Hemodynamic Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2018;30(3):385-393
DOI 10.5935/0103-507X.20180055
The approach for treating a hemodynamically unstable patient remains a diagnostic and therapeutic challenge. Stabilization of the patient should be rapid and effective, but there is not much room for error. This narrow window of intervention makes it necessary to use rapid and accurate hemodynamic evaluation methods. Echocardiography is the method of choice for the bedside evaluation of patients in circulatory shock. In fact, it was intensive care physicians who recognized the potential of Doppler echocardiography for the initial approach to patients in circulatory failure. An echocardiogram allows rapid anatomical and functional cardiac evaluation, which may include non-invasive hemodynamic evaluation using a Doppler study. Such an integrated study may provide data of extreme importance for understanding the mechanisms underlying the hemodynamic instability of the patient to allow the rapid institution of appropriate therapeutic measures. In the present article, we describe the most relevant echocardiographic findings using a practical approach for critical patients with hemodynamic instability.
Abstract
Rev Bras Ter Intensiva. 2018;30(3):385-393
DOI 10.5935/0103-507X.20180055
The approach for treating a hemodynamically unstable patient remains a diagnostic and therapeutic challenge. Stabilization of the patient should be rapid and effective, but there is not much room for error. This narrow window of intervention makes it necessary to use rapid and accurate hemodynamic evaluation methods. Echocardiography is the method of choice for the bedside evaluation of patients in circulatory shock. In fact, it was intensive care physicians who recognized the potential of Doppler echocardiography for the initial approach to patients in circulatory failure. An echocardiogram allows rapid anatomical and functional cardiac evaluation, which may include non-invasive hemodynamic evaluation using a Doppler study. Such an integrated study may provide data of extreme importance for understanding the mechanisms underlying the hemodynamic instability of the patient to allow the rapid institution of appropriate therapeutic measures. In the present article, we describe the most relevant echocardiographic findings using a practical approach for critical patients with hemodynamic instability.
Abstract
Rev Bras Ter Intensiva. 2018;30(4):460-470
DOI 10.5935/0103-507X.20180067
Follow-up of cardiac index and systemic vascular resistance index by bedside echocardiography until resuscitation.
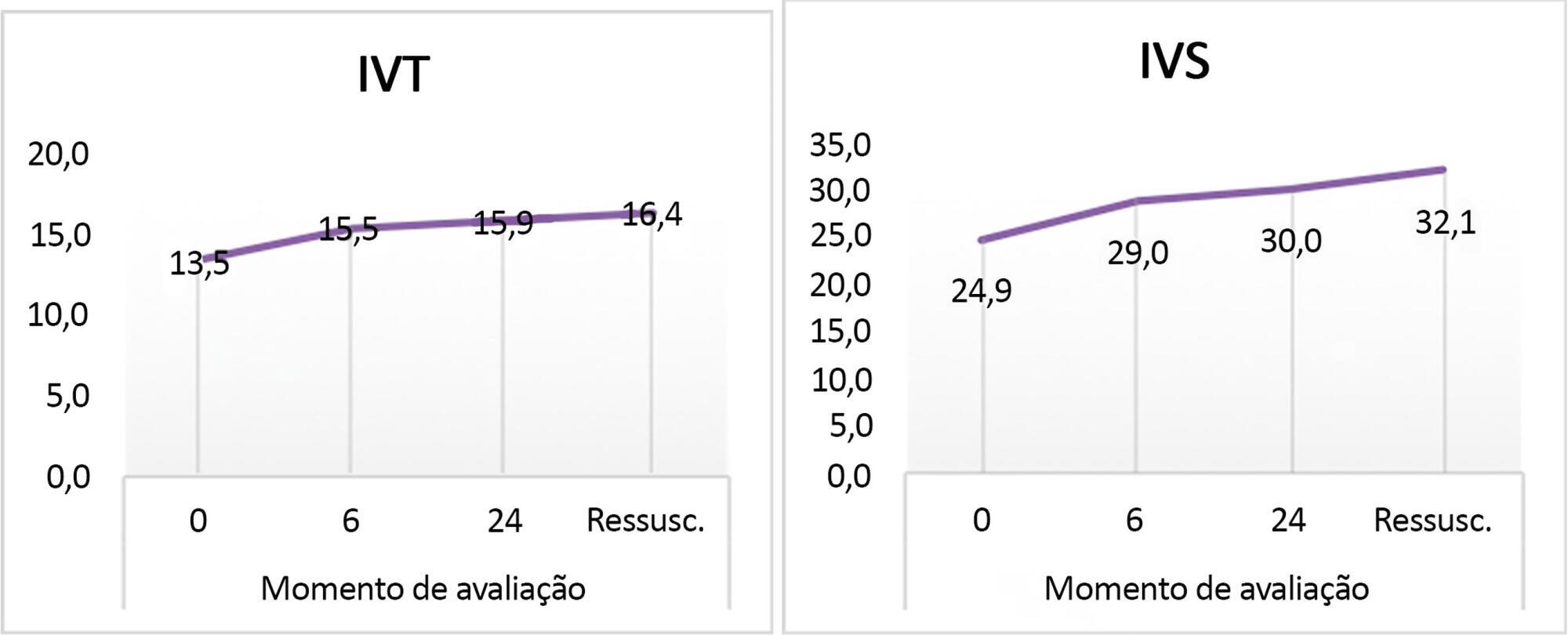
A set of hemodynamic parameters was obtained, including cardiac output, stroke volume, cardiac index, systemic vascular resistance index, velocity time integral, myocardial performance index, capillary refill time, and heart rate at 0 hours after fluid boluses before the start of inotropes, and followed up after 6 hours and 24 hours.
