
You searched for:"Claudia Maria Dantas de Maio Carrilho"
We found (7) results for your search.-
Original Article
IMPACTO-MR: a Brazilian nationwide platform study to assess infections and multidrug resistance in intensive care units
- Bruno M Tomazini
 ,
, - Antonio Paulo Nassar Jr ,
- Thiago Costa Lisboa ,
- Luciano César Pontes de Azevedo ,
- Viviane Cordeiro Veiga , [ … ],
- Alexandre Biasi Cavalcanti
Abstract
Original ArticleIMPACTO-MR: a Brazilian nationwide platform study to assess infections and multidrug resistance in intensive care units
Rev Bras Ter Intensiva. 2022;34(4):418-425
DOI 10.5935/0103-507X.20220209-en
- Bruno M Tomazini ,
- Antonio Paulo Nassar Jr ,
- Thiago Costa Lisboa ,
- Luciano César Pontes de Azevedo ,
- Viviane Cordeiro Veiga ,
- Daniela Ghidetti Mangas Catarino ,
- Debora Vacaro Fogazzi ,
- Beatriz Arns ,
- Filipe Teixeira Piastrelli ,
- Camila Dietrich ,
- Karina Leal Negrelli,
- Isabella de Andrade Jesuíno,
- Luiz Fernando Lima Reis,
- Renata Rodrigues de Mattos,
- Carla Cristina Gomes Pinheiro,
- Mariane Nascimento Luz,
- Clayse Carla da Silva Spadoni,
- Elisângela Emilene Moro,
- Flávia Regina Bueno,
- Camila Santana Justo Cintra Sampaio,
- Débora Patrício Silva,
- Franca Pellison Baldassare,
- Ana Cecilia Alcantara Silva,
- Thabata Veiga,
- Leticia Barbante,
- Marianne Lambauer,
- Viviane Bezerra Campos,
- Elton Santos,
- Renato Hideo Nakawaga Santos,
- Ligia Nasi Laranjeiras,
- Nanci Valeis,
- Eliana Santucci,
- Tamiris Abait Miranda,
- Ana Cristina Lagoeiro do Patrocínio,
- Andréa de Carvalho,
- Eduvirgens Maria Couto de Sousa,
- Ancelmo Honorato Ferraz de Sousa,
- Daniel Tavares Malheiro,
- Isabella Lott Bezerra,
- Mirian Batista Rodrigues,
- Julliana Chicuta Malicia,
- Sabrina Souza da Silva,
- Bruna dos Passos Gimenes,
- Guilhermo Prates Sesin,
- Alexandre Prehn Zavascki,
- Daniel Sganzerla,
- Gregory Saraiva Medeiros,
- Rosa da Rosa Minho dos Santos,
- Fernanda Kelly Romeiro Silva,
- Maysa Yukari Cheno,
- Carolinne Ferreira Abrahão,
- Haliton Alves de Oliveira Junior,
- Leonardo Lima Rocha,
- Pedro Aniceto Nunes Neto,
- Valéria Chagas Pereira,
- Luis Eduardo Miranda Paciência,
- Elaine Silva Bueno,
- Eliana Bernadete Caser,
- Larissa Zuqui Ribeiro,
- Caio Cesar Ferreira Fernandes,
- Juliana Mazzei Garcia,
- Vanildes de Fátima Fernandes Silva,
- Alisson Junior dos Santos,
- Flávia Ribeiro Machado,
- Maria Aparecida de Souza,
- Bianca Ramos Ferronato,
- Hugo Corrêa de Andrade Urbano,
- Danielle Conceição Aparecida Moreira,
- Vicente Cés de Souza-Dantas,
- Diego Meireles Duarte,
- Juliana Coelho,
- Rodrigo Cruvinel Figueiredo,
- Fernanda Foreque,
- Thiago Gomes Romano,
- Daniel Cubos,
- Vladimir Miguel Spirale,
- Roberta Schiavon Nogueira,
- Israel Silva Maia,
- Cassio Luis Zandonai,
- Wilson José Lovato,
- Rodrigo Barbosa Cerantola,
- Tatiana Gozzi Pancev Toledo,
- Pablo Oscar Tomba,
- Joyce Ramos de Almeida,
- Luciana Coelho Sanches,
- Leticia Pierini,
- Mariana Cunha,
- Michelle Tereza Sousa,
- Bruna Azevedo,
- Felipe Dal-Pizzol,
- Danusa de Castro Damasio,
- Marina Peres Bainy,
- Dagoberta Alves Vieira Beduhn,
- Joana D’Arc Vila Nova Jatobá,
- Maria Tereza Farias de Moura,
- Leila Rezegue de Moraes Rego,
- Adria Vanessa da Silva,
- Luana Pontes Oliveira,
- Eliene Sá Sodré Filho,
- Silvana Soares dos Santos,
- Itallo de Lima Neves,
- Vanessa Cristina de Aquino Leão,
- João Lucidio Lobato Paes,
- Marielle Cristina Mendes Silva,
- Cláudio Dornas de Oliveira,
- Raquel Caldeira Brant Santiago,
- Jorge Luiz da Rocha Paranhos,
- Iany Grinezia da Silva Wiermann,
- Durval Ferreira Fonseca Pedroso,
- Priscilla Yoshiko Sawada,
- Rejane Martins Prestes,
- Glícia Cardoso Nascimento,
- Cintia Magalhães Carvalho Grion,
- Claudia Maria Dantas de Maio Carrilho,
- Roberta Lacerda Almeida de Miranda Dantas,
- Eliane Pereira Silva,
- Antônio Carlos da Silva,
- Sheila Mara Bezerra de Oliveira,
- Nicole Alberti Golin,
- Rogerio Tregnago,
- Valéria Paes Lima,
- Kamilla Grasielle Nunes da Silva,
- Emerson Boschi,
- Viviane Buffon,
- André Sant’Ana Machado,
- Leticia Capeletti,
- Rafael Botelho Foernges,
- Andréia Schubert de Carvalho,
- Lúcio Couto de Oliveira Junior,
- Daniela Cunha de Oliveira,
- Everton Macêdo Silva,
- Julival Ribeiro,
- Francielle Constantino Pereira,
- Fernanda Borges Salgado,
- Caroline Deutschendorf,
- Cristofer Farias da Silva,
- Andre Luiz Nunes Gobatto,
- Carolaine Bomfim de Oliveira,
- Marianna Deway Andrade Dracoulakis,
- Natália Oliveira Santos Alvaia,
- Roberta Machado de Souza,
- Larissa Liz Cardoso de Araújo,
- Rodrigo Morel Vieira de Melo,
- Luiz Carlos Santana Passos,
- Claudia Fernanda de Lacerda Vidal,
- Fernanda Lopes de Albuquerque Rodrigues,
- Pedro Kurtz,
- Cássia Righy Shinotsuka,
- Maria Brandão Tavares,
- Igor das Virgens Santana,
- Luciana Macedo da Silva Gavinho,
- Alaís Brito Nascimento,
- Adriano J Pereira,
- Alexandre Biasi Cavalcanti
Views2ABSTRACT
Objective:
To describe the IMPACTO-MR, a Brazilian nationwide intensive care unit platform study focused on the impact of health care-associated infections due to multidrug-resistant bacteria.
