Point-of-care testing Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2020;32(2):312-318
DOI 10.5935/0103-507X.20200048
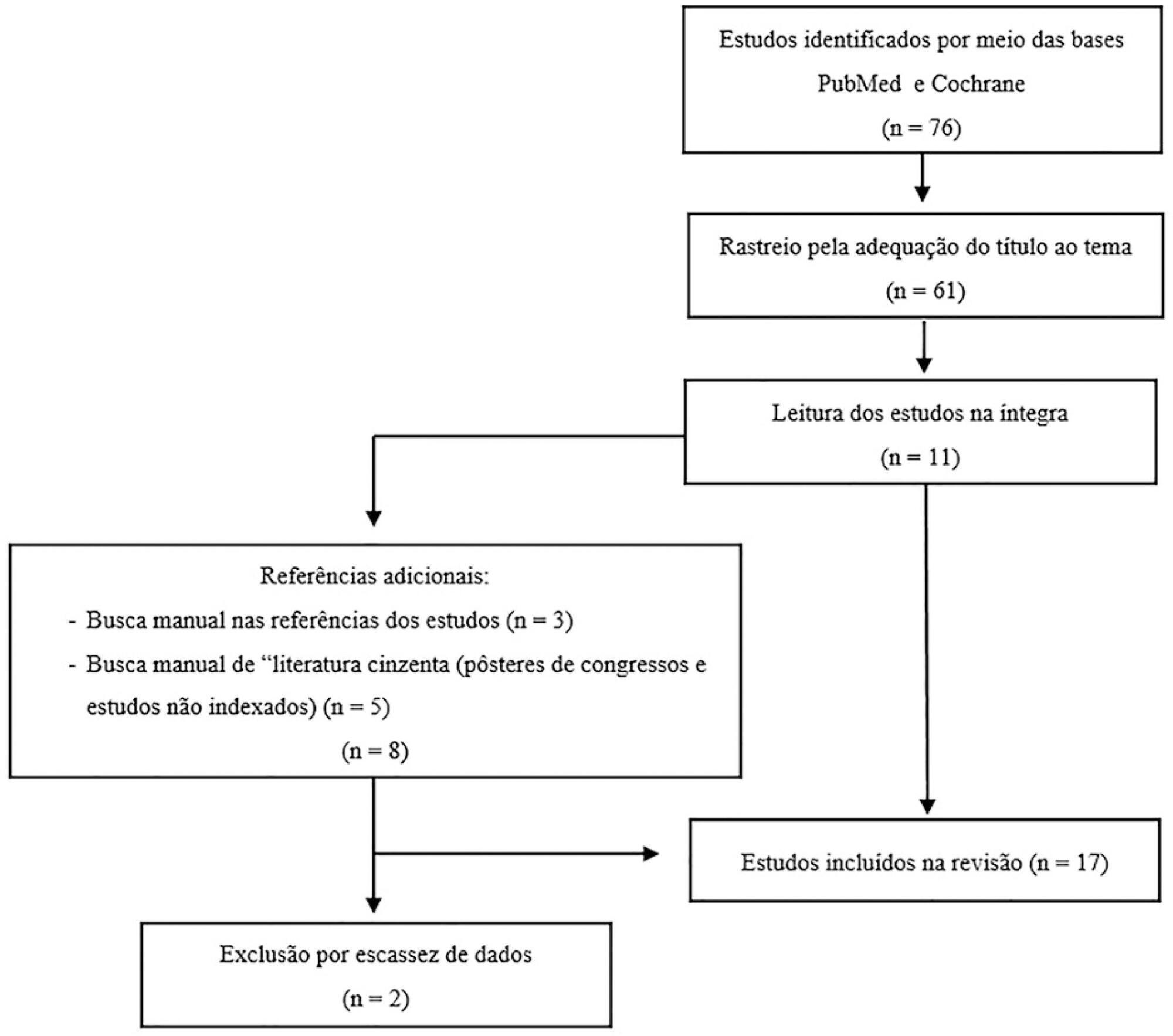
Among the potential complications of extracorporeal membrane oxygenation, neurological dysfunctions, including brain death, are not negligible. In Brazil, the diagnostic process of brain death is regulated by Federal Council of Medicine resolution 2,173 of 2017. Diagnostic tests for brain death include the apnea test, which assesses the presence of a ventilatory response to hypercapnic stimulus. However, gas exchange, including carbon dioxide removal, is maintained under extracorporeal membrane oxygenation, making the test challenging. In addition to the fact that the aforementioned resolution does not consider the specificities of the diagnostic process under extracorporeal membrane oxygenation, studies on the subject are scarce. This review aims to identify case studies (and/or case series) published in the PubMed® and Cochrane databases describing the process of brain death diagnosis. A total of 17 publications (2011 - 2019) were identified. The practical strategies described were to provide pretest supplemental oxygenation via mechanical ventilation and extracorporeal membrane oxygenation (fraction of inspired oxygen = 1.0) and, at the beginning of the test, titrate the sweep flow (0.5 - 1.0L/minute) to minimize carbon dioxide removal. It is also recommended to increase blood flow and/or sweep flow in the presence of hypoxemia and/or hypotension, which may be combined with fluid infusion and/or the escalation of inotropic/vasoactive drugs. If the partial pressure of carbon dioxide threshold is not reached, repeating the test under supplementation of carbon dioxide exogenous to the circuit is an alternative. Last, in cases of venoarterial extracorporeal membrane oxygenation, to measure gas variation and exclude differential hypoxia, blood samples of the native and extracorporeal (post-oxygenator) circulations are recommended.
