pulmonary compliance Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2008;20(3):213-219
DOI 10.1590/S0103-507X2008000300002
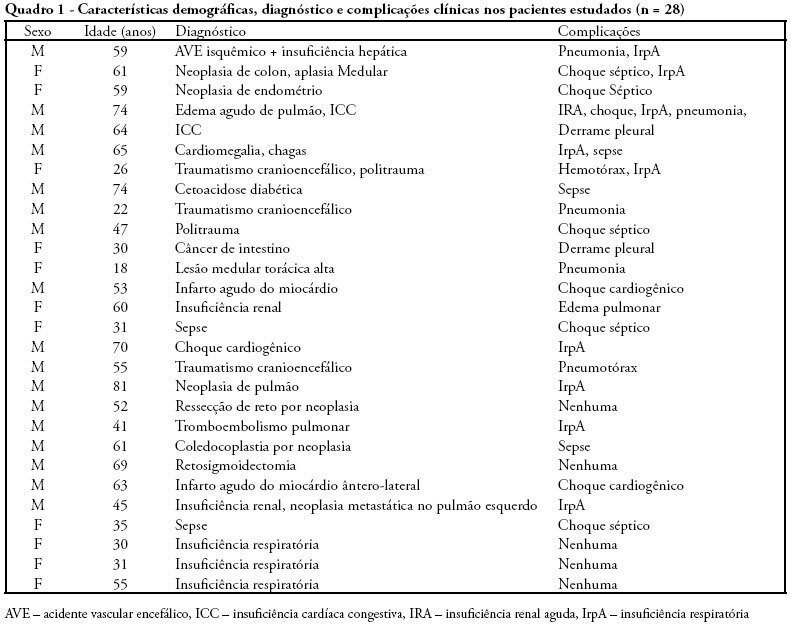
OBJECTIVES: This study is justified by the fact that in clinical practice, changes occur in patient's positioning in the bed during hospitalization in intensive care unity, it's necessary better understanding about possible adverse effects that such changes might cause mainly on the respiratory system condition. The objective this study was to evaluate if the patients positioning in bed can to alter the pulmonary complacency. METHODS: All included patients were submitted to mechanical ventilation and were sedated and curarized respiratory system compliance was assessed in three different positioning: lateral, dorsal and sitting. After an alveolar recruitment maneuver, patients were placed to a position throughout two hours, and in the last five minutes the data was collected from the mechanical ventilator display. RESULTS: twenty eight patients were prospectively assessed. Values of respiratory system compliance in the lateral position were 37,07 ± 12,9 in the dorsal were 39,2 ± 10,5 and in the sitting 43,4 ± 9,6 mL/cmH2O. There were a statistical difference when we compared to the sitting and dorsal with lateral positioning for respiratory system compliance (p = 0.0052) and tidal volume (p < 0.001). There was a negative correlation between mean values of positive end expiratory pressure a respiratory system compliance (r = 0.59, p = 0.002). The FIO2 administered was 0.6 for the lateral positioning and 0.5 for the dorsal and sitting positioning (p = 0.049). CONCLUSIONS: That body positioning in patients restrained to a bed and submitted to invasive mechanical ventilation leads to pulmonary compliance, tidal volume and SpO2 oscillations. In the sitting position the pulmonary compliance is higher than in others positions.
Abstract
Rev Bras Ter Intensiva. 2008;20(3):213-219
DOI 10.1590/S0103-507X2008000300002
OBJECTIVES: This study is justified by the fact that in clinical practice, changes occur in patient's positioning in the bed during hospitalization in intensive care unity, it's necessary better understanding about possible adverse effects that such changes might cause mainly on the respiratory system condition. The objective this study was to evaluate if the patients positioning in bed can to alter the pulmonary complacency. METHODS: All included patients were submitted to mechanical ventilation and were sedated and curarized respiratory system compliance was assessed in three different positioning: lateral, dorsal and sitting. After an alveolar recruitment maneuver, patients were placed to a position throughout two hours, and in the last five minutes the data was collected from the mechanical ventilator display. RESULTS: twenty eight patients were prospectively assessed. Values of respiratory system compliance in the lateral position were 37,07 ± 12,9 in the dorsal were 39,2 ± 10,5 and in the sitting 43,4 ± 9,6 mL/cmH2O. There were a statistical difference when we compared to the sitting and dorsal with lateral positioning for respiratory system compliance (p = 0.0052) and tidal volume (p < 0.001). There was a negative correlation between mean values of positive end expiratory pressure a respiratory system compliance (r = 0.59, p = 0.002). The FIO2 administered was 0.6 for the lateral positioning and 0.5 for the dorsal and sitting positioning (p = 0.049). CONCLUSIONS: That body positioning in patients restrained to a bed and submitted to invasive mechanical ventilation leads to pulmonary compliance, tidal volume and SpO2 oscillations. In the sitting position the pulmonary compliance is higher than in others positions.
Abstract
Rev Bras Ter Intensiva. 2007;19(2):161-169
DOI 10.1590/S0103-507X2007000200004
BACKGROUND AND OBJECTIVES: In mechanical ventilation, invasive and noninvasive, the knowledge of respiratory mechanic physiology is indispensable to take decisions and into the efficient management of modern ventilators. Monitoring of pulmonary mechanic parameters is been recommended from all the review works and clinical research. The objective of this study was review concepts of pulmonary mechanic and the methods used to obtain measures in the bed side, preparing a rational sequence to obtain this data. METHODS: It was obtained bibliographic review through data bank LILACS, MedLine and PubMed, from the last ten years. RESULTS: This review approaches parameters of resistance, pulmonary compliance and intrinsic PEEP as primordial into comprehension of acute respiratory failure and mechanic ventilatory support, mainly in acute respiratory distress syndrome (ARDS) and in chronic obstructive pulmonary disease (COPD). CONCLUSIONS: Monitoring pulmonary mechanics in patients under mechanical ventilation in intensive care units gives relevant informations and should be implemented in a rational and systematic way.
Abstract
Rev Bras Ter Intensiva. 2007;19(2):161-169
DOI 10.1590/S0103-507X2007000200004
BACKGROUND AND OBJECTIVES: In mechanical ventilation, invasive and noninvasive, the knowledge of respiratory mechanic physiology is indispensable to take decisions and into the efficient management of modern ventilators. Monitoring of pulmonary mechanic parameters is been recommended from all the review works and clinical research. The objective of this study was review concepts of pulmonary mechanic and the methods used to obtain measures in the bed side, preparing a rational sequence to obtain this data. METHODS: It was obtained bibliographic review through data bank LILACS, MedLine and PubMed, from the last ten years. RESULTS: This review approaches parameters of resistance, pulmonary compliance and intrinsic PEEP as primordial into comprehension of acute respiratory failure and mechanic ventilatory support, mainly in acute respiratory distress syndrome (ARDS) and in chronic obstructive pulmonary disease (COPD). CONCLUSIONS: Monitoring pulmonary mechanics in patients under mechanical ventilation in intensive care units gives relevant informations and should be implemented in a rational and systematic way.