Included were 45 patients with community-acquired septic shock. Septic foci were gastroenteritis (24%), intestinal perforation requiring emergency surgery (24%), pneumonia (20%), central nervous system infection (22%) and soft tissue infection (8%). Klebsiella and Enterobacter were the most frequent isolates. We estimated the factors affecting the cardiac index: high central venous pressure at zero time (r = 0.33, p = 0.024) and persistently high heart rate at hour 6 (r = 0.33, p = 0.03). The systemic vascular resistance index was high in most patients at 0 and 24 hours and at the time of resuscitation and inversely affected the cardiac index as well as affecting the velocity time integral (r = -0.416, -0.61, 0.55 and -0.295). Prolonged capillary refill time was a clinical predictor of the low velocity time integral at 24 hours (r = -0.4). The mortality was 27%. Lower systemic vascular resistance index and higher cardiac output were observed in nonsurviving patients.
There was a persistently high systemic vascular resistance index in cold shock patients that influenced the stroke volume index, cardiac index, and velocity time integral. The use of echocardiograms for hemodynamic measurements is important in pediatric septic shock patients to adjust dilators, and vasopressor doses and achieve resuscitation targets in a timely manner.
Abstract
Rev Bras Ter Intensiva. 2018;30(4):460-470
DOI 10.5935/0103-507X.20180067
Follow-up of cardiac index and systemic vascular resistance index by bedside echocardiography until resuscitation.
A set of hemodynamic parameters was obtained, including cardiac output, stroke volume, cardiac index, systemic vascular resistance index, velocity time integral, myocardial performance index, capillary refill time, and heart rate at 0 hours after fluid boluses before the start of inotropes, and followed up after 6 hours and 24 hours.
Included were 45 patients with community-acquired septic shock. Septic foci were gastroenteritis (24%), intestinal perforation requiring emergency surgery (24%), pneumonia (20%), central nervous system infection (22%) and soft tissue infection (8%). Klebsiella and Enterobacter were the most frequent isolates. We estimated the factors affecting the cardiac index: high central venous pressure at zero time (r = 0.33, p = 0.024) and persistently high heart rate at hour 6 (r = 0.33, p = 0.03). The systemic vascular resistance index was high in most patients at 0 and 24 hours and at the time of resuscitation and inversely affected the cardiac index as well as affecting the velocity time integral (r = -0.416, -0.61, 0.55 and -0.295). Prolonged capillary refill time was a clinical predictor of the low velocity time integral at 24 hours (r = -0.4). The mortality was 27%. Lower systemic vascular resistance index and higher cardiac output were observed in nonsurviving patients.
