
You searched for:"Arnaldo Aires Peixoto Júnior"
We found (5) results for your search.-
Original Articles
Pharmacist recommendations in an intensive care unit: three-year clinical activities
Rev Bras Ter Intensiva. 2015;27(2):149-154
Abstract
Original ArticlesPharmacist recommendations in an intensive care unit: three-year clinical activities
Rev Bras Ter Intensiva. 2015;27(2):149-154
DOI 10.5935/0103-507X.20150026
Views0See moreABSTRACT
Objective:
To analyze the clinical activities performed and the accepted pharmacist recommendations made by a pharmacist as a part of his/her daily routine in an adult clinical intensive care unit over a period of three years.
Methods:
A cross-sectional, descriptive, and exploratory study was conducted at a tertiary university hospital from June 2010 to May 2013, in which pharmacist recommendations were categorized and analyzed.
Results:
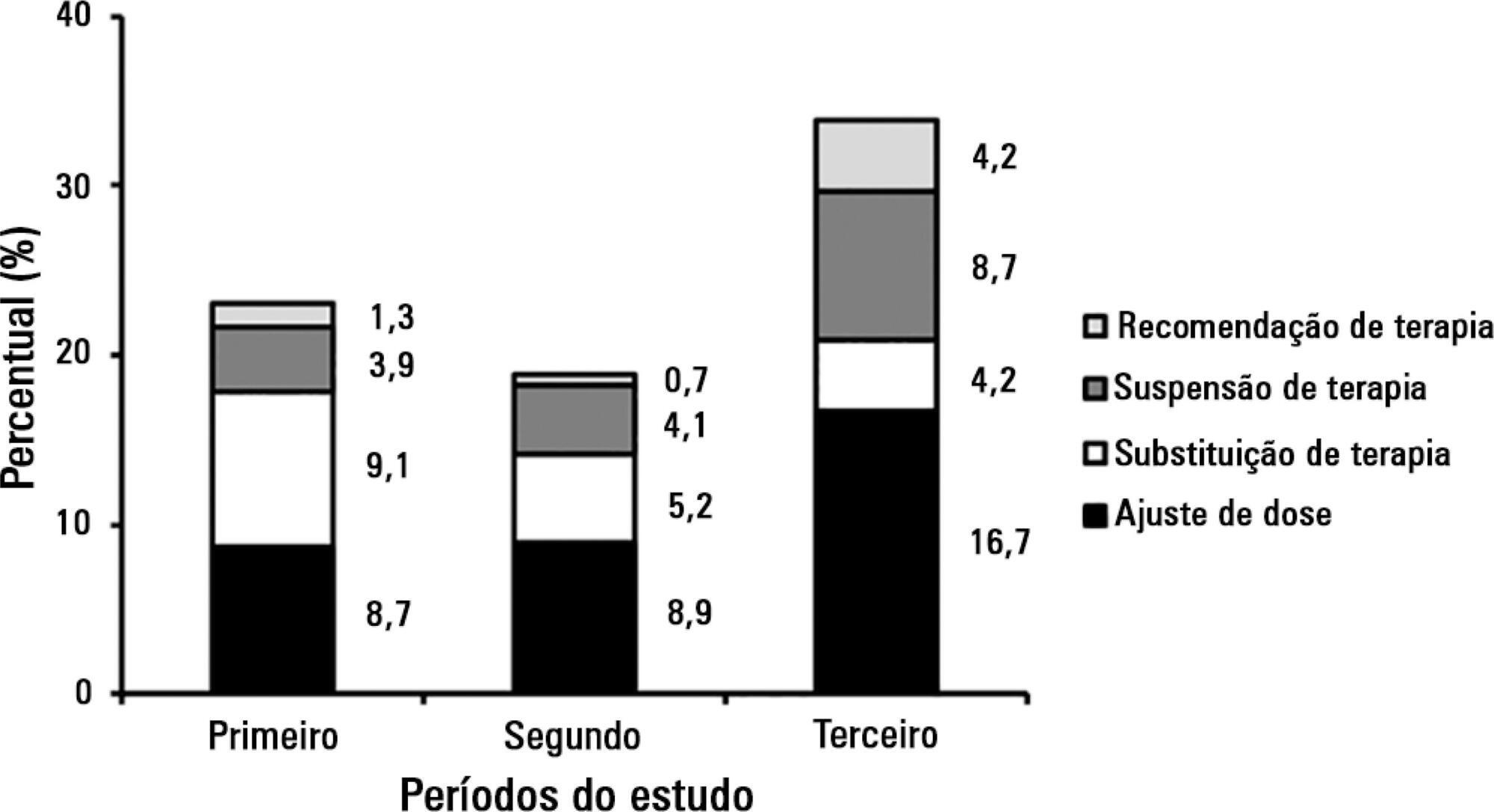
A total of 834 pharmacist recommendations (278 per year, on average) were analyzed and distributed across 21 categories. The recommendations were mainly made to physicians (n = 699; 83.8%) and concerned management of dilutions (n = 120; 14.4%), dose adjustment (n = 100; 12.0%), and adverse drug reactions (n = 91; 10.9%). A comparison per period demonstrated an increase in pharmacist recommendations with larger clinical content and a reduction of recommendations related to logistic aspects, such as drug supply, over time. The recommendations concerned 948 medications, particularly including systemic anti-infectious agents.
