-
Original Article
Oxygen delivery, carbon dioxide removal, energy transfer to lungs and pulmonary hypertension behavior during venous-venous extracorporeal membrane oxygenation support: a mathematical modeling approach
Rev Bras Ter Intensiva. 2019;31(2):113-121
Abstract
Original ArticleOxygen delivery, carbon dioxide removal, energy transfer to lungs and pulmonary hypertension behavior during venous-venous extracorporeal membrane oxygenation support: a mathematical modeling approach
Rev Bras Ter Intensiva. 2019;31(2):113-121
DOI 10.5935/0103-507X.20190018
Views0ABSTRACT
Objective:
To describe (1) the energy transfer from the ventilator to the lungs, (2) the match between venous-venous extracorporeal membrane oxygenation (ECMO) oxygen transfer and patient oxygen consumption (VO2), (3) carbon dioxide removal with ECMO, and (4) the potential effect of systemic venous oxygenation on pulmonary artery pressure.
Methods:
Mathematical modeling approach with hypothetical scenarios using computer simulation.
Results:
The transition from protective ventilation to ultraprotective ventilation in a patient with severe acute respiratory distress syndrome and a static respiratory compliance of 20mL/cm H2O reduced the energy transfer from the ventilator to the lungs from 35.3 to 2.6 joules/minute. A hypothetical patient, hyperdynamic and slightly anemic with VO2 = 200mL/minute, can reach an arterial oxygen saturation of 80%, while maintaining the match between the oxygen transfer by ECMO and the VO2 of the patient. Carbon dioxide is easily removed, and normal PaCO2 is easily reached. Venous blood oxygenation through the ECMO circuit may drive the PO2 stimulus of pulmonary hypoxic vasoconstriction to normal values.
Conclusion:
Ultraprotective ventilation largely reduces the energy transfer from the ventilator to the lungs. Severe hypoxemia on venous-venous-ECMO support may occur despite the matching between the oxygen transfer by ECMO and the VO2 of the patient. The normal range of PaCO2 is easy to reach. Venous-venous-ECMO support potentially relieves hypoxic pulmonary vasoconstriction.
Keywords:acute respiratory distress syndromeExtracorporeal membrane oxygenationIntensive Care UnitMathematical modelmechanical ventilationrespiratory failureSee moreViews0

Abstract
Original ArticleOxygen delivery, carbon dioxide removal, energy transfer to lungs and pulmonary hypertension behavior during venous-venous extracorporeal membrane oxygenation support: a mathematical modeling approach
Rev Bras Ter Intensiva. 2019;31(2):113-121
DOI 10.5935/0103-507X.20190018
Views0ABSTRACT
Objective:
To describe (1) the energy transfer from the ventilator to the lungs, (2) the match between venous-venous extracorporeal membrane oxygenation (ECMO) oxygen transfer and patient oxygen consumption (VO2), (3) carbon dioxide removal with ECMO, and (4) the potential effect of systemic venous oxygenation on pulmonary artery pressure.
Methods:
Mathematical modeling approach with hypothetical scenarios using computer simulation.
Results:
The transition from protective ventilation to ultraprotective ventilation in a patient with severe acute respiratory distress syndrome and a static respiratory compliance of 20mL/cm H2O reduced the energy transfer from the ventilator to the lungs from 35.3 to 2.6 joules/minute. A hypothetical patient, hyperdynamic and slightly anemic with VO2 = 200mL/minute, can reach an arterial oxygen saturation of 80%, while maintaining the match between the oxygen transfer by ECMO and the VO2 of the patient. Carbon dioxide is easily removed, and normal PaCO2 is easily reached. Venous blood oxygenation through the ECMO circuit may drive the PO2 stimulus of pulmonary hypoxic vasoconstriction to normal values.
Conclusion:
Ultraprotective ventilation largely reduces the energy transfer from the ventilator to the lungs. Severe hypoxemia on venous-venous-ECMO support may occur despite the matching between the oxygen transfer by ECMO and the VO2 of the patient. The normal range of PaCO2 is easy to reach. Venous-venous-ECMO support potentially relieves hypoxic pulmonary vasoconstriction.
