Respiratory distress syndrome, newborn Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2019;31(3):312-317
DOI 10.5935/0103-507X.20190056
To investigate the influence of respiratory distress syndrome management on clinical and echocardiographic parameters used for hemodynamic evaluation in ≤ 32- week newborns.
Thirty-three ≤ 32-week newborns were prospectively evaluated and subjected to invasive mechanical ventilation. The need for exogenous surfactant and clinical and echocardiographic parameters in the first 24 hours of life was detailed in this group of patients.
The mean airway pressure was significantly higher in newborn infants who required inotropes [10.8 (8.8 - 23) cmH2O versus 9 (6.2 - 12) cmH2O; p = 0.04]. A negative correlation was found between the mean airway pressure and velocity-time integral of the pulmonary artery (r = -0.39; p = 0.026), right ventricular output (r = -0.43; p = 0.017) and measurements of the tricuspid annular plane excursion (r = -0.37; p = 0.036). A negative correlation was found between the number of doses of exogenous surfactant and the right ventricular output (r = -0.39; p = 0.028) and pulmonary artery velocity-time integral (r = -0.35; p = 0.043).
In ≤ 32-week newborns under invasive mechanical ventilation, increases in the mean airway pressure and number of surfactant doses are correlated with the worsening of early cardiac function. Therefore, more aggressive management of respiratory distress syndrome may contribute to the hemodynamic instability of these patients.
Abstract
Rev Bras Ter Intensiva. 2019;31(3):312-317
DOI 10.5935/0103-507X.20190056
To investigate the influence of respiratory distress syndrome management on clinical and echocardiographic parameters used for hemodynamic evaluation in ≤ 32- week newborns.
Thirty-three ≤ 32-week newborns were prospectively evaluated and subjected to invasive mechanical ventilation. The need for exogenous surfactant and clinical and echocardiographic parameters in the first 24 hours of life was detailed in this group of patients.
The mean airway pressure was significantly higher in newborn infants who required inotropes [10.8 (8.8 - 23) cmH2O versus 9 (6.2 - 12) cmH2O; p = 0.04]. A negative correlation was found between the mean airway pressure and velocity-time integral of the pulmonary artery (r = -0.39; p = 0.026), right ventricular output (r = -0.43; p = 0.017) and measurements of the tricuspid annular plane excursion (r = -0.37; p = 0.036). A negative correlation was found between the number of doses of exogenous surfactant and the right ventricular output (r = -0.39; p = 0.028) and pulmonary artery velocity-time integral (r = -0.35; p = 0.043).
In ≤ 32-week newborns under invasive mechanical ventilation, increases in the mean airway pressure and number of surfactant doses are correlated with the worsening of early cardiac function. Therefore, more aggressive management of respiratory distress syndrome may contribute to the hemodynamic instability of these patients.
Abstract
Rev Bras Ter Intensiva. 2012;24(2):207-210
DOI 10.1590/S0103-507X2012000200018
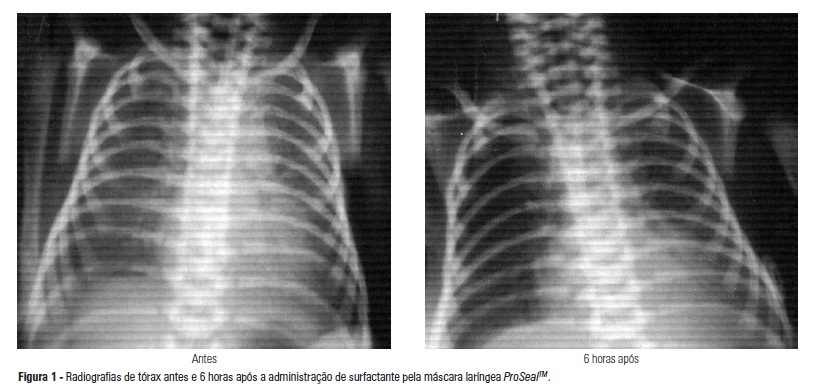
The administration of surfactant via tracheal cannula with mechanical ventilation is the conventional treatment for infant respiratory distress syndrome. Hemodynamic and respiratory changes due to tracheal intubation and the need for premedication justify the search for less invasive alternatives of surfactant administration. The objective of this study was to describe the use of the ProSealTM laryngeal mask airway as an option for the treatment of respiratory distress syndrome in a premature infant born at 31 weeks of gestation, at 1335 g, with respiratory difficulty after the first hour of life and exhibiting the clinical and radiologic features of respiratory distress syndrome. The surfactant was administered with the use of the ProSealTM laryngeal mask airway at 3.5 hours of life. It was well tolerated, with no need for tracheal intubation. Normal gasometry and radiologic improvement were observed after three and six hours of administration. Oxygen administration was suspended after eight days, with no comorbidities at discharge. The laryngeal mask airway seems to be a painless and less invasive alternative to treat respiratory distress syndrome and may reduce the need for tracheal intubation and mechanical ventilation. The efficacy and advantages of this route of treatment should be confirmed in a study of an adequate sample.
Abstract
Rev Bras Ter Intensiva. 2012;24(2):207-210
DOI 10.1590/S0103-507X2012000200018
The administration of surfactant via tracheal cannula with mechanical ventilation is the conventional treatment for infant respiratory distress syndrome. Hemodynamic and respiratory changes due to tracheal intubation and the need for premedication justify the search for less invasive alternatives of surfactant administration. The objective of this study was to describe the use of the ProSealTM laryngeal mask airway as an option for the treatment of respiratory distress syndrome in a premature infant born at 31 weeks of gestation, at 1335 g, with respiratory difficulty after the first hour of life and exhibiting the clinical and radiologic features of respiratory distress syndrome. The surfactant was administered with the use of the ProSealTM laryngeal mask airway at 3.5 hours of life. It was well tolerated, with no need for tracheal intubation. Normal gasometry and radiologic improvement were observed after three and six hours of administration. Oxygen administration was suspended after eight days, with no comorbidities at discharge. The laryngeal mask airway seems to be a painless and less invasive alternative to treat respiratory distress syndrome and may reduce the need for tracheal intubation and mechanical ventilation. The efficacy and advantages of this route of treatment should be confirmed in a study of an adequate sample.