Oximetry Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2022;34(1):185-196
DOI 10.5935/0103-507X.20220013-en
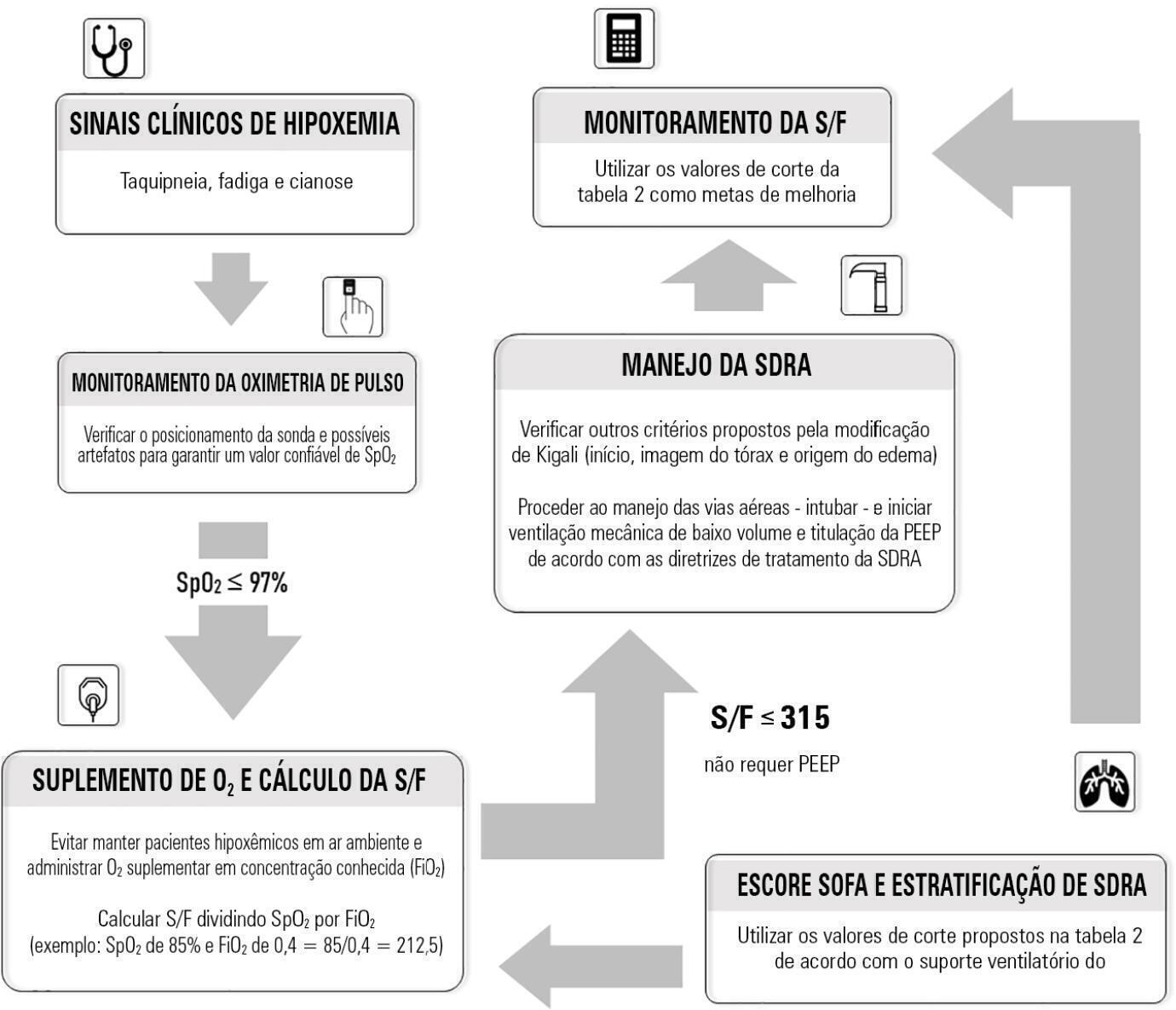
Although the PaO 2/FiO 2 derived from arterial blood gas analysis remains the gold standard for the diagnosis of acute respiratory failure, the SpO2/FiO2 has been investigated as a potential substitute. The current narrative review presents the state of the preclinical and clinical literature on the SpO2/FiO2 as a possible substitute for PaO2/FiO2 and for use as a diagnostic and prognostic marker; provides an overview of pulse oximetry and its limitations, and assesses the utility of SpO2/ FiO2 as a surrogate for PaO2/FiO2 in COVID-19 patients. Overall, 49 studies comparing SpO2/FiO2 and PaO2/FiO2 were found according to a minimal search strategy. Most were conducted on neonates, some were conducted on adults with acute respiratory distress syndrome, and a few were conducted in other clinical scenarios (including a very few on COVID-19 patients). There is some evidence that the SpO2/ FiO2 criteria can be a surrogate for PaO2/FiO2 in different clinical scenarios. This is reinforced by the fact that unnecessary invasive procedures should be avoided in patients with acute respiratory failure. It is undeniable that pulse oximeters are becoming increasingly widespread and can provide costless monitoring. Hence, replacing PaO2/FiO2 with SpO2/FiO2may allow resourcelimited facilities to objectively diagnose acute respiratory failure.
