Sodium Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2019;31(2):202-209
DOI 10.5935/0103-507X.20190032
To evaluate the effects of intravenous infusion of fluids and sodium on the first day of admission on infusion of enteral nutrition in the first 5 days in intensive care patients.
A prospective cohort study was conducted with critical nonsurgical patients admitted for at least 5 days who were on mechanical ventilation and receiving enteral nutrition. The amount of intravenous fluids and sodium infused on the first day and the volume of enteral nutrition infused in the first 5 days were investigated. The volume of intravenous fluids > 35mL/kg or ≤ 35mL/kg of body weight and sodium (above or below the 25th percentile) infused on the first day was compared with infused enteral nutrition.
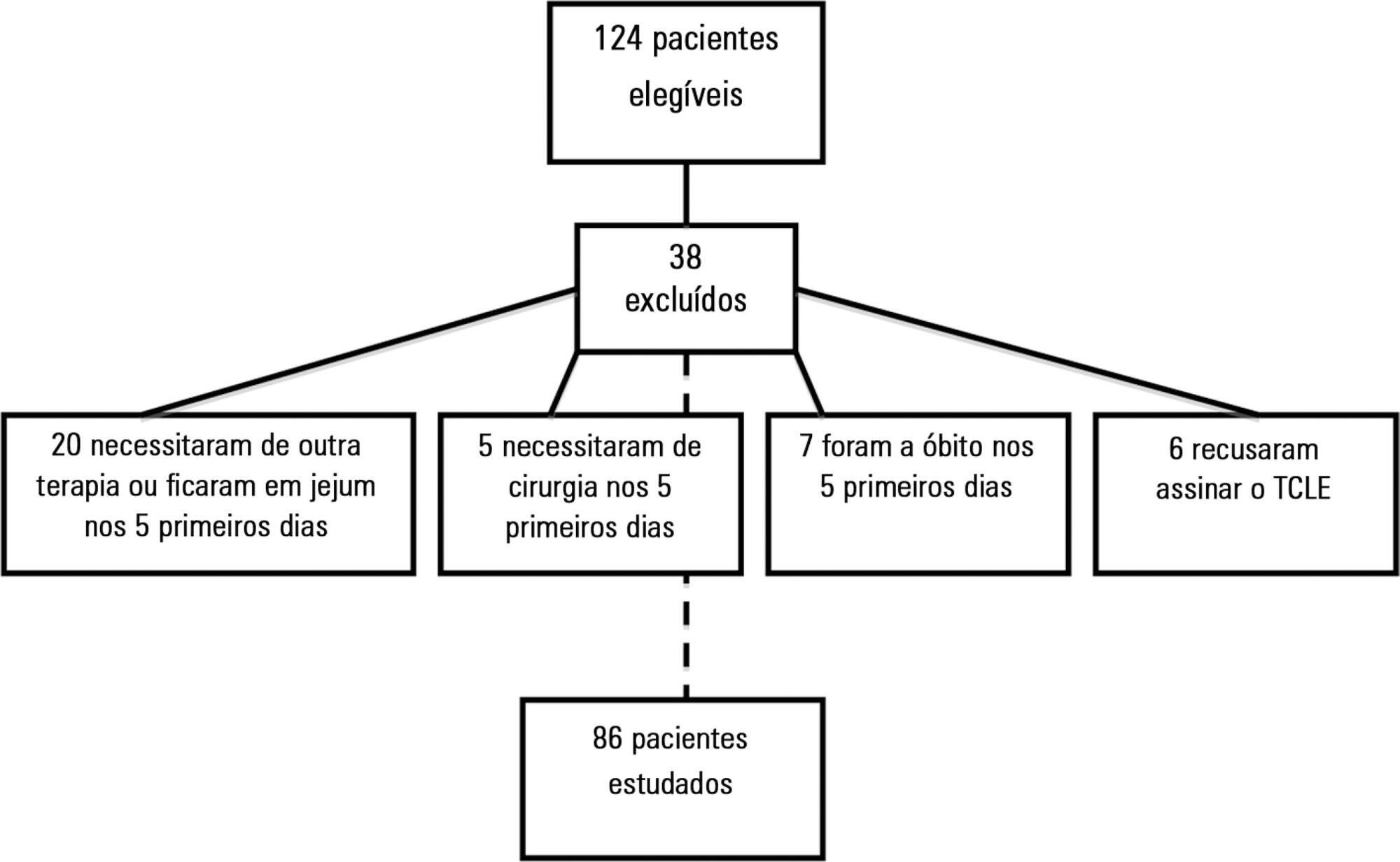
A total of 86 patients were studied, with a mean (± standard deviation) of 65 ± 17 years, of which 54.7% were female. On the first day, 3,393.7 ± 1,417.0mL of fluid (48.2 ± 23.0mL/kg) and 12.2 ± 5.1g of sodium were administered. Fifty-eight (67.4%) patients received more than 35mL/kg of fluids. In 5 days, 67 ± 19.8% (2,993.8 ± 1,324.4mL) of the prescribed enteral nutrition was received. Patients who received > 35mL/kg of intravenous fluids also received less enteral nutrition in 5 days (2,781.4 ± 1,337.9 versus 3,433.6 ± 1,202.2mL; p = 0.03) versus those who received ≤ 35mL/kg. Patients with intravenous sodium infusion above the 25th percentile (≥ 8.73g) on the first day received less enteral nutrition volume in 5 days (2,827.2 ± 1,398.0 versus 3,509.3 ± 911.9mL; p = 0.02).
The results of this study support the assumption that the administration of intravenous fluids > 35mL/kg and sodium ≥ 8.73g on the first day of hospitalization may contribute to the lower infusion of enteral nutrition in critically ill patients.
Abstract
Rev Bras Ter Intensiva. 2019;31(2):202-209
DOI 10.5935/0103-507X.20190032