Methods:
We described the IMPACTO-MR platform, its development, criteria for intensive care unit selection, characterization of core data collection, objectives, and future research projects to be held within the platform.
Results:
The core data were collected using the Epimed Monitor System® and consisted of demographic data, comorbidity data, functional status, clinical scores, admission diagnosis and secondary diagnoses, laboratory, clinical, and microbiological data, and organ support during intensive care unit stay, among others. From October 2019 to December 2020, 33,983 patients from 51 intensive care units were included in the core database.
Conclusion:
The IMPACTO-MR platform is a nationwide Brazilian intensive care unit clinical database focused on researching the impact of health care-associated infections due to multidrug-resistant bacteria. This platform provides data for individual intensive care unit development and research and multicenter observational and prospective trials.
Keywords:bacterialBacterial infectionsDatabaseDatabase management systemsDrug-resistanceIMPACTO-MRIntensive care unitsSoftwareSee moreViews2

Abstract
Original ArticleIMPACTO-MR: a Brazilian nationwide platform study to assess infections and multidrug resistance in intensive care units
Rev Bras Ter Intensiva. 2022;34(4):418-425
DOI 10.5935/0103-507X.20220209-en
- Bruno M Tomazini ,
- Antonio Paulo Nassar Jr ,
- Thiago Costa Lisboa ,
- Luciano César Pontes de Azevedo ,
- Viviane Cordeiro Veiga ,
- Daniela Ghidetti Mangas Catarino ,
- Debora Vacaro Fogazzi ,
- Beatriz Arns ,
- Filipe Teixeira Piastrelli ,
- Camila Dietrich ,
- Karina Leal Negrelli,
- Isabella de Andrade Jesuíno,
- Luiz Fernando Lima Reis,
- Renata Rodrigues de Mattos,
- Carla Cristina Gomes Pinheiro,
- Mariane Nascimento Luz,
- Clayse Carla da Silva Spadoni,
- Elisângela Emilene Moro,
- Flávia Regina Bueno,
- Camila Santana Justo Cintra Sampaio,
- Débora Patrício Silva,
- Franca Pellison Baldassare,
- Ana Cecilia Alcantara Silva,
- Thabata Veiga,
- Leticia Barbante,
- Marianne Lambauer,
- Viviane Bezerra Campos,
- Elton Santos,
- Renato Hideo Nakawaga Santos,
- Ligia Nasi Laranjeiras,
- Nanci Valeis,
- Eliana Santucci,
- Tamiris Abait Miranda,
- Ana Cristina Lagoeiro do Patrocínio,
- Andréa de Carvalho,
- Eduvirgens Maria Couto de Sousa,
- Ancelmo Honorato Ferraz de Sousa,
- Daniel Tavares Malheiro,
- Isabella Lott Bezerra,
- Mirian Batista Rodrigues,
- Julliana Chicuta Malicia,
- Sabrina Souza da Silva,
- Bruna dos Passos Gimenes,
- Guilhermo Prates Sesin,
- Alexandre Prehn Zavascki,
- Daniel Sganzerla,
- Gregory Saraiva Medeiros,
- Rosa da Rosa Minho dos Santos,
- Fernanda Kelly Romeiro Silva,
- Maysa Yukari Cheno,
- Carolinne Ferreira Abrahão,
- Haliton Alves de Oliveira Junior,
- Leonardo Lima Rocha,
- Pedro Aniceto Nunes Neto,
- Valéria Chagas Pereira,
- Luis Eduardo Miranda Paciência,
- Elaine Silva Bueno,
- Eliana Bernadete Caser,
- Larissa Zuqui Ribeiro,
- Caio Cesar Ferreira Fernandes,
- Juliana Mazzei Garcia,
- Vanildes de Fátima Fernandes Silva,
- Alisson Junior dos Santos,
- Flávia Ribeiro Machado,
- Maria Aparecida de Souza,
- Bianca Ramos Ferronato,
- Hugo Corrêa de Andrade Urbano,
- Danielle Conceição Aparecida Moreira,
- Vicente Cés de Souza-Dantas,
- Diego Meireles Duarte,
- Juliana Coelho,
- Rodrigo Cruvinel Figueiredo,
- Fernanda Foreque,
- Thiago Gomes Romano,
- Daniel Cubos,
- Vladimir Miguel Spirale,
- Roberta Schiavon Nogueira,
- Israel Silva Maia,
- Cassio Luis Zandonai,
- Wilson José Lovato,
- Rodrigo Barbosa Cerantola,
- Tatiana Gozzi Pancev Toledo,
- Pablo Oscar Tomba,
- Joyce Ramos de Almeida,
- Luciana Coelho Sanches,
- Leticia Pierini,
- Mariana Cunha,
- Michelle Tereza Sousa,
- Bruna Azevedo,
- Felipe Dal-Pizzol,
