Renal insufficiency Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2013;25(3):251-257
DOI 10.5935/0103-507X.20130044
To assess the oxygenation behavior and ventilatory mechanics after hemodialysis in patients under ventilatory support.
The present study was performed in the general intensive care unit of a tertiary public hospital. Patients over 18 years of age under mechanical ventilation and in need of dialysis support were included. Each patient was submitted to 2 evaluations (pre- and post-dialysis) regarding the cardiovascular and ventilatory parameters, the ventilatory mechanics and a laboratory evaluation.
Eighty patients with acute or chronic renal failure were included. The analysis of the ventilatory mechanics revealed a reduction in the plateau pressure and an increased static compliance after dialysis that was independent of a reduction in blood volume. The patients with acute renal failure also exhibited a reduction in peak pressure (p=0.024) and an increase in the dynamic compliance (p=0.026), whereas the patients with chronic renal failure exhibited an increase in the resistive pressure (p=0.046) and in the resistance of the respiratory system (p=0.044). The group of patients with no loss of blood volume after dialysis exhibited an increase in the resistive pressure (p=0.010) and in the resistance of the respiratory system (p=0.020), whereas the group with a loss of blood volume >2,000mL exhibited a reduction in the peak pressure (p=0.027). No changes in the partial pressure of oxygen in arterial blood (PaO2) or in the PaO2/the fraction of inspired oxygen (PaO2/FiO2) ratio were observed.
Hemodialysis was able to alter the mechanics of the respiratory system and specifically reduced the plateau pressure and increased the static compliance independent of a reduction in blood volume.
Abstract
Rev Bras Ter Intensiva. 2013;25(3):251-257
DOI 10.5935/0103-507X.20130044
To assess the oxygenation behavior and ventilatory mechanics after hemodialysis in patients under ventilatory support.
The present study was performed in the general intensive care unit of a tertiary public hospital. Patients over 18 years of age under mechanical ventilation and in need of dialysis support were included. Each patient was submitted to 2 evaluations (pre- and post-dialysis) regarding the cardiovascular and ventilatory parameters, the ventilatory mechanics and a laboratory evaluation.
Eighty patients with acute or chronic renal failure were included. The analysis of the ventilatory mechanics revealed a reduction in the plateau pressure and an increased static compliance after dialysis that was independent of a reduction in blood volume. The patients with acute renal failure also exhibited a reduction in peak pressure (p=0.024) and an increase in the dynamic compliance (p=0.026), whereas the patients with chronic renal failure exhibited an increase in the resistive pressure (p=0.046) and in the resistance of the respiratory system (p=0.044). The group of patients with no loss of blood volume after dialysis exhibited an increase in the resistive pressure (p=0.010) and in the resistance of the respiratory system (p=0.020), whereas the group with a loss of blood volume >2,000mL exhibited a reduction in the peak pressure (p=0.027). No changes in the partial pressure of oxygen in arterial blood (PaO2) or in the PaO2/the fraction of inspired oxygen (PaO2/FiO2) ratio were observed.
Hemodialysis was able to alter the mechanics of the respiratory system and specifically reduced the plateau pressure and increased the static compliance independent of a reduction in blood volume.
Abstract
Rev Bras Ter Intensiva. 2012;24(3):219-223
DOI 10.1590/S0103-507X2012000300003
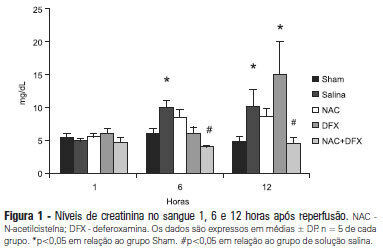
OBJECTIVE: Antioxidants are widely used in animal models to prevent renal injury after ischemia/reperfusion, but it is unknown if the benefits of antioxidants are additive. In this study, we aimed to investigate the protective effects of N-acetylcysteine plus deferoxamine in an animal model of kidney ischemia/reperfusion injury. METHODS: Bilateral kidney ischemia was mastintained for 45 minutes. N-acetylcysteine, deferoxamine or both were administered into the aorta above the renal arteries immediately prior to induction of ischemia. Five rats from each group were sacrificed 1, 6 or 12 hours after reperfusion for the determination of blood creatinine, kidney oxidative damage parameters and myeloperoxidase activity. RESULTS: The combination of N-acetylcysteine and deferoxamine, but not their isolated use, prevented the increase in creatinine after ischemia/reperfusion. This prevention was followed by a consistent decrease in myeloperoxidase activity and oxidative damage parameters both in the kidney cortex and medulla. CONCLUSION: Treatment with N-acetylcysteine and deferoxamine was superior to the isolated use of either compound in an animal model of kidney ischemia/reperfusion.