Conclusion:
The role that the pharmacist played in the intensive care unit of the institution where the study was performed evolved, shifting from reactive actions related to logistic aspects to effective clinical participation with the multi-professional staff (proactive actions).
Views0

Abstract
Original ArticlesPharmacist recommendations in an intensive care unit: three-year clinical activities
Rev Bras Ter Intensiva. 2015;27(2):149-154
DOI 10.5935/0103-507X.20150026
Views0See moreABSTRACT
Objective:
To analyze the clinical activities performed and the accepted pharmacist recommendations made by a pharmacist as a part of his/her daily routine in an adult clinical intensive care unit over a period of three years.
Methods:
A cross-sectional, descriptive, and exploratory study was conducted at a tertiary university hospital from June 2010 to May 2013, in which pharmacist recommendations were categorized and analyzed.
Results:
A total of 834 pharmacist recommendations (278 per year, on average) were analyzed and distributed across 21 categories. The recommendations were mainly made to physicians (n = 699; 83.8%) and concerned management of dilutions (n = 120; 14.4%), dose adjustment (n = 100; 12.0%), and adverse drug reactions (n = 91; 10.9%). A comparison per period demonstrated an increase in pharmacist recommendations with larger clinical content and a reduction of recommendations related to logistic aspects, such as drug supply, over time. The recommendations concerned 948 medications, particularly including systemic anti-infectious agents.
Conclusion:
The role that the pharmacist played in the intensive care unit of the institution where the study was performed evolved, shifting from reactive actions related to logistic aspects to effective clinical participation with the multi-professional staff (proactive actions).
-
Original Articles – Clinical Research
Gender and mortality in sepsis: do sex hormones impact the outcome?
Rev Bras Ter Intensiva. 2011;23(3):297-303
Abstract
Original Articles – Clinical ResearchGender and mortality in sepsis: do sex hormones impact the outcome?
Rev Bras Ter Intensiva. 2011;23(3):297-303
DOI 10.1590/S0103-507X2011000300007
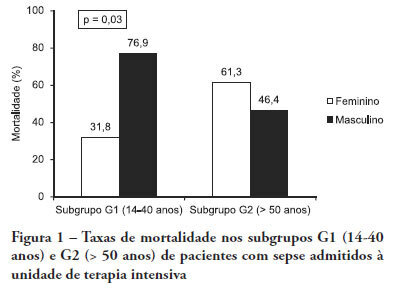
Views0See moreOBJECTIVE: Comparative assessment of the mortality rates of two septic patients’ ages and/or gender subgroups, admitted to the intensive care unit of a university hospital. METHODS: From December 2005 to April 2008, from a total of 628 patients, 133 were admitted to the intensive care unit with sepsis and included into two age subgroups: (G1) 14 – 40 years old and (G2) more than 50 years old. Patients aged between 41 and 50 years old (n = 8) were excluded. Demographic data, prognostic indicators (APACHE II score, organ dysfunction and circulatory shock) and outcome (mortality) were analyzed. RESULTS: Of the G1 patients (n = 44), 27 were female (61.4%), and in G2 (n = 81), 40 were female (49.4%). For both groups, mean APACHE II scores, multi-organ dysfunction and progression to circulatory shock rates were not significantly different between female and male patients. For G1, overall mortality rate was lower in female than in male patients (P = 0.04), while for G2, the opposite trend was observed. CONCLUSIONS: In this sample, reproductive age female patients younger than 40 years old showed lower mortality rates compared with age-matched male patients; for patients older than 50 years old, male patients had lower mortality rates than female patients.
