ICU Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2008;20(1):68-76
DOI 10.1590/S0103-507X2008000100011
BACKGROUND AND OBJECTIVES: In this study we discuss about risks to health of intensive care unity staff and suggest a proposal of integral approach of health. CONTENTS: Literature review, from 1997 to 2007, at Bireme database about "health education", "intensive care unity", "nursing" and "occupational health", regardless of design of study. CONCLUSIONS: All studies show that the environment of intensive care unity is unhealthy, which is also due to habits and attitudes of ICU health professionals. An approach to health education would be beneficial to minimize the problem. Strategies for continuing education are appropriate both in the prevention of occupational and environmental risks in intensive care units.
Abstract
Rev Bras Ter Intensiva. 2008;20(1):68-76
DOI 10.1590/S0103-507X2008000100011
BACKGROUND AND OBJECTIVES: In this study we discuss about risks to health of intensive care unity staff and suggest a proposal of integral approach of health. CONTENTS: Literature review, from 1997 to 2007, at Bireme database about "health education", "intensive care unity", "nursing" and "occupational health", regardless of design of study. CONCLUSIONS: All studies show that the environment of intensive care unity is unhealthy, which is also due to habits and attitudes of ICU health professionals. An approach to health education would be beneficial to minimize the problem. Strategies for continuing education are appropriate both in the prevention of occupational and environmental risks in intensive care units.
Abstract
Rev Bras Ter Intensiva. 2008;20(1):106-109
DOI 10.1590/S0103-507X2008000100018
BACKGROUND AND OBJECTIVES: Infection with the non-Candida yeast species Trichosporon have been recognized with increasing frequency over the last two decades. Invasive disease due to trichosporonosis has been reported from neutropenic patients with cancer and the mortality is high. Recently, others groups of patients have become susceptible to this rare fungi. We report the emerging of infection with pathogenic Trichosporon asahii in severely ill heart failure patients in a tertiary cardiological intensive care unit (CICU). We describe our data, and report a fatal case of disseminated trichosporonosis in a patient with heart failure. We also review literature pertaining to T. asahii infections. CASE REPORT: An 85 year-old woman with a history of hypertension, heart failure (ejection fraction (EJ): 30%) and pulmonary embolism was admitted to a medical cardiological ICU after cardiac arrest (ventricular fibrillation) resuscitated during a routine consultation. There were no neurological sequelae and the echocardiogram revels no changes, neither the cardiac biomarkers. Ventricular fibrillation was considered secondary to heart failure. The patient had extubation failure and difficult weaning needing long term mechanical ventilation even after tracheostomy. Her hospital course was complicated by acute renal failure and recurrent respiratory, urinary and systemic bacterial infections, which responded to broad-spectrum antibiotics. After a temporary improvement she developed urinary infection and subsequent septic shock. Cultures of urine and blood specimens grew T. asahii. Treatment with liposome amphotericin B (5 mg/kg/day) was started. Despite receiving vancomycin and imipenem, the clinical condition of the patient deteriorates. Blood taken for culture on the seventh day of amphotericin B therapy were negative but urine specimen still grew T. asahii. On the eighteenth day of antifungal therapy, the patient died with multiorgan failure. CONCLUSIONS: The increasing of severely ill patients, and the use of broad spectrum antibiotics, has predisposed the emerging of invasive infections by rare and new opportunistic fungal pathogens. Severe infection related to T. asahii, until recently restricted to neutropenic patients with cancer, has been frequently identified in heart failure patients with advanced age. The mortality is high. These data highlights the importance of considering this group of patients as a risk group for T. asahii infection.
