Patient positioning Archives - Critical Care Science (CCS)

Abstract
Crit Care Sci. 2024;36:e20240176en
DOI 10.62675/2965-2774.20240176-en
To systematically review the effect of the prone position on endotracheal intubation and mortality in nonintubated COVID-19 patients with acute respiratory distress syndrome.
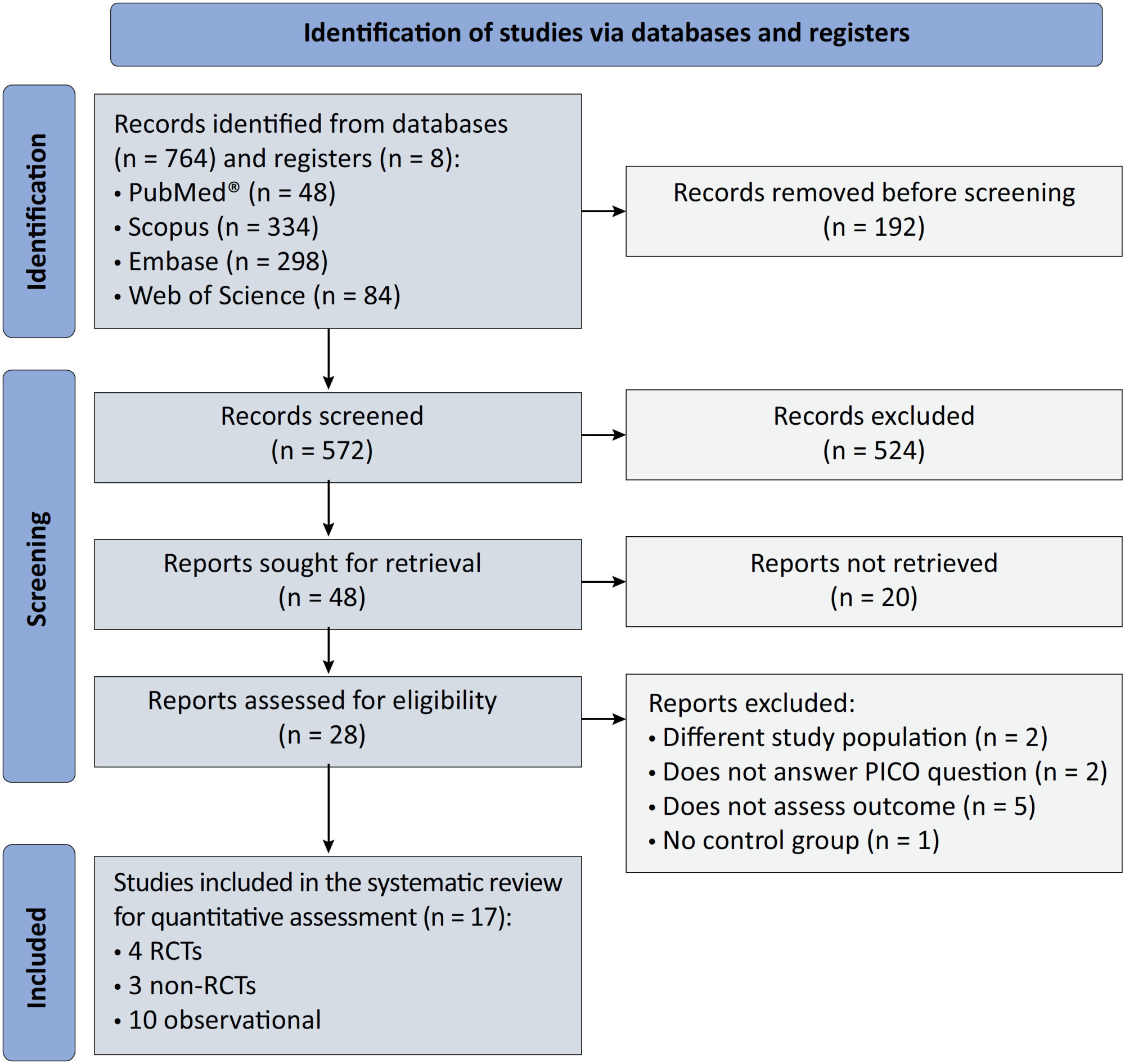
We registered the protocol (CRD42021286711) and searched for four databases and gray literature from inception to December 31, 2022. We included observational studies and clinical trials. There was no limit by date or the language of publication. We excluded case reports, case series, studies not available in full text, and those studies that included children < 18-years-old.
