC95% 1.01 - 1.05) but not with Rapid Response Team implementation (OR 0.89; IC95% 0.40 - 2.02).
Conclusion:
Even though Rapid Response Team implementation is associated with a reduction in in-hospital cardiac arrest, it was not associated with the mortality of in-hospital cardiac arrest victims. A significant decrease in cardiac arrests due to respiratory causes was noted after Rapid Response Team implementation.
- Marina Verçoza Viana
-
Special Article
Brazilian guidelines for the management of brain-dead potential organ donors. The task force of the Associação de Medicina Intensiva Brasileira, Associação Brasileira de Transplantes de Órgãos, Brazilian Research in Critical Care Network, and the General Coordination of the National Transplant System
- Glauco Adrieno Westphal ,
- Caroline Cabral Robinson,
- Alexandre Biasi Cavalcanti ,
- Anderson Ricardo Roman Gonçalves,
- Cátia Moreira Guterres, [ … ],
- Maicon Falavigna
Abstract
Special ArticleBrazilian guidelines for the management of brain-dead potential organ donors. The task force of the Associação de Medicina Intensiva Brasileira, Associação Brasileira de Transplantes de Órgãos, Brazilian Research in Critical Care Network, and the General Coordination of the National Transplant System
Rev Bras Ter Intensiva. 2021;33(1):1-11
DOI 10.5935/0103-507X.20210001
- Glauco Adrieno Westphal ,
- Caroline Cabral Robinson,
- Alexandre Biasi Cavalcanti ,
- Anderson Ricardo Roman Gonçalves,
- Cátia Moreira Guterres,
- Cassiano Teixeira ,
- Cinara Stein,
- Cristiano Augusto Franke,
- Daiana Barbosa da Silva,
- Daniela Ferreira Salomão Pontes,
- Diego Silva Leite Nunes,
- Edson Abdala,
- Felipe Dal-Pizzol ,
- Fernando Augusto Bozza ,
- Flávia Ribeiro Machado,
- Joel de Andrade,
- Luciane Nascimento Cruz,
- Luciano César Pontes Azevedo,
- Miriam Cristine Vahl Machado,
- Regis Goulart Rosa ,
- Roberto Ceratti Manfro,
- Rosana Reis Nothen,
- Suzana Margareth Lobo,
- Tatiana Helena Rech ,
- Thiago Costa Lisboa,
- Verônica Colpani,
- Maicon Falavigna
Views5See moreAbstract
Objective:
To contribute to updating the recommendations for brain-dead potential organ donor management.
Methods:
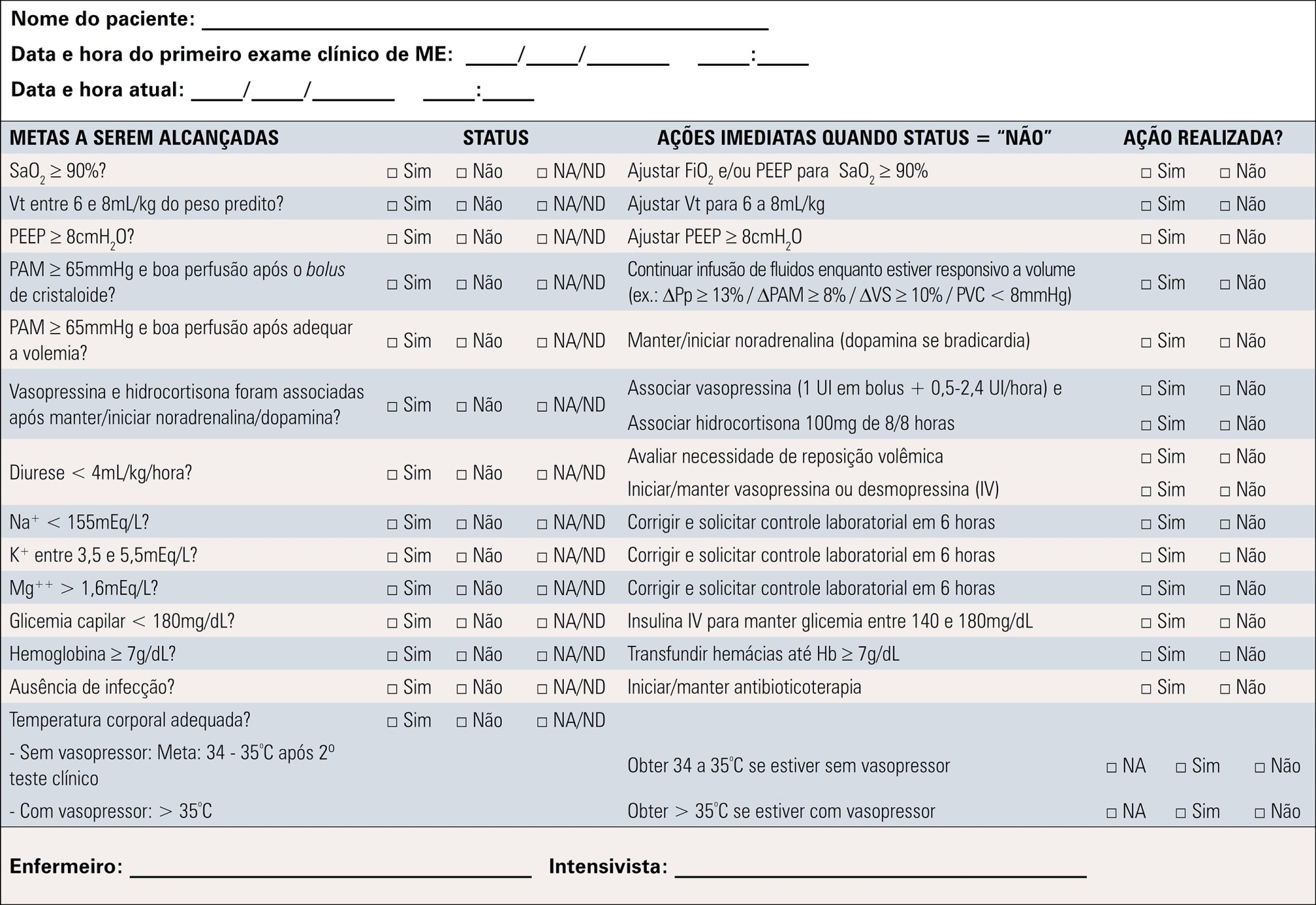
A group of 27 experts, including intensivists, transplant coordinators, transplant surgeons, and epidemiologists, answered questions related to the following topics were divided into mechanical ventilation, hemodynamics, endocrine-metabolic management, infection, body temperature, blood transfusion, and checklists use. The outcomes considered were cardiac arrests, number of organs removed or transplanted as well as function / survival of transplanted organs. The quality of evidence of the recommendations was assessed using the Grading of Recommendations Assessment, Development, and Evaluation system to classify the recommendations.
Results:
A total of 19 recommendations were drawn from the expert panel. Of these, 7 were classified as strong, 11 as weak and 1 was considered a good clinical practice.
Conclusion:
Despite the agreement among panel members on most recommendations, the grade of recommendation was mostly weak.
Views5Abstract
Special ArticleBrazilian guidelines for the management of brain-dead potential organ donors. The task force of the Associação de Medicina Intensiva Brasileira, Associação Brasileira de Transplantes de Órgãos, Brazilian Research in Critical Care Network, and the General Coordination of the National Transplant System
Rev Bras Ter Intensiva. 2021;33(1):1-11
DOI 10.5935/0103-507X.20210001
- Glauco Adrieno Westphal ,
- Caroline Cabral Robinson,
- Alexandre Biasi Cavalcanti ,
- Anderson Ricardo Roman Gonçalves,
- Cátia Moreira Guterres,
- Cassiano Teixeira ,
- Cinara Stein,
- Cristiano Augusto Franke,
- Daiana Barbosa da Silva,
- Daniela Ferreira Salomão Pontes,
- Diego Silva Leite Nunes,
- Edson Abdala,
- Felipe Dal-Pizzol ,
- Fernando Augusto Bozza ,
- Flávia Ribeiro Machado,
- Joel de Andrade,
- Luciane Nascimento Cruz,
- Luciano César Pontes Azevedo,
- Miriam Cristine Vahl Machado,
- Regis Goulart Rosa ,
- Roberto Ceratti Manfro,
- Rosana Reis Nothen,
- Suzana Margareth Lobo,
- Tatiana Helena Rech ,
- Thiago Costa Lisboa,
- Verônica Colpani,
- Maicon Falavigna
Views5See moreAbstract
Objective:
To contribute to updating the recommendations for brain-dead potential organ donor management.