Keywords:acute respiratory distress syndromeExtracorporeal membrane oxygenationIntensive Care UnitMathematical modelmechanical ventilationrespiratory failureSee more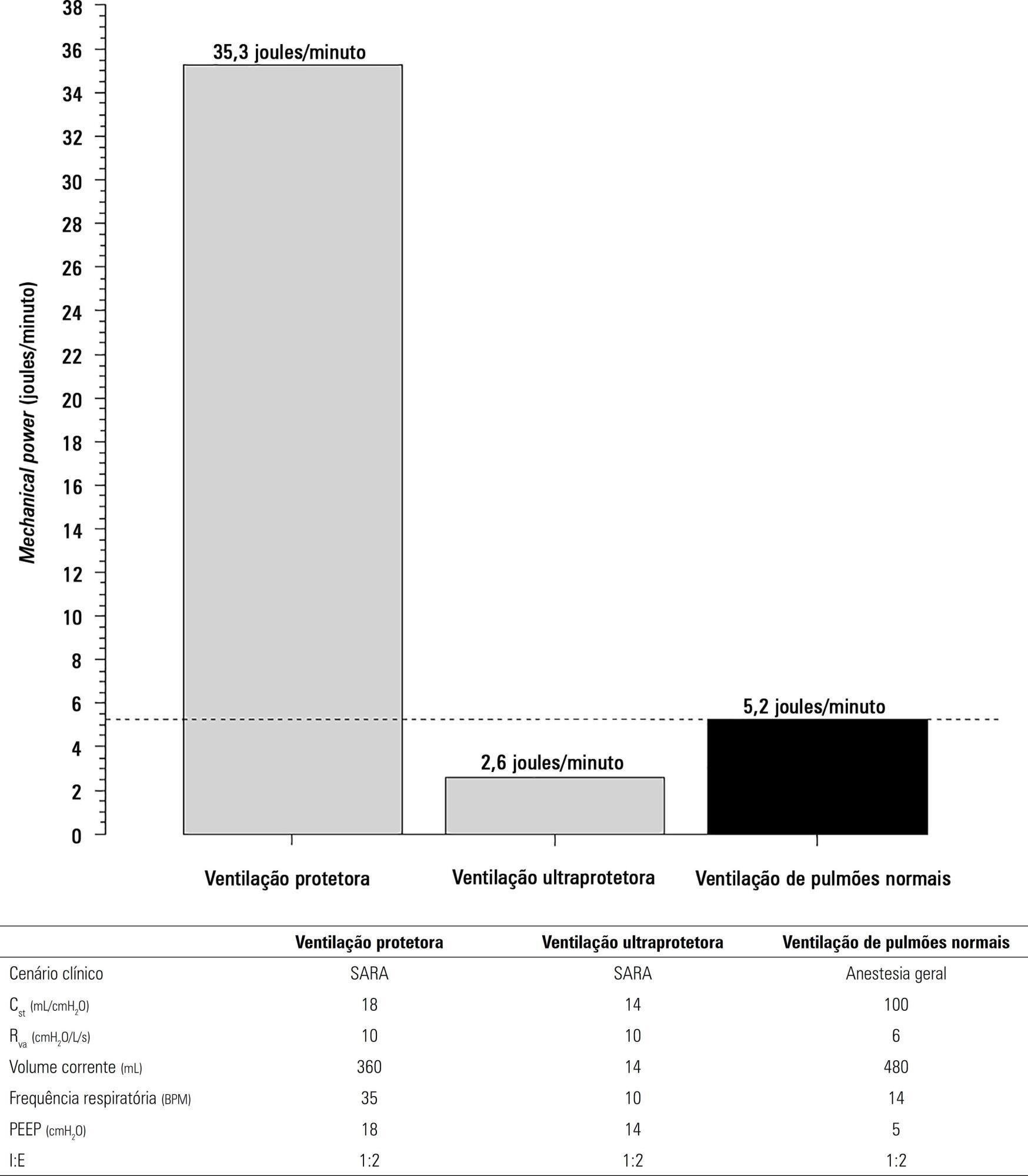
-
Original Article
Hidden hospital mortality in patients with sepsis discharged from the intensive care unit
Rev Bras Ter Intensiva. 2019;31(2):122-128
Abstract
Original ArticleHidden hospital mortality in patients with sepsis discharged from the intensive care unit
Rev Bras Ter Intensiva. 2019;31(2):122-128
DOI 10.5935/0103-507X.20190037
Views1See moreABSTRACT
Objective:
To evaluate the impact of the presence of sepsis on in-hospital mortality after intensive care unit discharge.