- Danusa de Castro Damasio,
- Marina Peres Bainy,
- Dagoberta Alves Vieira Beduhn,
- Joana D’Arc Vila Nova Jatobá,
- Maria Tereza Farias de Moura,
- Leila Rezegue de Moraes Rego,
- Adria Vanessa da Silva,
- Luana Pontes Oliveira,
- Eliene Sá Sodré Filho,
- Silvana Soares dos Santos,
- Itallo de Lima Neves,
- Vanessa Cristina de Aquino Leão,
- João Lucidio Lobato Paes,
- Marielle Cristina Mendes Silva,
- Cláudio Dornas de Oliveira,
- Raquel Caldeira Brant Santiago,
- Jorge Luiz da Rocha Paranhos,
- Iany Grinezia da Silva Wiermann,
- Durval Ferreira Fonseca Pedroso,
- Priscilla Yoshiko Sawada,
- Rejane Martins Prestes,
- Glícia Cardoso Nascimento,
- Cintia Magalhães Carvalho Grion,
- Claudia Maria Dantas de Maio Carrilho,
- Roberta Lacerda Almeida de Miranda Dantas,
- Eliane Pereira Silva,
- Antônio Carlos da Silva,
- Sheila Mara Bezerra de Oliveira,
- Nicole Alberti Golin,
- Rogerio Tregnago,
- Valéria Paes Lima,
- Kamilla Grasielle Nunes da Silva,
- Emerson Boschi,
- Viviane Buffon,
- André Sant’Ana Machado,
- Leticia Capeletti,
- Rafael Botelho Foernges,
- Andréia Schubert de Carvalho,
- Lúcio Couto de Oliveira Junior,
- Daniela Cunha de Oliveira,
- Everton Macêdo Silva,
- Julival Ribeiro,
- Francielle Constantino Pereira,
- Fernanda Borges Salgado,
- Caroline Deutschendorf,
- Cristofer Farias da Silva,
- Andre Luiz Nunes Gobatto,
- Carolaine Bomfim de Oliveira,
- Marianna Deway Andrade Dracoulakis,
- Natália Oliveira Santos Alvaia,
- Roberta Machado de Souza,
- Larissa Liz Cardoso de Araújo,
- Rodrigo Morel Vieira de Melo,
- Luiz Carlos Santana Passos,
- Claudia Fernanda de Lacerda Vidal,
- Fernanda Lopes de Albuquerque Rodrigues,
- Pedro Kurtz,
- Cássia Righy Shinotsuka,
- Maria Brandão Tavares,
- Igor das Virgens Santana,
- Luciana Macedo da Silva Gavinho,
- Alaís Brito Nascimento,
- Adriano J Pereira,
- Alexandre Biasi Cavalcanti
Views2ABSTRACT
Objective:
To describe the IMPACTO-MR, a Brazilian nationwide intensive care unit platform study focused on the impact of health care-associated infections due to multidrug-resistant bacteria.
Methods:
We described the IMPACTO-MR platform, its development, criteria for intensive care unit selection, characterization of core data collection, objectives, and future research projects to be held within the platform.
Results:
The core data were collected using the Epimed Monitor System® and consisted of demographic data, comorbidity data, functional status, clinical scores, admission diagnosis and secondary diagnoses, laboratory, clinical, and microbiological data, and organ support during intensive care unit stay, among others. From October 2019 to December 2020, 33,983 patients from 51 intensive care units were included in the core database.
Conclusion:
The IMPACTO-MR platform is a nationwide Brazilian intensive care unit clinical database focused on researching the impact of health care-associated infections due to multidrug-resistant bacteria. This platform provides data for individual intensive care unit development and research and multicenter observational and prospective trials.
Keywords:bacterialBacterial infectionsDatabaseDatabase management systemsDrug-resistanceIMPACTO-MRIntensive care unitsSoftwareSee more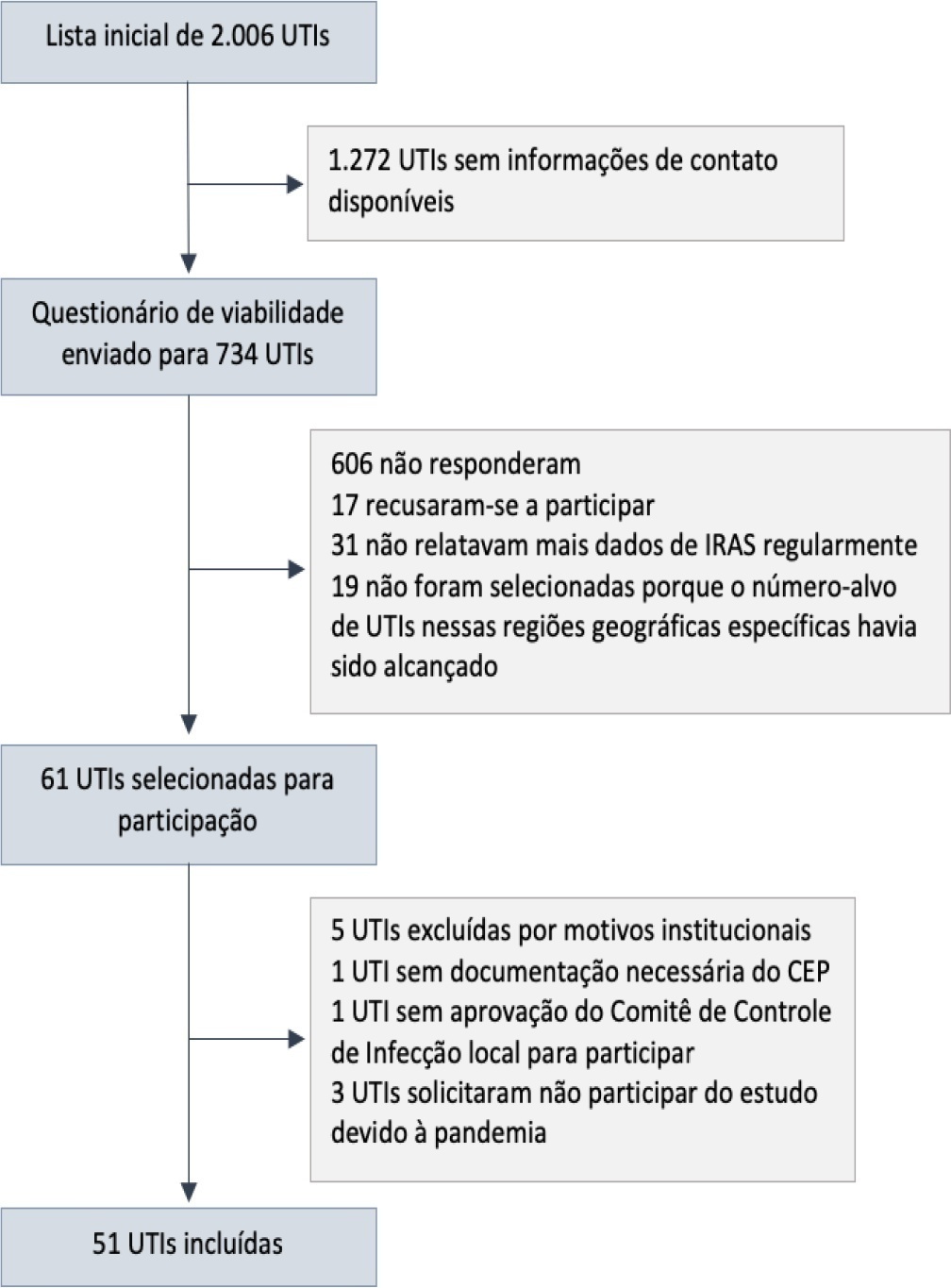
- Bruno M Tomazini
-
Original Article
Acute kidney injury and intra-abdominal hypertension in burn patients in intensive care
Rev Bras Ter Intensiva. 2018;30(1):15-20
Abstract
Original ArticleAcute kidney injury and intra-abdominal hypertension in burn patients in intensive care
Rev Bras Ter Intensiva. 2018;30(1):15-20
DOI 10.5935/0103-507X.20180001
Views0ABSTRACT
Objective:
To evaluate the frequency of intra-abdominal hypertension in major burn patients and its association with the occurrence of acute kidney injury.