We included ten observational studies, eight clinical trials, 3,969 patients, 1,120 endotracheal intubation events, and 843 deaths. All of the studies had a low risk of bias (Newcastle-Ottawa Scale and Risk of Bias 2 tools). We found that the conscious prone position decreased the odds of endotracheal intubation by 44% (OR 0.56; 95%CI 0.40 - 0.78) and mortality by 43% (OR 0.57; 95%CI 0.39 - 0.84) in nonintubated COVID-19 patients with acute respiratory distress syndrome. This protective effect on endotracheal intubation and mortality was more robust in those who spent > 8 hours/day in the conscious prone position (OR 0.43; 95%CI 0.26 - 0.72 and OR 0.38; 95%CI 0.24 - 0.60, respectively). The certainty of the evidence according to the GRADE criteria was moderate.
The conscious prone position decreased the odds of endotracheal intubation and mortality, especially when patients spent over 8 hours/day in the conscious prone position and treatment in the intensive care unit. However, our results should be cautiously interpreted due to limitations in evaluating randomized clinical trials, nonrandomized clinical trials and observational studies. However, despite systematic reviews with meta-analyses of randomized clinical trials, we must keep in mind that these studies remain heterogeneous from a clinical and methodological point of view.
Abstract
Crit Care Sci. 2024;36:e20240176en
DOI 10.62675/2965-2774.20240176-en
To systematically review the effect of the prone position on endotracheal intubation and mortality in nonintubated COVID-19 patients with acute respiratory distress syndrome.
We registered the protocol (CRD42021286711) and searched for four databases and gray literature from inception to December 31, 2022. We included observational studies and clinical trials. There was no limit by date or the language of publication. We excluded case reports, case series, studies not available in full text, and those studies that included children < 18-years-old.
We included ten observational studies, eight clinical trials, 3,969 patients, 1,120 endotracheal intubation events, and 843 deaths. All of the studies had a low risk of bias (Newcastle-Ottawa Scale and Risk of Bias 2 tools). We found that the conscious prone position decreased the odds of endotracheal intubation by 44% (OR 0.56; 95%CI 0.40 - 0.78) and mortality by 43% (OR 0.57; 95%CI 0.39 - 0.84) in nonintubated COVID-19 patients with acute respiratory distress syndrome. This protective effect on endotracheal intubation and mortality was more robust in those who spent > 8 hours/day in the conscious prone position (OR 0.43; 95%CI 0.26 - 0.72 and OR 0.38; 95%CI 0.24 - 0.60, respectively). The certainty of the evidence according to the GRADE criteria was moderate.
The conscious prone position decreased the odds of endotracheal intubation and mortality, especially when patients spent over 8 hours/day in the conscious prone position and treatment in the intensive care unit. However, our results should be cautiously interpreted due to limitations in evaluating randomized clinical trials, nonrandomized clinical trials and observational studies. However, despite systematic reviews with meta-analyses of randomized clinical trials, we must keep in mind that these studies remain heterogeneous from a clinical and methodological point of view.
Abstract
Rev Bras Ter Intensiva. 2015;27(4):347-352
DOI 10.5935/0103-507X.20150059
The positioning of a patient in bed may directly affect their respiratory mechanics. The objective of this study was to evaluate the respiratory mechanics of mechanically ventilated patients positioned with different head angles hospitalized in an intensive care unit.
