
You searched for:"Felippe Leopoldo Dexheimer Neto"
We found (6) results for your search.-
Letter to the Editor
Multiple organ dysfunction – we must take a closer look at muscle wasting!
Rev Bras Ter Intensiva. 2019;31(2):269-270
Abstract
Letter to the EditorMultiple organ dysfunction – we must take a closer look at muscle wasting!
Rev Bras Ter Intensiva. 2019;31(2):269-270
DOI 10.5935/0103-507X.20190021
Views1To the editor Organ dysfunction is quantified routinely by scores such as: the Sequential Organ Failure Assessment (SOFA) score, the Multiple Organ Dysfunction Score (MODS), and the Logistic Organ Dysfunction Score (LODS).() Once the number of organs failure is associated with intensive care unit (ICU) and hospital-mortality, these scores are helpful to only predict acute […]See moreViews1

Abstract
Letter to the EditorMultiple organ dysfunction – we must take a closer look at muscle wasting!
Rev Bras Ter Intensiva. 2019;31(2):269-270
DOI 10.5935/0103-507X.20190021
Views1To the editor Organ dysfunction is quantified routinely by scores such as: the Sequential Organ Failure Assessment (SOFA) score, the Multiple Organ Dysfunction Score (MODS), and the Logistic Organ Dysfunction Score (LODS).() Once the number of organs failure is associated with intensive care unit (ICU) and hospital-mortality, these scores are helpful to only predict acute […]See more -
Case Report
Use of thoracic electrical impedance tomography as an auxiliary tool for alveolar recruitment maneuvers in acute respiratory distress syndrome: case report and brief literature review
Rev Bras Ter Intensiva. 2015;27(4):406-411
Abstract
Case ReportUse of thoracic electrical impedance tomography as an auxiliary tool for alveolar recruitment maneuvers in acute respiratory distress syndrome: case report and brief literature review
Rev Bras Ter Intensiva. 2015;27(4):406-411
DOI 10.5935/0103-507X.20150068
Views0ABSTRACT
Thoracic electrical impedance tomography is a real-time, noninvasive monitoring tool of the regional pulmonary ventilation distribution. Its bedside use in patients with acute respiratory distress syndrome has the potential to aid in alveolar recruitment maneuvers, which are often necessary in cases of refractory hypoxemia. In this case report, we describe the monitoring results and interpretation of thoracic electrical impedance tomography used during alveolar recruitment maneuvers in a patient with acute respiratory distress syndrome, with transient application of high alveolar pressures and optimal positive end-expiratory pressure titration. Furthermore, we provide a brief literature review regarding the use of alveolar recruitment maneuvers and monitoring using thoracic electrical impedance tomography in patients with acute respiratory distress syndrome.
Keywords:Cardiography, impedanceCase reportsMonitoring, physiologicRespiratory insufficiency/physiopathologyRespiratory mechanicsSee moreViews0Abstract
Case ReportUse of thoracic electrical impedance tomography as an auxiliary tool for alveolar recruitment maneuvers in acute respiratory distress syndrome: case report and brief literature review
Rev Bras Ter Intensiva. 2015;27(4):406-411
DOI 10.5935/0103-507X.20150068
Views0ABSTRACT
Thoracic electrical impedance tomography is a real-time, noninvasive monitoring tool of the regional pulmonary ventilation distribution. Its bedside use in patients with acute respiratory distress syndrome has the potential to aid in alveolar recruitment maneuvers, which are often necessary in cases of refractory hypoxemia. In this case report, we describe the monitoring results and interpretation of thoracic electrical impedance tomography used during alveolar recruitment maneuvers in a patient with acute respiratory distress syndrome, with transient application of high alveolar pressures and optimal positive end-expiratory pressure titration. Furthermore, we provide a brief literature review regarding the use of alveolar recruitment maneuvers and monitoring using thoracic electrical impedance tomography in patients with acute respiratory distress syndrome.