Methods:
This was a prospective cohort study of a population of burn patients hospitalized in a specialized intensive care unit. A convenience sample was taken of adult patients hospitalized in the period from 1 August 2015 to 31 October 2016. Clinical and burn data were collected, and serial intra-abdominal pressure measurements taken. The significance level used was 5%.
Results:
A total of 46 patients were analyzed. Of these, 38 patients developed intra-abdominal hypertension (82.6%). The median increase in intra-abdominal pressure was 15.0mmHg (interquartile range: 12.0 to 19.0). Thirty-two patients (69.9%) developed acute kidney injury. The median time to development of acute kidney injury was 3 days (interquartile range: 1 – 7). The individual analysis of risk factors for acute kidney injury indicated an association with intra-abdominal hypertension (p = 0.041), use of glycopeptides (p = 0.001), use of vasopressors (p = 0.001) and use of mechanical ventilation (p = 0.006). Acute kidney injury was demonstrated to have an association with increased 30-day mortality (log-rank, p = 0.009).
Conclusion:
Intra-abdominal hypertension occurred in most patients, predominantly in grades I and II. The identified risk factors for the occurrence of acute kidney injury were intra-abdominal hypertension and use of glycopeptides, vasopressors and mechanical ventilation. Acute kidney injury was associated with increased 30-day mortality.
Keywords:Burn unitsburnsIntensive care unitsIntra-abdominal hypertensionMultiple organ failureRenal insufficiencySee moreViews0Abstract
Original ArticleAcute kidney injury and intra-abdominal hypertension in burn patients in intensive care
Rev Bras Ter Intensiva. 2018;30(1):15-20
DOI 10.5935/0103-507X.20180001
Views0ABSTRACT
Objective:
To evaluate the frequency of intra-abdominal hypertension in major burn patients and its association with the occurrence of acute kidney injury.
Methods:
This was a prospective cohort study of a population of burn patients hospitalized in a specialized intensive care unit. A convenience sample was taken of adult patients hospitalized in the period from 1 August 2015 to 31 October 2016. Clinical and burn data were collected, and serial intra-abdominal pressure measurements taken. The significance level used was 5%.
Results:
A total of 46 patients were analyzed. Of these, 38 patients developed intra-abdominal hypertension (82.6%). The median increase in intra-abdominal pressure was 15.0mmHg (interquartile range: 12.0 to 19.0). Thirty-two patients (69.9%) developed acute kidney injury. The median time to development of acute kidney injury was 3 days (interquartile range: 1 – 7). The individual analysis of risk factors for acute kidney injury indicated an association with intra-abdominal hypertension (p = 0.041), use of glycopeptides (p = 0.001), use of vasopressors (p = 0.001) and use of mechanical ventilation (p = 0.006). Acute kidney injury was demonstrated to have an association with increased 30-day mortality (log-rank, p = 0.009).
Conclusion:
Intra-abdominal hypertension occurred in most patients, predominantly in grades I and II. The identified risk factors for the occurrence of acute kidney injury were intra-abdominal hypertension and use of glycopeptides, vasopressors and mechanical ventilation. Acute kidney injury was associated with increased 30-day mortality.
Keywords:Burn unitsburnsIntensive care unitsIntra-abdominal hypertensionMultiple organ failureRenal insufficiencySee more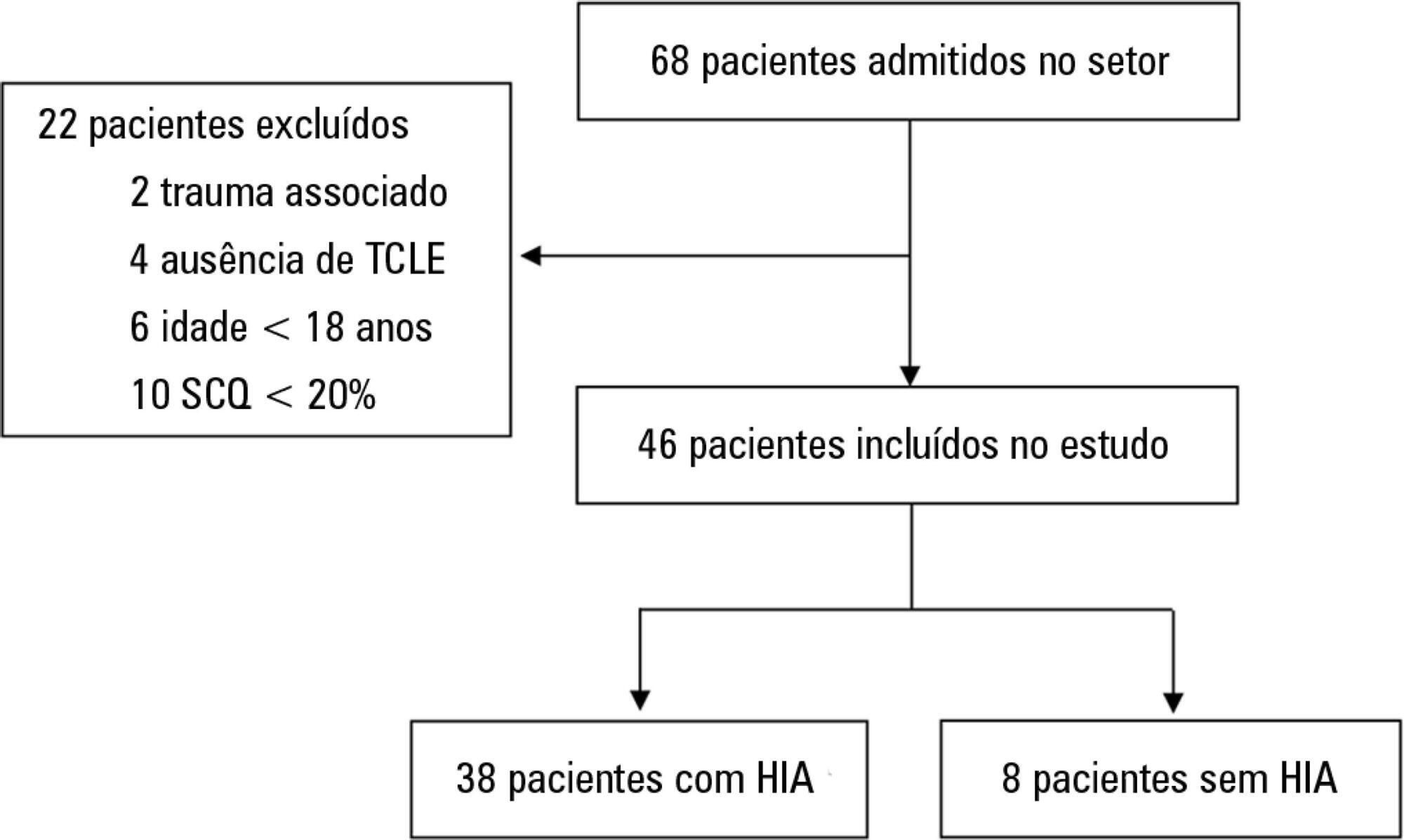
-
Original Articles
Evaluation of the five-year operation period of a rapid response team led by an intensive care physician at a university hospital
