
You searched for:"Luciana Coelho Sanches"
We found (4) results for your search.-
Original Article
IMPACTO-MR: a Brazilian nationwide platform study to assess infections and multidrug resistance in intensive care units
- Bruno M Tomazini
 ,
, - Antonio Paulo Nassar Jr ,
- Thiago Costa Lisboa ,
- Luciano César Pontes de Azevedo ,
- Viviane Cordeiro Veiga , [ … ],
- Alexandre Biasi Cavalcanti
Abstract
Original ArticleIMPACTO-MR: a Brazilian nationwide platform study to assess infections and multidrug resistance in intensive care units
Rev Bras Ter Intensiva. 2022;34(4):418-425
DOI 10.5935/0103-507X.20220209-en
- Bruno M Tomazini ,
- Antonio Paulo Nassar Jr ,
- Thiago Costa Lisboa ,
- Luciano César Pontes de Azevedo ,
- Viviane Cordeiro Veiga ,
- Daniela Ghidetti Mangas Catarino ,
- Debora Vacaro Fogazzi ,
- Beatriz Arns ,
- Filipe Teixeira Piastrelli ,
- Camila Dietrich ,
- Karina Leal Negrelli,
- Isabella de Andrade Jesuíno,
- Luiz Fernando Lima Reis,
- Renata Rodrigues de Mattos,
- Carla Cristina Gomes Pinheiro,
- Mariane Nascimento Luz,
- Clayse Carla da Silva Spadoni,
- Elisângela Emilene Moro,
- Flávia Regina Bueno,
- Camila Santana Justo Cintra Sampaio,
- Débora Patrício Silva,
- Franca Pellison Baldassare,
- Ana Cecilia Alcantara Silva,
- Thabata Veiga,
- Leticia Barbante,
- Marianne Lambauer,
- Viviane Bezerra Campos,
- Elton Santos,
- Renato Hideo Nakawaga Santos,
- Ligia Nasi Laranjeiras,
- Nanci Valeis,
- Eliana Santucci,
- Tamiris Abait Miranda,
- Ana Cristina Lagoeiro do Patrocínio,
- Andréa de Carvalho,
- Eduvirgens Maria Couto de Sousa,
- Ancelmo Honorato Ferraz de Sousa,
- Daniel Tavares Malheiro,
- Isabella Lott Bezerra,
- Mirian Batista Rodrigues,
- Julliana Chicuta Malicia,
- Sabrina Souza da Silva,
- Bruna dos Passos Gimenes,
- Guilhermo Prates Sesin,
- Alexandre Prehn Zavascki,
- Daniel Sganzerla,
- Gregory Saraiva Medeiros,
- Rosa da Rosa Minho dos Santos,
- Fernanda Kelly Romeiro Silva,
- Maysa Yukari Cheno,
- Carolinne Ferreira Abrahão,
- Haliton Alves de Oliveira Junior,
- Leonardo Lima Rocha,
- Pedro Aniceto Nunes Neto,
- Valéria Chagas Pereira,
- Luis Eduardo Miranda Paciência,
- Elaine Silva Bueno,
- Eliana Bernadete Caser,
- Larissa Zuqui Ribeiro,
- Caio Cesar Ferreira Fernandes,
- Juliana Mazzei Garcia,
- Vanildes de Fátima Fernandes Silva,
- Alisson Junior dos Santos,
- Flávia Ribeiro Machado,
- Maria Aparecida de Souza,
- Bianca Ramos Ferronato,
- Hugo Corrêa de Andrade Urbano,
- Danielle Conceição Aparecida Moreira,
- Vicente Cés de Souza-Dantas,
- Diego Meireles Duarte,
- Juliana Coelho,
- Rodrigo Cruvinel Figueiredo,
- Fernanda Foreque,
- Thiago Gomes Romano,
- Daniel Cubos,
- Vladimir Miguel Spirale,
- Roberta Schiavon Nogueira,
- Israel Silva Maia,
- Cassio Luis Zandonai,
- Wilson José Lovato,
- Rodrigo Barbosa Cerantola,
- Tatiana Gozzi Pancev Toledo,
- Pablo Oscar Tomba,
- Joyce Ramos de Almeida,
- Luciana Coelho Sanches,
- Leticia Pierini,
- Mariana Cunha,
- Michelle Tereza Sousa,
- Bruna Azevedo,
- Felipe Dal-Pizzol,
- Danusa de Castro Damasio,
- Marina Peres Bainy,
- Dagoberta Alves Vieira Beduhn,
- Joana D’Arc Vila Nova Jatobá,
- Maria Tereza Farias de Moura,
- Leila Rezegue de Moraes Rego,
- Adria Vanessa da Silva,
- Luana Pontes Oliveira,
- Eliene Sá Sodré Filho,
- Silvana Soares dos Santos,
- Itallo de Lima Neves,
- Vanessa Cristina de Aquino Leão,
- João Lucidio Lobato Paes,
- Marielle Cristina Mendes Silva,
- Cláudio Dornas de Oliveira,
- Raquel Caldeira Brant Santiago,
- Jorge Luiz da Rocha Paranhos,
- Iany Grinezia da Silva Wiermann,
- Durval Ferreira Fonseca Pedroso,
- Priscilla Yoshiko Sawada,
- Rejane Martins Prestes,
- Glícia Cardoso Nascimento,
- Cintia Magalhães Carvalho Grion,
- Claudia Maria Dantas de Maio Carrilho,
- Roberta Lacerda Almeida de Miranda Dantas,
- Eliane Pereira Silva,
- Antônio Carlos da Silva,
- Sheila Mara Bezerra de Oliveira,
- Nicole Alberti Golin,
- Rogerio Tregnago,
- Valéria Paes Lima,
- Kamilla Grasielle Nunes da Silva,
- Emerson Boschi,
- Viviane Buffon,
- André Sant’Ana Machado,
- Leticia Capeletti,
- Rafael Botelho Foernges,
- Andréia Schubert de Carvalho,
- Lúcio Couto de Oliveira Junior,
- Daniela Cunha de Oliveira,
- Everton Macêdo Silva,
- Julival Ribeiro,
- Francielle Constantino Pereira,
- Fernanda Borges Salgado,
- Caroline Deutschendorf,
- Cristofer Farias da Silva,
- Andre Luiz Nunes Gobatto,
- Carolaine Bomfim de Oliveira,
- Marianna Deway Andrade Dracoulakis,
- Natália Oliveira Santos Alvaia,
- Roberta Machado de Souza,
- Larissa Liz Cardoso de Araújo,
- Rodrigo Morel Vieira de Melo,
- Luiz Carlos Santana Passos,
- Claudia Fernanda de Lacerda Vidal,
- Fernanda Lopes de Albuquerque Rodrigues,
- Pedro Kurtz,
- Cássia Righy Shinotsuka,
- Maria Brandão Tavares,
- Igor das Virgens Santana,
- Luciana Macedo da Silva Gavinho,
- Alaís Brito Nascimento,
- Adriano J Pereira,
- Alexandre Biasi Cavalcanti
Views2ABSTRACT
Objective:
To describe the IMPACTO-MR, a Brazilian nationwide intensive care unit platform study focused on the impact of health care-associated infections due to multidrug-resistant bacteria.
