
You searched for:"Ederlon Rezende"
We found (15) results for your search.-
Commentary
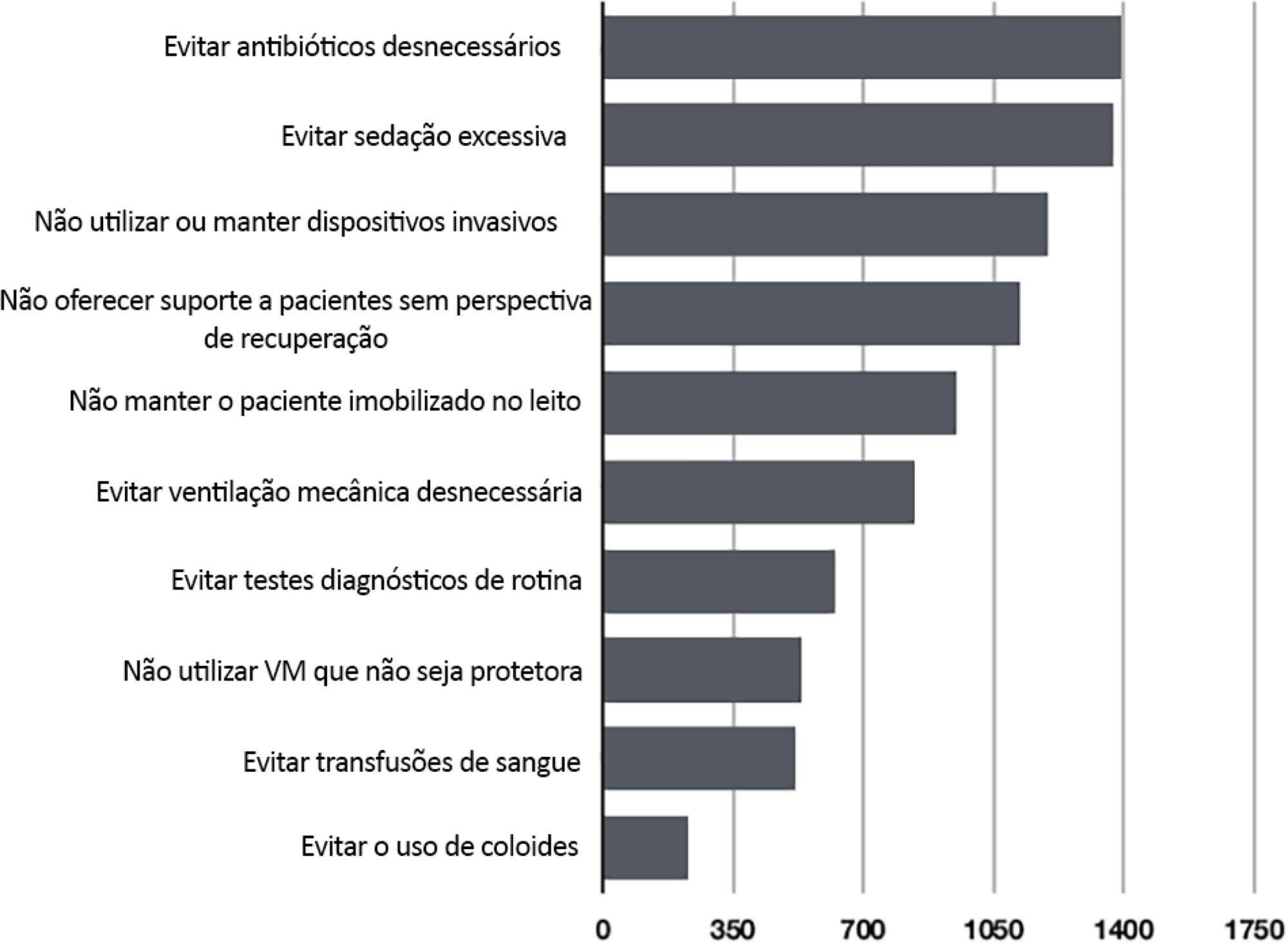
Choosing Wisely in intensive care medicine
Rev Bras Ter Intensiva. 2020;32(1):11-13
Abstract
Views1

Abstract
-
Commentary
Mortality due to sepsis in Brazil in a real scenario: the Brazilian ICUs project
Rev Bras Ter Intensiva. 2019;31(1):1-4
Abstract
CommentaryMortality due to sepsis in Brazil in a real scenario: the Brazilian ICUs project
Rev Bras Ter Intensiva. 2019;31(1):1-4
DOI 10.5935/0103-507X.20190008
Views1Worldwide, the number of sepsis patients per year is estimated at 15 to 17 million, contributing to more than 5 million deaths annually.(–) In Brazil, recent publications have indicated an increase in the number of cases of this syndrome in late years.() Many factors have contributed to this trend, such as population growth and rising […]See moreViews1Abstract
CommentaryMortality due to sepsis in Brazil in a real scenario: the Brazilian ICUs project
Rev Bras Ter Intensiva. 2019;31(1):1-4
DOI 10.5935/0103-507X.20190008
Views1Worldwide, the number of sepsis patients per year is estimated at 15 to 17 million, contributing to more than 5 million deaths annually.(–) In Brazil, recent publications have indicated an increase in the number of cases of this syndrome in late years.() Many factors have contributed to this trend, such as population growth and rising […]See more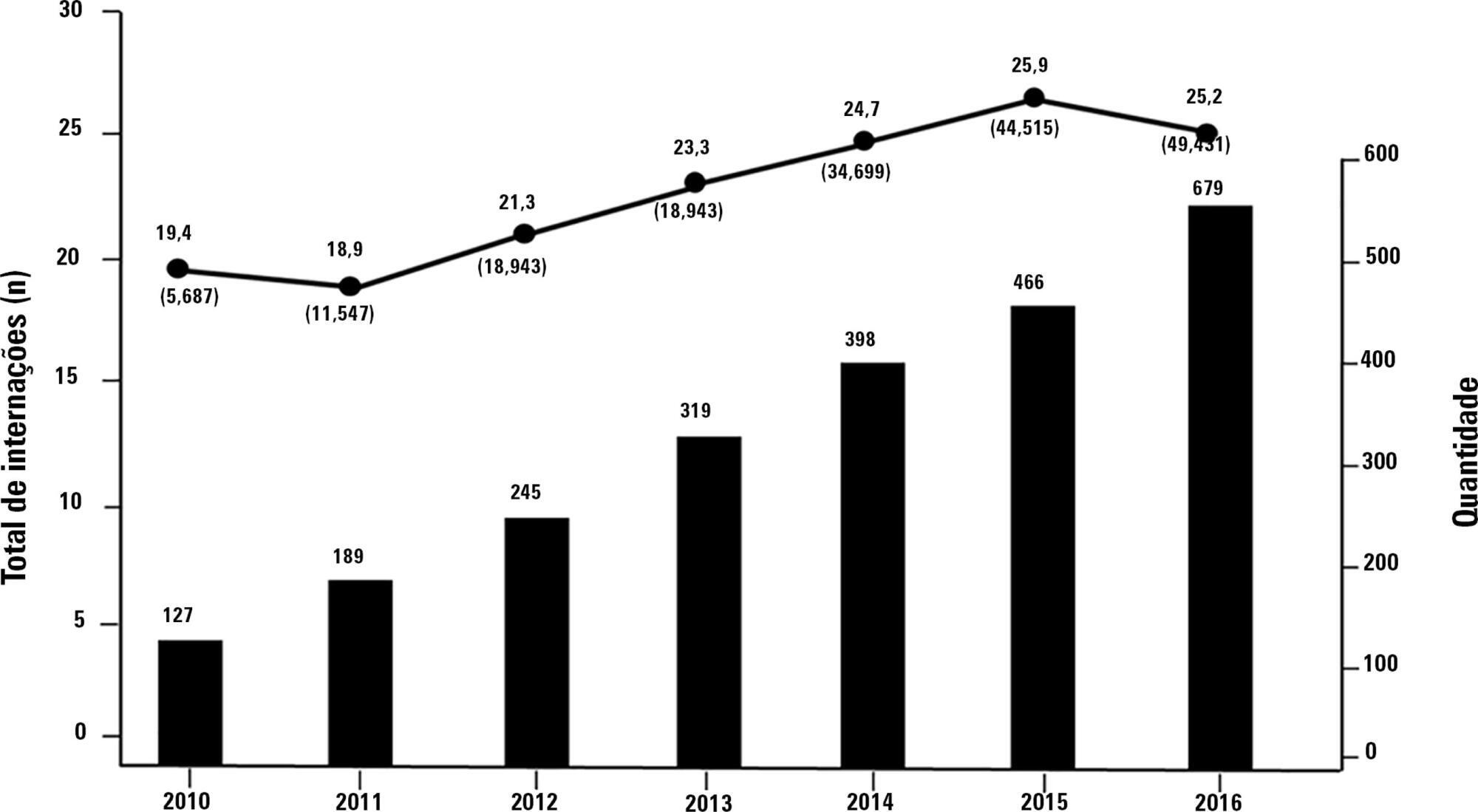
-
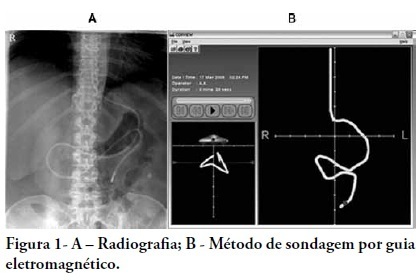
Effectiveness of post-pyloric tube placement using magnetic guidance
Rev Bras Ter Intensiva. 2011;23(1):49-55
Abstract
Effectiveness of post-pyloric tube placement using magnetic guidance
Rev Bras Ter Intensiva. 2011;23(1):49-55