Rev Bras Ter Intensiva. 2016;28(3):278-284
Abstract
Original ArticlesEvaluation of the five-year operation period of a rapid response team led by an intensive care physician at a university hospital
Rev Bras Ter Intensiva. 2016;28(3):278-284
DOI 10.5935/0103-507X.20160045
Views1ABSTRACT
Objective:
To evaluate the implementation of a multidisciplinary rapid response team led by an intensive care physician at a university hospital.
Methods:
This retrospective cohort study analyzed assessment forms that were completed during the assessments made by the rapid response team of a university hospital between March 2009 and February 2014.
Results:
Data were collected from 1,628 assessments performed by the rapid response team for 1,024 patients and included 1,423 code yellow events and 205 code blue events. The number of assessments was higher in the first year of operation of the rapid response team. The multivariate analysis indicated that age (OR 1.02; 95%CI 1.02 – 1.03; p < 0.001), being male (OR 1.48; 95%CI 1.09 - 2.01; p = 0.01), having more than one assessment (OR 3.31; 95%CI, 2.32 - 4.71; p < 0.001), hospitalization for clinical care (OR 1.77; 95%CI 1.29 - 2.42; p < 0.001), the request of admission to the intensive care unit after the code event (OR 4.75; 95%CI 3.43 - 6.59; p < 0.001), and admission to the intensive care unit before the code event (OR 2.13; 95%CI 1.41 - 3.21; p = 0.001) were risk factors for hospital mortality in patients who were seen for code yellow events.
Conclusion:
The hospital mortality rates were higher than those found in previous studies. The number of assessments was higher in the first year of operation of the rapid response team. Moreover, hospital mortality was higher among patients admitted for clinical care.
Keywords:Hospital mortalityHospital rapid response teamHospital, universitiesIntensive care unitsPatient safetySee moreViews1Abstract
Original ArticlesEvaluation of the five-year operation period of a rapid response team led by an intensive care physician at a university hospital
Rev Bras Ter Intensiva. 2016;28(3):278-284
DOI 10.5935/0103-507X.20160045
Views1ABSTRACT
Objective:
To evaluate the implementation of a multidisciplinary rapid response team led by an intensive care physician at a university hospital.
Methods:
This retrospective cohort study analyzed assessment forms that were completed during the assessments made by the rapid response team of a university hospital between March 2009 and February 2014.
Results:
Data were collected from 1,628 assessments performed by the rapid response team for 1,024 patients and included 1,423 code yellow events and 205 code blue events. The number of assessments was higher in the first year of operation of the rapid response team. The multivariate analysis indicated that age (OR 1.02; 95%CI 1.02 – 1.03; p < 0.001), being male (OR 1.48; 95%CI 1.09 - 2.01; p = 0.01), having more than one assessment (OR 3.31; 95%CI, 2.32 - 4.71; p < 0.001), hospitalization for clinical care (OR 1.77; 95%CI 1.29 - 2.42; p < 0.001), the request of admission to the intensive care unit after the code event (OR 4.75; 95%CI 3.43 - 6.59; p < 0.001), and admission to the intensive care unit before the code event (OR 2.13; 95%CI 1.41 - 3.21; p = 0.001) were risk factors for hospital mortality in patients who were seen for code yellow events.
Conclusion:
The hospital mortality rates were higher than those found in previous studies. The number of assessments was higher in the first year of operation of the rapid response team. Moreover, hospital mortality was higher among patients admitted for clinical care.