Methods:
We described the IMPACTO-MR platform, its development, criteria for intensive care unit selection, characterization of core data collection, objectives, and future research projects to be held within the platform.
Results:
The core data were collected using the Epimed Monitor System® and consisted of demographic data, comorbidity data, functional status, clinical scores, admission diagnosis and secondary diagnoses, laboratory, clinical, and microbiological data, and organ support during intensive care unit stay, among others. From October 2019 to December 2020, 33,983 patients from 51 intensive care units were included in the core database.
Conclusion:
The IMPACTO-MR platform is a nationwide Brazilian intensive care unit clinical database focused on researching the impact of health care-associated infections due to multidrug-resistant bacteria. This platform provides data for individual intensive care unit development and research and multicenter observational and prospective trials.
Keywords:bacterialBacterial infectionsDatabaseDatabase management systemsDrug-resistanceIMPACTO-MRIntensive care unitsSoftwareSee moreViews2

Abstract
Original ArticleIMPACTO-MR: a Brazilian nationwide platform study to assess infections and multidrug resistance in intensive care units
Rev Bras Ter Intensiva. 2022;34(4):418-425
DOI 10.5935/0103-507X.20220209-en
- Bruno M Tomazini ,
- Antonio Paulo Nassar Jr ,
- Thiago Costa Lisboa ,
- Luciano César Pontes de Azevedo ,
- Viviane Cordeiro Veiga ,
- Daniela Ghidetti Mangas Catarino ,
- Debora Vacaro Fogazzi ,
- Beatriz Arns ,
- Filipe Teixeira Piastrelli ,
- Camila Dietrich ,
- Karina Leal Negrelli,
- Isabella de Andrade Jesuíno,
- Luiz Fernando Lima Reis,
- Renata Rodrigues de Mattos,
- Carla Cristina Gomes Pinheiro,
- Mariane Nascimento Luz,
- Clayse Carla da Silva Spadoni,
- Elisângela Emilene Moro,
- Flávia Regina Bueno,
- Camila Santana Justo Cintra Sampaio,
- Débora Patrício Silva,
- Franca Pellison Baldassare,
- Ana Cecilia Alcantara Silva,
- Thabata Veiga,
- Leticia Barbante,
- Marianne Lambauer,
- Viviane Bezerra Campos,
- Elton Santos,
- Renato Hideo Nakawaga Santos,
- Ligia Nasi Laranjeiras,
- Nanci Valeis,
- Eliana Santucci,
- Tamiris Abait Miranda,
- Ana Cristina Lagoeiro do Patrocínio,
- Andréa de Carvalho,
- Eduvirgens Maria Couto de Sousa,
- Ancelmo Honorato Ferraz de Sousa,
- Daniel Tavares Malheiro,
- Isabella Lott Bezerra,
- Mirian Batista Rodrigues,
- Julliana Chicuta Malicia,
- Sabrina Souza da Silva,
- Bruna dos Passos Gimenes,
- Guilhermo Prates Sesin,
- Alexandre Prehn Zavascki,
- Daniel Sganzerla,
- Gregory Saraiva Medeiros,
- Rosa da Rosa Minho dos Santos,
- Fernanda Kelly Romeiro Silva,
- Maysa Yukari Cheno,
- Carolinne Ferreira Abrahão,
- Haliton Alves de Oliveira Junior,
- Leonardo Lima Rocha,
- Pedro Aniceto Nunes Neto,
- Valéria Chagas Pereira,
- Luis Eduardo Miranda Paciência,
- Elaine Silva Bueno,
- Eliana Bernadete Caser,
- Larissa Zuqui Ribeiro,
- Caio Cesar Ferreira Fernandes,
- Juliana Mazzei Garcia,
- Vanildes de Fátima Fernandes Silva,
- Alisson Junior dos Santos,
- Flávia Ribeiro Machado,
- Maria Aparecida de Souza,
- Bianca Ramos Ferronato,
- Hugo Corrêa de Andrade Urbano,
- Danielle Conceição Aparecida Moreira,
- Vicente Cés de Souza-Dantas,
- Diego Meireles Duarte,
- Juliana Coelho,
- Rodrigo Cruvinel Figueiredo,
- Fernanda Foreque,
- Thiago Gomes Romano,
- Daniel Cubos,