Abstract
Rev Bras Ter Intensiva. 2008;20(1):106-109
DOI 10.1590/S0103-507X2008000100018
BACKGROUND AND OBJECTIVES: Infection with the non-Candida yeast species Trichosporon have been recognized with increasing frequency over the last two decades. Invasive disease due to trichosporonosis has been reported from neutropenic patients with cancer and the mortality is high. Recently, others groups of patients have become susceptible to this rare fungi. We report the emerging of infection with pathogenic Trichosporon asahii in severely ill heart failure patients in a tertiary cardiological intensive care unit (CICU). We describe our data, and report a fatal case of disseminated trichosporonosis in a patient with heart failure. We also review literature pertaining to T. asahii infections. CASE REPORT: An 85 year-old woman with a history of hypertension, heart failure (ejection fraction (EJ): 30%) and pulmonary embolism was admitted to a medical cardiological ICU after cardiac arrest (ventricular fibrillation) resuscitated during a routine consultation. There were no neurological sequelae and the echocardiogram revels no changes, neither the cardiac biomarkers. Ventricular fibrillation was considered secondary to heart failure. The patient had extubation failure and difficult weaning needing long term mechanical ventilation even after tracheostomy. Her hospital course was complicated by acute renal failure and recurrent respiratory, urinary and systemic bacterial infections, which responded to broad-spectrum antibiotics. After a temporary improvement she developed urinary infection and subsequent septic shock. Cultures of urine and blood specimens grew T. asahii. Treatment with liposome amphotericin B (5 mg/kg/day) was started. Despite receiving vancomycin and imipenem, the clinical condition of the patient deteriorates. Blood taken for culture on the seventh day of amphotericin B therapy were negative but urine specimen still grew T. asahii. On the eighteenth day of antifungal therapy, the patient died with multiorgan failure. CONCLUSIONS: The increasing of severely ill patients, and the use of broad spectrum antibiotics, has predisposed the emerging of invasive infections by rare and new opportunistic fungal pathogens. Severe infection related to T. asahii, until recently restricted to neutropenic patients with cancer, has been frequently identified in heart failure patients with advanced age. The mortality is high. These data highlights the importance of considering this group of patients as a risk group for T. asahii infection.
Abstract
Rev Bras Ter Intensiva. 2008;20(1):24-30
DOI 10.1590/S0103-507X2008000100004
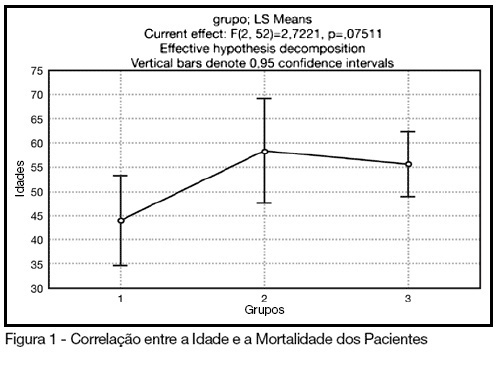
BACKGROUND AND OBJECTIVES: The control of patient discomfort in the intensive care unit (ICU) has become an integral part of critical care practice. The sedoanalgesic drugs could influence critically ill patient's morbimortality. Alpha²-adrenoceptor agonists might have an interesting future in ICU. The objective of this study is to evaluate the clonidine use for sedoanalgesia in ICU patients under prolonged mechanical ventilation. METHODS: Historical cohort study. Admitted patient files, January-December 2006, which stayed under mechanical ventilation, analgesia and sedation > 7days were analyzed. Demographic, clinical features and therapeutic data concerning analgesia and sedation were remarked. The data allowed classify the patients in three different groups: G1 = patients that used clonidine and other drugs; G2 = patients that used three or more drugs, without clonidine and G3 = patients that used fentanyl and midazolam. The mean daily doses of infused clonidine were registered, and the values of heat rate (HR), blood arterial pressure (BAP) before starting use of clonidine, after six hours and 24 hours were also registered. Statistical analyzes were performed using Variance Analysis (ANOVA), t tests and x² (significance p < 0.05). RESULTS: Were selected 55 patients. Fifteen (27.2%) belonged to G1, 11 (20%) belonged to G2 and 29 (52.7%) belonged to G3. The mean age of patients was 44 (G1), 50 (G2) and 56 (G3) (p = NS). The mean score APACHE II was 18 (G1), 20.4 (G2) and 20.7 (G3) (p = NS). G1 and G2 patients presented higher ICU length-of-stay (p < 0.05). The mean dose of clonidine used was 1.21 ± 0.54 mg/kg/min. G1 patients had HR and BAP decreased, however these effects were not considered clinically relevant. The mortality was lower in the patients from G1 (20%) when compared to G2 (54.5%) and G3 (62%) (p < 0.05). CONCLUSIONS: The clonidine use to analyzed patients did not result in clinical relevant side effects. The lower mortality index in patients that used clonidine was statistical significant.
