
You searched for:"Rafael Viegas Cremonese"
We found (3) results for your search.-
Original Article
Neutrophil-lymphocyte ratio in the early diagnosis of sepsis in an intensive care unit: a case-control study
Rev Bras Ter Intensiva. 2019;31(1):64-70
Abstract
Original ArticleNeutrophil-lymphocyte ratio in the early diagnosis of sepsis in an intensive care unit: a case-control study
Rev Bras Ter Intensiva. 2019;31(1):64-70
DOI 10.5935/0103-507X.20190010
Views0ABSTRACT
Objective:
To evaluate the neutrophil-lymphocyte ratio as a predictor of sepsis and mortality in patients admitted to an intensive care unit.
Methods:
Case-control study of adult patients admitted to an intensive care unit. Patients who had sepsis as the reason for admission and who had a previous complete blood count examination were included as case patients. The following statistical analyses were performed: ROC curves, binary logistic regression, and Mann-Whitney and Pearson’s chi-square tests. p < 0.05 was considered significant.
Results:
The ROC curve values were 0.62 for neutrophil-lymphocyte ratio, 0.98 for band neutrophils and 0.51 for total leukocytes. The presence of a neutrophil-lymphocyte ratio greater than 5.0, leukocyte count above 12,000mm3/mL and band neutrophil percentage above 10% were risk factors for sepsis; however, only the SAPS 3 and SOFA score were related to patient mortality.
Conclusion:
The neutrophil-lymphocyte ratio and band neutrophils in combination with other parameters may be markers for the early detection of sepsis in intensive care units.
Keywords:Blood cell countClinical laboratory techniquesIntensive care unitsLymphocyte count/methodsNeutrophilsSepsis/diagnosisSee moreViews0

Abstract
Original ArticleNeutrophil-lymphocyte ratio in the early diagnosis of sepsis in an intensive care unit: a case-control study
Rev Bras Ter Intensiva. 2019;31(1):64-70
DOI 10.5935/0103-507X.20190010
Views0ABSTRACT
Objective:
To evaluate the neutrophil-lymphocyte ratio as a predictor of sepsis and mortality in patients admitted to an intensive care unit.
Methods:
Case-control study of adult patients admitted to an intensive care unit. Patients who had sepsis as the reason for admission and who had a previous complete blood count examination were included as case patients. The following statistical analyses were performed: ROC curves, binary logistic regression, and Mann-Whitney and Pearson’s chi-square tests. p < 0.05 was considered significant.
Results:
The ROC curve values were 0.62 for neutrophil-lymphocyte ratio, 0.98 for band neutrophils and 0.51 for total leukocytes. The presence of a neutrophil-lymphocyte ratio greater than 5.0, leukocyte count above 12,000mm3/mL and band neutrophil percentage above 10% were risk factors for sepsis; however, only the SAPS 3 and SOFA score were related to patient mortality.
Conclusion:
The neutrophil-lymphocyte ratio and band neutrophils in combination with other parameters may be markers for the early detection of sepsis in intensive care units.
Keywords:Blood cell countClinical laboratory techniquesIntensive care unitsLymphocyte count/methodsNeutrophilsSepsis/diagnosisSee more -
Original Article
Out-of-bed extubation: a feasibility study
Rev Bras Ter Intensiva. 2014;26(3):263-268
Abstract
Original ArticleOut-of-bed extubation: a feasibility study
Rev Bras Ter Intensiva. 2014;26(3):263-268
DOI 10.5935/0103-507X.20140037
Views2See moreObjective:
In clinical intensive care practice, weaning from mechanical ventilation is accompanied by concurrent early patient mobilization. The aim of this study was to compare the success of extubation performed with patients seated in an armchair compared to extubation with patients in a supine position.
Methods:
A retrospective study, observational and non-randomized was conducted in a mixed-gender, 23-bed intensive care unit. The primary study outcome was success of extubation, which was defined as the patient tolerating the removal of the endotracheal tube for at least 48 hours. The differences between the study groups were assessed using Student’s t-test and chi-squared analysis.
Results:
Ninety-one patients were included from December 2010 and June 2011. The study population had a mean age of 71 years ± 12 months, a mean APACHE II score of 21±7.6, and a mean length of mechanical ventilation of 2.6±2 days. Extubation was performed in 33 patients who were seated in an armchair (36%) and in 58 patients in a supine position (64%). There were no significant differences in age, mean APACHE II score or length of mechanical ventilation between the two groups, and a similar extubation success rate was observed (82%, seated group versus 85%, supine group, p>0.05). Furthermore, no significant differences were found between the two groups in terms of post-extubation distress, need for tracheostomy, duration of mechanical ventilation weaning, or intensive care unit stay.