- Vladimir Miguel Spirale,
- Roberta Schiavon Nogueira,
- Israel Silva Maia,
- Cassio Luis Zandonai,
- Wilson José Lovato,
- Rodrigo Barbosa Cerantola,
- Tatiana Gozzi Pancev Toledo,
- Pablo Oscar Tomba,
- Joyce Ramos de Almeida,
- Luciana Coelho Sanches,
- Leticia Pierini,
- Mariana Cunha,
- Michelle Tereza Sousa,
- Bruna Azevedo,
- Felipe Dal-Pizzol,
- Danusa de Castro Damasio,
- Marina Peres Bainy,
- Dagoberta Alves Vieira Beduhn,
- Joana D’Arc Vila Nova Jatobá,
- Maria Tereza Farias de Moura,
- Leila Rezegue de Moraes Rego,
- Adria Vanessa da Silva,
- Luana Pontes Oliveira,
- Eliene Sá Sodré Filho,
- Silvana Soares dos Santos,
- Itallo de Lima Neves,
- Vanessa Cristina de Aquino Leão,
- João Lucidio Lobato Paes,
- Marielle Cristina Mendes Silva,
- Cláudio Dornas de Oliveira,
- Raquel Caldeira Brant Santiago,
- Jorge Luiz da Rocha Paranhos,
- Iany Grinezia da Silva Wiermann,
- Durval Ferreira Fonseca Pedroso,
- Priscilla Yoshiko Sawada,
- Rejane Martins Prestes,
- Glícia Cardoso Nascimento,
- Cintia Magalhães Carvalho Grion,
- Claudia Maria Dantas de Maio Carrilho,
- Roberta Lacerda Almeida de Miranda Dantas,
- Eliane Pereira Silva,
- Antônio Carlos da Silva,
- Sheila Mara Bezerra de Oliveira,
- Nicole Alberti Golin,
- Rogerio Tregnago,
- Valéria Paes Lima,
- Kamilla Grasielle Nunes da Silva,
- Emerson Boschi,
- Viviane Buffon,
- André Sant’Ana Machado,
- Leticia Capeletti,
- Rafael Botelho Foernges,
- Andréia Schubert de Carvalho,
- Lúcio Couto de Oliveira Junior,
- Daniela Cunha de Oliveira,
- Everton Macêdo Silva,
- Julival Ribeiro,
- Francielle Constantino Pereira,
- Fernanda Borges Salgado,
- Caroline Deutschendorf,
- Cristofer Farias da Silva,
- Andre Luiz Nunes Gobatto,
- Carolaine Bomfim de Oliveira,
- Marianna Deway Andrade Dracoulakis,
- Natália Oliveira Santos Alvaia,
- Roberta Machado de Souza,
- Larissa Liz Cardoso de Araújo,
- Rodrigo Morel Vieira de Melo,
- Luiz Carlos Santana Passos,
- Claudia Fernanda de Lacerda Vidal,
- Fernanda Lopes de Albuquerque Rodrigues,
- Pedro Kurtz,
- Cássia Righy Shinotsuka,
- Maria Brandão Tavares,
- Igor das Virgens Santana,
- Luciana Macedo da Silva Gavinho,
- Alaís Brito Nascimento,
- Adriano J Pereira,
- Alexandre Biasi Cavalcanti
Views2ABSTRACT
Objective:
To describe the IMPACTO-MR, a Brazilian nationwide intensive care unit platform study focused on the impact of health care-associated infections due to multidrug-resistant bacteria.
Methods:
We described the IMPACTO-MR platform, its development, criteria for intensive care unit selection, characterization of core data collection, objectives, and future research projects to be held within the platform.
Results:
The core data were collected using the Epimed Monitor System® and consisted of demographic data, comorbidity data, functional status, clinical scores, admission diagnosis and secondary diagnoses, laboratory, clinical, and microbiological data, and organ support during intensive care unit stay, among others. From October 2019 to December 2020, 33,983 patients from 51 intensive care units were included in the core database.
Conclusion:
The IMPACTO-MR platform is a nationwide Brazilian intensive care unit clinical database focused on researching the impact of health care-associated infections due to multidrug-resistant bacteria. This platform provides data for individual intensive care unit development and research and multicenter observational and prospective trials.