Abstract
Rev Bras Ter Intensiva. 2022;34(1):185-196
DOI 10.5935/0103-507X.20220013-en
Although the PaO 2/FiO 2 derived from arterial blood gas analysis remains the gold standard for the diagnosis of acute respiratory failure, the SpO2/FiO2 has been investigated as a potential substitute. The current narrative review presents the state of the preclinical and clinical literature on the SpO2/FiO2 as a possible substitute for PaO2/FiO2 and for use as a diagnostic and prognostic marker; provides an overview of pulse oximetry and its limitations, and assesses the utility of SpO2/ FiO2 as a surrogate for PaO2/FiO2 in COVID-19 patients. Overall, 49 studies comparing SpO2/FiO2 and PaO2/FiO2 were found according to a minimal search strategy. Most were conducted on neonates, some were conducted on adults with acute respiratory distress syndrome, and a few were conducted in other clinical scenarios (including a very few on COVID-19 patients). There is some evidence that the SpO2/ FiO2 criteria can be a surrogate for PaO2/FiO2 in different clinical scenarios. This is reinforced by the fact that unnecessary invasive procedures should be avoided in patients with acute respiratory failure. It is undeniable that pulse oximeters are becoming increasingly widespread and can provide costless monitoring. Hence, replacing PaO2/FiO2 with SpO2/FiO2may allow resourcelimited facilities to objectively diagnose acute respiratory failure.
Abstract
Rev Bras Ter Intensiva. 2011;23(3):283-290
DOI 10.1590/S0103-507X2011000300005
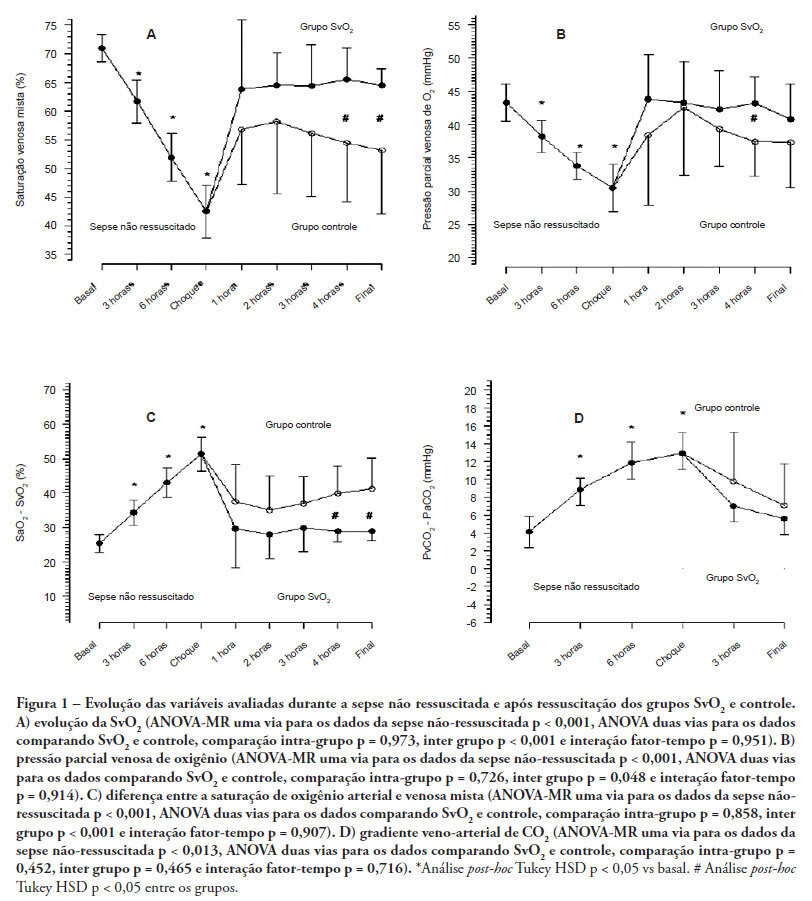
OBJECTIVES: Although fluid resuscitation guided by central venous oxygen saturation (SvcO2) is currently considered the gold standard in sepsis therapy, few studies have described hemodynamic and perfusion parameters during this procedure. This study aims to describe these parameters during septic shock without resuscitation and after 12 hours of goal-directed resuscitation. METHODS: Thirteen anesthetized pigs (35-45 kg) had peritonitis caused by fecal inoculation (0.75 g/kg). After developing persistent hypotension, both groups were given antibiotics and randomized either to the control group (n=7) or the experimental group (n=6). In the control group, hemodynamic control was optimized to maintain a central venous pressure of 8-12 mmHg, a urinary output above 0.5 mL/kg/hour and a mean arterial blood pressure above 65 mmHg. The experimental group received the above target therapy in addition to maintaining a SvO2 above 65%. The interventions included lactated Ringer's solution and norepinephrine for both groups and dobutamine in the SvO2 group. The animals were treated for 12 hours or until death. RESULTS: Untreated sepsis was associated with significant reductions in SvO2, PvO2, cardiac output and central venous pressure in addition to increased arteriovenous oxygen saturation and veno-arterial CO2 differences. Following resuscitation, these parameters were corrected in both groups. Goal-directed resuscitation was associated with a better hemodynamic profile, characterized by higher SvO2, cardiac output and central venous pressure. CONCLUSIONS: Non-resuscitated sepsis showed a hemodynamic profile suggesting hypovolemia, with worsened perfusion and hemodynamics, which is reversed upon fluid resuscitation. Goal-directed resuscitation is associated with significantly improved hemodynamic and perfusion parameters