Abstract
Rev Bras Ter Intensiva. 2020;32(2):312-318
DOI 10.5935/0103-507X.20200048
Among the potential complications of extracorporeal membrane oxygenation, neurological dysfunctions, including brain death, are not negligible. In Brazil, the diagnostic process of brain death is regulated by Federal Council of Medicine resolution 2,173 of 2017. Diagnostic tests for brain death include the apnea test, which assesses the presence of a ventilatory response to hypercapnic stimulus. However, gas exchange, including carbon dioxide removal, is maintained under extracorporeal membrane oxygenation, making the test challenging. In addition to the fact that the aforementioned resolution does not consider the specificities of the diagnostic process under extracorporeal membrane oxygenation, studies on the subject are scarce. This review aims to identify case studies (and/or case series) published in the PubMed® and Cochrane databases describing the process of brain death diagnosis. A total of 17 publications (2011 - 2019) were identified. The practical strategies described were to provide pretest supplemental oxygenation via mechanical ventilation and extracorporeal membrane oxygenation (fraction of inspired oxygen = 1.0) and, at the beginning of the test, titrate the sweep flow (0.5 - 1.0L/minute) to minimize carbon dioxide removal. It is also recommended to increase blood flow and/or sweep flow in the presence of hypoxemia and/or hypotension, which may be combined with fluid infusion and/or the escalation of inotropic/vasoactive drugs. If the partial pressure of carbon dioxide threshold is not reached, repeating the test under supplementation of carbon dioxide exogenous to the circuit is an alternative. Last, in cases of venoarterial extracorporeal membrane oxygenation, to measure gas variation and exclude differential hypoxia, blood samples of the native and extracorporeal (post-oxygenator) circulations are recommended.
Abstract
Rev Bras Ter Intensiva. 2017;29(4):476-480
DOI 10.5935/0103-507X.20170071
To evaluate the intra- and inter-reliability and the ease of measuring the quadriceps muscle thickness using bedside ultrasound.
This is a prospective, observational study. The assessment of quadriceps muscle thickness was performed at two reference points and was quantified using portable B-mode ultrasound in two healthy volunteers. For standardization of measurements and validation of image collections, the team was trained through theoretical and practical classes, with a 6-hour workload.
A total of 112 images were examined by the coach and compared with the trainees. Pearson's correlation analysis found an excellent relationship between the coach and all trainees (R2 > 0.90). The best association was between the coach and the dietitians (R2: 0.99; p < 0.001), and the worst association was between the coach and the medical trainees (R2: 0.92; p < 0.001). In the Bland-Altman comparison, the highest error rate found between coach and trainees was 5.12% (95% confidence interval [CI] 3.64-12.37), and the lowest was 1.01% (95%CI 0.72 - 2.58); the highest bias of the values described was -0.12 ± 0.19, and the lowest was -0.01 ± 0.04.
The data analyzed showed a good correlation between the measurements made by the coach and trainees, indicating that ultrasound of the quadriceps muscle is a viable and easily applicable tool.
Abstract
Rev Bras Ter Intensiva. 2017;29(4):476-480
DOI 10.5935/0103-507X.20170071
To evaluate the intra- and inter-reliability and the ease of measuring the quadriceps muscle thickness using bedside ultrasound.
This is a prospective, observational study. The assessment of quadriceps muscle thickness was performed at two reference points and was quantified using portable B-mode ultrasound in two healthy volunteers. For standardization of measurements and validation of image collections, the team was trained through theoretical and practical classes, with a 6-hour workload.
A total of 112 images were examined by the coach and compared with the trainees. Pearson's correlation analysis found an excellent relationship between the coach and all trainees (R2 > 0.90). The best association was between the coach and the dietitians (R2: 0.99; p < 0.001), and the worst association was between the coach and the medical trainees (R2: 0.92; p < 0.001). In the Bland-Altman comparison, the highest error rate found between coach and trainees was 5.12% (95% confidence interval [CI] 3.64-12.37), and the lowest was 1.01% (95%CI 0.72 - 2.58); the highest bias of the values described was -0.12 ± 0.19, and the lowest was -0.01 ± 0.04.
The data analyzed showed a good correlation between the measurements made by the coach and trainees, indicating that ultrasound of the quadriceps muscle is a viable and easily applicable tool.

Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (115) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)