Abstract
Rev Bras Ter Intensiva. 2008;20(1):24-30
DOI 10.1590/S0103-507X2008000100004
BACKGROUND AND OBJECTIVES: The control of patient discomfort in the intensive care unit (ICU) has become an integral part of critical care practice. The sedoanalgesic drugs could influence critically ill patient's morbimortality. Alpha²-adrenoceptor agonists might have an interesting future in ICU. The objective of this study is to evaluate the clonidine use for sedoanalgesia in ICU patients under prolonged mechanical ventilation. METHODS: Historical cohort study. Admitted patient files, January-December 2006, which stayed under mechanical ventilation, analgesia and sedation > 7days were analyzed. Demographic, clinical features and therapeutic data concerning analgesia and sedation were remarked. The data allowed classify the patients in three different groups: G1 = patients that used clonidine and other drugs; G2 = patients that used three or more drugs, without clonidine and G3 = patients that used fentanyl and midazolam. The mean daily doses of infused clonidine were registered, and the values of heat rate (HR), blood arterial pressure (BAP) before starting use of clonidine, after six hours and 24 hours were also registered. Statistical analyzes were performed using Variance Analysis (ANOVA), t tests and x² (significance p < 0.05). RESULTS: Were selected 55 patients. Fifteen (27.2%) belonged to G1, 11 (20%) belonged to G2 and 29 (52.7%) belonged to G3. The mean age of patients was 44 (G1), 50 (G2) and 56 (G3) (p = NS). The mean score APACHE II was 18 (G1), 20.4 (G2) and 20.7 (G3) (p = NS). G1 and G2 patients presented higher ICU length-of-stay (p < 0.05). The mean dose of clonidine used was 1.21 ± 0.54 mg/kg/min. G1 patients had HR and BAP decreased, however these effects were not considered clinically relevant. The mortality was lower in the patients from G1 (20%) when compared to G2 (54.5%) and G3 (62%) (p < 0.05). CONCLUSIONS: The clonidine use to analyzed patients did not result in clinical relevant side effects. The lower mortality index in patients that used clonidine was statistical significant.
Abstract
Rev Bras Ter Intensiva. 2006;18(4):412-417
DOI 10.1590/S0103-507X2006000400016
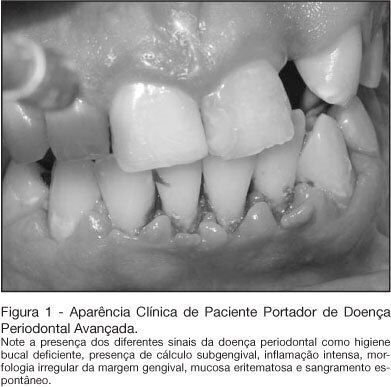
BACKGROUND AND OBJECTIVES: In the intensive care unit, the nosocomial respiratory infection is responsible for high rates of morbidity, mortality and expressive increase in hospitals costs. Its establishment feels more commonly by the aspiration of the content present within the mouth and the pharynx. Thus we intended to review the literature on the participation of the oral condition in the establishment of the nosocomial respiratory infection. CONTENTS: Deficient oral hygiene is common in patients under intensive care, which provides the colonization of oral biofilm for pathogenic microorganisms, especially for respiratory pathogens. The studies clearly show that the amount of oral biofilm in patients under intensive care increases according to period hospitalization meanwhile there also is an increase in respiratory pathogens. That colonizes the oral biofilm. This biofilm is an important resource of pathogens in patients under intensive care. CONCLUSIONS: In spite of well-established hypotheses that narrow down the relationships between lung infections and the oral condition, the studies are not still completely defined. However, due to strong possibilities that these hypotheses are true, it is necessary to have and maintain the oral health, in addition to more integration of dentistry and of Medicine, seeking patients' global treatment, the prevention of diseases, and more humanization at the intensive care unit.