Methods:
A group of 27 experts, including intensivists, transplant coordinators, transplant surgeons, and epidemiologists, answered questions related to the following topics were divided into mechanical ventilation, hemodynamics, endocrine-metabolic management, infection, body temperature, blood transfusion, and checklists use. The outcomes considered were cardiac arrests, number of organs removed or transplanted as well as function / survival of transplanted organs. The quality of evidence of the recommendations was assessed using the Grading of Recommendations Assessment, Development, and Evaluation system to classify the recommendations.
Results:
A total of 19 recommendations were drawn from the expert panel. Of these, 7 were classified as strong, 11 as weak and 1 was considered a good clinical practice.
Conclusion:
Despite the agreement among panel members on most recommendations, the grade of recommendation was mostly weak.
- Glauco Adrieno Westphal
-
Review Articles
Chronic critical illness: are we saving patients or creating victims?
Rev Bras Ter Intensiva. 2017;29(1):87-95
Abstract
Review ArticlesChronic critical illness: are we saving patients or creating victims?
Rev Bras Ter Intensiva. 2017;29(1):87-95
DOI 10.5935/0103-507X.20170013
Views1See moreABSTRACT
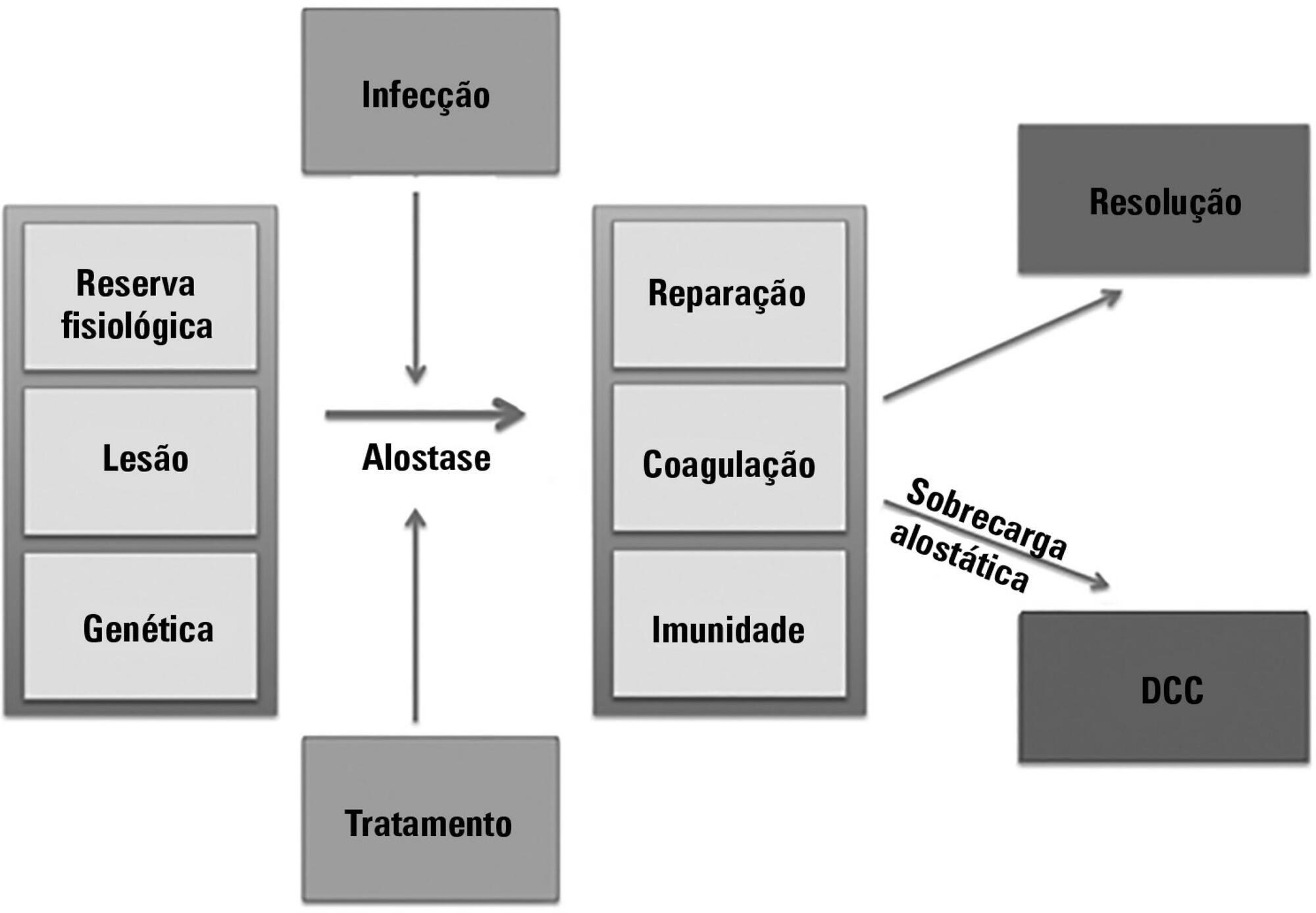
The technological advancements that allow support for organ dysfunction have led to an increase in survival rates for the most critically ill patients. Some of these patients survive the initial acute critical condition but continue to suffer from organ dysfunction and remain in an inflammatory state for long periods of time. This group of critically ill patients has been described since the 1980s and has had different diagnostic criteria over the years. These patients are known to have lengthy hospital stays, undergo significant alterations in muscle and bone metabolism, show immunodeficiency, consume substantial health resources, have reduced functional and cognitive capacity after discharge, create a sizable workload for caregivers, and present high long-term mortality rates. The aim of this review is to report on the most current evidence in terms of the definition, pathophysiology, clinical manifestations, treatment, and prognosis of persistent critical illness.
Views1Abstract
Review ArticlesChronic critical illness: are we saving patients or creating victims?
Rev Bras Ter Intensiva. 2017;29(1):87-95
DOI 10.5935/0103-507X.20170013