Keywords:bacterialBacterial infectionsDatabaseDatabase management systemsDrug-resistanceIMPACTO-MRIntensive care unitsSoftwareSee more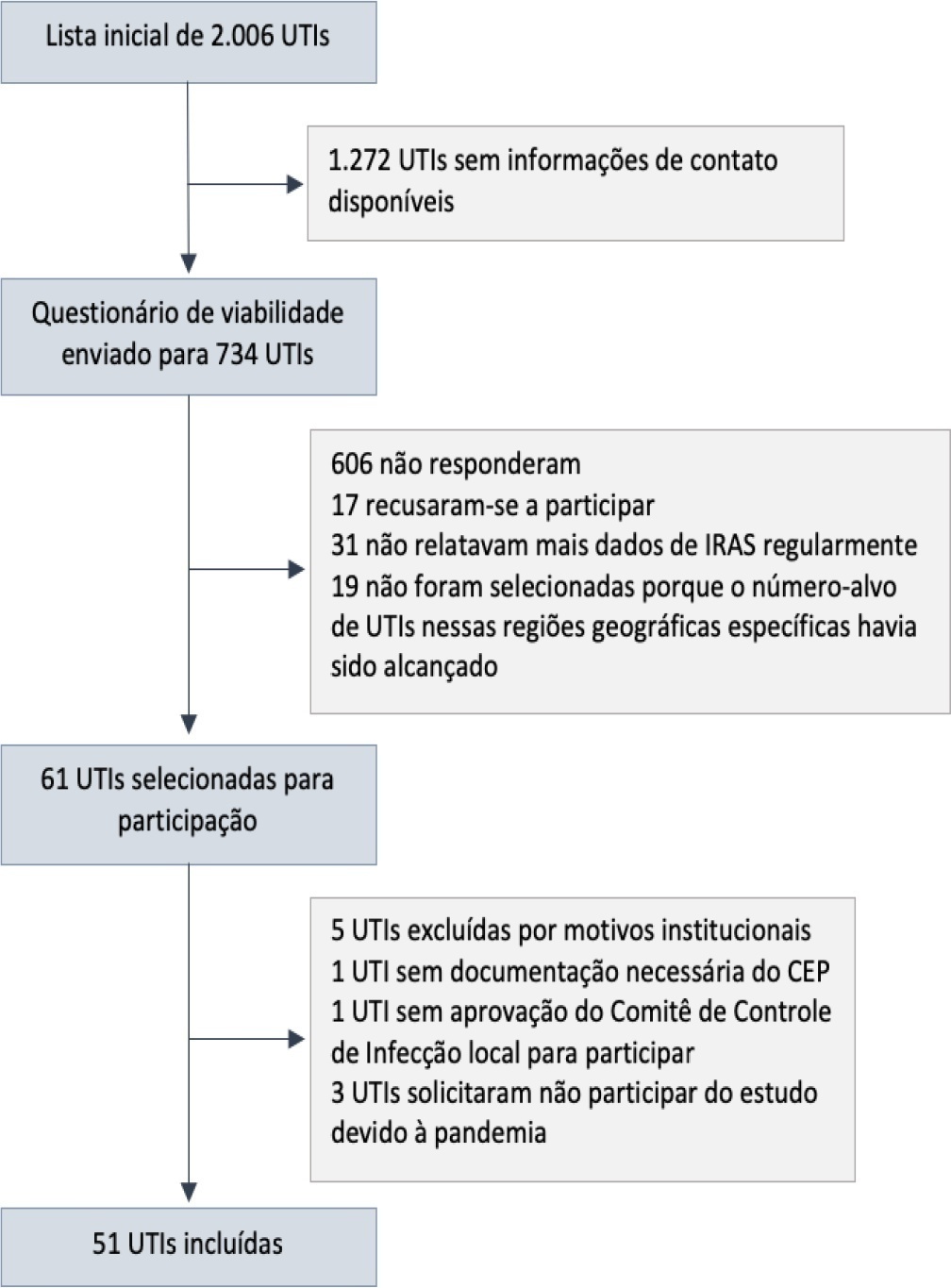
- Bruno M Tomazini
-
Original Article
Epidemiology and outcome of high-surgical-risk patients admitted to an intensive care unit in Brazil
- João Manoel Silva Júnior ,
- Renato Carneiro de Freitas Chaves ,
- Thiago Domingos Corrêa ,
- Murillo Santucci Cesar de Assunção ,
- Henrique Tadashi Katayama, [ … ],
- Suzana Margareth Ajeje Lobo
Abstract
Original ArticleEpidemiology and outcome of high-surgical-risk patients admitted to an intensive care unit in Brazil
Rev Bras Ter Intensiva. 2020;32(1):17-27
DOI 10.5935/0103-507X.20200005
- João Manoel Silva Júnior ,
- Renato Carneiro de Freitas Chaves ,
- Thiago Domingos Corrêa ,
- Murillo Santucci Cesar de Assunção ,
- Henrique Tadashi Katayama,
- Fabio Eduardo Bosso,
- Cristina Prata Amendola,
- Ary Serpa Neto ,
- Luiz Marcelo Sá Malbouisson,
- Neymar Elias de Oliveira,
- Viviane Cordeiro Veiga ,
- Salomón Soriano Ordinola Rojas,
- Natalia Fioravante Postalli,
- Thais Kawagoe Alvarisa,
- Bruno Melo Nobrega de Lucena,
- Raphael Augusto Gomes de Oliveira,
- Luciana Coelho Sanches,
- Ulysses Vasconcellos de Andrade e Silva,
- Antonio Paulo Nassar Junior ,
- Álvaro Réa-Neto,
- Alexandre Amaral,
- José Mário Teles,
- Flávio Geraldo Rezende de Freitas,
- Antônio Tonete Bafi,
- Eduardo Souza Pacheco,
- Fernando José Ramos,
- José Mauro Vieira Júnior,
- Maria Augusta Santos Rahe Pereira,
- Fábio Sartori Schwerz,
- Giovanna Padoa de Menezes,
- Danielle Dourado Magalhães,
- Cristine Pilati Pileggi Castro,
- Sabrina Frighetto Henrich,
- Diogo Oliveira Toledo,
- Bruna Fernanda Camargo Silva Parra,
- Fernando Suparregui Dias ,
- Luiza Zerman,
- Fernanda Formolo,
- Marciano de Sousa Nobrega,
- Claudio Piras,
- Stéphanie de Barros Piras,
- Rodrigo Conti,
- Paulo Lisboa Bittencourt,
- Ricardo Azevedo Cruz D’Oliveira,
- André Ricardo de Oliveira Estrela,
- Mirella Cristine de Oliveira,
- Fernanda Baeumle Reese,
- Jarbas da Silva Motta Júnior,
- Bruna Martins Dzivielevski da Câmara,
- Paula Geraldes David-João,
- Luana Alves Tannous,
- Viviane Bernardes de Oliveira Chaiben,
- Lorena Macedo Araújo Miranda,
- José Arthur dos Santos Brasil,
- Rafael Alexandre de Oliveira Deucher,
- Marcos Henrique Borges Ferreira,
- Denner Luiz Vilela,
- Guilherme Cincinato de Almeida,
- Wagner Luis Nedel ,
- Matheus Golenia dos Passos,
- Luiz Gustavo Marin,
- Wilson de Oliveira Filho,
- Raoni Machado Coutinho,
- Michele Cristina Lima de Oliveira,
- Gilberto Friedman,
- André Meregalli,
- Jorge Amilton Höher,
- Afonso José Celente Soares,
- Suzana Margareth Ajeje Lobo
Views1ABSTRACT
Objective:
To define the epidemiological profile and the main determinants of morbidity and mortality in noncardiac high surgical risk patients in Brazil.