Abstract
Rev Bras Ter Intensiva. 2006;18(4):412-417
DOI 10.1590/S0103-507X2006000400016
BACKGROUND AND OBJECTIVES: In the intensive care unit, the nosocomial respiratory infection is responsible for high rates of morbidity, mortality and expressive increase in hospitals costs. Its establishment feels more commonly by the aspiration of the content present within the mouth and the pharynx. Thus we intended to review the literature on the participation of the oral condition in the establishment of the nosocomial respiratory infection. CONTENTS: Deficient oral hygiene is common in patients under intensive care, which provides the colonization of oral biofilm for pathogenic microorganisms, especially for respiratory pathogens. The studies clearly show that the amount of oral biofilm in patients under intensive care increases according to period hospitalization meanwhile there also is an increase in respiratory pathogens. That colonizes the oral biofilm. This biofilm is an important resource of pathogens in patients under intensive care. CONCLUSIONS: In spite of well-established hypotheses that narrow down the relationships between lung infections and the oral condition, the studies are not still completely defined. However, due to strong possibilities that these hypotheses are true, it is necessary to have and maintain the oral health, in addition to more integration of dentistry and of Medicine, seeking patients' global treatment, the prevention of diseases, and more humanization at the intensive care unit.
Abstract
Rev Bras Ter Intensiva. 2007;19(4):485-489
DOI 10.1590/S0103-507X2007000400014
BACKGROUND AND OBJECTIVES: The suffering with the death and the prolonged time of patient's admission in a intensive care unit (ICU) are factors that leads to necessity the best communication with the personal that works in ICU, patients and their family, and its justify this work, whose objective is discuss this subject. CONTENTS: The professional experience of the author was used in this issue and the articles written during the last five years about death, communication and ICU were reviewed by means of MedLine, Up to Date, Google and Brazilian Journal of Intensive Therapy. CONCLUSIONS: It was concluded that the physician, the patient together with her/his family, and the multiprofessional staff of the ICU is one of the main factors that interferes with the process of satisfying both the patient and the ones who work on such unities. For adequate information, the physician must be conscious about therapeutic limits, and must learn how to treat the patient during the process of dying. In this way, the physician will be apt to talk about death. The ideal situation would be that the professional, responsible to give the news, should be experience, from the technical point of view as well as ethical, and should be the same person, as always as possible, when necessary. The patient mostly little be able to influence in her/his process of dying, but if communication is possible, it be simple, honest and humane. The patient's family members have the right of being together with the one who they love, and of being steadily informed about the real situation. All the members in the process must know the truth and the chosen therapeutic orientation to be taken. Communication should be done in a quiet and prived place.
Abstract
Rev Bras Ter Intensiva. 2007;19(4):485-489
DOI 10.1590/S0103-507X2007000400014
BACKGROUND AND OBJECTIVES: The suffering with the death and the prolonged time of patient's admission in a intensive care unit (ICU) are factors that leads to necessity the best communication with the personal that works in ICU, patients and their family, and its justify this work, whose objective is discuss this subject. CONTENTS: The professional experience of the author was used in this issue and the articles written during the last five years about death, communication and ICU were reviewed by means of MedLine, Up to Date, Google and Brazilian Journal of Intensive Therapy. CONCLUSIONS: It was concluded that the physician, the patient together with her/his family, and the multiprofessional staff of the ICU is one of the main factors that interferes with the process of satisfying both the patient and the ones who work on such unities. For adequate information, the physician must be conscious about therapeutic limits, and must learn how to treat the patient during the process of dying. In this way, the physician will be apt to talk about death. The ideal situation would be that the professional, responsible to give the news, should be experience, from the technical point of view as well as ethical, and should be the same person, as always as possible, when necessary. The patient mostly little be able to influence in her/his process of dying, but if communication is possible, it be simple, honest and humane. The patient's family members have the right of being together with the one who they love, and of being steadily informed about the real situation. All the members in the process must know the truth and the chosen therapeutic orientation to be taken. Communication should be done in a quiet and prived place.