Views0Abstract
Original Articles – Clinical ResearchGender and mortality in sepsis: do sex hormones impact the outcome?
Rev Bras Ter Intensiva. 2011;23(3):297-303
DOI 10.1590/S0103-507X2011000300007
Views0See moreOBJECTIVE: Comparative assessment of the mortality rates of two septic patients’ ages and/or gender subgroups, admitted to the intensive care unit of a university hospital. METHODS: From December 2005 to April 2008, from a total of 628 patients, 133 were admitted to the intensive care unit with sepsis and included into two age subgroups: (G1) 14 – 40 years old and (G2) more than 50 years old. Patients aged between 41 and 50 years old (n = 8) were excluded. Demographic data, prognostic indicators (APACHE II score, organ dysfunction and circulatory shock) and outcome (mortality) were analyzed. RESULTS: Of the G1 patients (n = 44), 27 were female (61.4%), and in G2 (n = 81), 40 were female (49.4%). For both groups, mean APACHE II scores, multi-organ dysfunction and progression to circulatory shock rates were not significantly different between female and male patients. For G1, overall mortality rate was lower in female than in male patients (P = 0.04), while for G2, the opposite trend was observed. CONCLUSIONS: In this sample, reproductive age female patients younger than 40 years old showed lower mortality rates compared with age-matched male patients; for patients older than 50 years old, male patients had lower mortality rates than female patients.
-
Original Articles
Validation of an early warning score in pre-intensive care unit
Rev Bras Ter Intensiva. 2008;20(2):124-127
Abstract
Original ArticlesValidation of an early warning score in pre-intensive care unit
Rev Bras Ter Intensiva. 2008;20(2):124-127
DOI 10.1590/S0103-507X2008000200002
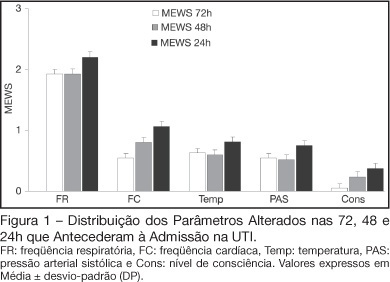
Views0See moreBACKGROUND AND OBJECTIVES: Prognosis of patients in the intensive care unit (ICU) has a relation with their severity just before admission. The Modified Early Warning Score (MEWS) was used to evaluate the severe condition of patients 12, 24 and 72 hours before admission in the ICU, assess the most prevalent parameters and correlate the MEWS before ICU with the outcome (survival versus death). METHODS: Retrospective analyses of 65 patients consecutively admitted to the ICU from July to October, 2006 evaluating the physiological parameters 72 hours prior to admission. RESULTS: APACHE II mean was 22.2 ± 7.9 points, mortality was 54.6% and standardized mortality ratio means was 1.24. MEWS means were 3.7 ± 0.2; 4.0 ± 0.2 and 5.1 ± 0.2 points, calculated 72, 48 and 24 hours previous to ICU admission, respectively. An increasing percentage of patients with MEWS > 3 points within 72, 48 and 24 hours before admission – 43.8%, 59.4% and 73.4%, respectively was recorded. Among the included physiological parameters respiratory rate contributed the most to the MEWS. Highest mortality was found in patients with MEWS > 3 points already found 72 hours before admission. Patients who died presented with a significant increase in the MEWS 24 hours prior to admission to the ICU (in relation to the MEWS recorded 72 hours before) but the situation was not identified in survivors. CONCLUSIONS: MEWS closely identified the severity of patients admitted to the ICU, suggesting that it can be a reliable score, useful in the situations preceding the ICU.