Methods:
This was a prospective, observational and multicenter study. All noncardiac surgical patients admitted to intensive care units, i.e., those considered high risk, within a 1-month period were evaluated and monitored daily for a maximum of 7 days in the intensive care unit to determine complications. The 28-day postoperative, intensive care unit and hospital mortality rates were evaluated.
Results:
Twenty-nine intensive care units participated in the study. Surgeries were performed in 25,500 patients, of whom 904 (3.5%) were high-risk (95% confidence interval – 95%CI 3.3% – 3.8%) and were included in the study. Of the participating patients, 48.3% were from private intensive care units, and 51.7% were from public intensive care units. The length of stay in the intensive care unit was 2.0 (1.0 – 4.0) days, and the length of hospital stay was 9.5 (5.4 – 18.6) days. The complication rate was 29.9% (95%CI 26.4 – 33.7), and the 28-day postoperative mortality rate was 9.6% (95%CI 7.4 – 12.1). The independent risk factors for complications were the Simplified Acute Physiology Score 3 (SAPS 3; odds ratio – OR = 1.02; 95%CI 1.01 – 1.03) and Sequential Organ Failure Assessment Score (SOFA) on admission to the intensive care unit (OR = 1.17; 95%CI 1.09 – 1.25), surgical time (OR = 1.001, 95%CI 1.000 – 1.002) and emergency surgeries (OR = 1.93, 95%CI, 1.10 – 3.38). In addition, there were associations with 28-day mortality (OR = 1.032; 95%CI 1.011 – 1.052), SAPS 3 (OR = 1.041; 95%CI 1.107 – 1.279), SOFA (OR = 1.175, 95%CI 1.069 – 1.292) and emergency surgeries (OR = 2.509; 95%CI 1.040 – 6.051).
Conclusion:
Higher prognostic scores, elderly patients, longer surgical times and emergency surgeries were strongly associated with higher 28-day mortality and more complications during the intensive care unit stay.
Keywords:BrazilIntensive care unitspostoperative carePostoperative complications/mortalitySurgical procedures, operative/epidemiologySurgical procedures, operative/mortalitySee moreViews1Abstract
Original ArticleEpidemiology and outcome of high-surgical-risk patients admitted to an intensive care unit in Brazil
Rev Bras Ter Intensiva. 2020;32(1):17-27
DOI 10.5935/0103-507X.20200005
- João Manoel Silva Júnior ,
- Renato Carneiro de Freitas Chaves ,
- Thiago Domingos Corrêa ,
- Murillo Santucci Cesar de Assunção ,
- Henrique Tadashi Katayama,
- Fabio Eduardo Bosso,
- Cristina Prata Amendola,
- Ary Serpa Neto ,
- Luiz Marcelo Sá Malbouisson,
- Neymar Elias de Oliveira,
- Viviane Cordeiro Veiga ,
- Salomón Soriano Ordinola Rojas,
- Natalia Fioravante Postalli,
- Thais Kawagoe Alvarisa,
- Bruno Melo Nobrega de Lucena,
- Raphael Augusto Gomes de Oliveira,
- Luciana Coelho Sanches,
- Ulysses Vasconcellos de Andrade e Silva,
- Antonio Paulo Nassar Junior ,
- Álvaro Réa-Neto,
- Alexandre Amaral,
- José Mário Teles,
- Flávio Geraldo Rezende de Freitas,
- Antônio Tonete Bafi,
- Eduardo Souza Pacheco,
- Fernando José Ramos,
- José Mauro Vieira Júnior,
- Maria Augusta Santos Rahe Pereira,
- Fábio Sartori Schwerz,
- Giovanna Padoa de Menezes,
- Danielle Dourado Magalhães,
- Cristine Pilati Pileggi Castro,
- Sabrina Frighetto Henrich,
- Diogo Oliveira Toledo,
- Bruna Fernanda Camargo Silva Parra,
- Fernando Suparregui Dias ,
- Luiza Zerman,
- Fernanda Formolo,
- Marciano de Sousa Nobrega,
- Claudio Piras,
- Stéphanie de Barros Piras,
- Rodrigo Conti,
- Paulo Lisboa Bittencourt,
- Ricardo Azevedo Cruz D’Oliveira,
- André Ricardo de Oliveira Estrela,
- Mirella Cristine de Oliveira,
- Fernanda Baeumle Reese,
- Jarbas da Silva Motta Júnior,
- Bruna Martins Dzivielevski da Câmara,
- Paula Geraldes David-João,
- Luana Alves Tannous,
- Viviane Bernardes de Oliveira Chaiben,
- Lorena Macedo Araújo Miranda,
- José Arthur dos Santos Brasil,
- Rafael Alexandre de Oliveira Deucher,
- Marcos Henrique Borges Ferreira,
- Denner Luiz Vilela,
- Guilherme Cincinato de Almeida,
- Wagner Luis Nedel ,
- Matheus Golenia dos Passos,
- Luiz Gustavo Marin,
- Wilson de Oliveira Filho,
- Raoni Machado Coutinho,
- Michele Cristina Lima de Oliveira,
- Gilberto Friedman,
- André Meregalli,
- Jorge Amilton Höher,
- Afonso José Celente Soares,
- Suzana Margareth Ajeje Lobo
Views1ABSTRACT
Objective:
To define the epidemiological profile and the main determinants of morbidity and mortality in noncardiac high surgical risk patients in Brazil.