Keywords:Cardiography, impedanceCase reportsMonitoring, physiologicRespiratory insufficiency/physiopathologyRespiratory mechanicsSee more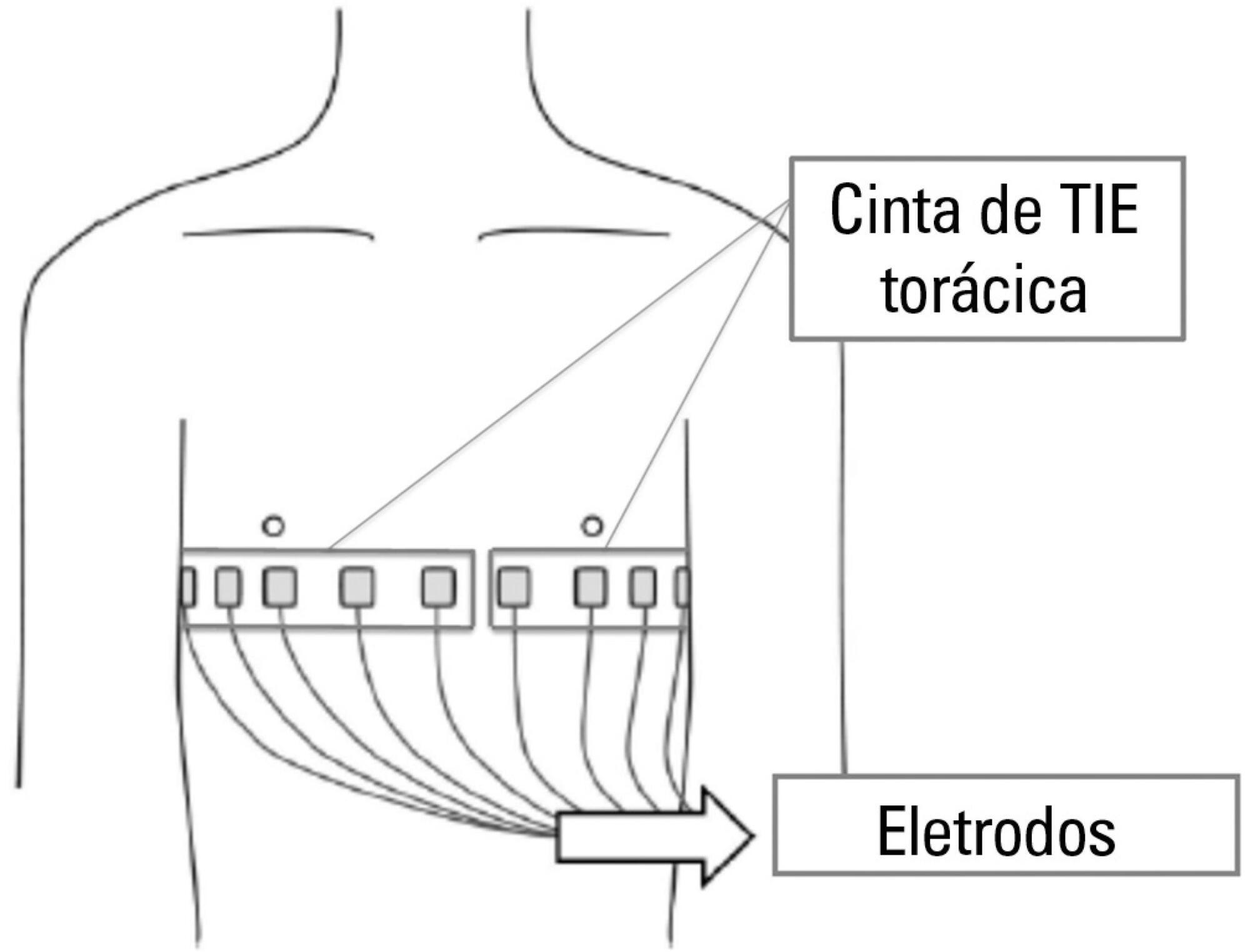
-
Case Report
Platypnea-orthodeoxia syndrome in patients presenting enlarged aortic root: case report and literature review
Rev Bras Ter Intensiva. 2014;26(3):313-316
Abstract
Case ReportPlatypnea-orthodeoxia syndrome in patients presenting enlarged aortic root: case report and literature review
Rev Bras Ter Intensiva. 2014;26(3):313-316
DOI 10.5935/0103-507X.20140044
Views0See moreWe describe herein a case of a patient who, when in orthostatic positions, had severe hypoxemia and ventilatory dysfunction. Although the severity of symptoms required hospitalization in an intensive care setting, the initial tests only identified the presence of enlarged aortic root, which did not explain the condition. The association of these events with an unusual etiology, namely intracardiac shunt, characterized the diagnosis of platypnea-orthodeoxia syndrome. The literature review shows that, with advancing research methods, there was a progressive increase in the identification of this condition, and this association should be part of the differential diagnosis of dyspnea in patients with enlarged aortic root.