DOI 10.1590/S0103-507X2011000100009
Views0See moreOBJECTIVE: Appropriate nutritional support is important to the outcomes of critically ill patients. However, a significant portion of these patients experience intestinal motility problems. Administration of enteral nutrition by means of tubes placed in the post-pyloric position has been suggested to improve the nutrition tolerance. The aim of this study was to compare the rate of successful post-pyloric placement using a real-time electromagnetic positioning device to the success rate using the conventional placement method. METHODS: This was a prospective, randomized and controlled study, conducted in a tertiary hospital over a period of three months. The patients were randomized to one of two groups: electromagnetically guided system group, whose patients underwent real-time monitoring of post-pyloric tube placement; or the control group, whose patients underwent tube placment using to the conventional blinded technique. The rates of successful post-pyloric placement and the procedure times were assessed and compared between the groups. RESULTS: Thirty-seven patients were enrolled, 18 in the electromagnetic group and 19 in the control group. The final tube position was evaluated using radiography. The electromagnetic guided group showed better success rates and shorter procedure times when compared to the control group. Additionally, in the electromagnetic guided group, higher pH values were found in the fluids aspirated from the probe, suggesting successful postpyloric placement. CONCLUSION: The electromagnetically guided method provided better placement accuracy than did the conventional technique.
Views0Abstract
Effectiveness of post-pyloric tube placement using magnetic guidance