Methods:
This was a prospective, observational and multicenter study. All noncardiac surgical patients admitted to intensive care units, i.e., those considered high risk, within a 1-month period were evaluated and monitored daily for a maximum of 7 days in the intensive care unit to determine complications. The 28-day postoperative, intensive care unit and hospital mortality rates were evaluated.
Results:
Twenty-nine intensive care units participated in the study. Surgeries were performed in 25,500 patients, of whom 904 (3.5%) were high-risk (95% confidence interval – 95%CI 3.3% – 3.8%) and were included in the study. Of the participating patients, 48.3% were from private intensive care units, and 51.7% were from public intensive care units. The length of stay in the intensive care unit was 2.0 (1.0 – 4.0) days, and the length of hospital stay was 9.5 (5.4 – 18.6) days. The complication rate was 29.9% (95%CI 26.4 – 33.7), and the 28-day postoperative mortality rate was 9.6% (95%CI 7.4 – 12.1). The independent risk factors for complications were the Simplified Acute Physiology Score 3 (SAPS 3; odds ratio – OR = 1.02; 95%CI 1.01 – 1.03) and Sequential Organ Failure Assessment Score (SOFA) on admission to the intensive care unit (OR = 1.17; 95%CI 1.09 – 1.25), surgical time (OR = 1.001, 95%CI 1.000 – 1.002) and emergency surgeries (OR = 1.93, 95%CI, 1.10 – 3.38). In addition, there were associations with 28-day mortality (OR = 1.032; 95%CI 1.011 – 1.052), SAPS 3 (OR = 1.041; 95%CI 1.107 – 1.279), SOFA (OR = 1.175, 95%CI 1.069 – 1.292) and emergency surgeries (OR = 2.509; 95%CI 1.040 – 6.051).
Conclusion:
Higher prognostic scores, elderly patients, longer surgical times and emergency surgeries were strongly associated with higher 28-day mortality and more complications during the intensive care unit stay.
Keywords:BrazilIntensive care unitspostoperative carePostoperative complications/mortalitySurgical procedures, operative/epidemiologySurgical procedures, operative/mortalitySee more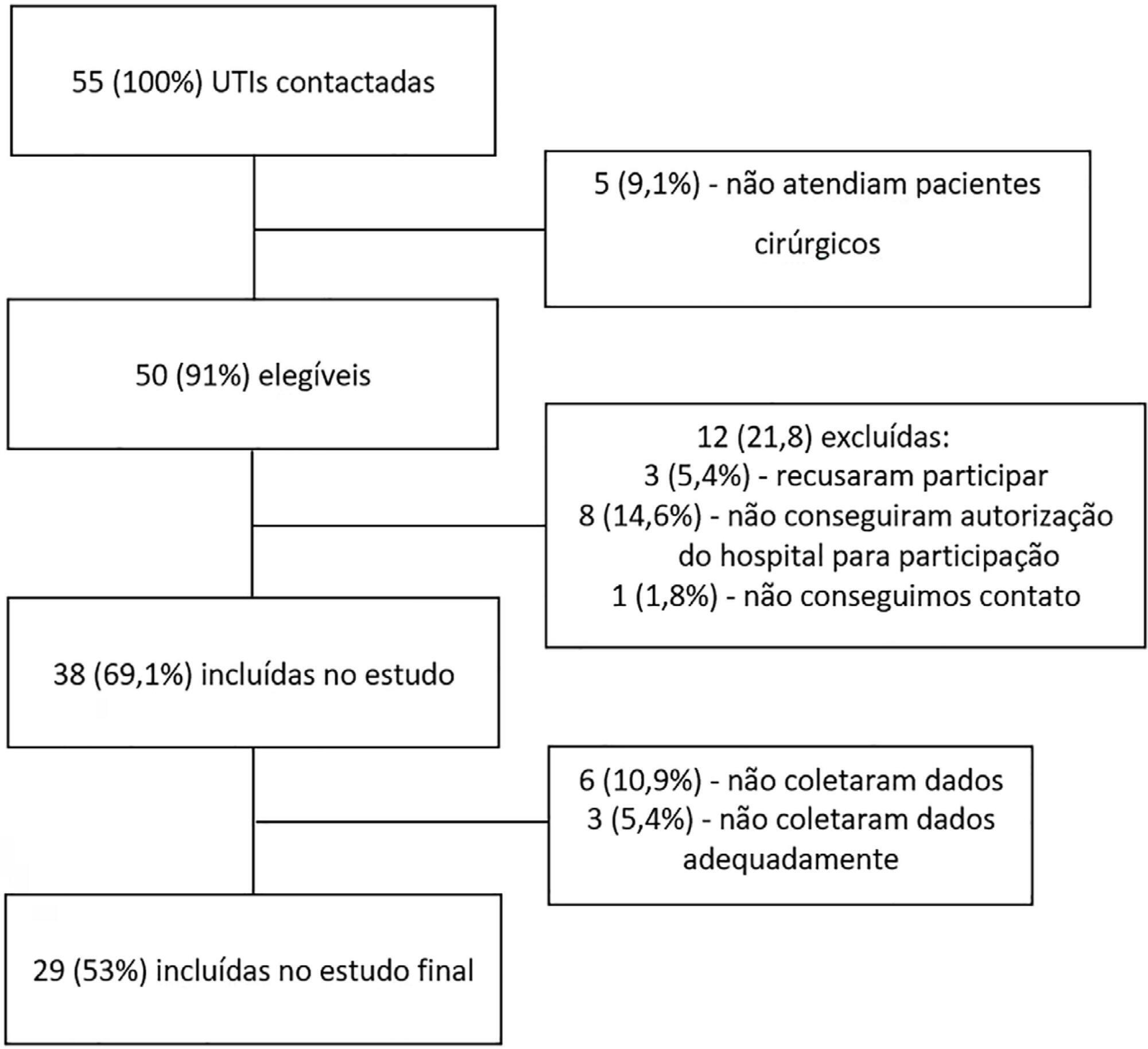
- João Manoel Silva Júnior
-
Original Articles – Basic Research
Association between organ dysfunction and cytokine concentrations during the early phases of septic shock
Rev Bras Ter Intensiva. 2011;23(4):426-433
Abstract
Original Articles – Basic ResearchAssociation between organ dysfunction and cytokine concentrations during the early phases of septic shock
Rev Bras Ter Intensiva. 2011;23(4):426-433
DOI 10.1590/S0103-507X2011000400006
Views1OBJECTIVE: To investigate the correlation of organ dysfunction and its progression with inflammatory response during the early phases of septic shock by assessing baseline cytokine concentrations. METHODS: This study included patients over 18 years old with septic shock within the first 48 hours after the onset of organ dysfunction. Interleukin 6 (IL-6), interleukin 8 (IL-8), interleukin 10 (IL-10) and C-reactive protein levels were assessed at inclusion and after 24 hours, and the differences between these values were calculated. The progression of organ dysfunction was assessed using the Sequential