Views0Abstract
Case ReportPlatypnea-orthodeoxia syndrome in patients presenting enlarged aortic root: case report and literature review
Rev Bras Ter Intensiva. 2014;26(3):313-316
DOI 10.5935/0103-507X.20140044
Views0See moreWe describe herein a case of a patient who, when in orthostatic positions, had severe hypoxemia and ventilatory dysfunction. Although the severity of symptoms required hospitalization in an intensive care setting, the initial tests only identified the presence of enlarged aortic root, which did not explain the condition. The association of these events with an unusual etiology, namely intracardiac shunt, characterized the diagnosis of platypnea-orthodeoxia syndrome. The literature review shows that, with advancing research methods, there was a progressive increase in the identification of this condition, and this association should be part of the differential diagnosis of dyspnea in patients with enlarged aortic root.

-
Original Article
Out-of-bed extubation: a feasibility study
Rev Bras Ter Intensiva. 2014;26(3):263-268
Abstract
Original ArticleOut-of-bed extubation: a feasibility study
Rev Bras Ter Intensiva. 2014;26(3):263-268
DOI 10.5935/0103-507X.20140037
Views2See moreObjective:
In clinical intensive care practice, weaning from mechanical ventilation is accompanied by concurrent early patient mobilization. The aim of this study was to compare the success of extubation performed with patients seated in an armchair compared to extubation with patients in a supine position.
Methods:
A retrospective study, observational and non-randomized was conducted in a mixed-gender, 23-bed intensive care unit. The primary study outcome was success of extubation, which was defined as the patient tolerating the removal of the endotracheal tube for at least 48 hours. The differences between the study groups were assessed using Student’s t-test and chi-squared analysis.
Results:
Ninety-one patients were included from December 2010 and June 2011. The study population had a mean age of 71 years ± 12 months, a mean APACHE II score of 21±7.6, and a mean length of mechanical ventilation of 2.6±2 days. Extubation was performed in 33 patients who were seated in an armchair (36%) and in 58 patients in a supine position (64%). There were no significant differences in age, mean APACHE II score or length of mechanical ventilation between the two groups, and a similar extubation success rate was observed (82%, seated group versus 85%, supine group, p>0.05). Furthermore, no significant differences were found between the two groups in terms of post-extubation distress, need for tracheostomy, duration of mechanical ventilation weaning, or intensive care unit stay.
Conclusion:
Our results suggest that the clinical outcomes of patients extubated in a seated position are similar to those of patients extubated in a supine position. This new practice of seated extubation was not associated with adverse events and allowed extubation to occur simultaneously with early mobilization.
Views2Abstract
Original ArticleOut-of-bed extubation: a feasibility study
Rev Bras Ter Intensiva. 2014;26(3):263-268
DOI 10.5935/0103-507X.20140037
Views2See moreObjective:
In clinical intensive care practice, weaning from mechanical ventilation is accompanied by concurrent early patient mobilization. The aim of this study was to compare the success of extubation performed with patients seated in an armchair compared to extubation with patients in a supine position.
Methods:
A retrospective study, observational and non-randomized was conducted in a mixed-gender, 23-bed intensive care unit. The primary study outcome was success of extubation, which was defined as the patient tolerating the removal of the endotracheal tube for at least 48 hours. The differences between the study groups were assessed using Student’s t-test and chi-squared analysis.