Abstract
Rev Bras Ter Intensiva. 2007;19(4):434-436
DOI 10.1590/S0103-507X2007000400005
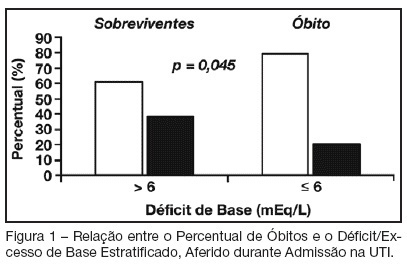
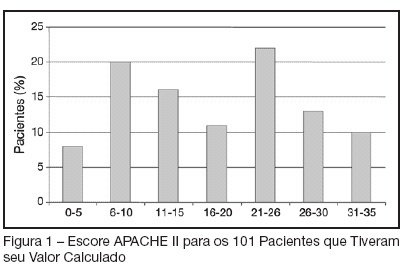
BACKGROUND AND OBJECTIVES: Base deficit is considered an indicator of tissue injury, shock and resuscitation. The objective of this study was to establish an association between base deficit obtained on the admission of patients in intensive care unit (ICU) and their prognosis. METHODS: A retrospective study with analysis of 110 patients admitted consecutively in the ICU, during the period of June to December 2006. RESULTS: There was a predominance of women, with age mean 54.2 ± 18.7 years old. Length of stay in ICU was 6.5 ± 7.4 days and the mean APACHE II score was 21 ± 8.1 points. The standardized mortality ratio was 0.715. Mortality was higher in patients with base deficit > 6 mEq/L (38.9%) than in those with base deficit < 6 mEq/L (20.6%); p < 0.05. Patients with early mortality had lower base deficit (7.75 ± 8.33 mEq/L) than survivors (3.17 ± 5.43 mEq/L); p < 0.05. Patients with permanence in ICU until 7 days and patients that stayed in this unit for more than 7 days had similar base deficit. CONCLUSIONS: Base deficit had been associated with early mortality during ICU internment. Base deficit > 6 mEq/L is a marker of significant mortality.
Abstract
Rev Bras Ter Intensiva. 2007;19(4):434-436
DOI 10.1590/S0103-507X2007000400005
BACKGROUND AND OBJECTIVES: Base deficit is considered an indicator of tissue injury, shock and resuscitation. The objective of this study was to establish an association between base deficit obtained on the admission of patients in intensive care unit (ICU) and their prognosis. METHODS: A retrospective study with analysis of 110 patients admitted consecutively in the ICU, during the period of June to December 2006. RESULTS: There was a predominance of women, with age mean 54.2 ± 18.7 years old. Length of stay in ICU was 6.5 ± 7.4 days and the mean APACHE II score was 21 ± 8.1 points. The standardized mortality ratio was 0.715. Mortality was higher in patients with base deficit > 6 mEq/L (38.9%) than in those with base deficit < 6 mEq/L (20.6%); p < 0.05. Patients with early mortality had lower base deficit (7.75 ± 8.33 mEq/L) than survivors (3.17 ± 5.43 mEq/L); p < 0.05. Patients with permanence in ICU until 7 days and patients that stayed in this unit for more than 7 days had similar base deficit. CONCLUSIONS: Base deficit had been associated with early mortality during ICU internment. Base deficit > 6 mEq/L is a marker of significant mortality.
Abstract
Rev Bras Ter Intensiva. 2007;19(4):456-462
DOI 10.1590/S0103-507X2007000400009
BACKGROUND AND OBJECTIVES: There are deficiencies on Intensive Medicine (IM) teaching in most of medical undergraduate schools. Those deficiencies may imply damages on their clinical competence. The objective of this study was to analyze current status of IM teaching and the medical undergraduate student interest in this speciality. METHODS: A cross-sectional study was performed in 2005. We applied a self-reported questionnaire to enrolled students between the sixth and the last semesters of two medical schools from Salvador-Bahia. The questionnaire contained questions about students' interest and knowledge on IM, and opinion on IM teaching in their schools. RESULTS: We studied 570 students. Most of them (57.5%) had never realized a clerkship in intensive care unit (ICU) despite classifying its usefulness as high (mean of 4.14 ± 1.05, in a scale from 1 to 5). IM interest was high or very high in 53.7% of sample. Almost all students (97%) thought that IM topics should be more explored at their curriculum. Only 42.1% reported to be able to assess a critical care patient and this assurance was higher among students with previous clerkship in ICU (p < 0.001). Shock, cardiopulmonary resuscitation and sepsis were the most interesting topics in ICU for students' opinion. CONCLUSIONS: This study revealed a high interest in IM among medical undergraduate students. However, most had never practice a clerkship in ICU, demonstrating to be an important factor on undergraduate student performance faced to a critical care patient.