Views0Abstract
Original ArticlesValidation of an early warning score in pre-intensive care unit
Rev Bras Ter Intensiva. 2008;20(2):124-127
DOI 10.1590/S0103-507X2008000200002
Views0See moreBACKGROUND AND OBJECTIVES: Prognosis of patients in the intensive care unit (ICU) has a relation with their severity just before admission. The Modified Early Warning Score (MEWS) was used to evaluate the severe condition of patients 12, 24 and 72 hours before admission in the ICU, assess the most prevalent parameters and correlate the MEWS before ICU with the outcome (survival versus death). METHODS: Retrospective analyses of 65 patients consecutively admitted to the ICU from July to October, 2006 evaluating the physiological parameters 72 hours prior to admission. RESULTS: APACHE II mean was 22.2 ± 7.9 points, mortality was 54.6% and standardized mortality ratio means was 1.24. MEWS means were 3.7 ± 0.2; 4.0 ± 0.2 and 5.1 ± 0.2 points, calculated 72, 48 and 24 hours previous to ICU admission, respectively. An increasing percentage of patients with MEWS > 3 points within 72, 48 and 24 hours before admission – 43.8%, 59.4% and 73.4%, respectively was recorded. Among the included physiological parameters respiratory rate contributed the most to the MEWS. Highest mortality was found in patients with MEWS > 3 points already found 72 hours before admission. Patients who died presented with a significant increase in the MEWS 24 hours prior to admission to the ICU (in relation to the MEWS recorded 72 hours before) but the situation was not identified in survivors. CONCLUSIONS: MEWS closely identified the severity of patients admitted to the ICU, suggesting that it can be a reliable score, useful in the situations preceding the ICU.
-
Morbidity and mortality of elderly patients admitted to an Intensive Care Unit of a University Hospital in Fortaleza
Rev Bras Ter Intensiva. 2006;18(3):263-267
Abstract
Morbidity and mortality of elderly patients admitted to an Intensive Care Unit of a University Hospital in Fortaleza
Rev Bras Ter Intensiva. 2006;18(3):263-267
DOI 10.1590/S0103-507X2006000300008
Views0See moreBACKGROUND AND OBJECTIVES: To identify the severity of elderly patients admitted to the intensive care unit (ICU) in a university hospital, relating it to the in-ICU mortality. METHODS: Retrospective study, with analysis of 130 patients admitted to ICU from March 2004 to July 2005. RESULTS: Of the 130 patients, there was a predominance of women, and mean 72.2 ± 7.3 years. There were more patients between 65 and 74 years old. More than 80% of the patients had come from the university hospital itself. The main dysfunctions were from the cardiocirculatory and respiratory systems. Sepsis caused 23.8% of the admissions. Length of stay in ICU was 8.2 ± 7.6 days. The mean of APACHE II was 18.2 ± 7.2. Lesser values of APACHE II, length of stay and mortality were observed in patients with cardiocirculatory dysfunction. The in-ICU mortality was 33.9%, 6.2% before 48 hours. The standardized mortality ratio (SMR) was 0.988. CONCLUSIONS: The age groups did not determine difference between values of APACHE II. They were related neither to higher mortality rate, nor to higher ICU length of stay. Patients with cardiocirculatory dysfunctions had lesser values of APACHE II, ICU length of stay and in-ICU mortality.
Views0Abstract
Morbidity and mortality of elderly patients admitted to an Intensive Care Unit of a University Hospital in Fortaleza
Rev Bras Ter Intensiva. 2006;18(3):263-267
DOI 10.1590/S0103-507X2006000300008
Views0See moreBACKGROUND AND OBJECTIVES: To identify the severity of elderly patients admitted to the intensive care unit (ICU) in a university hospital, relating it to the in-ICU mortality. METHODS: Retrospective study, with analysis of 130 patients admitted to ICU from March 2004 to July 2005. RESULTS: Of the 130 patients, there was a predominance of women, and mean 72.2 ± 7.3 years. There were more patients between 65 and 74 years old. More than 80% of the patients had come from the university hospital itself. The main dysfunctions were from the cardiocirculatory and respiratory systems. Sepsis caused 23.8% of the admissions. Length of stay in ICU was 8.2 ± 7.6 days. The mean of APACHE II was 18.2 ± 7.2. Lesser values of APACHE II, length of stay and mortality were observed in patients with cardiocirculatory dysfunction. The in-ICU mortality was 33.9%, 6.2% before 48 hours. The standardized mortality ratio (SMR) was 0.988. CONCLUSIONS: The age groups did not determine difference between values of APACHE II. They were related neither to higher mortality rate, nor to higher ICU length of stay. Patients with cardiocirculatory dysfunctions had lesser values of APACHE II, ICU length of stay and in-ICU mortality.