Abstract
Rev Bras Ter Intensiva. 2011;23(3):283-290
DOI 10.1590/S0103-507X2011000300005
OBJECTIVES: Although fluid resuscitation guided by central venous oxygen saturation (SvcO2) is currently considered the gold standard in sepsis therapy, few studies have described hemodynamic and perfusion parameters during this procedure. This study aims to describe these parameters during septic shock without resuscitation and after 12 hours of goal-directed resuscitation. METHODS: Thirteen anesthetized pigs (35-45 kg) had peritonitis caused by fecal inoculation (0.75 g/kg). After developing persistent hypotension, both groups were given antibiotics and randomized either to the control group (n=7) or the experimental group (n=6). In the control group, hemodynamic control was optimized to maintain a central venous pressure of 8-12 mmHg, a urinary output above 0.5 mL/kg/hour and a mean arterial blood pressure above 65 mmHg. The experimental group received the above target therapy in addition to maintaining a SvO2 above 65%. The interventions included lactated Ringer's solution and norepinephrine for both groups and dobutamine in the SvO2 group. The animals were treated for 12 hours or until death. RESULTS: Untreated sepsis was associated with significant reductions in SvO2, PvO2, cardiac output and central venous pressure in addition to increased arteriovenous oxygen saturation and veno-arterial CO2 differences. Following resuscitation, these parameters were corrected in both groups. Goal-directed resuscitation was associated with a better hemodynamic profile, characterized by higher SvO2, cardiac output and central venous pressure. CONCLUSIONS: Non-resuscitated sepsis showed a hemodynamic profile suggesting hypovolemia, with worsened perfusion and hemodynamics, which is reversed upon fluid resuscitation. Goal-directed resuscitation is associated with significantly improved hemodynamic and perfusion parameters
Abstract
Rev Bras Ter Intensiva. 2009;21(4):349-352
DOI 10.1590/S0103-507X2009000400003
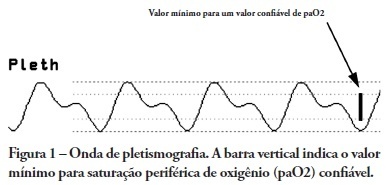
OBJECTIVES: Arterial pulse pressure respiratory variation is a good predictor of fluid response in ventilated patients. Recently, it was shown that respiratory variation in arterial pulse pressure correlates with variation in pulse oximetry plethysmographic waveform amplitude. We wanted to evaluate the correlation between respiratory variation in arterial pulse pressure and respiratory variation in pulse oximetry plethysmographic waveform amplitude, and to determine whether this correlation was influenced by norepinephrine administration. METHODS: Prospective study of sixty patients with normal sinus rhythm on mechanical ventilation, profoundly sedated and with stable hemodynamics. Oxygenation index and invasive arterial pressure were monitored. Respiratory variation in arterial pulse pressure and respiratory variation in pulse oximetry plethysmographic waveform amplitude were recorded simultaneously