Methods:
Retrospective, observational, single-center study. All consecutive patients discharged alive from the intensive care unit of Hospital Vila Franca de Xira (Portugal) from January 1 to December 31, 2015 (N = 473) were included and followed until death or hospital discharge. In-hospital mortality after intensive care unit discharge was calculated for septic and non-septic patients.
Results:
A total of 61 patients (12.9%) died in the hospital after being discharged alive from the intensive care unit. This rate was higher among the patients with sepsis on admission, 21.4%, whereas the in-hospital, post-intensive care unit mortality rate for the remaining patients was nearly half that, 9.3% (p < 0.001). Other patient characteristics associated with mortality were advanced age (p = 0.02), male sex (p < 0.001), lower body mass index (p = 0.02), end-stage renal disease (p = 0.04) and high Simplified Acute Physiology Score II (SAPS II) at intensive care unit admission (p < 0.001), the presence of shock (p < 0.001) and medical admission (p < 0.001). We developed a logistic regression model and identified the independent predictors of in-hospital mortality after intensive care unit discharge.
Conclusion:
Admission to the intensive care unit with a sepsis diagnosis is associated with an increased risk of dying in the hospital, not only in the intensive care unit but also after resolution of the acute process and discharge from the intensive care unit.
Views1Abstract
Original ArticleHidden hospital mortality in patients with sepsis discharged from the intensive care unit
Rev Bras Ter Intensiva. 2019;31(2):122-128
DOI 10.5935/0103-507X.20190037
Views1See moreABSTRACT
Objective:
To evaluate the impact of the presence of sepsis on in-hospital mortality after intensive care unit discharge.
Methods:
Retrospective, observational, single-center study. All consecutive patients discharged alive from the intensive care unit of Hospital Vila Franca de Xira (Portugal) from January 1 to December 31, 2015 (N = 473) were included and followed until death or hospital discharge. In-hospital mortality after intensive care unit discharge was calculated for septic and non-septic patients.
Results:
A total of 61 patients (12.9%) died in the hospital after being discharged alive from the intensive care unit. This rate was higher among the patients with sepsis on admission, 21.4%, whereas the in-hospital, post-intensive care unit mortality rate for the remaining patients was nearly half that, 9.3% (p < 0.001). Other patient characteristics associated with mortality were advanced age (p = 0.02), male sex (p < 0.001), lower body mass index (p = 0.02), end-stage renal disease (p = 0.04) and high Simplified Acute Physiology Score II (SAPS II) at intensive care unit admission (p < 0.001), the presence of shock (p < 0.001) and medical admission (p < 0.001). We developed a logistic regression model and identified the independent predictors of in-hospital mortality after intensive care unit discharge.
Conclusion:
Admission to the intensive care unit with a sepsis diagnosis is associated with an increased risk of dying in the hospital, not only in the intensive care unit but also after resolution of the acute process and discharge from the intensive care unit.