-
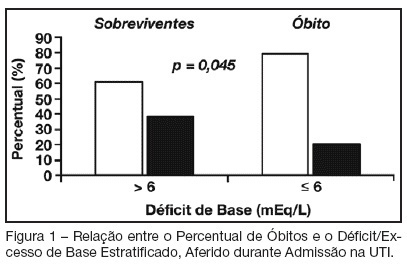
Base deficit at intensive care unit admission: an early mortality indicator
Rev Bras Ter Intensiva. 2007;19(4):434-436
Abstract
Base deficit at intensive care unit admission: an early mortality indicator
Rev Bras Ter Intensiva. 2007;19(4):434-436
DOI 10.1590/S0103-507X2007000400005
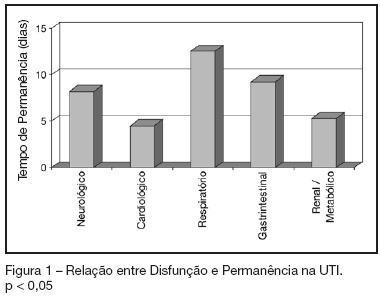
Views0See moreBACKGROUND AND OBJECTIVES: Base deficit is considered an indicator of tissue injury, shock and resuscitation. The objective of this study was to establish an association between base deficit obtained on the admission of patients in intensive care unit (ICU) and their prognosis. METHODS: A retrospective study with analysis of 110 patients admitted consecutively in the ICU, during the period of June to December 2006. RESULTS: There was a predominance of women, with age mean 54.2 ± 18.7 years old. Length of stay in ICU was 6.5 ± 7.4 days and the mean APACHE II score was 21 ± 8.1 points. The standardized mortality ratio was 0.715. Mortality was higher in patients with base deficit > 6 mEq/L (38.9%) than in those with base deficit < 6 mEq/L (20.6%); p < 0.05. Patients with early mortality had lower base deficit (7.75 ± 8.33 mEq/L) than survivors (3.17 ± 5.43 mEq/L); p < 0.05. Patients with permanence in ICU until 7 days and patients that stayed in this unit for more than 7 days had similar base deficit. CONCLUSIONS: Base deficit had been associated with early mortality during ICU internment. Base deficit > 6 mEq/L is a marker of significant mortality.
Views0Abstract
Base deficit at intensive care unit admission: an early mortality indicator
Rev Bras Ter Intensiva. 2007;19(4):434-436
DOI 10.1590/S0103-507X2007000400005
Views0See moreBACKGROUND AND OBJECTIVES: Base deficit is considered an indicator of tissue injury, shock and resuscitation. The objective of this study was to establish an association between base deficit obtained on the admission of patients in intensive care unit (ICU) and their prognosis. METHODS: A retrospective study with analysis of 110 patients admitted consecutively in the ICU, during the period of June to December 2006. RESULTS: There was a predominance of women, with age mean 54.2 ± 18.7 years old. Length of stay in ICU was 6.5 ± 7.4 days and the mean APACHE II score was 21 ± 8.1 points. The standardized mortality ratio was 0.715. Mortality was higher in patients with base deficit > 6 mEq/L (38.9%) than in those with base deficit < 6 mEq/L (20.6%); p < 0.05. Patients with early mortality had lower base deficit (7.75 ± 8.33 mEq/L) than survivors (3.17 ± 5.43 mEq/L); p < 0.05. Patients with permanence in ICU until 7 days and patients that stayed in this unit for more than 7 days had similar base deficit. CONCLUSIONS: Base deficit had been associated with early mortality during ICU internment. Base deficit > 6 mEq/L is a marker of significant mortality.
Search
Search in:
KEY WORDS
Case reports Child Coronavirus infections COVID-19 Critical care Critical illness Extracorporeal membrane oxygenation Infant, newborn Intensive care Intensive care units Intensive care units, pediatric mechanical ventilation Mortality Physical therapy modalities Prognosis Respiration, artificial Respiratory insufficiency risk factors SARS-CoV-2 Sepsis