in a beat-to-beat evaluation, and were compared using the Pearson coefficient of agreement and linear regression. RESULTS: Thirty patients (50%) required norepinephrine. There was a significant correlation (K = 0.66; p < 0.001) between respiratory variation in arterial pulse pressure and respiratory variation in pulse oximetry plethysmographic waveform amplitude. Area under the ROC curve was 0.88 (range, 0.79 - 0.97), with a best cutoff value of 14% to predict a respiratory variation in arterial pulse pressure of 13. The use of norepinephrine did not influence the correlation (K = 0.63, p = 0.001, respectively). CONCLUSIONS: Respiratory variation in arterial pulse pressure above 13% can be accurately predicted by a respiratory variation in pulse oximetry plethysmographic waveform amplitude of 14%. The use of norepinephrine does not alter this relationship.
Abstract
Rev Bras Ter Intensiva. 2009;21(4):349-352
DOI 10.1590/S0103-507X2009000400003
OBJECTIVES: Arterial pulse pressure respiratory variation is a good predictor of fluid response in ventilated patients. Recently, it was shown that respiratory variation in arterial pulse pressure correlates with variation in pulse oximetry plethysmographic waveform amplitude. We wanted to evaluate the correlation between respiratory variation in arterial pulse pressure and respiratory variation in pulse oximetry plethysmographic waveform amplitude, and to determine whether this correlation was influenced by norepinephrine administration. METHODS: Prospective study of sixty patients with normal sinus rhythm on mechanical ventilation, profoundly sedated and with stable hemodynamics. Oxygenation index and invasive arterial pressure were monitored. Respiratory variation in arterial pulse pressure and respiratory variation in pulse oximetry plethysmographic waveform amplitude were recorded simultaneously in a beat-to-beat evaluation, and were compared using the Pearson coefficient of agreement and linear regression. RESULTS: Thirty patients (50%) required norepinephrine. There was a significant correlation (K = 0.66; p < 0.001) between respiratory variation in arterial pulse pressure and respiratory variation in pulse oximetry plethysmographic waveform amplitude. Area under the ROC curve was 0.88 (range, 0.79 - 0.97), with a best cutoff value of 14% to predict a respiratory variation in arterial pulse pressure of 13. The use of norepinephrine did not influence the correlation (K = 0.63, p = 0.001, respectively). CONCLUSIONS: Respiratory variation in arterial pulse pressure above 13% can be accurately predicted by a respiratory variation in pulse oximetry plethysmographic waveform amplitude of 14%. The use of norepinephrine does not alter this relationship.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):398-404
DOI 10.1590/S0103-507X2008000400013
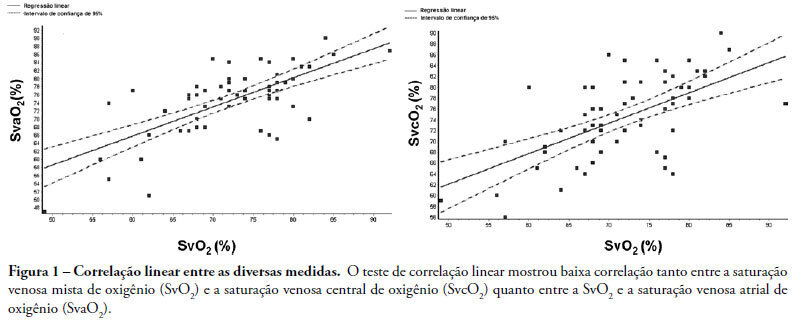