Keywords:Hospital mortalityHospital rapid response teamHospital, universitiesIntensive care unitsPatient safetySee more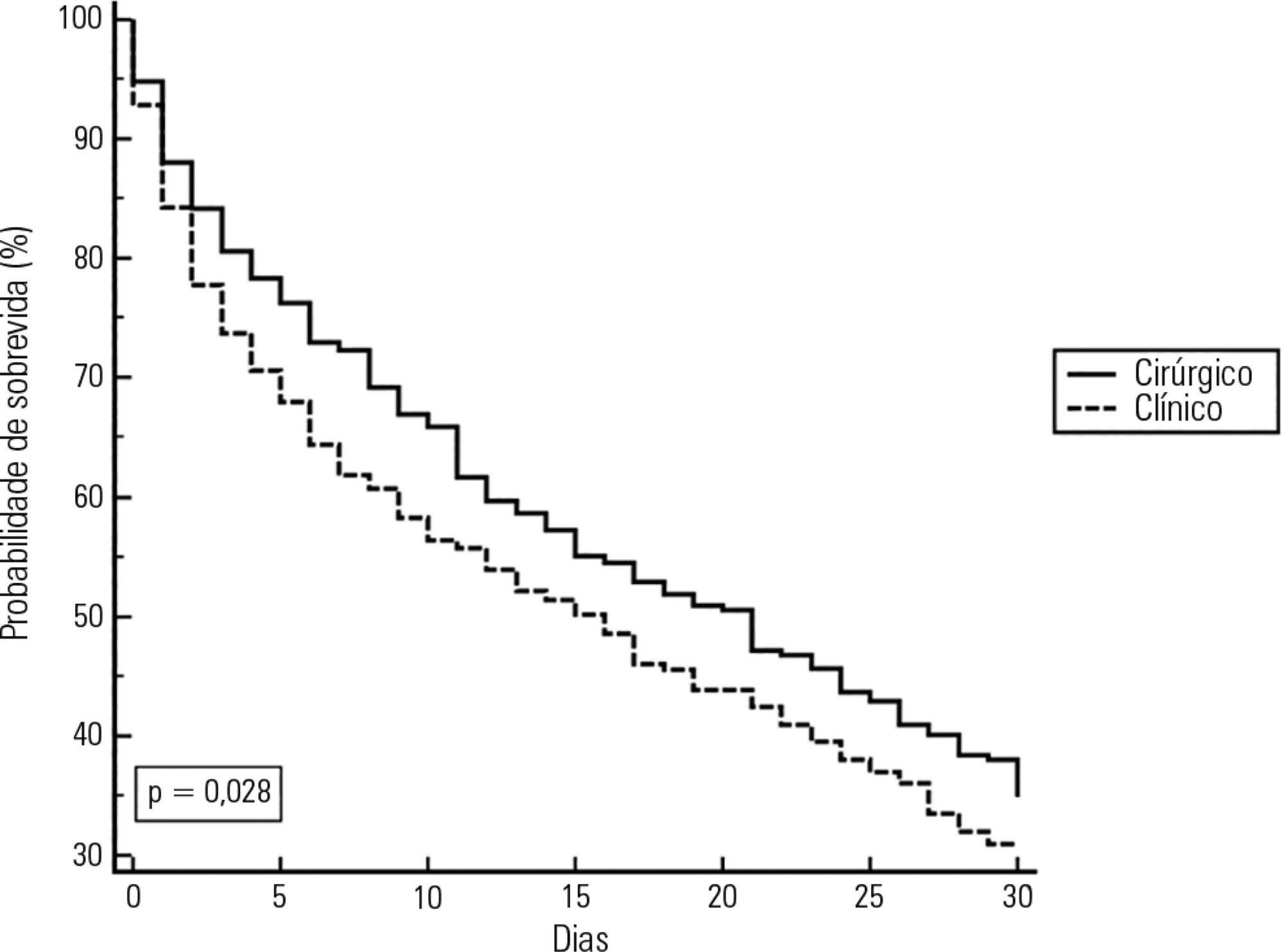
-
Original Articles
Currently used dosage regimens of vancomycin fail to achieve therapeutic levels in approximately 40% of intensive care unit patients
Rev Bras Ter Intensiva. 2016;28(4):380-386
Abstract
Original ArticlesCurrently used dosage regimens of vancomycin fail to achieve therapeutic levels in approximately 40% of intensive care unit patients
Rev Bras Ter Intensiva. 2016;28(4):380-386
DOI 10.5935/0103-507X.20160071
Views2See moreABSTRACT
Objective:
This study aimed to assess whether currently used dosages of vancomycin for treatment of serious gram-positive bacterial infections in intensive care unit patients provided initial therapeutic vancomycin trough levels and to examine possible factors associated with the presence of adequate initial vancomycin trough levels in these patients.
Methods:
A prospective descriptive study with convenience sampling was performed. Nursing note and medical record data were collected from September 2013 to July 2014 for patients who met inclusion criteria. Eighty-three patients were included. Initial vancomycin trough levels were obtained immediately before vancomycin fourth dose. Acute kidney injury was defined as an increase of at least 0.3mg/dL in serum creatinine within 48 hours.
Results:
Considering vancomycin trough levels recommended for serious gram-positive infection treatment (15 – 20µg/mL), patients were categorized as presenting with low, adequate, and high vancomycin trough levels (35 [42.2%], 18 [21.7%], and 30 [36.1%] patients, respectively). Acute kidney injury patients had significantly greater vancomycin trough levels (p = 0.0055, with significance for a trend, p = 0.0023).
Conclusion:
Surprisingly, more than 40% of the patients did not reach an effective initial vancomycin trough level. Studies on pharmacokinetic and dosage regimens of vancomycin in intensive care unit patients are necessary to circumvent this high proportion of failures to obtain adequate initial vancomycin trough levels. Vancomycin use without trough serum level monitoring in critically ill patients should be discouraged.
Views2Abstract
Original ArticlesCurrently used dosage regimens of vancomycin fail to achieve therapeutic levels in approximately 40% of intensive care unit patients
Rev Bras Ter Intensiva. 2016;28(4):380-386
DOI 10.5935/0103-507X.20160071
Views2See moreABSTRACT
Objective:
This study aimed to assess whether currently used dosages of vancomycin for treatment of serious gram-positive bacterial infections in intensive care unit patients provided initial therapeutic vancomycin trough levels and to examine possible factors associated with the presence of adequate initial vancomycin trough levels in these patients.
Methods:
A prospective descriptive study with convenience sampling was performed. Nursing note and medical record data were collected from September 2013 to July 2014 for patients who met inclusion criteria. Eighty-three patients were included. Initial vancomycin trough levels were obtained immediately before vancomycin fourth dose. Acute kidney injury was defined as an increase of at least 0.3mg/dL in serum creatinine within 48 hours.
Results:
Considering vancomycin trough levels recommended for serious gram-positive infection treatment (15 – 20µg/mL), patients were categorized as presenting with low, adequate, and high vancomycin trough levels (35 [42.2%], 18 [21.7%], and 30 [36.1%] patients, respectively). Acute kidney injury patients had significantly greater vancomycin trough levels (p = 0.0055, with significance for a trend, p = 0.0023).
Conclusion:
Surprisingly, more than 40% of the patients did not reach an effective initial vancomycin trough level. Studies on pharmacokinetic and dosage regimens of vancomycin in intensive care unit patients are necessary to circumvent this high proportion of failures to obtain adequate initial vancomycin trough levels. Vancomycin use without trough serum level monitoring in critically ill patients should be discouraged.
