Hypoxia Archives - Critical Care Science (CCS)

Abstract
Crit Care Sci. 2023;35(2):156-162
DOI 10.5935/2965-2774.20230343-pt
To identify risk factors for nonresponse to prone positioning in mechanically ventilated patients with COVID-19-associated severe acute respiratory distress syndrome and refractory hypoxemia in a tertiary care hospital in Colombia.
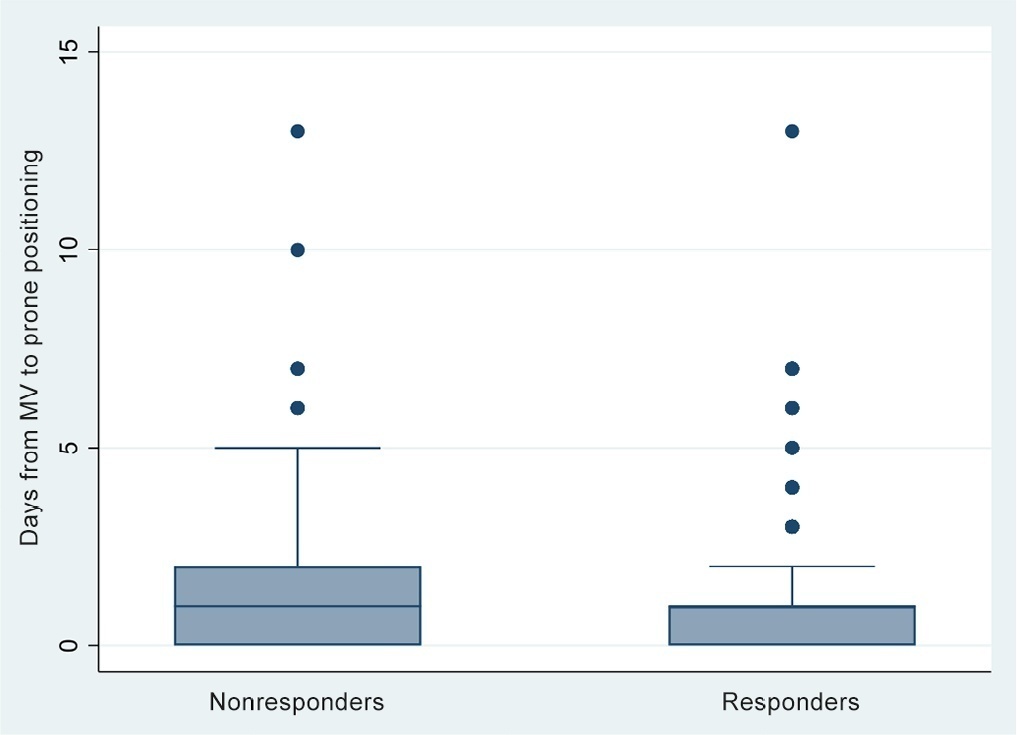
Observational study based on a retrospective cohort of mechanically ventilated patients with severe acute respiratory distress syndrome due to SARS-CoV-2 who underwent prone positioning due to refractory hypoxemia. The study considered an improvement ≥ 20% in the PaO2/FiO2 ratio after the first cycle of 16 hours in the prone position to be a ‘response’. Nonresponding patients were considered cases, and responding patients were controls. We controlled for clinical, laboratory, and radiological variables.
A total of 724 patients were included (58.67 ± 12.37 years, 67.7% males). Of those, 21.9% were nonresponders. Mortality was 54.1% for nonresponders and 31.3% for responders (p < 0.001). Variables associated with nonresponse were time from the start of mechanical ventilation to pronation (OR 1.23; 95%CI 1.10 - 1.41); preintubation PaO2/FiO2 ratio (OR 0.62; 95%CI 0.40 - 0.96); preprone PaO2/FiO2 ratio (OR 1.88. 95%CI 1.22 - 2.94); and radiologic multilobe consolidation (OR 2.12; 95%CI 1.33 - 3.33) or mixed pattern (OR 1.72; 95%CI 1.07 - 2.85) compared with a ground-glass pattern.
This study identified factors associated with nonresponse to prone positioning in patients with refractory hypoxemia and acute respiratory distress syndrome due to SARS-CoV-2 receiving mechanical ventilation. Recognizing such factors helps identify candidates for other rescue strategies, including more extensive prone positioning or extracorporeal membrane oxygenation. Further studies are needed to assess the consistency of these findings in populations with acute respiratory distress syndrome of other etiologies.