Organ Failure Assessment (SOFA) score upon admission and 24 hours later for a delta-SOFA determination and were categorized as either worsened or improved. The results were expressed as means + standard deviation or median (25-75% percentiles). Values with descriptive p values of 0.05 or less were considered significant. RESULTS: Overall, we included 41 patients with median SOFA scores of 8.0 (6.5-10.0) upon admission (T0) and 8.0 (6.0-10.0) 24 hours later (T1). Worsened, improved or unchanged SOFA scores were observed in 11 (Group 1), 17 (Group 2) and 13 (Group 3) patients, respectively. For Group 1, the baseline IL-6, IL-8 and IL-10 values were higher, and a significant increase of IL-8 levels was found after 24 hours. The change in the SOFA score after 24 hours was significantly, although weakly, correlated with baseline IL-6 and IL-8 concentrations. CONCLUSIONS: Higher baseline IL-6, IL-8 and IL-10 levels are associated with unfavorable organ dysfunction outcomes. Increased IL-8 levels within the first 24 hours are correlated with a worsening dysfunction.
Keywords:CytokinesetiologyMultiple organ failureShock, septicsystemic inflammatory response syndromeSee moreViews1Abstract
Original Articles – Basic ResearchAssociation between organ dysfunction and cytokine concentrations during the early phases of septic shock
Rev Bras Ter Intensiva. 2011;23(4):426-433
DOI 10.1590/S0103-507X2011000400006
Views1OBJECTIVE: To investigate the correlation of organ dysfunction and its progression with inflammatory response during the early phases of septic shock by assessing baseline cytokine concentrations. METHODS: This study included patients over 18 years old with septic shock within the first 48 hours after the onset of organ dysfunction. Interleukin 6 (IL-6), interleukin 8 (IL-8), interleukin 10 (IL-10) and C-reactive protein levels were assessed at inclusion and after 24 hours, and the differences between these values were calculated. The progression of organ dysfunction was assessed using the Sequential Organ Failure Assessment (SOFA) score upon admission and 24 hours later for a delta-SOFA determination and were categorized as either worsened or improved. The results were expressed as means + standard deviation or median (25-75% percentiles). Values with descriptive p values of 0.05 or less were considered significant. RESULTS: Overall, we included 41 patients with median SOFA scores of 8.0 (6.5-10.0) upon admission (T0) and 8.0 (6.0-10.0) 24 hours later (T1). Worsened, improved or unchanged SOFA scores were observed in 11 (Group 1), 17 (Group 2) and 13 (Group 3) patients, respectively. For Group 1, the baseline IL-6, IL-8 and IL-10 values were higher, and a significant increase of IL-8 levels was found after 24 hours. The change in the SOFA score after 24 hours was significantly, although weakly, correlated with baseline IL-6 and IL-8 concentrations. CONCLUSIONS: Higher baseline IL-6, IL-8 and IL-10 levels are associated with unfavorable organ dysfunction outcomes. Increased IL-8 levels within the first 24 hours are correlated with a worsening dysfunction.