Rev Bras Ter Intensiva. 2011;23(1):49-55
DOI 10.1590/S0103-507X2011000100009
Views0See moreOBJECTIVE: Appropriate nutritional support is important to the outcomes of critically ill patients. However, a significant portion of these patients experience intestinal motility problems. Administration of enteral nutrition by means of tubes placed in the post-pyloric position has been suggested to improve the nutrition tolerance. The aim of this study was to compare the rate of successful post-pyloric placement using a real-time electromagnetic positioning device to the success rate using the conventional placement method. METHODS: This was a prospective, randomized and controlled study, conducted in a tertiary hospital over a period of three months. The patients were randomized to one of two groups: electromagnetically guided system group, whose patients underwent real-time monitoring of post-pyloric tube placement; or the control group, whose patients underwent tube placment using to the conventional blinded technique. The rates of successful post-pyloric placement and the procedure times were assessed and compared between the groups. RESULTS: Thirty-seven patients were enrolled, 18 in the electromagnetic group and 19 in the control group. The final tube position was evaluated using radiography. The electromagnetic guided group showed better success rates and shorter procedure times when compared to the control group. Additionally, in the electromagnetic guided group, higher pH values were found in the fluids aspirated from the probe, suggesting successful postpyloric placement. CONCLUSION: The electromagnetically guided method provided better placement accuracy than did the conventional technique.