Conclusion:
Our results suggest that the clinical outcomes of patients extubated in a seated position are similar to those of patients extubated in a supine position. This new practice of seated extubation was not associated with adverse events and allowed extubation to occur simultaneously with early mobilization.
Views2Abstract
Original ArticleOut-of-bed extubation: a feasibility study
Rev Bras Ter Intensiva. 2014;26(3):263-268
DOI 10.5935/0103-507X.20140037
Views2See moreObjective:
In clinical intensive care practice, weaning from mechanical ventilation is accompanied by concurrent early patient mobilization. The aim of this study was to compare the success of extubation performed with patients seated in an armchair compared to extubation with patients in a supine position.
Methods:
A retrospective study, observational and non-randomized was conducted in a mixed-gender, 23-bed intensive care unit. The primary study outcome was success of extubation, which was defined as the patient tolerating the removal of the endotracheal tube for at least 48 hours. The differences between the study groups were assessed using Student’s t-test and chi-squared analysis.
Results:
Ninety-one patients were included from December 2010 and June 2011. The study population had a mean age of 71 years ± 12 months, a mean APACHE II score of 21±7.6, and a mean length of mechanical ventilation of 2.6±2 days. Extubation was performed in 33 patients who were seated in an armchair (36%) and in 58 patients in a supine position (64%). There were no significant differences in age, mean APACHE II score or length of mechanical ventilation between the two groups, and a similar extubation success rate was observed (82%, seated group versus 85%, supine group, p>0.05). Furthermore, no significant differences were found between the two groups in terms of post-extubation distress, need for tracheostomy, duration of mechanical ventilation weaning, or intensive care unit stay.
Conclusion:
Our results suggest that the clinical outcomes of patients extubated in a seated position are similar to those of patients extubated in a supine position. This new practice of seated extubation was not associated with adverse events and allowed extubation to occur simultaneously with early mobilization.
-
Original Articles
Functional and psychological features immediately after discharge from an Intensive Care Unit: prospective cohort study
Rev Bras Ter Intensiva. 2013;25(3):218-224
Abstract
Original ArticlesFunctional and psychological features immediately after discharge from an Intensive Care Unit: prospective cohort study
Rev Bras Ter Intensiva. 2013;25(3):218-224
DOI 10.5935/0103-507X.20130038
Views1See moreOBJECTIVE:
To assess the functional and psychological features of patients immediately after discharge from the intensive care unit.
METHODS:
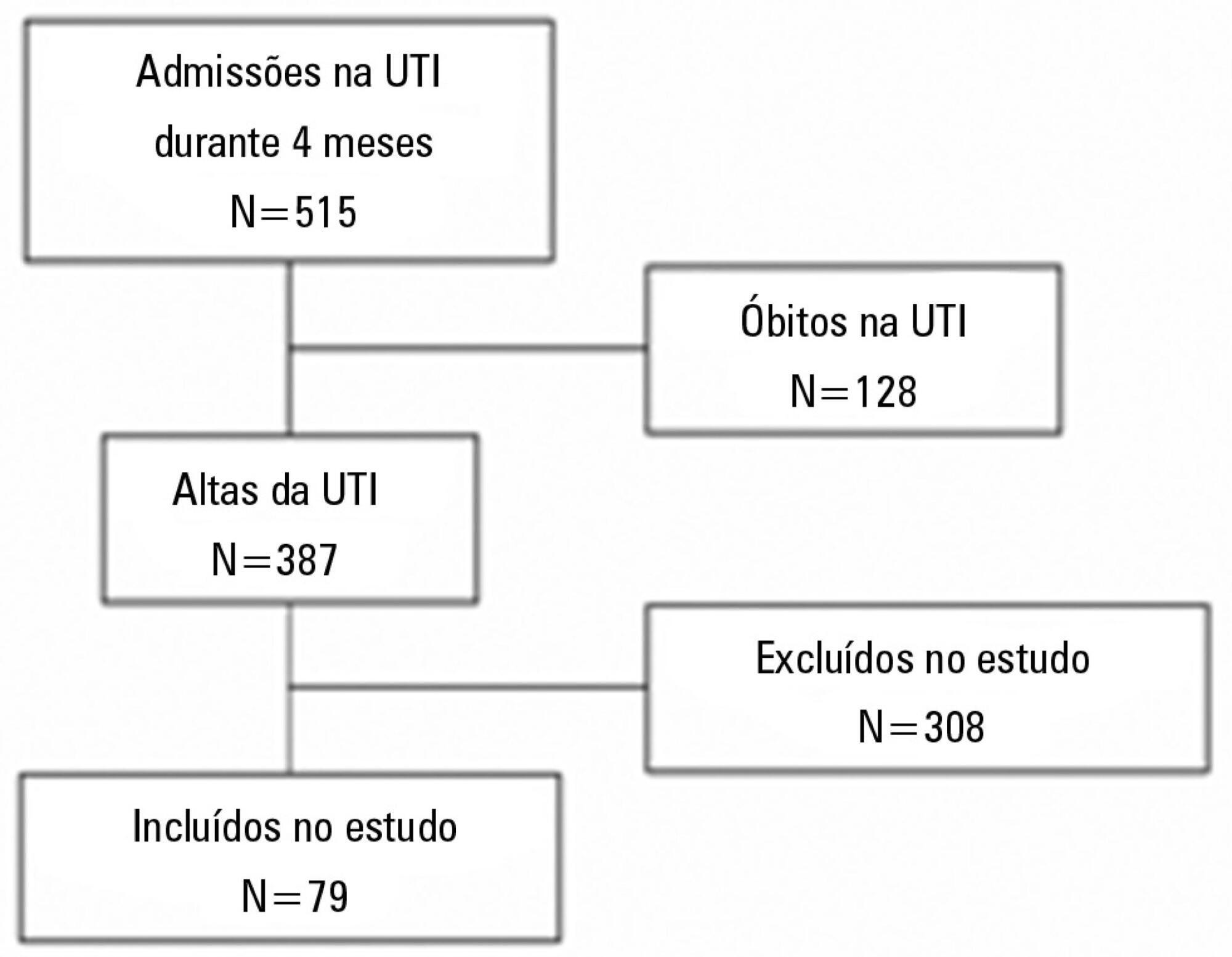
Prospective cohort study. Questionnaires and scales assessing the degree of dependence and functional capacity (modified Barthel and Karnofsky scales) and psychological problems (Hospital Anxiety and Depression Scale), in addition to the Epworth Sleepiness Scale, were administered during interviews conducted over the first week after intensive care unit discharge, to all survivors who had been admitted to this service from August to November 2012 and had remained longer than 72 hours.
RESULTS:
The degree of dependence as measured by the modified Barthel scale increased after intensive care unit discharge compared with the data before admission (57±30 versus 47±36; p<0.001) in all 79 participants. This impairment was homogeneous among all the categories in the modified Barthel scale (p<0.001) in the 64 participants who were independent or partially dependent (Karnofsky score ≥40) before admission. The impairment affected the categories of personal hygiene (p=0.01) and stair climbing (p=0.04) only in the 15 participants who were highly dependent (Karnofsky score <40) before admission. Assessment of the psychological changes identified mood disorders (anxiety and/or depression) in 31% of the sample, whereas sleep disorders occurred in 43.3%.
CONCLUSIONS:
Patients who remained in an intensive care unit for 72 hours or longer exhibited a reduced functional capacity and an increased degree of dependence during the first week after intensive care unit discharge. In addition, the incidence of depressive symptoms, anxiety, and sleep disorders was high among that population.
Views1Abstract
Original ArticlesFunctional and psychological features immediately after discharge from an Intensive Care Unit: prospective cohort study
Rev Bras Ter Intensiva. 2013;25(3):218-224
DOI 10.5935/0103-507X.20130038
Views1See moreOBJECTIVE:
To assess the functional and psychological features of patients immediately after discharge from the intensive care unit.
METHODS:
Prospective cohort study. Questionnaires and scales assessing the degree of dependence and functional capacity (modified Barthel and Karnofsky scales) and psychological problems (Hospital Anxiety and Depression Scale), in addition to the Epworth Sleepiness Scale, were administered during interviews conducted over the first week after intensive care unit discharge, to all survivors who had been admitted to this service from August to November 2012 and had remained longer than 72 hours.
RESULTS:
The degree of dependence as measured by the modified Barthel scale increased after intensive care unit discharge compared with the data before admission (57±30 versus 47±36; p<0.001) in all 79 participants. This impairment was homogeneous among all the categories in the modified Barthel scale (p<0.001) in the 64 participants who were independent or partially dependent (Karnofsky score ≥40) before admission. The impairment affected the categories of personal hygiene (p=0.01) and stair climbing (p=0.04) only in the 15 participants who were highly dependent (Karnofsky score <40) before admission. Assessment of the psychological changes identified mood disorders (anxiety and/or depression) in 31% of the sample, whereas sleep disorders occurred in 43.3%.
CONCLUSIONS:
Patients who remained in an intensive care unit for 72 hours or longer exhibited a reduced functional capacity and an increased degree of dependence during the first week after intensive care unit discharge. In addition, the incidence of depressive symptoms, anxiety, and sleep disorders was high among that population.
Search
Search in:
KEY WORDS
Case reports Child Coronavirus infections COVID-19 Critical care Critical illness Extracorporeal membrane oxygenation Infant, newborn Intensive care Intensive care units Intensive care units, pediatric mechanical ventilation Mortality Physical therapy modalities Prognosis Respiration, artificial Respiratory insufficiency risk factors SARS-CoV-2 Sepsis