Ultrasonography Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2011;23(2):217-221
DOI 10.1590/S0103-507X2011000200015
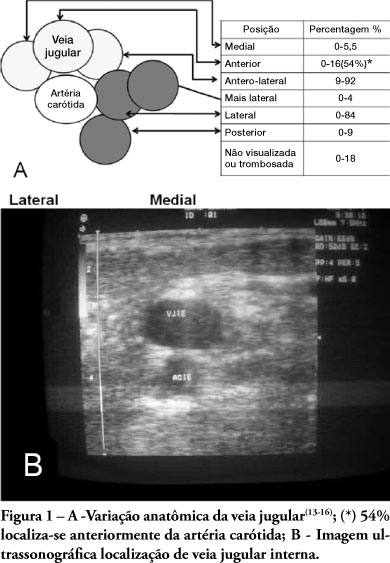
In recent years, international health quality assurance organizations have been recommending ultrasound guidance for central venous punctures. This article reviews the evidence behind these recommendations. The MEDLINE, PubMed and SCIELO databases were searched for the following MeSH terms: central venous access, ultrasonography, and adults. The search was conducted on September 24, 2010, and selected meta-analyses, randomized clinical trials and reviews, retrieving 291 papers. The 21 most important papers were analyzed in this review. The internal jugular vein is the most studied ultrasound-guided puncture site, with meta-analysis showing lower relative risks of failure and complications. In addition, the largest available randomized clinical trial demonstrated a reduced central venous catheter-associated blood stream infection rate. There are few studies involving subclavian vein puncture; however, ultrasound was shown to be beneficial in two meta-analyses (however, with small numbers of patients). Regarding the femoral venous site, only one randomized clinical trial (20 patients) was identified, showing positive findings. In a British cost-effectiveness study, ultrasound use lead to resource savings for different sites of venous puncture. There is strong evidence for ultrasound benefit for internal jugular vein puncture. Although the method appears attractive for the other sites, the data are not sufficient to support any recommendation.
Abstract
Rev Bras Ter Intensiva. 2011;23(2):217-221
DOI 10.1590/S0103-507X2011000200015
In recent years, international health quality assurance organizations have been recommending ultrasound guidance for central venous punctures. This article reviews the evidence behind these recommendations. The MEDLINE, PubMed and SCIELO databases were searched for the following MeSH terms: central venous access, ultrasonography, and adults. The search was conducted on September 24, 2010, and selected meta-analyses, randomized clinical trials and reviews, retrieving 291 papers. The 21 most important papers were analyzed in this review. The internal jugular vein is the most studied ultrasound-guided puncture site, with meta-analysis showing lower relative risks of failure and complications. In addition, the largest available randomized clinical trial demonstrated a reduced central venous catheter-associated blood stream infection rate. There are few studies involving subclavian vein puncture; however, ultrasound was shown to be beneficial in two meta-analyses (however, with small numbers of patients). Regarding the femoral venous site, only one randomized clinical trial (20 patients) was identified, showing positive findings. In a British cost-effectiveness study, ultrasound use lead to resource savings for different sites of venous puncture. There is strong evidence for ultrasound benefit for internal jugular vein puncture. Although the method appears attractive for the other sites, the data are not sufficient to support any recommendation.
Abstract
Rev Bras Ter Intensiva. 2010;22(3):291-299
DOI 10.1590/S0103-507X2010000300012
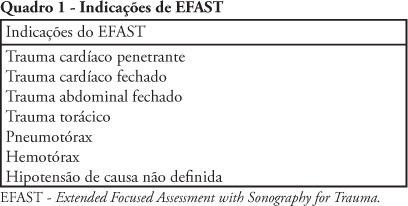
Trauma is the leading cause of death in people below 45 years-old in Brazil, and responsible for one third of all intensive care unit admissions. The increasing knowledge on ultrasound diagnosis methods and its availability for life-threatening injuries (such as cardiac tamponade and abdominal cavity solid organs rupture leading to hemorrhagic shock) diagnosis and monitoring, lead to the development o the FAST (Focused Assessment with Sonography for Trauma) protocol, aimed to be used both in the emergency and intensive care unit settings. Due to its reproducibility, lack of radiation exposure, and bedside feasibility, this technology is being increasingly accepted. A new protocol extension, the Extended-FAST, provides valuable information for improved patients' management, extending its availability from the abdominal conditions to other diagnosis such as hemothorax, pleural effusion and pneumothorax. We must underline that this technique is able to replace computed tomography and diagnostic peritoneal wash, and do not delay surgical procedure instead of perform this exam . Thus, its careful appraisal in connection with the clinical information should guide the therapeutic approaches, specially in inhospitable sites such as intensive care units in war zones, rural or distant places, were other imagery methods are not available.
Abstract
Rev Bras Ter Intensiva. 2010;22(3):291-299
DOI 10.1590/S0103-507X2010000300012
Trauma is the leading cause of death in people below 45 years-old in Brazil, and responsible for one third of all intensive care unit admissions. The increasing knowledge on ultrasound diagnosis methods and its availability for life-threatening injuries (such as cardiac tamponade and abdominal cavity solid organs rupture leading to hemorrhagic shock) diagnosis and monitoring, lead to the development o the FAST (Focused Assessment with Sonography for Trauma) protocol, aimed to be used both in the emergency and intensive care unit settings. Due to its reproducibility, lack of radiation exposure, and bedside feasibility, this technology is being increasingly accepted. A new protocol extension, the Extended-FAST, provides valuable information for improved patients' management, extending its availability from the abdominal conditions to other diagnosis such as hemothorax, pleural effusion and pneumothorax. We must underline that this technique is able to replace computed tomography and diagnostic peritoneal wash, and do not delay surgical procedure instead of perform this exam . Thus, its careful appraisal in connection with the clinical information should guide the therapeutic approaches, specially in inhospitable sites such as intensive care units in war zones, rural or distant places, were other imagery methods are not available.
Abstract
Rev Bras Ter Intensiva. 2009;21(2):190-196
DOI 10.1590/S0103-507X2009000200012
Use of ultrasound introduced as part of intensive care therapy makes viable bedside invasive procedures and diagnosis. Due to portability, combined with team training, its use guarantees less complications related to insertion, as well as patients' safety. It also reduces severe conditions related to the catheter, such as pneumothorax among others. Probably, in a near future, as purchase of ultrasound equipment becomes easier and team training more adequate, this tool will become essential in daily clinical practice.
Abstract
Rev Bras Ter Intensiva. 2009;21(2):190-196
DOI 10.1590/S0103-507X2009000200012
Use of ultrasound introduced as part of intensive care therapy makes viable bedside invasive procedures and diagnosis. Due to portability, combined with team training, its use guarantees less complications related to insertion, as well as patients' safety. It also reduces severe conditions related to the catheter, such as pneumothorax among others. Probably, in a near future, as purchase of ultrasound equipment becomes easier and team training more adequate, this tool will become essential in daily clinical practice.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (116) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)