Abstract
Crit Care Sci. 2023;35(2):156-162
DOI 10.5935/2965-2774.20230343-pt
To identify risk factors for nonresponse to prone positioning in mechanically ventilated patients with COVID-19-associated severe acute respiratory distress syndrome and refractory hypoxemia in a tertiary care hospital in Colombia.
Observational study based on a retrospective cohort of mechanically ventilated patients with severe acute respiratory distress syndrome due to SARS-CoV-2 who underwent prone positioning due to refractory hypoxemia. The study considered an improvement ≥ 20% in the PaO2/FiO2 ratio after the first cycle of 16 hours in the prone position to be a ‘response’. Nonresponding patients were considered cases, and responding patients were controls. We controlled for clinical, laboratory, and radiological variables.
A total of 724 patients were included (58.67 ± 12.37 years, 67.7% males). Of those, 21.9% were nonresponders. Mortality was 54.1% for nonresponders and 31.3% for responders (p < 0.001). Variables associated with nonresponse were time from the start of mechanical ventilation to pronation (OR 1.23; 95%CI 1.10 - 1.41); preintubation PaO2/FiO2 ratio (OR 0.62; 95%CI 0.40 - 0.96); preprone PaO2/FiO2 ratio (OR 1.88. 95%CI 1.22 - 2.94); and radiologic multilobe consolidation (OR 2.12; 95%CI 1.33 - 3.33) or mixed pattern (OR 1.72; 95%CI 1.07 - 2.85) compared with a ground-glass pattern.
This study identified factors associated with nonresponse to prone positioning in patients with refractory hypoxemia and acute respiratory distress syndrome due to SARS-CoV-2 receiving mechanical ventilation. Recognizing such factors helps identify candidates for other rescue strategies, including more extensive prone positioning or extracorporeal membrane oxygenation. Further studies are needed to assess the consistency of these findings in populations with acute respiratory distress syndrome of other etiologies.
Abstract
Rev Bras Ter Intensiva. 2022;34(4):402-409
DOI 10.5935/0103-507X.20220299-en
To characterize the pressures, resistances, oxygenation, and decarboxylation efficacy of two oxygenators associated in series or in parallel during venous-venous extracorporeal membrane oxygenation support.
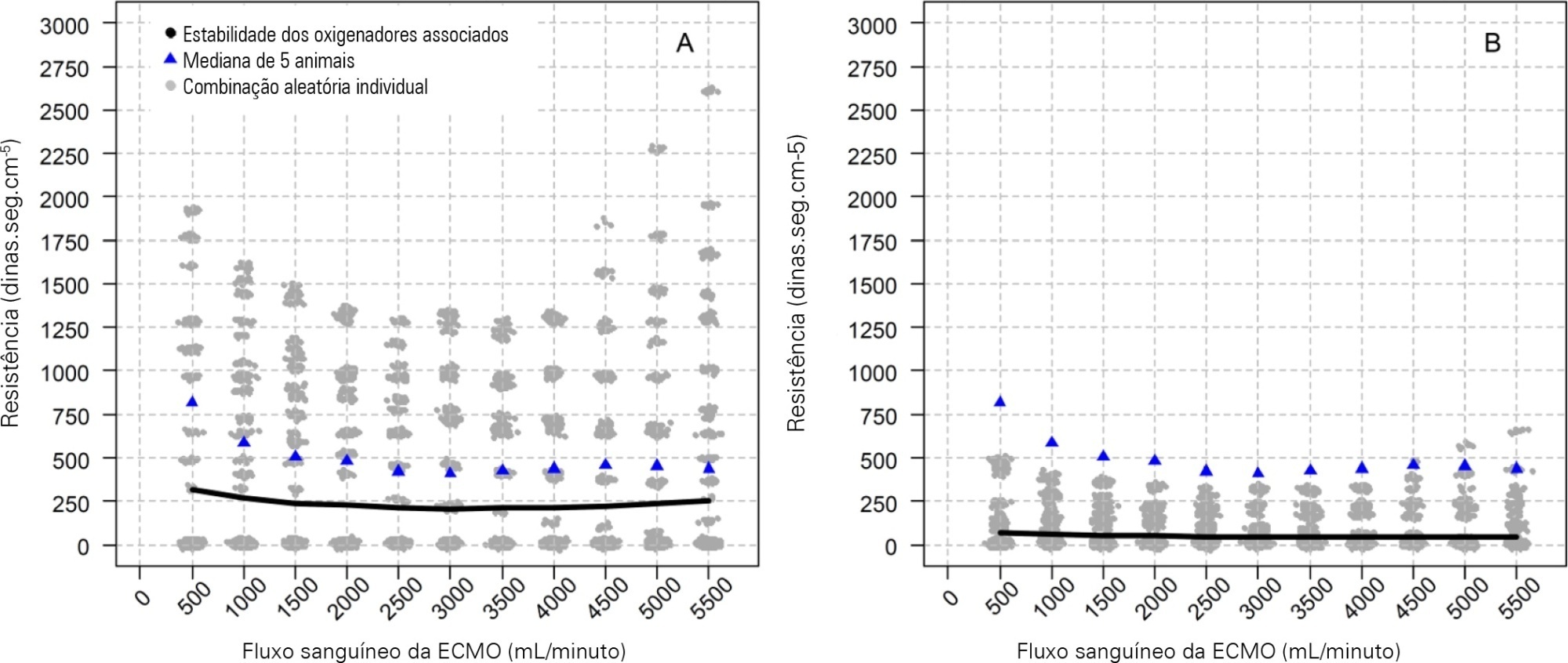
Using the results of a swine severe respiratory failure associated with multiple organ dysfunction venous-venous extracorporeal membrane oxygenation support model and mathematical modeling, we explored the effects on oxygenation, decarboxylation and circuit pressures of in-parallel and in-series associations of oxygenators.