Results:
Ninety-one patients were included from December 2010 and June 2011. The study population had a mean age of 71 years ± 12 months, a mean APACHE II score of 21±7.6, and a mean length of mechanical ventilation of 2.6±2 days. Extubation was performed in 33 patients who were seated in an armchair (36%) and in 58 patients in a supine position (64%). There were no significant differences in age, mean APACHE II score or length of mechanical ventilation between the two groups, and a similar extubation success rate was observed (82%, seated group versus 85%, supine group, p>0.05). Furthermore, no significant differences were found between the two groups in terms of post-extubation distress, need for tracheostomy, duration of mechanical ventilation weaning, or intensive care unit stay.
Conclusion:
Our results suggest that the clinical outcomes of patients extubated in a seated position are similar to those of patients extubated in a supine position. This new practice of seated extubation was not associated with adverse events and allowed extubation to occur simultaneously with early mobilization.
-
Ultrasound-guided central venous catheterization: what is the evidence?
Rev Bras Ter Intensiva. 2011;23(2):217-221
Abstract
Ultrasound-guided central venous catheterization: what is the evidence?
Rev Bras Ter Intensiva. 2011;23(2):217-221
DOI 10.1590/S0103-507X2011000200015
Views0See moreIn recent years, international health quality assurance organizations have been recommending ultrasound guidance for central venous punctures. This article reviews the evidence behind these recommendations. The MEDLINE, PubMed and SCIELO databases were searched for the following MeSH terms: central venous access, ultrasonography, and adults. The search was conducted on September 24, 2010, and selected meta-analyses, randomized clinical trials and reviews, retrieving 291 papers. The 21 most important papers were analyzed in this review. The internal jugular vein is the most studied ultrasound-guided puncture site, with meta-analysis showing lower relative risks of failure and complications. In addition, the largest available randomized clinical trial demonstrated a reduced central venous catheter-associated blood stream infection rate. There are few studies involving subclavian vein puncture; however, ultrasound was shown to be beneficial in two meta-analyses (however, with small numbers of patients). Regarding the femoral venous site, only one randomized clinical trial (20 patients) was identified, showing positive findings. In a British cost-effectiveness study, ultrasound use lead to resource savings for different sites of venous puncture. There is strong evidence for ultrasound benefit for internal jugular vein puncture. Although the method appears attractive for the other sites, the data are not sufficient to support any recommendation.
Views0Abstract
Ultrasound-guided central venous catheterization: what is the evidence?
Rev Bras Ter Intensiva. 2011;23(2):217-221
DOI 10.1590/S0103-507X2011000200015
Views0See moreIn recent years, international health quality assurance organizations have been recommending ultrasound guidance for central venous punctures. This article reviews the evidence behind these recommendations. The MEDLINE, PubMed and SCIELO databases were searched for the following MeSH terms: central venous access, ultrasonography, and adults. The search was conducted on September 24, 2010, and selected meta-analyses, randomized clinical trials and reviews, retrieving 291 papers. The 21 most important papers were analyzed in this review. The internal jugular vein is the most studied ultrasound-guided puncture site, with meta-analysis showing lower relative risks of failure and complications. In addition, the largest available randomized clinical trial demonstrated a reduced central venous catheter-associated blood stream infection rate. There are few studies involving subclavian vein puncture; however, ultrasound was shown to be beneficial in two meta-analyses (however, with small numbers of patients). Regarding the femoral venous site, only one randomized clinical trial (20 patients) was identified, showing positive findings. In a British cost-effectiveness study, ultrasound use lead to resource savings for different sites of venous puncture. There is strong evidence for ultrasound benefit for internal jugular vein puncture. Although the method appears attractive for the other sites, the data are not sufficient to support any recommendation.