To evaluate the effects of intravenous infusion of fluids and sodium on the first day of admission on infusion of enteral nutrition in the first 5 days in intensive care patients.
A prospective cohort study was conducted with critical nonsurgical patients admitted for at least 5 days who were on mechanical ventilation and receiving enteral nutrition. The amount of intravenous fluids and sodium infused on the first day and the volume of enteral nutrition infused in the first 5 days were investigated. The volume of intravenous fluids > 35mL/kg or ≤ 35mL/kg of body weight and sodium (above or below the 25th percentile) infused on the first day was compared with infused enteral nutrition.
A total of 86 patients were studied, with a mean (± standard deviation) of 65 ± 17 years, of which 54.7% were female. On the first day, 3,393.7 ± 1,417.0mL of fluid (48.2 ± 23.0mL/kg) and 12.2 ± 5.1g of sodium were administered. Fifty-eight (67.4%) patients received more than 35mL/kg of fluids. In 5 days, 67 ± 19.8% (2,993.8 ± 1,324.4mL) of the prescribed enteral nutrition was received. Patients who received > 35mL/kg of intravenous fluids also received less enteral nutrition in 5 days (2,781.4 ± 1,337.9 versus 3,433.6 ± 1,202.2mL; p = 0.03) versus those who received ≤ 35mL/kg. Patients with intravenous sodium infusion above the 25th percentile (≥ 8.73g) on the first day received less enteral nutrition volume in 5 days (2,827.2 ± 1,398.0 versus 3,509.3 ± 911.9mL; p = 0.02).
The results of this study support the assumption that the administration of intravenous fluids > 35mL/kg and sodium ≥ 8.73g on the first day of hospitalization may contribute to the lower infusion of enteral nutrition in critically ill patients.
Abstract
Rev Bras Ter Intensiva. 2016;28(2):154-160
DOI 10.5935/0103-507X.20160030
To evaluate the presence of hyponatremia and natriuresis and their association with atrial natriuretic factor in neurosurgery patients.