Five animals with a median weight of 80kg were tested. Both configurations increased the oxygen partial pressure after the oxygenators. The return cannula oxygen content was also slightly higher, but the impact on systemic oxygenation was minimal using oxygenators with a high rated flow (~ 7L/minute). Both configurations significantly reduced the systemic carbon dioxide partial pressure. As the extracorporeal membrane oxygenation blood flow increased, the oxygenator resistance decreased initially with a further increase with higher blood flows but with a small clinical impact.
Association of oxygenators in parallel or in series during venous-venous extracorporeal membrane oxygenation support provides a modest increase in carbon dioxide partial pressure removal with a slight improvement in oxygenation. The effect of oxygenator associations on extracorporeal circuit pressures is minimal.
Abstract
Rev Bras Ter Intensiva. 2022;34(4):402-409
DOI 10.5935/0103-507X.20220299-en
To characterize the pressures, resistances, oxygenation, and decarboxylation efficacy of two oxygenators associated in series or in parallel during venous-venous extracorporeal membrane oxygenation support.
Using the results of a swine severe respiratory failure associated with multiple organ dysfunction venous-venous extracorporeal membrane oxygenation support model and mathematical modeling, we explored the effects on oxygenation, decarboxylation and circuit pressures of in-parallel and in-series associations of oxygenators.
Five animals with a median weight of 80kg were tested. Both configurations increased the oxygen partial pressure after the oxygenators. The return cannula oxygen content was also slightly higher, but the impact on systemic oxygenation was minimal using oxygenators with a high rated flow (~ 7L/minute). Both configurations significantly reduced the systemic carbon dioxide partial pressure. As the extracorporeal membrane oxygenation blood flow increased, the oxygenator resistance decreased initially with a further increase with higher blood flows but with a small clinical impact.
Association of oxygenators in parallel or in series during venous-venous extracorporeal membrane oxygenation support provides a modest increase in carbon dioxide partial pressure removal with a slight improvement in oxygenation. The effect of oxygenator associations on extracorporeal circuit pressures is minimal.