-
Original Articles
Parenteral colistin for the treatment of severe infections: a single center experience
Rev Bras Ter Intensiva. 2013;25(4):297-305
Abstract
Original ArticlesParenteral colistin for the treatment of severe infections: a single center experience
Rev Bras Ter Intensiva. 2013;25(4):297-305
DOI 10.5935/0103-507X.20130051
Views2Objective:
To describe a single center experience involving the administration of colistin to treat nosocomial infections caused by multidrug-resistant Gram-negative bacteria and identify factors associated with acute kidney injury and mortality.
Methods:
This retrospective longitudinal study evaluates critically ill patients with infections caused by multidrug-resistant Gram-negative bacteria. All adult patients who required treatment with intravenous colistin (colistimethate sodium) from January to December 2008 were considered eligible for the study. Data include demographics, diagnosis, duration of treatment, presence of acute kidney injury and 30-day mortality.
Results:
Colistin was used to treat an infection in 109 (13.8%) of the 789 patients admitted to the intensive care unit. The 30-day mortality observed in these patients was 71.6%. Twenty-nine patients (26.6%) presented kidney injury prior to colistin treatment, and six of these patients were able to recover kidney function even during colistin treatment. Twenty-one patients (19.2%) developed acute kidney injury while taking colistin, and 11 of these patients required dialysis. The variable independently associated with the presence of acute kidney injury was the Sequential Organ Failure Assessment at the beginning of colistin treatment (OR 1.46; 95%CI 1.20-1.79; p<0.001). The factors age (OR 1.03; 95%CI 1.00-1.05; p=0.02) and vasopressor use (OR 12.48; 95%CI 4.49-34.70; p<0.001) were associated with death in the logistic-regression model.
Conclusions:
Organ dysfunction at the beginning of colistin treatment was associated with acute kidney injury. In a small group of patients, we were able to observe an improvement of kidney function during colistin treatment. Age and vasopressor use were associated with death.
Keywords:Acinetobacter baumanniiAcute kidney injuryColistin/therapeutic useCross infection/drug therapyDeathIntensive carePseudomonas aeruginosaSee moreViews2Abstract
Original ArticlesParenteral colistin for the treatment of severe infections: a single center experience
Rev Bras Ter Intensiva. 2013;25(4):297-305
DOI 10.5935/0103-507X.20130051
Views2Objective:
To describe a single center experience involving the administration of colistin to treat nosocomial infections caused by multidrug-resistant Gram-negative bacteria and identify factors associated with acute kidney injury and mortality.
Methods:
This retrospective longitudinal study evaluates critically ill patients with infections caused by multidrug-resistant Gram-negative bacteria. All adult patients who required treatment with intravenous colistin (colistimethate sodium) from January to December 2008 were considered eligible for the study. Data include demographics, diagnosis, duration of treatment, presence of acute kidney injury and 30-day mortality.
Results:
Colistin was used to treat an infection in 109 (13.8%) of the 789 patients admitted to the intensive care unit. The 30-day mortality observed in these patients was 71.6%. Twenty-nine patients (26.6%) presented kidney injury prior to colistin treatment, and six of these patients were able to recover kidney function even during colistin treatment. Twenty-one patients (19.2%) developed acute kidney injury while taking colistin, and 11 of these patients required dialysis. The variable independently associated with the presence of acute kidney injury was the Sequential Organ Failure Assessment at the beginning of colistin treatment (OR 1.46; 95%CI 1.20-1.79; p<0.001). The factors age (OR 1.03; 95%CI 1.00-1.05; p=0.02) and vasopressor use (OR 12.48; 95%CI 4.49-34.70; p<0.001) were associated with death in the logistic-regression model.
Conclusions:
Organ dysfunction at the beginning of colistin treatment was associated with acute kidney injury. In a small group of patients, we were able to observe an improvement of kidney function during colistin treatment. Age and vasopressor use were associated with death.
Keywords:Acinetobacter baumanniiAcute kidney injuryColistin/therapeutic useCross infection/drug therapyDeathIntensive carePseudomonas aeruginosaSee more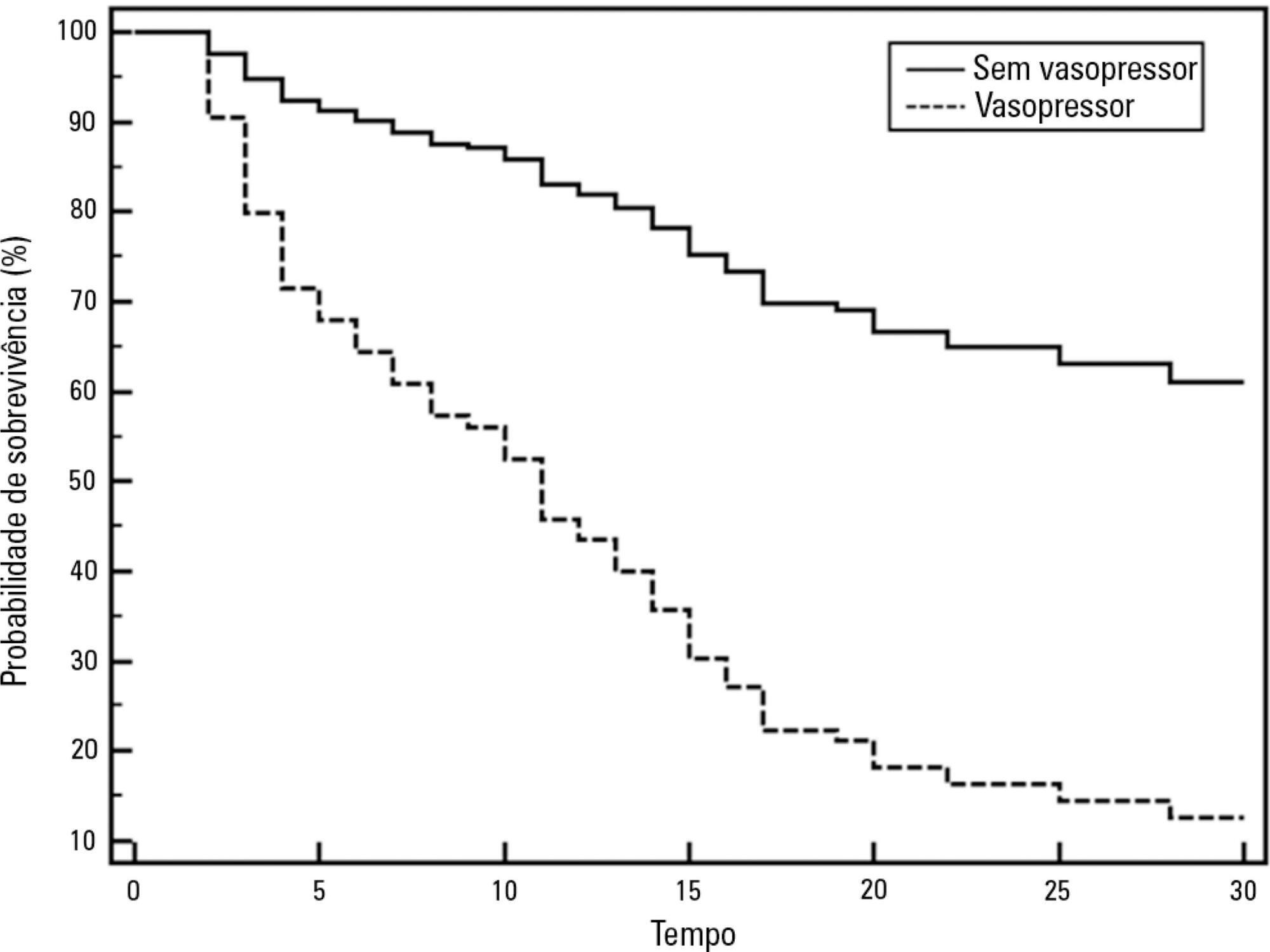