Abstract
Rev Bras Ter Intensiva. 2007;19(4):456-462
DOI 10.1590/S0103-507X2007000400009
BACKGROUND AND OBJECTIVES: There are deficiencies on Intensive Medicine (IM) teaching in most of medical undergraduate schools. Those deficiencies may imply damages on their clinical competence. The objective of this study was to analyze current status of IM teaching and the medical undergraduate student interest in this speciality. METHODS: A cross-sectional study was performed in 2005. We applied a self-reported questionnaire to enrolled students between the sixth and the last semesters of two medical schools from Salvador-Bahia. The questionnaire contained questions about students' interest and knowledge on IM, and opinion on IM teaching in their schools. RESULTS: We studied 570 students. Most of them (57.5%) had never realized a clerkship in intensive care unit (ICU) despite classifying its usefulness as high (mean of 4.14 ± 1.05, in a scale from 1 to 5). IM interest was high or very high in 53.7% of sample. Almost all students (97%) thought that IM topics should be more explored at their curriculum. Only 42.1% reported to be able to assess a critical care patient and this assurance was higher among students with previous clerkship in ICU (p < 0.001). Shock, cardiopulmonary resuscitation and sepsis were the most interesting topics in ICU for students' opinion. CONCLUSIONS: This study revealed a high interest in IM among medical undergraduate students. However, most had never practice a clerkship in ICU, demonstrating to be an important factor on undergraduate student performance faced to a critical care patient.
Abstract
Rev Bras Ter Intensiva. 2007;19(4):414-420
DOI 10.1590/S0103-507X2007000400002
BACKGROUND AND OBJECTIVES: To determine the prevalence of intensive care unit (ICU)-acquired infections and the risk factors for these infections, identify the predominant infecting organisms, and evaluate the relationship between ICU-acquired infection and mortality. METHODS: A 1-day point prevalence study. Sixteen ICU of the State of Rio Grande do Sul-Brazil, excluding coronary care and pediatric units. All patients < 12 yrs occupying an ICU bed over a 24-hour period. The 16 ICU provided 174 case reports. Main outcomes: rates of ICU-acquired infection, resistance patterns of microbiological isolates, and potential risks factors for ICU-acquired infection and death. RESULTS: A total of 122 patients (71%) was infected and 51 (29%) had ICU-acquired infection. Pneumonia (58.2%), lower tract respiratory infection (22.9%), urinary tract infection (18%) were the most frequents types of ICU infection. Most frequently microorganisms reported were staphylococcus aureus (42% [64% resistant to oxacilin]) and pseudomonas aeruginosa (31%). Six risk factors for ICU acquired infection were identified: urinary catheterization, central vascular line, tracheal intubation for prolonged time (> 4 days), chronic disease and increased length of ICU stay (> 30 days). The risks factors associated with death were age, APACHE II, organ dysfunction, and tracheal intubation with or without mechanical ventilation. CONCLUSIONS: ICU-acquired infection is common and often associated with microbiological isolates of resistant organisms. This study may serve as an epidemiological reference to help the discussion of regional infection control policies.
Abstract
Rev Bras Ter Intensiva. 2007;19(4):414-420
DOI 10.1590/S0103-507X2007000400002
BACKGROUND AND OBJECTIVES: To determine the prevalence of intensive care unit (ICU)-acquired infections and the risk factors for these infections, identify the predominant infecting organisms, and evaluate the relationship between ICU-acquired infection and mortality. METHODS: A 1-day point prevalence study. Sixteen ICU of the State of Rio Grande do Sul-Brazil, excluding coronary care and pediatric units. All patients < 12 yrs occupying an ICU bed over a 24-hour period. The 16 ICU provided 174 case reports. Main outcomes: rates of ICU-acquired infection, resistance patterns of microbiological isolates, and potential risks factors for ICU-acquired infection and death. RESULTS: A total of 122 patients (71%) was infected and 51 (29%) had ICU-acquired infection. Pneumonia (58.2%), lower tract respiratory infection (22.9%), urinary tract infection (18%) were the most frequents types of ICU infection. Most frequently microorganisms reported were staphylococcus aureus (42% [64% resistant to oxacilin]) and pseudomonas aeruginosa (31%). Six risk factors for ICU acquired infection were identified: urinary catheterization, central vascular line, tracheal intubation for prolonged time (> 4 days), chronic disease and increased length of ICU stay (> 30 days). The risks factors associated with death were age, APACHE II, organ dysfunction, and tracheal intubation with or without mechanical ventilation. CONCLUSIONS: ICU-acquired infection is common and often associated with microbiological isolates of resistant organisms. This study may serve as an epidemiological reference to help the discussion of regional infection control policies.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (116) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)