-
Letters to the Editor Rev Bras Ter Intensiva. 2011;23(1):113-113
-
Original Articles
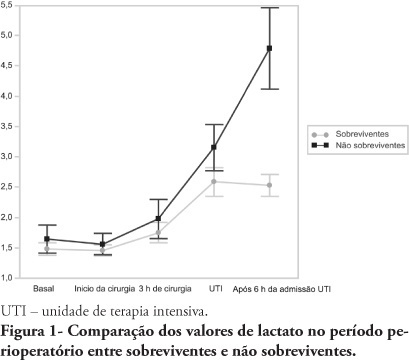
Intraoperative lactate measurements are not predictive of death in high risk surgical patients
Rev Bras Ter Intensiva. 2010;22(3):229-235
Abstract
Original ArticlesIntraoperative lactate measurements are not predictive of death in high risk surgical patients
Rev Bras Ter Intensiva. 2010;22(3):229-235
DOI 10.1590/S0103-507X2010000300003
Views0See moreOBJECTIVES: An increased lactate level is classically considered a marker for poorer prognosis, however little information is available on intraoperative lactate’s kinetics and its connection with prognosis. This study aimed to evaluate the time when perioperative lactate is most relevant for prognosis. METHODS: This was an observational prospective study conducted in a tertiary hospital. Patients with requested intensive care unit postoperative stay, aged > 18 years, undergoing major surgery were included. Palliative surgery patients and those with heart and/or severe liver failure were excluded. Arterial lactate levels were measured immediately before the surgery start (T0), after anesthesia induction (T1), 3 hours after the surgery start (T2), intensive care unit admission (T3) and 6 hours after the intensive care unit admission (T4). RESULTS: Sixty seven patients were included. The mean lactate values for the patients’ T0, T1, T2 and T4 were 1.5 ± 0.8 mmol/L, 1.5 ± 0.7 mmol/L, 1.8 ± 1.2 mmol/L, 2.7 ± 1.7 mmol/L and 3.1 ± 2.0 mmol/L, respectively. The hospital mortality rate was 25.8%, and surviving and non-surviving patients lactate values in the intensive care unit were 2.5 ± 1. and 4.8 ± 2.8 mmol/L (P < 0.0001), respectively. The other times measurements showed no statistically significant differences between the groups. CONCLUSIONS: In surgical patients, intraoperative arterial lactate levels failed to show a predictive value; however during the postoperative period, this assessment was shown to be useful for hospital mortality prediction.
Views0Abstract
Original ArticlesIntraoperative lactate measurements are not predictive of death in high risk surgical patients
Rev Bras Ter Intensiva. 2010;22(3):229-235
DOI 10.1590/S0103-507X2010000300003
Views0See moreOBJECTIVES: An increased lactate level is classically considered a marker for poorer prognosis, however little information is available on intraoperative lactate’s kinetics and its connection with prognosis. This study aimed to evaluate the time when perioperative lactate is most relevant for prognosis. METHODS: This was an observational prospective study conducted in a tertiary hospital. Patients with requested intensive care unit postoperative stay, aged > 18 years, undergoing major surgery were included. Palliative surgery patients and those with heart and/or severe liver failure were excluded. Arterial lactate levels were measured immediately before the surgery start (T0), after anesthesia induction (T1), 3 hours after the surgery start (T2), intensive care unit admission (T3) and 6 hours after the intensive care unit admission (T4). RESULTS: Sixty seven patients were included. The mean lactate values for the patients’ T0, T1, T2 and T4 were 1.5 ± 0.8 mmol/L, 1.5 ± 0.7 mmol/L, 1.8 ± 1.2 mmol/L, 2.7 ± 1.7 mmol/L and 3.1 ± 2.0 mmol/L, respectively. The hospital mortality rate was 25.8%, and surviving and non-surviving patients lactate values in the intensive care unit were 2.5 ± 1. and 4.8 ± 2.8 mmol/L (P < 0.0001), respectively. The other times measurements showed no statistically significant differences between the groups. CONCLUSIONS: In surgical patients, intraoperative arterial lactate levels failed to show a predictive value; however during the postoperative period, this assessment was shown to be useful for hospital mortality prediction.