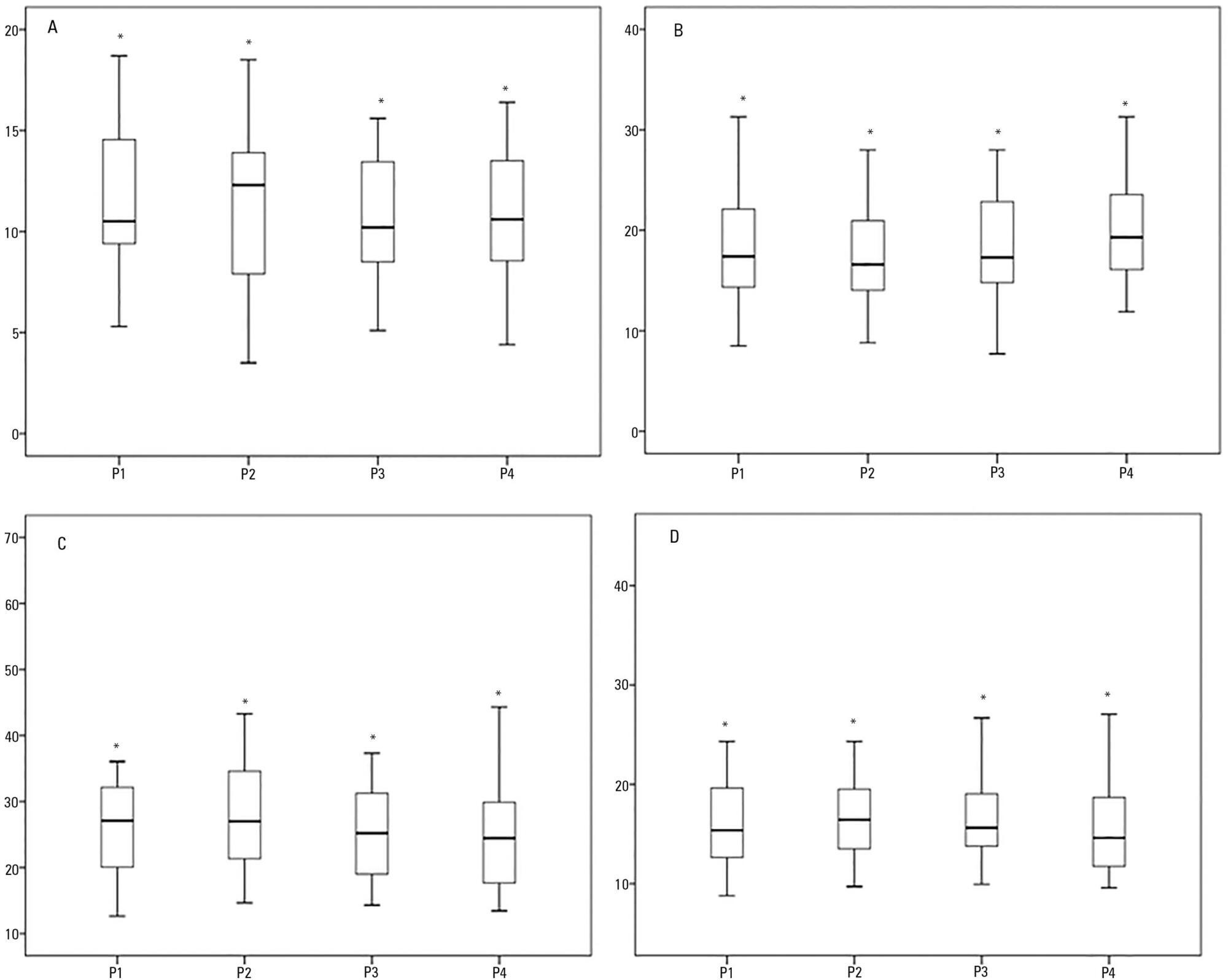
This was a prospective physiological study in which static and dynamic compliance, resistive airway pressure, and peripheral oxygen saturation were measured with the head at four different positions (0° = P1, 30° = P2, 45° = P3, and 60° = P4). Repeated-measures analysis of variance (ANOVA) with a Bonferroni post-test and Friedman analysis were used to compare the values obtained at the different positions.
A comparison of the 35 evaluated patients revealed that the resistive airway pressure values in the 0° position were higher than those obtained when patients were positioned at greater angles. The elastic pressure analysis revealed that the 60° position produced the highest value relative to the other positions. Regarding static compliance, a reduction in values was observed from the 0° position to the 60° position. The dynamic compliance analysis revealed that the 30° angle produced the greatest value compared to the other positions. The peripheral oxygen saturation showed little variation, with the highest value obtained at the 0° position.
The highest dynamic compliance value was observed at the 30° position, and the highest oxygenation value was observed at the 0° position.
Abstract
Rev Bras Ter Intensiva. 2015;27(4):347-352
DOI 10.5935/0103-507X.20150059
The positioning of a patient in bed may directly affect their respiratory mechanics. The objective of this study was to evaluate the respiratory mechanics of mechanically ventilated patients positioned with different head angles hospitalized in an intensive care unit.