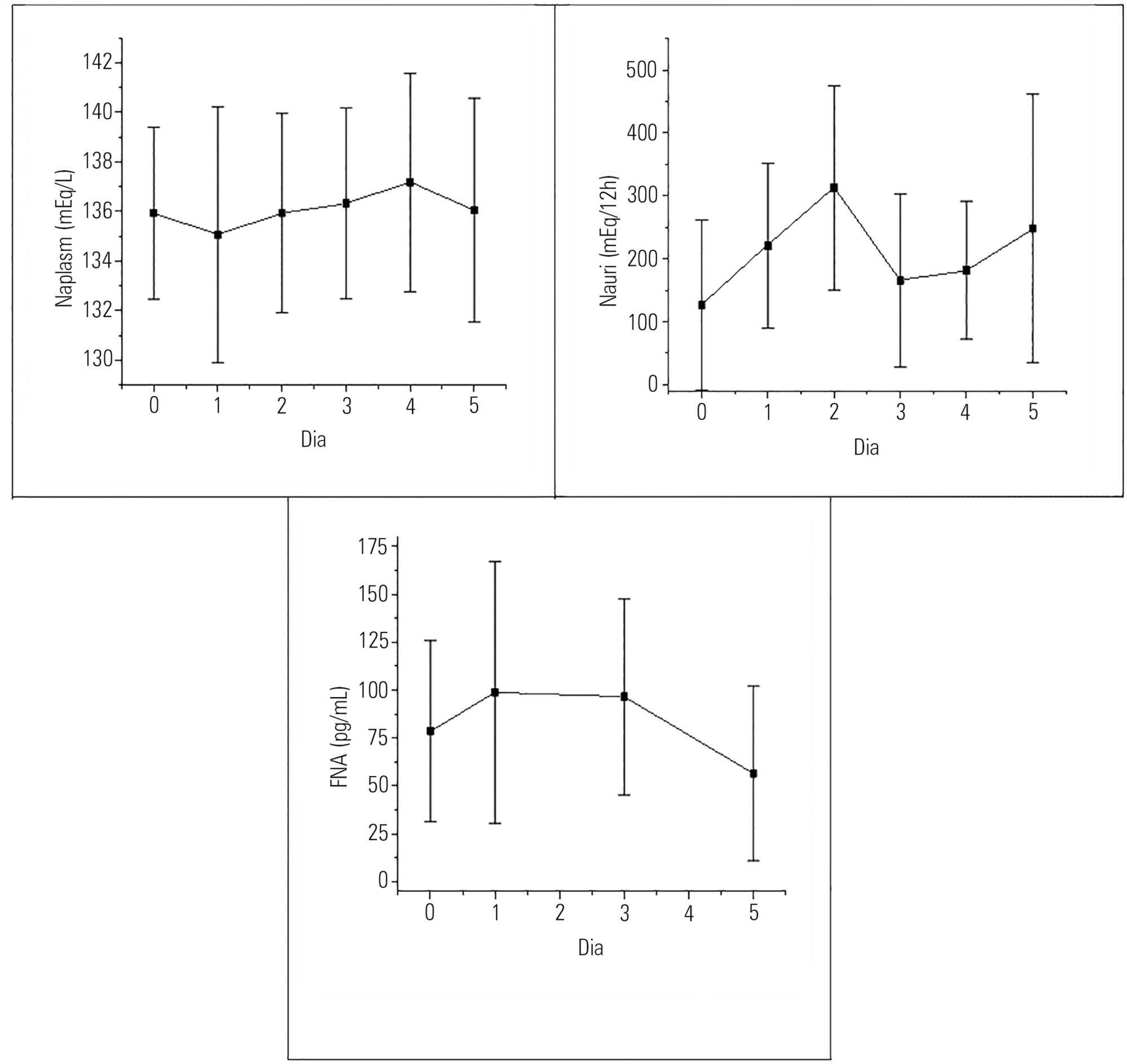
The study included 30 patients who had been submitted to intracranial tumor resection and cerebral aneurism clipping. Both plasma and urinary sodium and plasma atrial natriuretic factor were measured during the preoperative and postoperative time periods.
Hyponatremia was present in 63.33% of the patients, particularly on the first postoperative day. Natriuresis was present in 93.33% of the patients, particularly on the second postoperative day. Plasma atrial natriuretic factor was increased in 92.60% of the patients in at least one of the postoperative days; however, there was no statistically significant association between the atrial natriuretic factor and plasma sodium and between the atrial natriuretic factor and urinary sodium.