-
Original Articles
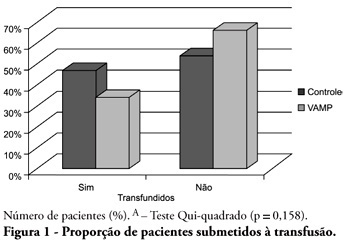
Closed system for blood sampling and transfusion in critically ill patients
Rev Bras Ter Intensiva. 2010;22(1):5-10
Abstract
Original ArticlesClosed system for blood sampling and transfusion in critically ill patients
Rev Bras Ter Intensiva. 2010;22(1):5-10
DOI 10.1590/S0103-507X2010000100003
Views0See moreOBJECTIVE: Anemia is common in severely ill patients, and blood sampling plays a relevant causative role. Consequently, blood transfusions are frequent an related to several complications. Trying to reduce the transfusion-related risk, minimizing blood loss is mandatory. Thus, this work aimed to evaluate a closed blood sampling system as a strategy to spare unnecessary blood losses and transfusions. METHODS: This was a prospective, randomized, controlled, multicenter, 6 months, clinical trial. The patients were assigned to either VAMP (Venous Arterial Blood Management Protection) group, using a closed blood sampling system, or control group. The groups’ transfusion rate, as well as hemoglobin (Hb) and Hematocrit (Ht) changes were compared for 14 days. RESULTS: Were included 127 patients, 65 assigned to the control group, and 62 to VAMP. During the intensive care unit stay, both groups experienced both hemoglobin and hematocrit drops. However, when the final Ht and Hb were compared between the groups, a difference was identified with higher values in the VAMP group (p=0.03; p=0.006, respectively). No statistical difference was found for both groups transfusion rates, although the VAMP group had an absolute 12% blood transfusion reduction. CONCLUSION: The use of a closed blood sampling system was able to minimize blood count values changes, however failed to reduce transfusions rate.
Views0Abstract
Original ArticlesClosed system for blood sampling and transfusion in critically ill patients
Rev Bras Ter Intensiva. 2010;22(1):5-10
DOI 10.1590/S0103-507X2010000100003
Views0See moreOBJECTIVE: Anemia is common in severely ill patients, and blood sampling plays a relevant causative role. Consequently, blood transfusions are frequent an related to several complications. Trying to reduce the transfusion-related risk, minimizing blood loss is mandatory. Thus, this work aimed to evaluate a closed blood sampling system as a strategy to spare unnecessary blood losses and transfusions. METHODS: This was a prospective, randomized, controlled, multicenter, 6 months, clinical trial. The patients were assigned to either VAMP (Venous Arterial Blood Management Protection) group, using a closed blood sampling system, or control group. The groups’ transfusion rate, as well as hemoglobin (Hb) and Hematocrit (Ht) changes were compared for 14 days. RESULTS: Were included 127 patients, 65 assigned to the control group, and 62 to VAMP. During the intensive care unit stay, both groups experienced both hemoglobin and hematocrit drops. However, when the final Ht and Hb were compared between the groups, a difference was identified with higher values in the VAMP group (p=0.03; p=0.006, respectively). No statistical difference was found for both groups transfusion rates, although the VAMP group had an absolute 12% blood transfusion reduction. CONCLUSION: The use of a closed blood sampling system was able to minimize blood count values changes, however failed to reduce transfusions rate.