This was a prospective physiological study in which static and dynamic compliance, resistive airway pressure, and peripheral oxygen saturation were measured with the head at four different positions (0° = P1, 30° = P2, 45° = P3, and 60° = P4). Repeated-measures analysis of variance (ANOVA) with a Bonferroni post-test and Friedman analysis were used to compare the values obtained at the different positions.
A comparison of the 35 evaluated patients revealed that the resistive airway pressure values in the 0° position were higher than those obtained when patients were positioned at greater angles. The elastic pressure analysis revealed that the 60° position produced the highest value relative to the other positions. Regarding static compliance, a reduction in values was observed from the 0° position to the 60° position. The dynamic compliance analysis revealed that the 30° angle produced the greatest value compared to the other positions. The peripheral oxygen saturation showed little variation, with the highest value obtained at the 0° position.
The highest dynamic compliance value was observed at the 30° position, and the highest oxygenation value was observed at the 0° position.
Abstract
Rev Bras Ter Intensiva. 2014;26(3):263-268
DOI 10.5935/0103-507X.20140037
In clinical intensive care practice, weaning from mechanical ventilation is accompanied by concurrent early patient mobilization. The aim of this study was to compare the success of extubation performed with patients seated in an armchair compared to extubation with patients in a supine position.
A retrospective study, observational and non-randomized was conducted in a mixed-gender, 23-bed intensive care unit. The primary study outcome was success of extubation, which was defined as the patient tolerating the removal of the endotracheal tube for at least 48 hours. The differences between the study groups were assessed using Student's t-test and chi-squared analysis.
Ninety-one patients were included from December 2010 and June 2011. The study population had a mean age of 71 years ± 12 months, a mean APACHE II score of 21±7.6, and a mean length of mechanical ventilation of 2.6±2 days. Extubation was performed in 33 patients who were seated in an armchair (36%) and in 58 patients in a supine position (64%). There were no significant differences in age, mean APACHE II score or length of mechanical ventilation between the two groups, and a similar extubation success rate was observed (82%, seated group versus 85%, supine group, p>0.05). Furthermore, no significant differences were found between the two groups in terms of post-extubation distress, need for tracheostomy, duration of mechanical ventilation weaning, or intensive care unit stay.
Our results suggest that the clinical outcomes of patients extubated in a seated position are similar to those of patients extubated in a supine position. This new practice of seated extubation was not associated with adverse events and allowed extubation to occur simultaneously with early mobilization.
Abstract
Rev Bras Ter Intensiva. 2014;26(3):263-268
DOI 10.5935/0103-507X.20140037
In clinical intensive care practice, weaning from mechanical ventilation is accompanied by concurrent early patient mobilization. The aim of this study was to compare the success of extubation performed with patients seated in an armchair compared to extubation with patients in a supine position.
A retrospective study, observational and non-randomized was conducted in a mixed-gender, 23-bed intensive care unit. The primary study outcome was success of extubation, which was defined as the patient tolerating the removal of the endotracheal tube for at least 48 hours. The differences between the study groups were assessed using Student's t-test and chi-squared analysis.
Ninety-one patients were included from December 2010 and June 2011. The study population had a mean age of 71 years ± 12 months, a mean APACHE II score of 21±7.6, and a mean length of mechanical ventilation of 2.6±2 days. Extubation was performed in 33 patients who were seated in an armchair (36%) and in 58 patients in a supine position (64%). There were no significant differences in age, mean APACHE II score or length of mechanical ventilation between the two groups, and a similar extubation success rate was observed (82%, seated group versus 85%, supine group, p>0.05). Furthermore, no significant differences were found between the two groups in terms of post-extubation distress, need for tracheostomy, duration of mechanical ventilation weaning, or intensive care unit stay.
Our results suggest that the clinical outcomes of patients extubated in a seated position are similar to those of patients extubated in a supine position. This new practice of seated extubation was not associated with adverse events and allowed extubation to occur simultaneously with early mobilization.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (33) COVID-19 (45) Critical care (115) Critical illness (54) ICU (25) Infant, newborn (27) Intensive care (72) Intensive care units (254) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (75) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (117) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)