-
Original Articles
Appropriate medical professionals communication reduces intensive care unit mortality
Rev Bras Ter Intensiva. 2010;22(2):112-117
Abstract
Original ArticlesAppropriate medical professionals communication reduces intensive care unit mortality
Rev Bras Ter Intensiva. 2010;22(2):112-117
DOI 10.1590/S0103-507X2010000200003
Views0See moreOBJECTIVES: Communication issues between healthcare professionals in intensive care units may be related to critically ill patients’ increased mortality. This study aimed to evaluate if communication issues involving assistant physicians and routine intensive care unit physicians would impact critically ill patients’ morbidity and mortality. METHODS: This was a cohort study that included non-consecutive patients admitted to the intensive care unit for 18 months. The patients were categorized in 3 groups according to their assistant doctors’ versus routine doctors communication uses: DC – daily communication during the stay (>75% of the days); EC – eventual communication (25 to 75% of the days); RC – rare communication (< 25% of the days). Demographic data, severity scores, reason for admission to the intensive care unit and interventions were recorded. The consequences of the medical professionals communication failures (delayed procedures, diagnostic tests, antibiotics, ventilatory weaning, vasopressors) and medical prescriptions inadequacies (no bed head elevation, no stress ulceration and deep venous thrombosis drug prophylaxis), and their relationship with the patients outcomes were analyzed. RESULTS: 792 patients were included, and categorized as follows: DC (n=529); EC (n=187) and RC (n=76). The mortality was increased in the RC patients group (26.3%) versus the remainder groups (DC = 13.6% and EC = 17.1%; p<0.05). A multivariate analysis showed that delayed antibiotics [RR 1.83 (CI95%: 1.36 -2.25)], delayed ventilatory weaning [RR 1.63 (CI95%: 1.25-2.04)] and no deep venous thrombosis prophylaxis [RR 1.98 (CI95%: 1.43 - 3.12)] contributed independently for the increased mortality. CONCLUSION: The failure in the assistant and routine intensive care doctors communication may increase the patients’ mortality, particularly due to delayed antibiotics and ventilation weaning, and lack of deep venous thrombosis prophylaxis prescription.
Views0Abstract
Original ArticlesAppropriate medical professionals communication reduces intensive care unit mortality
Rev Bras Ter Intensiva. 2010;22(2):112-117
DOI 10.1590/S0103-507X2010000200003
Views0See moreOBJECTIVES: Communication issues between healthcare professionals in intensive care units may be related to critically ill patients’ increased mortality. This study aimed to evaluate if communication issues involving assistant physicians and routine intensive care unit physicians would impact critically ill patients’ morbidity and mortality. METHODS: This was a cohort study that included non-consecutive patients admitted to the intensive care unit for 18 months. The patients were categorized in 3 groups according to their assistant doctors’ versus routine doctors communication uses: DC – daily communication during the stay (>75% of the days); EC – eventual communication (25 to 75% of the days); RC – rare communication (< 25% of the days). Demographic data, severity scores, reason for admission to the intensive care unit and interventions were recorded. The consequences of the medical professionals communication failures (delayed procedures, diagnostic tests, antibiotics, ventilatory weaning, vasopressors) and medical prescriptions inadequacies (no bed head elevation, no stress ulceration and deep venous thrombosis drug prophylaxis), and their relationship with the patients outcomes were analyzed. RESULTS: 792 patients were included, and categorized as follows: DC (n=529); EC (n=187) and RC (n=76). The mortality was increased in the RC patients group (26.3%) versus the remainder groups (DC = 13.6% and EC = 17.1%; p<0.05). A multivariate analysis showed that delayed antibiotics [RR 1.83 (CI95%: 1.36 -2.25)], delayed ventilatory weaning [RR 1.63 (CI95%: 1.25-2.04)] and no deep venous thrombosis prophylaxis [RR 1.98 (CI95%: 1.43 - 3.12)] contributed independently for the increased mortality. CONCLUSION: The failure in the assistant and routine intensive care doctors communication may increase the patients’ mortality, particularly due to delayed antibiotics and ventilation weaning, and lack of deep venous thrombosis prophylaxis prescription.
Search
Search in:
KEY WORDS
Case reports Child Coronavirus infections COVID-19 Critical care Critical illness Extracorporeal membrane oxygenation Infant, newborn Intensive care Intensive care units Intensive care units, pediatric mechanical ventilation Mortality Physical therapy modalities Prognosis Respiration, artificial Respiratory insufficiency risk factors SARS-CoV-2 Sepsis