Blood pressure Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2017;29(4):490-498
DOI 10.5935/0103-507X.20170068
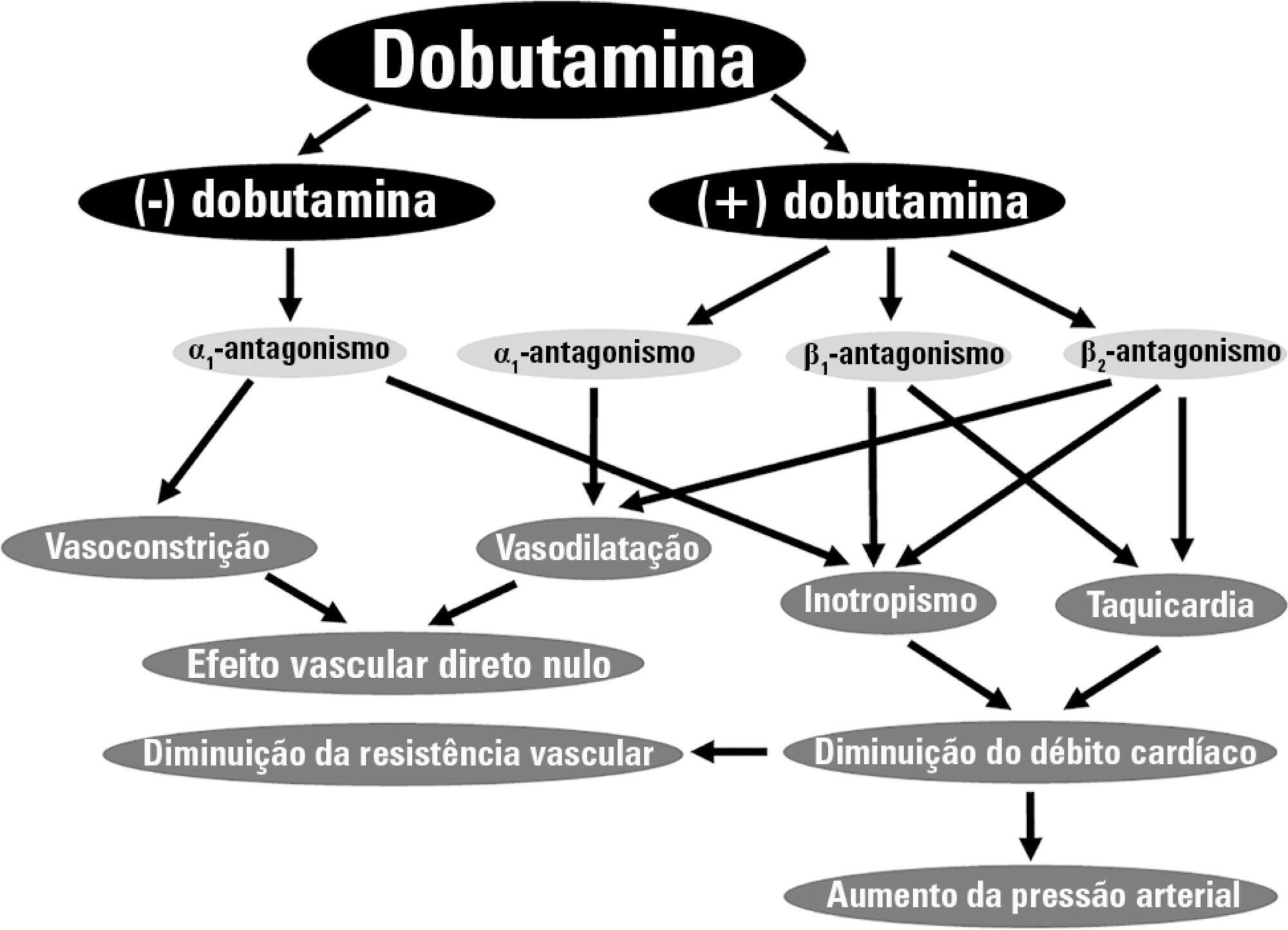
Dobutamine is the inotrope most commonly used in septic shock patients to increase cardiac output and correct hypoperfusion. Although some experimental and clinical studies have shown that dobutamine can improve systemic and regional hemodynamics, other research has found that its effects are heterogenous and unpredictable. In this review, we analyze the pharmacodynamic properties of dobutamine and its physiologic effects. Our goal is to show that the effects of dobutamine might differ between healthy subjects, in experimental and clinical cardiac failure, in animal models and in patients with septic shock. We discuss evidence supporting the claim that dobutamine, in septic shock, frequently behaves as a chronotropic and vasodilatory drug, without evidence of inotropic action. Since the side effects are very common, and the therapeutic benefits are unclear, we suggest that dobutamine should be used cautiously in septic shock. Before a definitive therapeutic decision, the efficacy and tolerance of dobutamine should be assessed during a brief time with close monitoring of its positive and negative side effects.
