Qualitative research Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2018;30(3):347-357
DOI 10.5935/0103-507X.20180053
To determine the optimal number of adult intensive care unit beds to reduce patient's queue waiting time and to propose policy strategies.
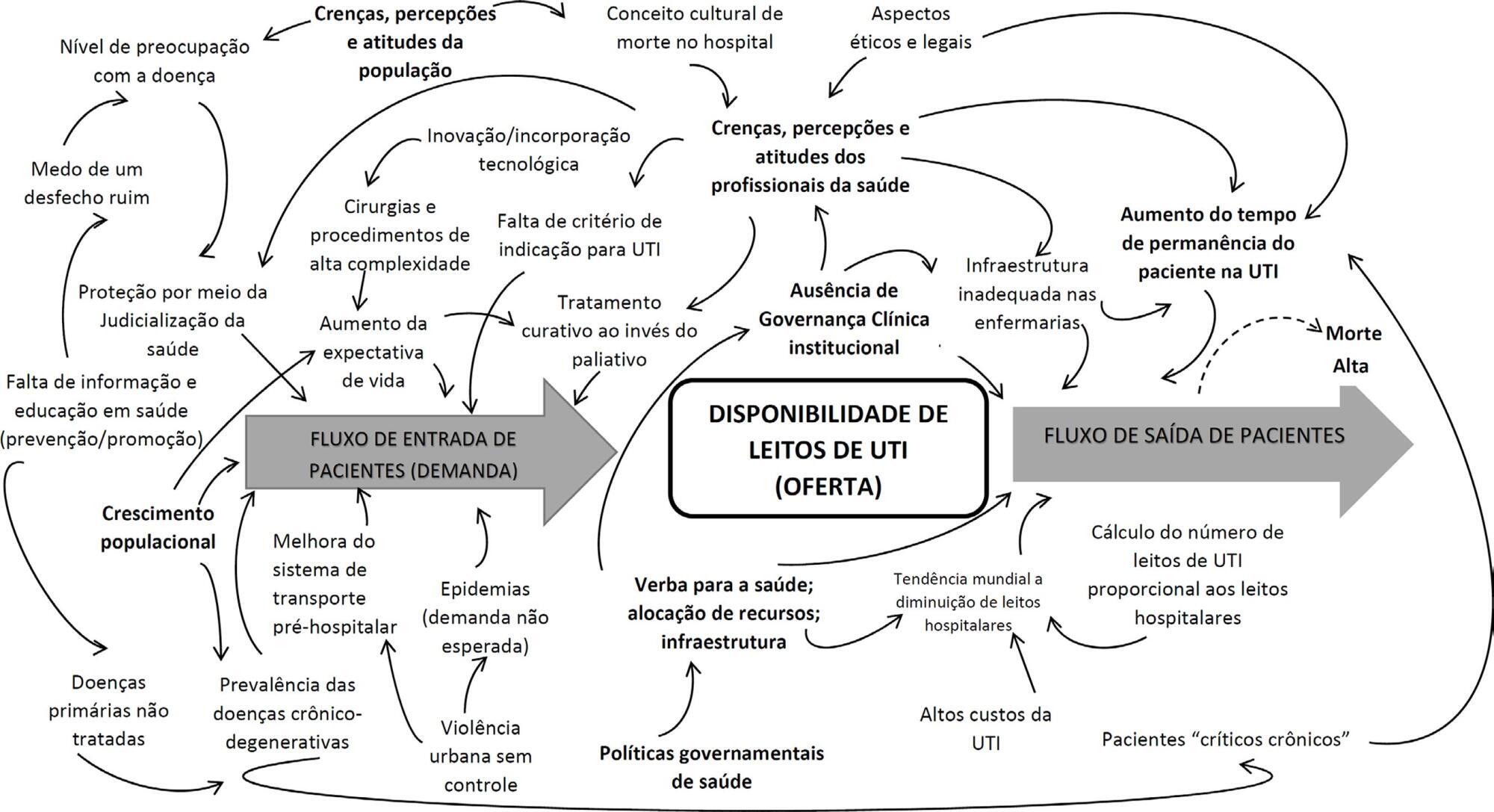
Multimethodological approach: (a) quantitative time series and queueing theory were used to predict the demand and estimate intensive care unit beds in different scenarios; (b) qualitative focus group and content analysis were used to explore physicians' attitudes and provide insights into their behaviors and belief-driven healthcare delivery changes.