-
Original Article
Clinical and epidemiological characteristics of whooping cough in hospitalized patients of a tertiary care hospital in Peru
Rev Bras Ter Intensiva. 2019;31(2):129-137
Abstract
Original ArticleClinical and epidemiological characteristics of whooping cough in hospitalized patients of a tertiary care hospital in Peru
Rev Bras Ter Intensiva. 2019;31(2):129-137
DOI 10.5935/0103-507X.20190029
Views0See moreABSTRACT
Objective:
Describe the clinical and epidemiological characteristics of patients under 2 years of age hospitalized with whooping cough in a tertiary care children’s hospital in Peru.
Methods:
This was a case series of patients under 2 years of age who were hospitalized with a diagnosis of whooping cough in 2012.
Results:
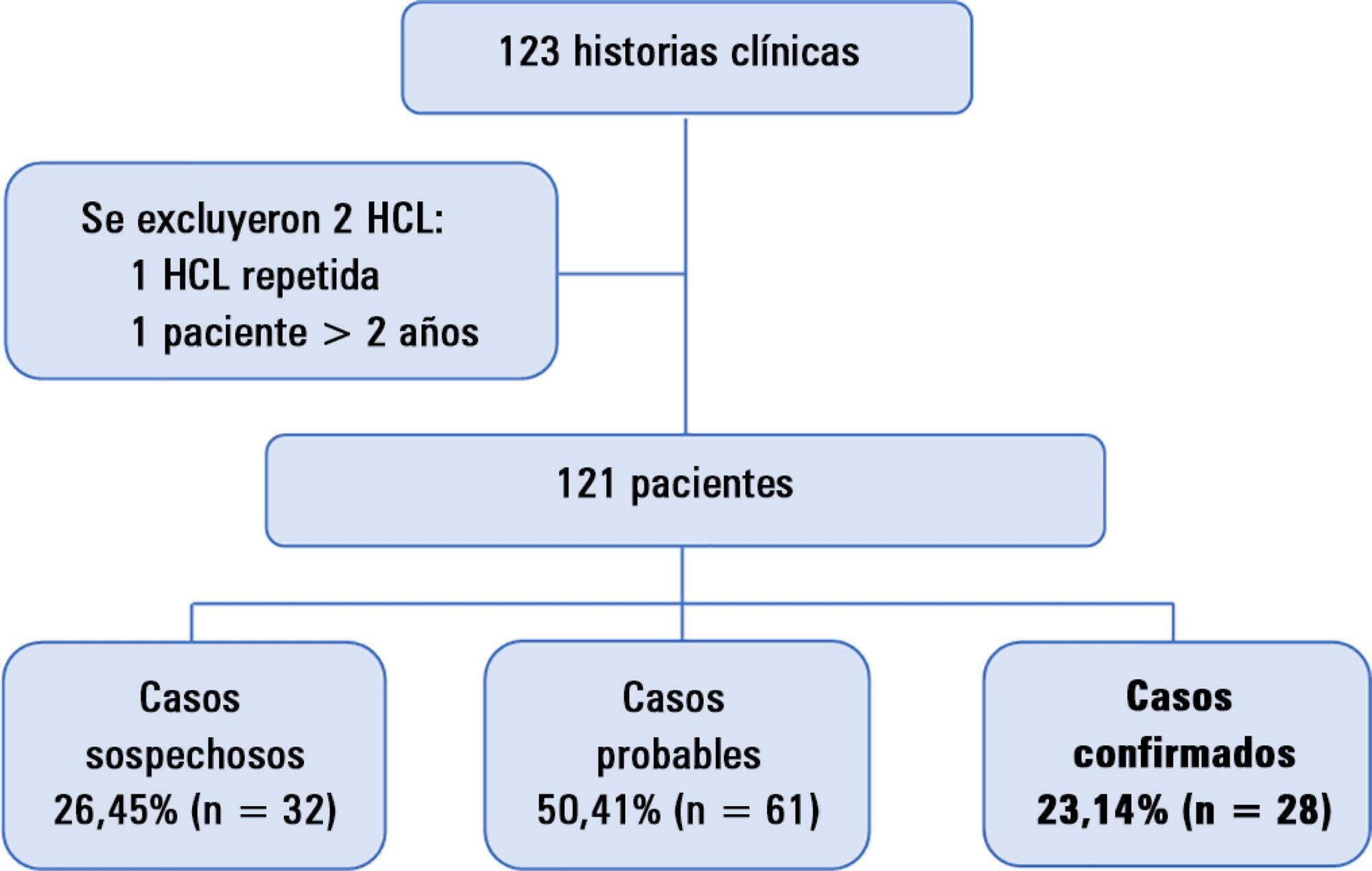
A total of 121 patients were hospitalized. Diagnostic testing (direct immunofluorescence, polymerase chain reaction, culture) was carried out in 53.72% of patients. Overall, 23.15% (n = 28) were confirmed cases, all of whom were patients less than 10 months old, and none of whom had received 3 doses of whooping cough vaccine. A total of 96.43% (n = 27) of cases were under 6 months of age, 42.86% (n = 12) were younger than 3 months, and 10.71% (n = 3) were admitted to the intensive care unit. Of these cases, all were younger than 2 months old, and one patient died. The most common symptoms in the confirmed cases were coughing (96.43%), facial redness (96.43%), paroxysmal coughing (92.86%), and coughing-related cyanosis (78.57%). The most frequent probable epidemiological contact was the mother (17.86%), and the majority of cases occurred in the summer (46.43%).
Conclusion:
Whooping cough is a cause of morbidity and mortality, especially in those younger than 6 months of age and in those who are not immunized or only partially immunized. Vaccination rates should be improved and case confirmation encouraged to prevent the underdiagnosis of this disease.
Views0Abstract
Original ArticleClinical and epidemiological characteristics of whooping cough in hospitalized patients of a tertiary care hospital in Peru
Rev Bras Ter Intensiva. 2019;31(2):129-137
DOI 10.5935/0103-507X.20190029
Views0See moreABSTRACT
Objective:
Describe the clinical and epidemiological characteristics of patients under 2 years of age hospitalized with whooping cough in a tertiary care children’s hospital in Peru.
Methods:
This was a case series of patients under 2 years of age who were hospitalized with a diagnosis of whooping cough in 2012.
Results:
A total of 121 patients were hospitalized. Diagnostic testing (direct immunofluorescence, polymerase chain reaction, culture) was carried out in 53.72% of patients. Overall, 23.15% (n = 28) were confirmed cases, all of whom were patients less than 10 months old, and none of whom had received 3 doses of whooping cough vaccine. A total of 96.43% (n = 27) of cases were under 6 months of age, 42.86% (n = 12) were younger than 3 months, and 10.71% (n = 3) were admitted to the intensive care unit. Of these cases, all were younger than 2 months old, and one patient died. The most common symptoms in the confirmed cases were coughing (96.43%), facial redness (96.43%), paroxysmal coughing (92.86%), and coughing-related cyanosis (78.57%). The most frequent probable epidemiological contact was the mother (17.86%), and the majority of cases occurred in the summer (46.43%).
Conclusion:
Whooping cough is a cause of morbidity and mortality, especially in those younger than 6 months of age and in those who are not immunized or only partially immunized. Vaccination rates should be improved and case confirmation encouraged to prevent the underdiagnosis of this disease.
-
Original Article
Quality assessment of adult intensive care services: application of a tool adjusted to the reality of low-income countries
Rev Bras Ter Intensiva. 2019;31(2):138-146
Abstract
Original ArticleQuality assessment of adult intensive care services: application of a tool adjusted to the reality of low-income countries
Rev Bras Ter Intensiva. 2019;31(2):138-146
DOI 10.5935/0103-507X.20190031
Views1See moreABSTRACT
Objective:
To assess the quality of adult intensive care units.
Methods:
This population-based, cross-sectional, observational, analytical study evaluated management type in Maranhão, Brazil. An assessment instrument was applied that assigned scores to each service (maximum 124 points). The units were categorized as insufficient (< 50% of the maximum score), typical (≥ 50% and <80% of the maximum score), or sufficient (≥ 80% of the maximum score).