-
Prognostic factors in elderly patients admitted in the intensive care unit
Rev Bras Ter Intensiva. 2009;21(3):255-261
Abstract
Prognostic factors in elderly patients admitted in the intensive care unit
Rev Bras Ter Intensiva. 2009;21(3):255-261
DOI 10.1590/S0103-507X2009000300004
Views0See moreCurrently, aging of the population is a widespread global phenomenon. Therefore, the assessment of prognosis in elderly patients is needed. This study aims to identify risk factors in a population of elderly patients admitted in the intensive care unit METHODS: A prospective study in the intensive care unit of a general tertiary hospital was carried out for five months. Patients with 65 years or more of age, who stayed in the intensive care unit for 24 hours or more were included and those at the-end-of-life, patients readmitted to intensive care unit during the same hospital stay were excluded. RESULTS: In this study 199 patients were involved, with a mean age of 75.4±6.8 years, and 58.8% were female. Mortality was 57.3%. The mean APACHE II, SOFA, MODS and Katz index (assessment of daily activities) were respectively 20.0±5.8, 6.8±3.9, 2.4±1.9 and 5.3±1.6. Most patients were postoperative 59.3% and 41.6% were under invasive mechanical ventilation. At regression analysis, the independent determinants of higher mortality were: older age (76.9±6.7 years death versus 73.3±6.5 years discharge, P<0.001, OR=1.08, CI 95% 1.01-1. 16), the Katz index (4.9±1.9 deaths versus 5.7±0.9 discharge, p=0.001, OR=0.66, CI 95% 0.45-0.98), hyperglycemia (158.1±69.0 death versus 139.6±48.5 discharge p=0.041; OR=1.02; CI 95% 1.01-1.03) and need for mechanical ventilation at admission to the intensive care unit (57.0% death versus 20.5% discharge p <0.001, OR=3.57, CI 95% 1.24-10.3). CONCLUSION: Elderly patients admitted to the intensive care unit that have difficulties in performing daily activities, hyperglycemia and who are under invasive mechanical ventilation had a worse hospital prognosis.
Views0Abstract
Prognostic factors in elderly patients admitted in the intensive care unit
Rev Bras Ter Intensiva. 2009;21(3):255-261
DOI 10.1590/S0103-507X2009000300004
Views0See moreCurrently, aging of the population is a widespread global phenomenon. Therefore, the assessment of prognosis in elderly patients is needed. This study aims to identify risk factors in a population of elderly patients admitted in the intensive care unit METHODS: A prospective study in the intensive care unit of a general tertiary hospital was carried out for five months. Patients with 65 years or more of age, who stayed in the intensive care unit for 24 hours or more were included and those at the-end-of-life, patients readmitted to intensive care unit during the same hospital stay were excluded. RESULTS: In this study 199 patients were involved, with a mean age of 75.4±6.8 years, and 58.8% were female. Mortality was 57.3%. The mean APACHE II, SOFA, MODS and Katz index (assessment of daily activities) were respectively 20.0±5.8, 6.8±3.9, 2.4±1.9 and 5.3±1.6. Most patients were postoperative 59.3% and 41.6% were under invasive mechanical ventilation. At regression analysis, the independent determinants of higher mortality were: older age (76.9±6.7 years death versus 73.3±6.5 years discharge, P<0.001, OR=1.08, CI 95% 1.01-1. 16), the Katz index (4.9±1.9 deaths versus 5.7±0.9 discharge, p=0.001, OR=0.66, CI 95% 0.45-0.98), hyperglycemia (158.1±69.0 death versus 139.6±48.5 discharge p=0.041; OR=1.02; CI 95% 1.01-1.03) and need for mechanical ventilation at admission to the intensive care unit (57.0% death versus 20.5% discharge p <0.001, OR=3.57, CI 95% 1.24-10.3). CONCLUSION: Elderly patients admitted to the intensive care unit that have difficulties in performing daily activities, hyperglycemia and who are under invasive mechanical ventilation had a worse hospital prognosis.