-
Artigo Original
Ventilator-associated pneumonia in surgical Intensive Care Unit
Rev Bras Ter Intensiva. 2006;18(1):38-44
Abstract
Artigo OriginalVentilator-associated pneumonia in surgical Intensive Care Unit
Rev Bras Ter Intensiva. 2006;18(1):38-44
DOI 10.1590/S0103-507X2006000100008
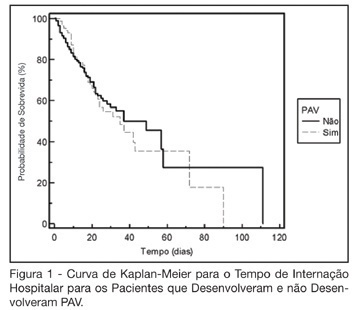
Views0See moreBACKGROUND AND OBJECTIVES: The ventilator-associated pneumonia (VAP) is a severe infection that presents multiple causes which can vary depending on the type of intensive care unit, type of patients, emphasizing the needs for vigilance measures with local data. The aim of this study is to describe the incidence, risk factors and mortality of VAP in patients in a surgical ICU. METHODS: Prospective cohort conducted from January 2004 to January 2005. It was included all the patients in mechanical ventilation, followed daily to collect data about demographics, diagnostic, APACHE II and TISS 28 scores, duration of mechanical ventilation, length of stay, incidence of VAP and mortality. RESULTS: 462 patients were studied; age 57.2 ± 16.6 years, 55% men. The mean APACHE II score was 18.3 and the incidence of VAP was 18.8%. The TISS score at admission OR = 1.050 (IC 95%: 1.003-1.050) and the enteral nutrition OR = 5.609 (IC 3.351-9.388) were factors associated with VAP and the prophylactic use of antibiotics was a factor of protection OR = 0.399 (IC95%: 0.177-0.902). The patients with VAP had longer length of stay in ICU (10.3 ± 10.7 vs 4.9 ± 3.3 days), higher median of duration of mechanical ventilation (4 vs 1 days), higher mean of TISS 28 (24.4 ± 4.6 vs 22.8 ± 4.5), and higher crude mortality (46 vs 28.8%) when compared with the patients without VAP. CONCLUSIONS: VAP was a frequent infection in surgical patients in mechanical ventilation. Enteral nutrition and admission TISS were risk factors and the previous use of antibiotics was protection factor to develop VAP. In our sample the results demonstrate that VAP is associated with higher duration in mechanical ventilation, longer length of stay and higher mortality.
Views0Abstract
Artigo OriginalVentilator-associated pneumonia in surgical Intensive Care Unit
Rev Bras Ter Intensiva. 2006;18(1):38-44
DOI 10.1590/S0103-507X2006000100008
Views0See moreBACKGROUND AND OBJECTIVES: The ventilator-associated pneumonia (VAP) is a severe infection that presents multiple causes which can vary depending on the type of intensive care unit, type of patients, emphasizing the needs for vigilance measures with local data. The aim of this study is to describe the incidence, risk factors and mortality of VAP in patients in a surgical ICU. METHODS: Prospective cohort conducted from January 2004 to January 2005. It was included all the patients in mechanical ventilation, followed daily to collect data about demographics, diagnostic, APACHE II and TISS 28 scores, duration of mechanical ventilation, length of stay, incidence of VAP and mortality. RESULTS: 462 patients were studied; age 57.2 ± 16.6 years, 55% men. The mean APACHE II score was 18.3 and the incidence of VAP was 18.8%. The TISS score at admission OR = 1.050 (IC 95%: 1.003-1.050) and the enteral nutrition OR = 5.609 (IC 3.351-9.388) were factors associated with VAP and the prophylactic use of antibiotics was a factor of protection OR = 0.399 (IC95%: 0.177-0.902). The patients with VAP had longer length of stay in ICU (10.3 ± 10.7 vs 4.9 ± 3.3 days), higher median of duration of mechanical ventilation (4 vs 1 days), higher mean of TISS 28 (24.4 ± 4.6 vs 22.8 ± 4.5), and higher crude mortality (46 vs 28.8%) when compared with the patients without VAP. CONCLUSIONS: VAP was a frequent infection in surgical patients in mechanical ventilation. Enteral nutrition and admission TISS were risk factors and the previous use of antibiotics was protection factor to develop VAP. In our sample the results demonstrate that VAP is associated with higher duration in mechanical ventilation, longer length of stay and higher mortality.
Search
Search in:
KEY WORDS
Case reports Child Coronavirus infections COVID-19 Critical care Critical illness Extracorporeal membrane oxygenation Infant, newborn Intensive care Intensive care units Intensive care units, pediatric mechanical ventilation Mortality Physical therapy modalities Prognosis Respiration, artificial Respiratory insufficiency risk factors SARS-CoV-2 Sepsis