Results:
Of the 26 intensive care units in Maranhão, 23 were evaluated; 15 (65.2%) were located in the state capital, and 14 (60.9%) were public. The mean final score was 67.2 (54.2% of the maximum). The worst performance was observed with regard to processes (50.9%) in the units located outside the capital (p = 0.037) and for hospitals with 68 beds or fewer (p = 0.027). The result of the assessment categorized services as a function of the overall total points earned. Specifically, 8 (34.8%) services were assessed as insufficient, 13 (56.5%) were assessed as typical, and 2 (8.7%) were assessed as sufficient.
Conclusion:
The majority of the intensive care units in this study were assessed as typical. These services must be better qualified. The priorities are the processes of the units located outside the capital and in small hospitals.
Views1Abstract
Original ArticleQuality assessment of adult intensive care services: application of a tool adjusted to the reality of low-income countries
Rev Bras Ter Intensiva. 2019;31(2):138-146
DOI 10.5935/0103-507X.20190031
Views1See moreABSTRACT
Objective:
To assess the quality of adult intensive care units.
Methods:
This population-based, cross-sectional, observational, analytical study evaluated management type in Maranhão, Brazil. An assessment instrument was applied that assigned scores to each service (maximum 124 points). The units were categorized as insufficient (< 50% of the maximum score), typical (≥ 50% and <80% of the maximum score), or sufficient (≥ 80% of the maximum score).
Results:
Of the 26 intensive care units in Maranhão, 23 were evaluated; 15 (65.2%) were located in the state capital, and 14 (60.9%) were public. The mean final score was 67.2 (54.2% of the maximum). The worst performance was observed with regard to processes (50.9%) in the units located outside the capital (p = 0.037) and for hospitals with 68 beds or fewer (p = 0.027). The result of the assessment categorized services as a function of the overall total points earned. Specifically, 8 (34.8%) services were assessed as insufficient, 13 (56.5%) were assessed as typical, and 2 (8.7%) were assessed as sufficient.
Conclusion:
The majority of the intensive care units in this study were assessed as typical. These services must be better qualified. The priorities are the processes of the units located outside the capital and in small hospitals.
-
Original Article
Satisfaction of family members of critically ill patients admitted to a public hospital intensive care unit and correlated factors
Rev Bras Ter Intensiva. 2019;31(2):147-155
Abstract
Original ArticleSatisfaction of family members of critically ill patients admitted to a public hospital intensive care unit and correlated factors
Rev Bras Ter Intensiva. 2019;31(2):147-155
DOI 10.5935/0103-507X.20190024
Views1See moreABSTRACT
Objective:
To analyze the satisfaction, medical situation understanding and symptoms of anxiety and depression in family members of patients admitted to the intensive care unit.
Methods:
The family members of patients who were hospitalized for ≥ 72 hours were invited to participate in the study, which was performed in a public hospital. Questionnaires were answered to assess the understanding of the diagnosis, treatment and prognosis, and the support received in the intensive care unit. The family needs were also evaluated using a modified version of the Critical Care Family Needs Inventory (CCFNI). The Hospital Anxiety and Depression Scale (HADS) was used to assess the symptoms of anxiety and depression.
Results:
A total of 35 family members were interviewed within the patients’ first week of stay in the intensive care unit. Most patients (57.1%) were male, aged 54 ± 19 years. Sepsis was the main reason for admission to the intensive care unit (40%); the median of the Simplified Acute Physiology Score (SAPS) 3 was 68 (48 – 77), and 51.4% of the patients died in the intensive care unit. The majority of the family members were female (74.3%) and were sons or daughters of patients (54.3%), with a mean age of 43.2 ± 14 years. Overall, 77.1% of the family members were satisfied with the intensive care unit. A total of 37.1% of the family members did not understand the prognosis. Receiving clear and complete information in the intensive care unit and the doctor being accessible were factors that were significantly correlated with the overall family satisfaction. The prevalence of symptoms of anxiety (60%) and depression (54.3%) in the family members was high.