Abstract
Rev Bras Ter Intensiva. 2020;32(2):319-325
DOI 10.5935/0103-507X.20200032
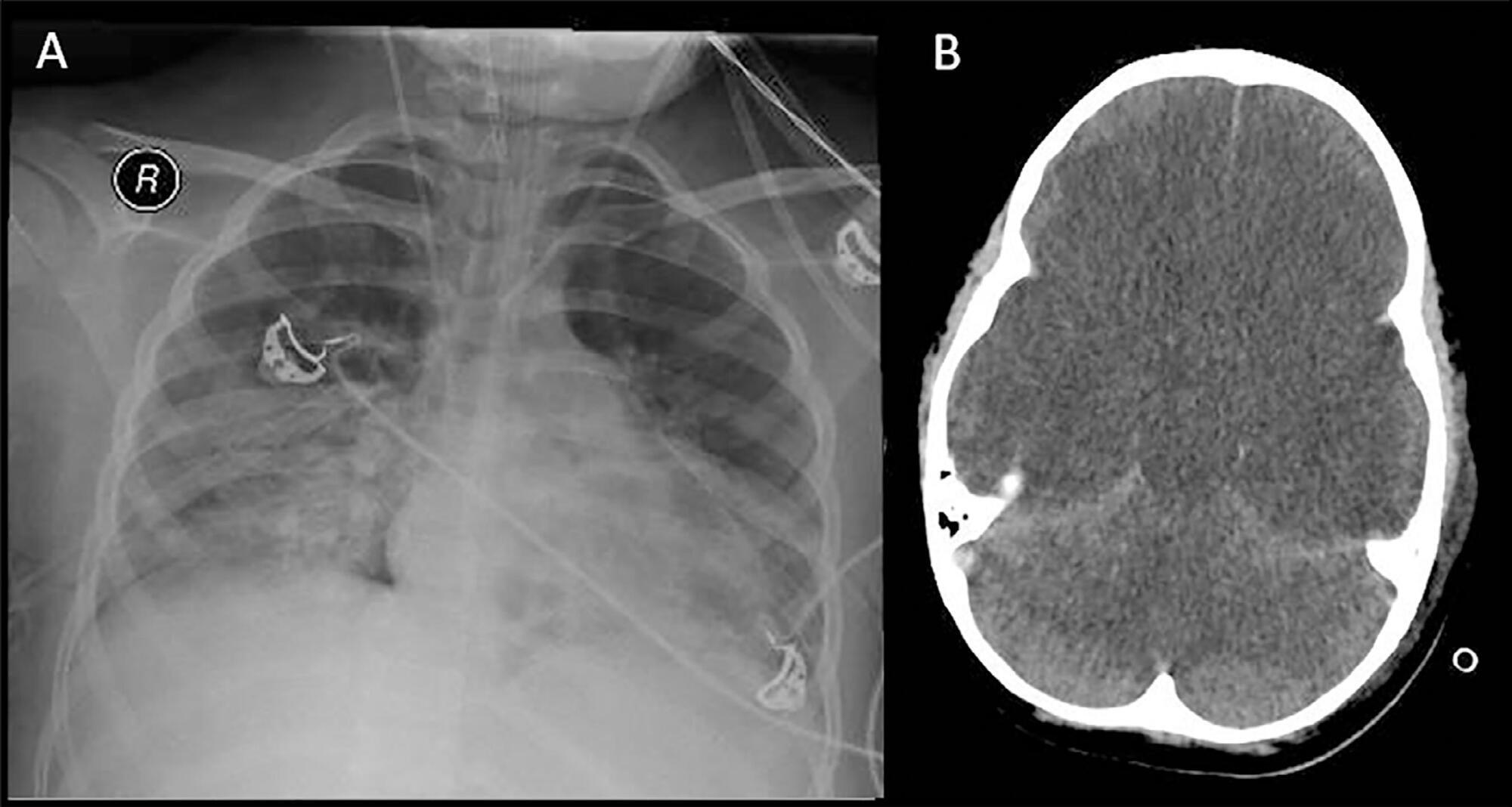
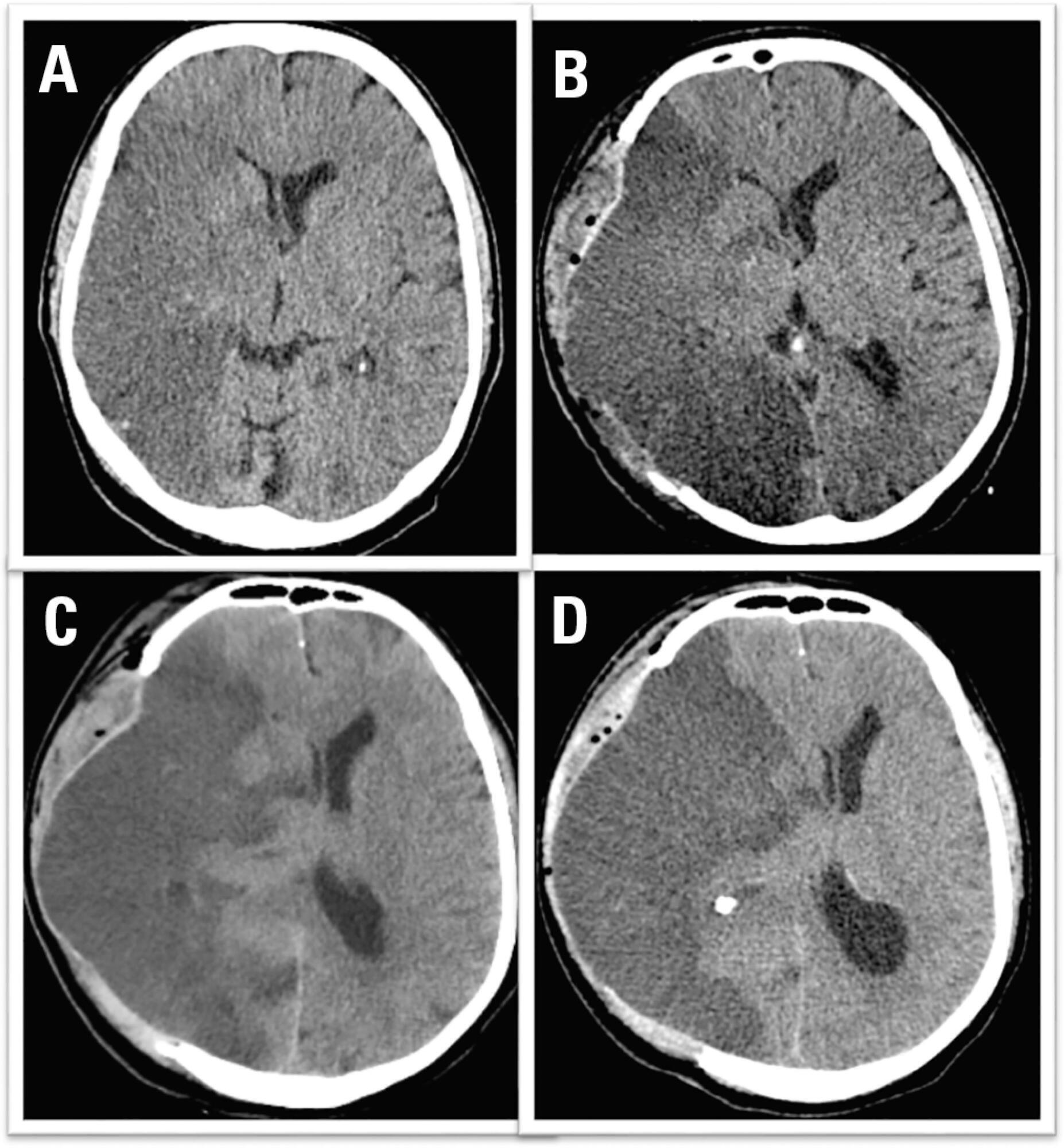
The apnea test, which involves disconnection from the mechanical ventilator, presents risks during the determination of brain death, especially in hypoxemic patients. We describe the performance of the apnea test without disconnection from the mechanical ventilator in two patients. The first case involved an 8-year-old boy admitted with severe hypoxemia due to pneumonia. He presented with cardiorespiratory arrest, followed by unresponsive coma due to hypoxic-ischemic encephalopathy. Two clinical exams revealed the absence of brainstem reflexes, and transcranial Doppler ultrasound revealed brain circulatory arrest. Three attempts were made to perform the apnea test, which were interrupted by hypoxemia; therefore, the apnea test was performed without disconnection from the mechanical ventilator, adjusting the continuous airway pressure to 10cmH2O and the inspired fraction of oxygen to 100%. The oxygen saturation was maintained at 100% for 10 minutes. Posttest blood gas analysis results were as follows: pH, 6.90; partial pressure of oxygen, 284.0mmHg; partial pressure of carbon dioxide, 94.0mmHg; and oxygen saturation, 100%. The second case involved a 43-year-old woman admitted with subarachnoid hemorrhage (Hunt-Hess V and Fisher IV). Two clinical exams revealed unresponsive coma and absence of all brainstem reflexes. Brain scintigraphy showed no radioisotope uptake into the brain parenchyma. The first attempt at the apnea test was stopped after 5 minutes due to hypothermia (34.9°C). After rewarming, the apnea test was repeated without disconnection from the mechanical ventilator, showing maintenance of the functional residual volume with electrical bioimpedance. Posttest blood gas analysis results were as follows: pH, 7.01; partial pressure of oxygen, 232.0mmHg; partial pressure of carbon dioxide, 66.9mmHg; and oxygen saturation, 99.0%. The apnea test without disconnection from the mechanical ventilator allowed the preservation of oxygenation in both cases. The use of continuous airway pressure during the apnea test seems to be a safe alternative in order to maintain alveolar recruitment and oxygenation during brain death determination.