Abstract
Rev Bras Ter Intensiva. 2017;29(4):490-498
DOI 10.5935/0103-507X.20170068
Dobutamine is the inotrope most commonly used in septic shock patients to increase cardiac output and correct hypoperfusion. Although some experimental and clinical studies have shown that dobutamine can improve systemic and regional hemodynamics, other research has found that its effects are heterogenous and unpredictable. In this review, we analyze the pharmacodynamic properties of dobutamine and its physiologic effects. Our goal is to show that the effects of dobutamine might differ between healthy subjects, in experimental and clinical cardiac failure, in animal models and in patients with septic shock. We discuss evidence supporting the claim that dobutamine, in septic shock, frequently behaves as a chronotropic and vasodilatory drug, without evidence of inotropic action. Since the side effects are very common, and the therapeutic benefits are unclear, we suggest that dobutamine should be used cautiously in septic shock. Before a definitive therapeutic decision, the efficacy and tolerance of dobutamine should be assessed during a brief time with close monitoring of its positive and negative side effects.
Abstract
Rev Bras Ter Intensiva. 2009;21(4):349-352
DOI 10.1590/S0103-507X2009000400003
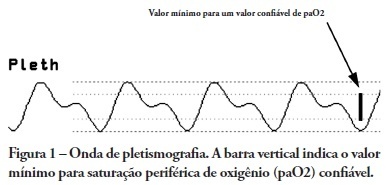
OBJECTIVES: Arterial pulse pressure respiratory variation is a good predictor of fluid response in ventilated patients. Recently, it was shown that respiratory variation in arterial pulse pressure correlates with variation in pulse oximetry plethysmographic waveform amplitude. We wanted to evaluate the correlation between respiratory variation in arterial pulse pressure and respiratory variation in pulse oximetry plethysmographic waveform amplitude, and to determine whether this correlation was influenced by norepinephrine administration. METHODS: Prospective study of sixty patients with normal sinus rhythm on mechanical ventilation, profoundly sedated and with stable hemodynamics. Oxygenation index and invasive arterial pressure were monitored. Respiratory variation in arterial pulse pressure and respiratory variation in pulse oximetry plethysmographic waveform amplitude were recorded simultaneously in a beat-to-beat evaluation, and were compared using the Pearson coefficient of agreement and linear regression. RESULTS: Thirty patients (50%) required norepinephrine. There was a significant correlation (K = 0.66; p < 0.001) between respiratory variation in arterial pulse pressure and respiratory variation in pulse oximetry plethysmographic waveform amplitude. Area under the ROC curve was 0.88 (range, 0.79 - 0.97), with a best cutoff value of 14% to predict a respiratory variation in arterial pulse pressure of 13. The use of norepinephrine did not influence the correlation (K = 0.63, p = 0.001, respectively). CONCLUSIONS: Respiratory variation in arterial pulse pressure above 13% can be accurately predicted by a respiratory variation in pulse oximetry plethysmographic waveform amplitude of 14%. The use of norepinephrine does not alter this relationship.
Abstract
Rev Bras Ter Intensiva. 2009;21(4):349-352
DOI 10.1590/S0103-507X2009000400003
OBJECTIVES: Arterial pulse pressure respiratory variation is a good predictor of fluid response in ventilated patients. Recently, it was shown that respiratory variation in arterial pulse pressure correlates with variation in pulse oximetry plethysmographic waveform amplitude. We wanted to evaluate the correlation between respiratory variation in arterial pulse pressure and respiratory variation in pulse oximetry plethysmographic waveform amplitude, and to determine whether this correlation was influenced by norepinephrine administration. METHODS: Prospective study of sixty patients with normal sinus rhythm on mechanical ventilation, profoundly sedated and with stable hemodynamics. Oxygenation index and invasive arterial pressure were monitored. Respiratory variation in arterial pulse pressure and respiratory variation in pulse oximetry plethysmographic waveform amplitude were recorded simultaneously in a beat-to-beat evaluation, and were compared using the Pearson coefficient of agreement and linear regression. RESULTS: Thirty patients (50%) required norepinephrine. There was a significant correlation (K = 0.66; p < 0.001) between respiratory variation in arterial pulse pressure and respiratory variation in pulse oximetry plethysmographic waveform amplitude. Area under the ROC curve was 0.88 (range, 0.79 - 0.97), with a best cutoff value of 14% to predict a respiratory variation in arterial pulse pressure of 13. The use of norepinephrine did not influence the correlation (K = 0.63, p = 0.001, respectively). CONCLUSIONS: Respiratory variation in arterial pulse pressure above 13% can be accurately predicted by a respiratory variation in pulse oximetry plethysmographic waveform amplitude of 14%. The use of norepinephrine does not alter this relationship.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (116) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)