There was a persistently high systemic vascular resistance index in cold shock patients that influenced the stroke volume index, cardiac index, and velocity time integral. The use of echocardiograms for hemodynamic measurements is important in pediatric septic shock patients to adjust dilators, and vasopressor doses and achieve resuscitation targets in a timely manner.
Abstract
Rev Bras Ter Intensiva. 2009;21(4):349-352
DOI 10.1590/S0103-507X2009000400003
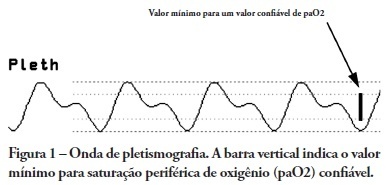
OBJECTIVES: Arterial pulse pressure respiratory variation is a good predictor of fluid response in ventilated patients. Recently, it was shown that respiratory variation in arterial pulse pressure correlates with variation in pulse oximetry plethysmographic waveform amplitude. We wanted to evaluate the correlation between respiratory variation in arterial pulse pressure and respiratory variation in pulse oximetry plethysmographic waveform amplitude, and to determine whether this correlation was influenced by norepinephrine administration. METHODS: Prospective study of sixty patients with normal sinus rhythm on mechanical ventilation, profoundly sedated and with stable hemodynamics. Oxygenation index and invasive arterial pressure were monitored. Respiratory variation in arterial pulse pressure and respiratory variation in pulse oximetry plethysmographic waveform amplitude were recorded simultaneously in a beat-to-beat evaluation, and were compared using the Pearson coefficient of agreement and linear regression. RESULTS: Thirty patients (50%) required norepinephrine. There was a significant correlation (K = 0.66; p < 0.001) between respiratory variation in arterial pulse pressure and respiratory variation in pulse oximetry plethysmographic waveform amplitude. Area under the ROC curve was 0.88 (range, 0.79 - 0.97), with a best cutoff value of 14% to predict a respiratory variation in arterial pulse pressure of 13. The use of norepinephrine did not influence the correlation (K = 0.63, p = 0.001, respectively). CONCLUSIONS: Respiratory variation in arterial pulse pressure above 13% can be accurately predicted by a respiratory variation in pulse oximetry plethysmographic waveform amplitude of 14%. The use of norepinephrine does not alter this relationship.
Abstract
Rev Bras Ter Intensiva. 2009;21(4):349-352
DOI 10.1590/S0103-507X2009000400003
OBJECTIVES: Arterial pulse pressure respiratory variation is a good predictor of fluid response in ventilated patients. Recently, it was shown that respiratory variation in arterial pulse pressure correlates with variation in pulse oximetry plethysmographic waveform amplitude. We wanted to evaluate the correlation between respiratory variation in arterial pulse pressure and respiratory variation in pulse oximetry plethysmographic waveform amplitude, and to determine whether this correlation was influenced by norepinephrine administration. METHODS: Prospective study of sixty patients with normal sinus rhythm on mechanical ventilation, profoundly sedated and with stable hemodynamics. Oxygenation index and invasive arterial pressure were monitored. Respiratory variation in arterial pulse pressure and respiratory variation in pulse oximetry plethysmographic waveform amplitude were recorded simultaneously in a beat-to-beat evaluation, and were compared using the Pearson coefficient of agreement and linear regression. RESULTS: Thirty patients (50%) required norepinephrine. There was a significant correlation (K = 0.66; p < 0.001) between respiratory variation in arterial pulse pressure and respiratory variation in pulse oximetry plethysmographic waveform amplitude. Area under the ROC curve was 0.88 (range, 0.79 - 0.97), with a best cutoff value of 14% to predict a respiratory variation in arterial pulse pressure of 13. The use of norepinephrine did not influence the correlation (K = 0.63, p = 0.001, respectively). CONCLUSIONS: Respiratory variation in arterial pulse pressure above 13% can be accurately predicted by a respiratory variation in pulse oximetry plethysmographic waveform amplitude of 14%. The use of norepinephrine does not alter this relationship.