Abstract
Rev Bras Ter Intensiva. 2020;32(2):319-325
DOI 10.5935/0103-507X.20200032
The apnea test, which involves disconnection from the mechanical ventilator, presents risks during the determination of brain death, especially in hypoxemic patients. We describe the performance of the apnea test without disconnection from the mechanical ventilator in two patients. The first case involved an 8-year-old boy admitted with severe hypoxemia due to pneumonia. He presented with cardiorespiratory arrest, followed by unresponsive coma due to hypoxic-ischemic encephalopathy. Two clinical exams revealed the absence of brainstem reflexes, and transcranial Doppler ultrasound revealed brain circulatory arrest. Three attempts were made to perform the apnea test, which were interrupted by hypoxemia; therefore, the apnea test was performed without disconnection from the mechanical ventilator, adjusting the continuous airway pressure to 10cmH2O and the inspired fraction of oxygen to 100%. The oxygen saturation was maintained at 100% for 10 minutes. Posttest blood gas analysis results were as follows: pH, 6.90; partial pressure of oxygen, 284.0mmHg; partial pressure of carbon dioxide, 94.0mmHg; and oxygen saturation, 100%. The second case involved a 43-year-old woman admitted with subarachnoid hemorrhage (Hunt-Hess V and Fisher IV). Two clinical exams revealed unresponsive coma and absence of all brainstem reflexes. Brain scintigraphy showed no radioisotope uptake into the brain parenchyma. The first attempt at the apnea test was stopped after 5 minutes due to hypothermia (34.9°C). After rewarming, the apnea test was repeated without disconnection from the mechanical ventilator, showing maintenance of the functional residual volume with electrical bioimpedance. Posttest blood gas analysis results were as follows: pH, 7.01; partial pressure of oxygen, 232.0mmHg; partial pressure of carbon dioxide, 66.9mmHg; and oxygen saturation, 99.0%. The apnea test without disconnection from the mechanical ventilator allowed the preservation of oxygenation in both cases. The use of continuous airway pressure during the apnea test seems to be a safe alternative in order to maintain alveolar recruitment and oxygenation during brain death determination.
Abstract
Rev Bras Ter Intensiva. 2019;31(1):106-110
DOI 10.5935/0103-507X.20190015
We report the case of a patient in whom brain death was suspected and associated with atelectasis and moderate to severe hypoxemia even though the patient was subjected to protective ventilation, a closed tracheal suction system, positive end-expiratory pressure, and recruitment maneuvers. Faced with the failure to obtain an adequate partial pressure of oxygen for the apnea test, we elected to place the patient in a prone position, use higher positive end-expiratory pressure, perform a new recruitment maneuver, and ventilate with a higher tidal volume (8mL/kg) without exceeding the plateau pressure of 30cmH2O. The apnea test was performed with the patient in a prone position, with continuous positive airway pressure coupled with a T-piece. The delay in diagnosis was 10 hours, and organ donation was not possible due to circulatory arrest. This report demonstrates the difficulties in obtaining higher levels of the partial pressure of oxygen for the apnea test. The delays in the diagnosis of brain death and in the organ donation process are discussed, as well as potential strategies to optimize the partial pressure of oxygen to perform the apnea test according to the current recommendations.
Abstract
Rev Bras Ter Intensiva. 2019;31(1):106-110
DOI 10.5935/0103-507X.20190015
We report the case of a patient in whom brain death was suspected and associated with atelectasis and moderate to severe hypoxemia even though the patient was subjected to protective ventilation, a closed tracheal suction system, positive end-expiratory pressure, and recruitment maneuvers. Faced with the failure to obtain an adequate partial pressure of oxygen for the apnea test, we elected to place the patient in a prone position, use higher positive end-expiratory pressure, perform a new recruitment maneuver, and ventilate with a higher tidal volume (8mL/kg) without exceeding the plateau pressure of 30cmH2O. The apnea test was performed with the patient in a prone position, with continuous positive airway pressure coupled with a T-piece. The delay in diagnosis was 10 hours, and organ donation was not possible due to circulatory arrest. This report demonstrates the difficulties in obtaining higher levels of the partial pressure of oxygen for the apnea test. The delays in the diagnosis of brain death and in the organ donation process are discussed, as well as potential strategies to optimize the partial pressure of oxygen to perform the apnea test according to the current recommendations.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (116) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)