A total of 33,101 requests for 268 regulated intensive care unit beds in one year resulted in 25% admissions, 55% queue abandonment and 20% deaths. Maintaining current intensive care unit arrival and exit rates, there would need 628 beds to ensure a maximum wait time of six hours. A reduction of the current abandonment rates due to clinical improvement or the average intensive care unit length of stay would decrease the number of beds to 471 and 366, respectively. If both were reduced, the number would reach 275 beds. The interviews generated 3 main themes: (1) the doctor's conflict: fair, legal, ethical and shared priorities in the decision-making process; (2) a failure of access: invisible queues and a lack of infrastructure; and (3) societal drama: deterioration of public policies and health care networks.
The queue should be treated as a complex societal problem with a multifactorial origin requiring integrated solutions. Improving intensive care unit protocols and reengineering the general wards may decrease the length of stay. It is essential to redefine and consolidate the regulatory centers to organize the queue and provide available resources in a timely manner, by using priority criteria, working with stakeholders to guarantee clinical governance and network organization.
Abstract
Rev Bras Ter Intensiva. 2018;30(3):347-357
DOI 10.5935/0103-507X.20180053
To determine the optimal number of adult intensive care unit beds to reduce patient's queue waiting time and to propose policy strategies.
Multimethodological approach: (a) quantitative time series and queueing theory were used to predict the demand and estimate intensive care unit beds in different scenarios; (b) qualitative focus group and content analysis were used to explore physicians' attitudes and provide insights into their behaviors and belief-driven healthcare delivery changes.
A total of 33,101 requests for 268 regulated intensive care unit beds in one year resulted in 25% admissions, 55% queue abandonment and 20% deaths. Maintaining current intensive care unit arrival and exit rates, there would need 628 beds to ensure a maximum wait time of six hours. A reduction of the current abandonment rates due to clinical improvement or the average intensive care unit length of stay would decrease the number of beds to 471 and 366, respectively. If both were reduced, the number would reach 275 beds. The interviews generated 3 main themes: (1) the doctor's conflict: fair, legal, ethical and shared priorities in the decision-making process; (2) a failure of access: invisible queues and a lack of infrastructure; and (3) societal drama: deterioration of public policies and health care networks.
The queue should be treated as a complex societal problem with a multifactorial origin requiring integrated solutions. Improving intensive care unit protocols and reengineering the general wards may decrease the length of stay. It is essential to redefine and consolidate the regulatory centers to organize the queue and provide available resources in a timely manner, by using priority criteria, working with stakeholders to guarantee clinical governance and network organization.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):370-375
DOI 10.1590/S0103-507X2008000400009
OBJECTIVE: The aim of this study was to understand the experience of family members, during a patient's stay in the intensive care unit of public and private hospitals using an approximation to the phenomenology referential. METHODS: We interviewed 27 relatives of adult patients, 10 from a public institution and 17 from a private one. RESULTS: From analyses of interviews in a public institution, four thematic categories emerged. In a private institution six categories were identified. Searching for differences and similarities, four similar thematic categories were perceived in both institutions and two categories were absent in the public hospital. CONCLUSION: There are no significant differences between categories in private and public hospitals. This indicates that family behavior and reactions to patient's admission to the ICU are not associated with social or financial aspects. However, a greater knowledge of government policies and programs is necessary, because they favor humanization by allowing family members to accompany the patient in tertiary services.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):370-375
DOI 10.1590/S0103-507X2008000400009
OBJECTIVE: The aim of this study was to understand the experience of family members, during a patient's stay in the intensive care unit of public and private hospitals using an approximation to the phenomenology referential. METHODS: We interviewed 27 relatives of adult patients, 10 from a public institution and 17 from a private one. RESULTS: From analyses of interviews in a public institution, four thematic categories emerged. In a private institution six categories were identified. Searching for differences and similarities, four similar thematic categories were perceived in both institutions and two categories were absent in the public hospital. CONCLUSION: There are no significant differences between categories in private and public hospitals. This indicates that family behavior and reactions to patient's admission to the ICU are not associated with social or financial aspects. However, a greater knowledge of government policies and programs is necessary, because they favor humanization by allowing family members to accompany the patient in tertiary services.