Keywords:CytokinesetiologyMultiple organ failureShock, septicsystemic inflammatory response syndromeSee more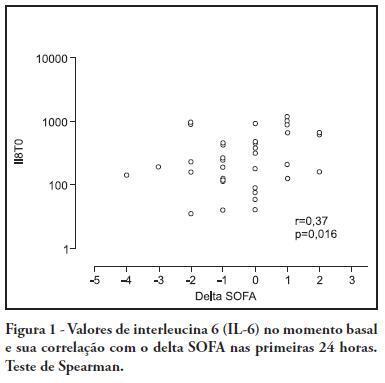
-
Original Articles
Central and mixed venous oxygen saturation in septic shock: is there a clinically relevant difference?
Rev Bras Ter Intensiva. 2008;20(4):398-404
Abstract
Original ArticlesCentral and mixed venous oxygen saturation in septic shock: is there a clinically relevant difference?
Rev Bras Ter Intensiva. 2008;20(4):398-404
DOI 10.1590/S0103-507X2008000400013
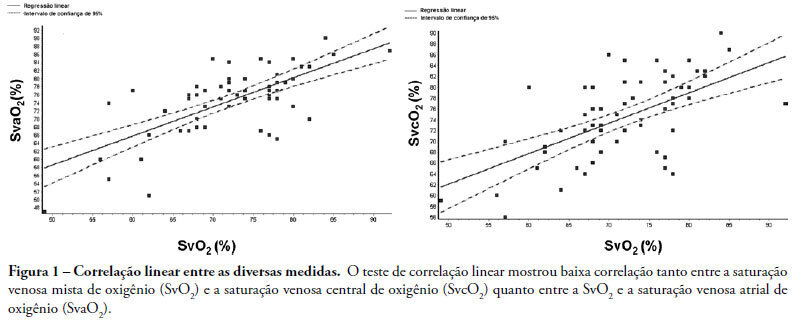
Views0See moreINTRODUCTION: Central venous oxygen saturation (SvcO2) has been proposed as an alternative for mixed venous oxygen saturation (SvO2), with a variable level of acceptance according to available data. This study aimed to evaluate possible differences between SvO2 and SvcO2 or atrial venous saturation (SvaO2), with emphasis on the role of cardiac output and their impact on clinical management of the septic patient. METHODS: This is an observational, prospective study of patients with septic shock monitored by pulmonary artery catheter. Blood was obtained simultaneously for SvcO2, SvO2 and SvaO2 determination. Linear correlation (significant if p<0.05) and agreement analysis (Bland-Altman) were performed with samples and subgroups according to cardiac output. Moreover, agreement about clinical management based on these samples was evaluated. RESULTS: Sixty one measurements from 23 patients were obtained, median age of 65.0 (49.0-75.0) years and mean APACHE II of 27.7±6.3. Mean values of SvO2, SvcO2 and SvaO2 were 72.20±8.26%, 74.61±7.60% and 74.64±8.47%. Linear correlation test showed a weak correlation between SvO2 and SvcO2 (r=0.61, p<0.0001) and also between SvO2 and SvaO2 (r=0.70, p<0.0001). Agreements between SvcO2/SvO2 and SvaO2/SvO2 were -2.40±1.96 (-16.20 and 11.40) and -2.40±1.96 (-15.10 and 10.20), respectively, with no difference in the cardiac output subgroups. No agreement was found in clinical management for 27.8% of the cases, both for SvcO2/SvO2 and for SvaO2/SvO2. CONCLUSION: This study showed that the correlation and agreement between SvO2 and SvcO2 is weak and may lead to different clinical management.
Views0Abstract
Original ArticlesCentral and mixed venous oxygen saturation in septic shock: is there a clinically relevant difference?
Rev Bras Ter Intensiva. 2008;20(4):398-404
DOI 10.1590/S0103-507X2008000400013
Views0See moreINTRODUCTION: Central venous oxygen saturation (SvcO2) has been proposed as an alternative for mixed venous oxygen saturation (SvO2), with a variable level of acceptance according to available data. This study aimed to evaluate possible differences between SvO2 and SvcO2 or atrial venous saturation (SvaO2), with emphasis on the role of cardiac output and their impact on clinical management of the septic patient. METHODS: This is an observational, prospective study of patients with septic shock monitored by pulmonary artery catheter. Blood was obtained simultaneously for SvcO2, SvO2 and SvaO2 determination. Linear correlation (significant if p<0.05) and agreement analysis (Bland-Altman) were performed with samples and subgroups according to cardiac output. Moreover, agreement about clinical management based on these samples was evaluated. RESULTS: Sixty one measurements from 23 patients were obtained, median age of 65.0 (49.0-75.0) years and mean APACHE II of 27.7±6.3. Mean values of SvO2, SvcO2 and SvaO2 were 72.20±8.26%, 74.61±7.60% and 74.64±8.47%. Linear correlation test showed a weak correlation between SvO2 and SvcO2 (r=0.61, p<0.0001) and also between SvO2 and SvaO2 (r=0.70, p<0.0001). Agreements between SvcO2/SvO2 and SvaO2/SvO2 were -2.40±1.96 (-16.20 and 11.40) and -2.40±1.96 (-15.10 and 10.20), respectively, with no difference in the cardiac output subgroups. No agreement was found in clinical management for 27.8% of the cases, both for SvcO2/SvO2 and for SvaO2/SvO2. CONCLUSION: This study showed that the correlation and agreement between SvO2 and SvcO2 is weak and may lead to different clinical management.
Search
Search in:
KEY WORDS
Case reports Child Coronavirus infections COVID-19 Critical care Critical illness Extracorporeal membrane oxygenation Infant, newborn Intensive care Intensive care units Intensive care units, pediatric mechanical ventilation Mortality Physical therapy modalities Prognosis Respiration, artificial Respiratory insufficiency risk factors SARS-CoV-2 Sepsis