INTRODUCTION: Central venous oxygen saturation (SvcO2) has been proposed as an alternative for mixed venous oxygen saturation (SvO2), with a variable level of acceptance according to available data. This study aimed to evaluate possible differences between SvO2 and SvcO2 or atrial venous saturation (SvaO2), with emphasis on the role of cardiac output and their impact on clinical management of the septic patient. METHODS: This is an observational, prospective study of patients with septic shock monitored by pulmonary artery catheter. Blood was obtained simultaneously for SvcO2, SvO2 and SvaO2 determination. Linear correlation (significant if p<0.05) and agreement analysis (Bland-Altman) were performed with samples and subgroups according to cardiac output. Moreover, agreement about clinical management based on these samples was evaluated. RESULTS: Sixty one measurements from 23 patients were obtained, median age of 65.0 (49.0-75.0) years and mean APACHE II of 27.7±6.3. Mean values of SvO2, SvcO2 and SvaO2 were 72.20±8.26%, 74.61±7.60% and 74.64±8.47%. Linear correlation test showed a weak correlation between SvO2 and SvcO2 (r=0.61, p<0.0001) and also between SvO2 and SvaO2 (r=0.70, p<0.0001). Agreements between SvcO2/SvO2 and SvaO2/SvO2 were -2.40±1.96 (-16.20 and 11.40) and -2.40±1.96 (-15.10 and 10.20), respectively, with no difference in the cardiac output subgroups. No agreement was found in clinical management for 27.8% of the cases, both for SvcO2/SvO2 and for SvaO2/SvO2. CONCLUSION: This study showed that the correlation and agreement between SvO2 and SvcO2 is weak and may lead to different clinical management.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):398-404
DOI 10.1590/S0103-507X2008000400013
INTRODUCTION: Central venous oxygen saturation (SvcO2) has been proposed as an alternative for mixed venous oxygen saturation (SvO2), with a variable level of acceptance according to available data. This study aimed to evaluate possible differences between SvO2 and SvcO2 or atrial venous saturation (SvaO2), with emphasis on the role of cardiac output and their impact on clinical management of the septic patient. METHODS: This is an observational, prospective study of patients with septic shock monitored by pulmonary artery catheter. Blood was obtained simultaneously for SvcO2, SvO2 and SvaO2 determination. Linear correlation (significant if p<0.05) and agreement analysis (Bland-Altman) were performed with samples and subgroups according to cardiac output. Moreover, agreement about clinical management based on these samples was evaluated. RESULTS: Sixty one measurements from 23 patients were obtained, median age of 65.0 (49.0-75.0) years and mean APACHE II of 27.7±6.3. Mean values of SvO2, SvcO2 and SvaO2 were 72.20±8.26%, 74.61±7.60% and 74.64±8.47%. Linear correlation test showed a weak correlation between SvO2 and SvcO2 (r=0.61, p<0.0001) and also between SvO2 and SvaO2 (r=0.70, p<0.0001). Agreements between SvcO2/SvO2 and SvaO2/SvO2 were -2.40±1.96 (-16.20 and 11.40) and -2.40±1.96 (-15.10 and 10.20), respectively, with no difference in the cardiac output subgroups. No agreement was found in clinical management for 27.8% of the cases, both for SvcO2/SvO2 and for SvaO2/SvO2. CONCLUSION: This study showed that the correlation and agreement between SvO2 and SvcO2 is weak and may lead to different clinical management.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (116) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)