Abstract
Rev Bras Ter Intensiva. 2012;24(3):219-223
DOI 10.1590/S0103-507X2012000300003
OBJECTIVE: Antioxidants are widely used in animal models to prevent renal injury after ischemia/reperfusion, but it is unknown if the benefits of antioxidants are additive. In this study, we aimed to investigate the protective effects of N-acetylcysteine plus deferoxamine in an animal model of kidney ischemia/reperfusion injury. METHODS: Bilateral kidney ischemia was mastintained for 45 minutes. N-acetylcysteine, deferoxamine or both were administered into the aorta above the renal arteries immediately prior to induction of ischemia. Five rats from each group were sacrificed 1, 6 or 12 hours after reperfusion for the determination of blood creatinine, kidney oxidative damage parameters and myeloperoxidase activity. RESULTS: The combination of N-acetylcysteine and deferoxamine, but not their isolated use, prevented the increase in creatinine after ischemia/reperfusion. This prevention was followed by a consistent decrease in myeloperoxidase activity and oxidative damage parameters both in the kidney cortex and medulla. CONCLUSION: Treatment with N-acetylcysteine and deferoxamine was superior to the isolated use of either compound in an animal model of kidney ischemia/reperfusion.
Abstract
Rev Bras Ter Intensiva. 2011;23(4):507-509
DOI 10.1590/S0103-507X2011000400017
The authors report the case of an immunocompetent man who presented with acute impairment of the neurological system, hypertensive crisis and renal failure. The patient was eventually diagnosed with Rhodotorula mucilaginosa meningitis and infective endocarditis. To the best of our knowledge, this is the first description of simultaneous infection of the meninges and endothelium caused by Rhodotorula in a non-immunocompromised patient.
Abstract
Rev Bras Ter Intensiva. 2011;23(4):507-509
DOI 10.1590/S0103-507X2011000400017
The authors report the case of an immunocompetent man who presented with acute impairment of the neurological system, hypertensive crisis and renal failure. The patient was eventually diagnosed with Rhodotorula mucilaginosa meningitis and infective endocarditis. To the best of our knowledge, this is the first description of simultaneous infection of the meninges and endothelium caused by Rhodotorula in a non-immunocompromised patient.
Abstract
Rev Bras Ter Intensiva. 2006;18(3):282-291
DOI 10.1590/S0103-507X2006000300011
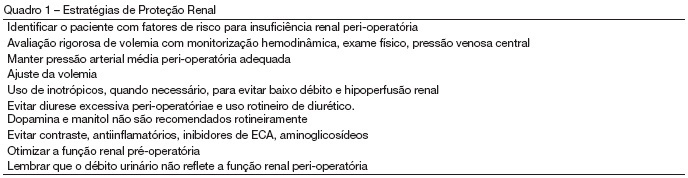
BACKGROUND AND OBJECTIVES: Perioperative renal dysfunction is an important cause of morbidity and mortality. With increase of life expectancy, older patients with more co-morbidity are being submitted to high risk surgical procedures, what make clinical practice related to organ protection possible modifier of short and long term survival. This review about renal protection in surgical intensive care unit points risk factors and discusses scientific evidence related to reduction of renal dysfunction in perioperative. CONTENTS: Although low extraction and adequate renal reserve of oxygen, the kidney is extremely sensible to hypoperfusion being renal acute insufficiency a frequent complication of hemodynamic instability. This apparent paradox, high oxygen content and reduced extraction with high incidence of renal damage to hypotension reflects the intra-renal gradient of oxygen, what makes renal medulla highly susceptible to ischemia. Factors associated with renal lesion are observed in all fases of perioperative period: fasting, contrast use, hypovolemia, hypotension, catecholamine and cytokine release, extracorporeal circulation, trauma, rabdomiolisys and aortic clamp. CONCLUSIONS: Management of renal damage is based in principals of perioperative renal physiology and glomerular hemodynamic. Clinical practice directed to organic protection should be implemented to minimize the impact this dysfunction.
Abstract
Rev Bras Ter Intensiva. 2006;18(3):282-291
DOI 10.1590/S0103-507X2006000300011
BACKGROUND AND OBJECTIVES: Perioperative renal dysfunction is an important cause of morbidity and mortality. With increase of life expectancy, older patients with more co-morbidity are being submitted to high risk surgical procedures, what make clinical practice related to organ protection possible modifier of short and long term survival. This review about renal protection in surgical intensive care unit points risk factors and discusses scientific evidence related to reduction of renal dysfunction in perioperative. CONTENTS: Although low extraction and adequate renal reserve of oxygen, the kidney is extremely sensible to hypoperfusion being renal acute insufficiency a frequent complication of hemodynamic instability. This apparent paradox, high oxygen content and reduced extraction with high incidence of renal damage to hypotension reflects the intra-renal gradient of oxygen, what makes renal medulla highly susceptible to ischemia. Factors associated with renal lesion are observed in all fases of perioperative period: fasting, contrast use, hypovolemia, hypotension, catecholamine and cytokine release, extracorporeal circulation, trauma, rabdomiolisys and aortic clamp. CONCLUSIONS: Management of renal damage is based in principals of perioperative renal physiology and glomerular hemodynamic. Clinical practice directed to organic protection should be implemented to minimize the impact this dysfunction.