-
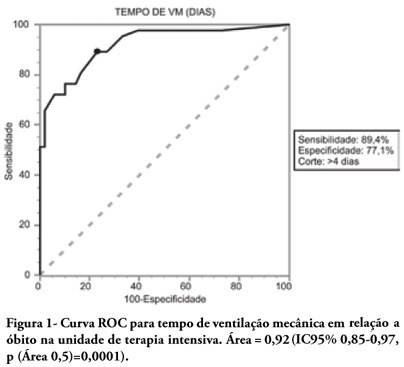
Aged patients with respiratory dysfunction: epidemiological profile and mortality risk factors
Rev Bras Ter Intensiva. 2009;21(3):262-268
Abstract
Aged patients with respiratory dysfunction: epidemiological profile and mortality risk factors
Rev Bras Ter Intensiva. 2009;21(3):262-268
DOI 10.1590/S0103-507X2009000300005
Views0See moreOBJECTIVES: To describe the population of aged as compared to young patients under mechanical ventilation and to analyze the mortality risk factors of this group in an intensive care unit. METHODS: This was a prospective observational trial in patients over 18 years of age, admitted in an intensive care unit and under mechanical ventilation, during one year. Patients were divided into two groups according to age: Group 1 – patients over 65 years old; and Group 2, 65 years old or younger. RESULTS: eighty one mechanic ventilation patients were included, 62 aged and 18 younger, mean ages from aged was 76 years, while in the younger it was 56 years. As compared to the control, aged patients had longer mechanic ventilation time , higher intensive care unit and hospital mortality: 63.1% versus 26.3% and 74.2% versus 47.4% (P<0.05), respectively. In addition, the aged under mechanic ventilation had increased desintubation failures, difficult ventilatory weaning and deaths directly related to respiratory dysfunction. The mechanic ventilation time was an independent risk factor for death in the intensive care unit in aged patients (OR= 2.7, p=0.02). The area under the ROC curve of mechanic ventilation about intensive care unit death was 0.92 (95% CI 0.85-0.97, p (area 0.5)=0.0001), cutoff point of 4 days, sensitivity 89.4% and specificity 77.1%. CONCLUSIONS: Mechanic ventilation patients over 65years of age have a worse prognosis than the younger, and the longer the mechanic ventilation time, the higher will be intensive care mortality.
Views0Abstract
Aged patients with respiratory dysfunction: epidemiological profile and mortality risk factors
Rev Bras Ter Intensiva. 2009;21(3):262-268
DOI 10.1590/S0103-507X2009000300005
Views0See moreOBJECTIVES: To describe the population of aged as compared to young patients under mechanical ventilation and to analyze the mortality risk factors of this group in an intensive care unit. METHODS: This was a prospective observational trial in patients over 18 years of age, admitted in an intensive care unit and under mechanical ventilation, during one year. Patients were divided into two groups according to age: Group 1 – patients over 65 years old; and Group 2, 65 years old or younger. RESULTS: eighty one mechanic ventilation patients were included, 62 aged and 18 younger, mean ages from aged was 76 years, while in the younger it was 56 years. As compared to the control, aged patients had longer mechanic ventilation time , higher intensive care unit and hospital mortality: 63.1% versus 26.3% and 74.2% versus 47.4% (P<0.05), respectively. In addition, the aged under mechanic ventilation had increased desintubation failures, difficult ventilatory weaning and deaths directly related to respiratory dysfunction. The mechanic ventilation time was an independent risk factor for death in the intensive care unit in aged patients (OR= 2.7, p=0.02). The area under the ROC curve of mechanic ventilation about intensive care unit death was 0.92 (95% CI 0.85-0.97, p (area 0.5)=0.0001), cutoff point of 4 days, sensitivity 89.4% and specificity 77.1%. CONCLUSIONS: Mechanic ventilation patients over 65years of age have a worse prognosis than the younger, and the longer the mechanic ventilation time, the higher will be intensive care mortality.
Search
Search in:
KEY WORDS
Case reports Child Coronavirus infections COVID-19 Critical care Critical illness Extracorporeal membrane oxygenation Infant, newborn Intensive care Intensive care units Intensive care units, pediatric mechanical ventilation Mortality Physical therapy modalities Prognosis Respiration, artificial Respiratory insufficiency risk factors SARS-CoV-2 Sepsis