Hyponatremia and natriuresis were present in most patients after neurosurgery; however, the atrial natriuretic factor cannot be considered to be directly responsible for these alterations in neurosurgery patients. Other natriuretic factors are likely to be involved.
Abstract
Rev Bras Ter Intensiva. 2016;28(2):154-160
DOI 10.5935/0103-507X.20160030
To evaluate the presence of hyponatremia and natriuresis and their association with atrial natriuretic factor in neurosurgery patients.
The study included 30 patients who had been submitted to intracranial tumor resection and cerebral aneurism clipping. Both plasma and urinary sodium and plasma atrial natriuretic factor were measured during the preoperative and postoperative time periods.
Hyponatremia was present in 63.33% of the patients, particularly on the first postoperative day. Natriuresis was present in 93.33% of the patients, particularly on the second postoperative day. Plasma atrial natriuretic factor was increased in 92.60% of the patients in at least one of the postoperative days; however, there was no statistically significant association between the atrial natriuretic factor and plasma sodium and between the atrial natriuretic factor and urinary sodium.
Hyponatremia and natriuresis were present in most patients after neurosurgery; however, the atrial natriuretic factor cannot be considered to be directly responsible for these alterations in neurosurgery patients. Other natriuretic factors are likely to be involved.
Abstract
Rev Bras Ter Intensiva. 2016;28(2):120-131
DOI 10.5935/0103-507X.20160026
The aim of this study was to investigate the clinical and laboratorial factors associated with serum sodium variation during continuous renal replacement therapy and to assess whether the perfect admixture formula could predict 24-hour sodium variation.
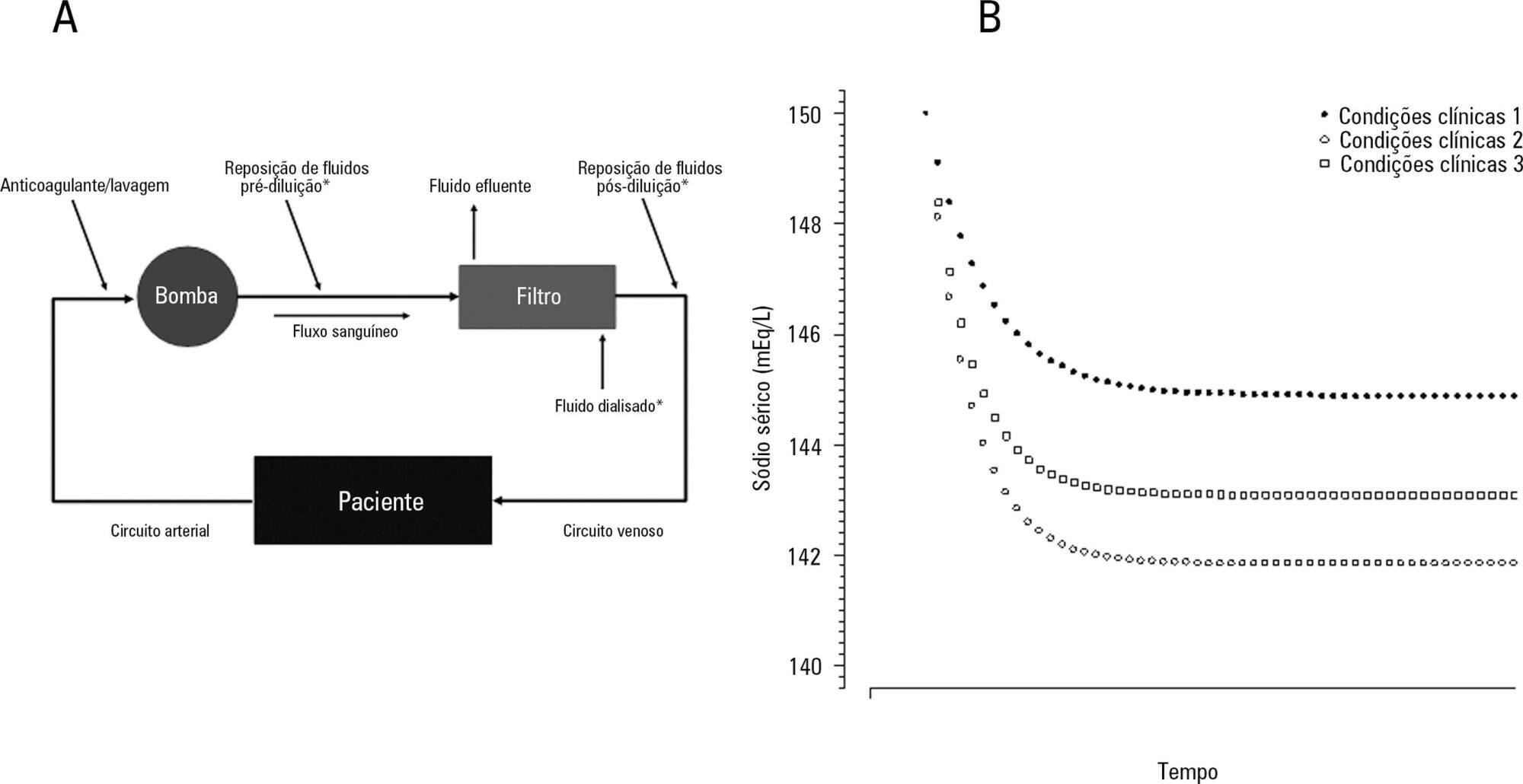
Thirty-six continuous renal replacement therapy sessions of 33 patients, in which the affluent prescription was unchanged during the first 24 hours, were retrieved from a prospective collected database and then analyzed. A mixed linear model was performed to investigate the factors associated with large serum sodium variations (≥ 8mEq/L), and a Bland-Altman plot was generated to assess the agreement between the predicted and observed variations.