Views1See moreABSTRACT
The technological advancements that allow support for organ dysfunction have led to an increase in survival rates for the most critically ill patients. Some of these patients survive the initial acute critical condition but continue to suffer from organ dysfunction and remain in an inflammatory state for long periods of time. This group of critically ill patients has been described since the 1980s and has had different diagnostic criteria over the years. These patients are known to have lengthy hospital stays, undergo significant alterations in muscle and bone metabolism, show immunodeficiency, consume substantial health resources, have reduced functional and cognitive capacity after discharge, create a sizable workload for caregivers, and present high long-term mortality rates. The aim of this review is to report on the most current evidence in terms of the definition, pathophysiology, clinical manifestations, treatment, and prognosis of persistent critical illness.
-
Author’s Response
AUTHORS’ RESPONSE
Rev Bras Ter Intensiva. 2015;27(1):85-88
Abstract
Author’s ResponseAUTHORS’ RESPONSE
Rev Bras Ter Intensiva. 2015;27(1):85-88
DOI 10.5935/0103-507X.20150015
Views0We thank Mattos and Nunes for their careful reading, comments and concerns about our study.() Since April 2011, the Brazilian Health Ministry has created a system devoted to the care for health technology assessment, which is called “Comissão Nacional de Incorporação de Tecnologias para o SUS (CONITEC)”. Moreover, the method for technology incorporation is positively […]See moreViews0Abstract
Author’s ResponseAUTHORS’ RESPONSE
Rev Bras Ter Intensiva. 2015;27(1):85-88
DOI 10.5935/0103-507X.20150015
Views0We thank Mattos and Nunes for their careful reading, comments and concerns about our study.() Since April 2011, the Brazilian Health Ministry has created a system devoted to the care for health technology assessment, which is called “Comissão Nacional de Incorporação de Tecnologias para o SUS (CONITEC)”. Moreover, the method for technology incorporation is positively […]See more
Search
Search in:
KEY WORDS
Case reports Child Coronavirus infections COVID-19 Critical care Critical illness Extracorporeal membrane oxygenation Infant, newborn Intensive care Intensive care units Intensive care units, pediatric mechanical ventilation Mortality Physical therapy modalities Prognosis Respiration, artificial Respiratory insufficiency risk factors SARS-CoV-2 Sepsis