Personal autonomy Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2019;31(3):386-392
DOI 10.5935/0103-507X.20190051
The improvement in cardiopulmonary resuscitation quality has reduced the mortality of individuals treated for cardiac arrest. However, survivors have a high risk of severe brain damage in cases of return of spontaneous circulation. Data suggest that cases of cardiac arrest in critically ill patients with non-shockable rhythms have only a 6% chance of returning of spontaneous circulation, and of these, only one-third recover their autonomy. Should we, therefore, opt for a procedure in which the chance of survival is minimal and the risk of hospital death or severe and definitive brain damage is approximately 70%? Is it worth discussing patient resuscitation in cases of cardiac arrest? Would this discussion bring any benefit to the patients and their family members? Advanced discussions on do-not-resuscitate are based on the ethical principle of respect for patient autonomy, as the wishes of family members and physicians often do not match those of patients. In addition to the issue of autonomy, advanced discussions can help the medical and care team anticipate future problems and, thus, better plan patient care. Our opinion is that discussions regarding the resuscitation of critically ill patients should be performed for all patients within the first 24 to 48 hours after admission to the intensive care unit.
Abstract
Rev Bras Ter Intensiva. 2019;31(3):386-392
DOI 10.5935/0103-507X.20190051
The improvement in cardiopulmonary resuscitation quality has reduced the mortality of individuals treated for cardiac arrest. However, survivors have a high risk of severe brain damage in cases of return of spontaneous circulation. Data suggest that cases of cardiac arrest in critically ill patients with non-shockable rhythms have only a 6% chance of returning of spontaneous circulation, and of these, only one-third recover their autonomy. Should we, therefore, opt for a procedure in which the chance of survival is minimal and the risk of hospital death or severe and definitive brain damage is approximately 70%? Is it worth discussing patient resuscitation in cases of cardiac arrest? Would this discussion bring any benefit to the patients and their family members? Advanced discussions on do-not-resuscitate are based on the ethical principle of respect for patient autonomy, as the wishes of family members and physicians often do not match those of patients. In addition to the issue of autonomy, advanced discussions can help the medical and care team anticipate future problems and, thus, better plan patient care. Our opinion is that discussions regarding the resuscitation of critically ill patients should be performed for all patients within the first 24 to 48 hours after admission to the intensive care unit.
Abstract
Rev Bras Ter Intensiva. 2013;25(2):93-98
DOI 10.5935/0103-507X.20130019
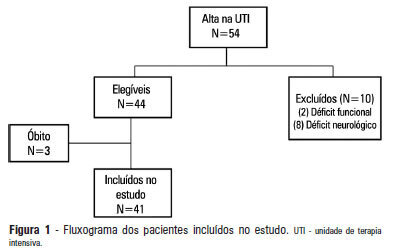
OBJECTIVE: 1) To evaluate the functional independence measures immediately after discharge from an intensive care unit and to compare these values with the FIMs 30 days after that period. 2) To evaluate the possible associated risk factors. METHODS: The present investigation was a prospective cohort study that included individuals who were discharged from the intensive care unit and underwent physiotherapy in the unit. Functional independence was evaluated using the functional independence measure immediately upon discharge from the intensive care unit and 30 days thereafter via a phone call. The patients were admitted to the Hospital Santa Clara intensive care unit during the period from May 2011 to August 2011. RESULTS: During the predetermined period of data collection, 44 patients met the criteria for inclusion in the study. The mean age of the patients was 55.4±10.5 years. Twenty-seven of the subjects were female, and 15 patients were admitted due to pulmonary disease. The patients exhibited an functional independence measure of 84.1±24.2. When this measure was compared to the measure at 30 days after discharge, there was improvement across the functional independence variables except for that concerned with sphincter control. There were no significant differences when comparing the gender, age, clinical diagnosis, length of stay in the intensive care unit, duration of mechanical ventilation, and the presence of sepsis during this period. CONCLUSION: Functional independence, as evaluated by the functional independence measure scale, was improved at 30 days after discharge from the intensive care unit, but it was not possible to define the potentially related factors.
Abstract
Rev Bras Ter Intensiva. 2013;25(2):93-98
DOI 10.5935/0103-507X.20130019
OBJECTIVE: 1) To evaluate the functional independence measures immediately after discharge from an intensive care unit and to compare these values with the FIMs 30 days after that period. 2) To evaluate the possible associated risk factors. METHODS: The present investigation was a prospective cohort study that included individuals who were discharged from the intensive care unit and underwent physiotherapy in the unit. Functional independence was evaluated using the functional independence measure immediately upon discharge from the intensive care unit and 30 days thereafter via a phone call. The patients were admitted to the Hospital Santa Clara intensive care unit during the period from May 2011 to August 2011. RESULTS: During the predetermined period of data collection, 44 patients met the criteria for inclusion in the study. The mean age of the patients was 55.4±10.5 years. Twenty-seven of the subjects were female, and 15 patients were admitted due to pulmonary disease. The patients exhibited an functional independence measure of 84.1±24.2. When this measure was compared to the measure at 30 days after discharge, there was improvement across the functional independence variables except for that concerned with sphincter control. There were no significant differences when comparing the gender, age, clinical diagnosis, length of stay in the intensive care unit, duration of mechanical ventilation, and the presence of sepsis during this period. CONCLUSION: Functional independence, as evaluated by the functional independence measure scale, was improved at 30 days after discharge from the intensive care unit, but it was not possible to define the potentially related factors.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (116) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)