Abstract
Rev Bras Ter Intensiva. 2009;21(2):212-218
DOI 10.1590/S0103-507X2009000200015
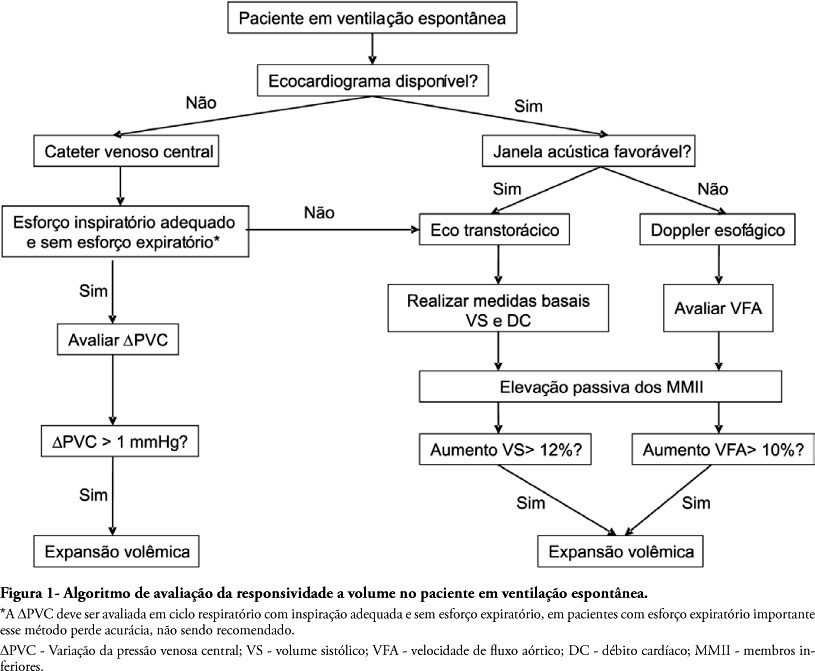
To assess fluid responsiveness in patients under spontaneous breathing activity ventilation remains a challenge for intensive care physicians. Much of the knowledge on heart-lung interactions and dynamic indexes of fluid responsiveness may not be useful for these patients. Historically, the most frequently used variables to guide fluid responsiveness on this population have been the static preload indexes. However, more recently, dynamic indexes from less invasive devices are being often used, even though their usefulness on spontaneously-breathing subjects remains controversial. The purpose of this article was to review evidences on the assessment of fluid responsiveness in patients under spontaneous ventilation. A search in literature showed poor evidence for use of static variables, such as filling pressures and ventricular end-diastolic volumes. Dynamic indexes, such as pulse pressure variation and other indexes had not been appropriately tested during spontaneous ventilation. Favorable results were found with central venous pressure variation and with transthoracic echocardiography or transesophageal Doppler dynamic indexes, especially when associated to passive lower limb elevation. We conclude that although central venous pressure variation and echocardiography variables could aid bedside clinicians in assessing fluid responsiveness during spontaneous ventilation, more studies on this subject are definitely required.
Abstract
Rev Bras Ter Intensiva. 2009;21(2):212-218
DOI 10.1590/S0103-507X2009000200015
To assess fluid responsiveness in patients under spontaneous breathing activity ventilation remains a challenge for intensive care physicians. Much of the knowledge on heart-lung interactions and dynamic indexes of fluid responsiveness may not be useful for these patients. Historically, the most frequently used variables to guide fluid responsiveness on this population have been the static preload indexes. However, more recently, dynamic indexes from less invasive devices are being often used, even though their usefulness on spontaneously-breathing subjects remains controversial. The purpose of this article was to review evidences on the assessment of fluid responsiveness in patients under spontaneous ventilation. A search in literature showed poor evidence for use of static variables, such as filling pressures and ventricular end-diastolic volumes. Dynamic indexes, such as pulse pressure variation and other indexes had not been appropriately tested during spontaneous ventilation. Favorable results were found with central venous pressure variation and with transthoracic echocardiography or transesophageal Doppler dynamic indexes, especially when associated to passive lower limb elevation. We conclude that although central venous pressure variation and echocardiography variables could aid bedside clinicians in assessing fluid responsiveness during spontaneous ventilation, more studies on this subject are definitely required.