In continuous renal replacement therapy 24-hour sessions, SAPS 3 (p = 0.022) and baseline hypernatremia (p = 0.023) were statistically significant predictors of serum sodium variations ≥ 8mEq/L in univariate analysis, but only hypernatremia demonstrated an independent association (β = 0.429, p < 0.001). The perfect admixture formula for sodium prediction at 24 hours demonstrated poor agreement with the observed values.
Hypernatremia at the time of continuous renal replacement therapy initiation is an important factor associated with clinically significant serum sodium variation. The use of 4% citrate or acid citrate dextrose - formula A 2.2% as anticoagulants was not associated with higher serum sodium variations. A mathematical prediction for the serum sodium concentration after 24 hours was not feasible.
Abstract
Rev Bras Ter Intensiva. 2016;28(2):120-131
DOI 10.5935/0103-507X.20160026
The aim of this study was to investigate the clinical and laboratorial factors associated with serum sodium variation during continuous renal replacement therapy and to assess whether the perfect admixture formula could predict 24-hour sodium variation.
Thirty-six continuous renal replacement therapy sessions of 33 patients, in which the affluent prescription was unchanged during the first 24 hours, were retrieved from a prospective collected database and then analyzed. A mixed linear model was performed to investigate the factors associated with large serum sodium variations (≥ 8mEq/L), and a Bland-Altman plot was generated to assess the agreement between the predicted and observed variations.
In continuous renal replacement therapy 24-hour sessions, SAPS 3 (p = 0.022) and baseline hypernatremia (p = 0.023) were statistically significant predictors of serum sodium variations ≥ 8mEq/L in univariate analysis, but only hypernatremia demonstrated an independent association (β = 0.429, p < 0.001). The perfect admixture formula for sodium prediction at 24 hours demonstrated poor agreement with the observed values.
Hypernatremia at the time of continuous renal replacement therapy initiation is an important factor associated with clinically significant serum sodium variation. The use of 4% citrate or acid citrate dextrose - formula A 2.2% as anticoagulants was not associated with higher serum sodium variations. A mathematical prediction for the serum sodium concentration after 24 hours was not feasible.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (116) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)