Conclusion:
The emotional distress of family members is high during a patient’s hospitalization in the intensive care unit, although satisfaction is also high. Clear and complete information provided by the intensivist and the support received in the intensive care unit are significantly correlated with the satisfaction of family members in a public hospital.
Views1Abstract
Original ArticleSatisfaction of family members of critically ill patients admitted to a public hospital intensive care unit and correlated factors
Rev Bras Ter Intensiva. 2019;31(2):147-155
DOI 10.5935/0103-507X.20190024
Views1See moreABSTRACT
Objective:
To analyze the satisfaction, medical situation understanding and symptoms of anxiety and depression in family members of patients admitted to the intensive care unit.
Methods:
The family members of patients who were hospitalized for ≥ 72 hours were invited to participate in the study, which was performed in a public hospital. Questionnaires were answered to assess the understanding of the diagnosis, treatment and prognosis, and the support received in the intensive care unit. The family needs were also evaluated using a modified version of the Critical Care Family Needs Inventory (CCFNI). The Hospital Anxiety and Depression Scale (HADS) was used to assess the symptoms of anxiety and depression.
Results:
A total of 35 family members were interviewed within the patients’ first week of stay in the intensive care unit. Most patients (57.1%) were male, aged 54 ± 19 years. Sepsis was the main reason for admission to the intensive care unit (40%); the median of the Simplified Acute Physiology Score (SAPS) 3 was 68 (48 – 77), and 51.4% of the patients died in the intensive care unit. The majority of the family members were female (74.3%) and were sons or daughters of patients (54.3%), with a mean age of 43.2 ± 14 years. Overall, 77.1% of the family members were satisfied with the intensive care unit. A total of 37.1% of the family members did not understand the prognosis. Receiving clear and complete information in the intensive care unit and the doctor being accessible were factors that were significantly correlated with the overall family satisfaction. The prevalence of symptoms of anxiety (60%) and depression (54.3%) in the family members was high.
Conclusion:
The emotional distress of family members is high during a patient’s hospitalization in the intensive care unit, although satisfaction is also high. Clear and complete information provided by the intensivist and the support received in the intensive care unit are significantly correlated with the satisfaction of family members in a public hospital.
-
Original Article
Efficacy and safety of high-flow nasal cannula oxygen therapy in moderate acute hypercapnic respiratory failure
Rev Bras Ter Intensiva. 2019;31(2):156-163
Abstract
Original ArticleEfficacy and safety of high-flow nasal cannula oxygen therapy in moderate acute hypercapnic respiratory failure
Rev Bras Ter Intensiva. 2019;31(2):156-163
DOI 10.5935/0103-507X.20190026
Views1ABSTRACT
Objective:
To assess the efficacy and safety of high-flow nasal cannula oxygen therapy in treating moderate hypercapnic respiratory failure in patients who cannot tolerate or have contraindications to noninvasive mechanical ventilation.
Methods:
A prospective observational 13-month study involving subjects admitted to an intensive care unit with or developing moderate hypercapnic respiratory failure. Clinical and gas exchange parameters were recorded at regular intervals during the first 24 hours. The endpoints were a oxygen saturation between 88 and 92% along with a reduction in breathing effort (respiratory rate) and pH normalization (≥ 7.35). Subjects were considered nonresponders if they required ventilatory support.
Results:
Thirty subjects were treated with high-flow nasal cannula oxygen therapy. They consisted of a mixed population with chronic obstructive pulmonary disease exacerbation, acute cardiogenic pulmonary edema, and postoperative and postextubation respiratory failure. A nonsignificant improvement was observed in respiratory rate (28.0 ± 0.9 versus 24.3 ± 1.5, p = 0.22), which was apparent in the first four hours of treatment. The pH improved, although normal levels were only reached after 24 hours on high-flow nasal cannula therapy (7.28 ± 0.02 versus 7.37 ± 0.01, p = 0.02). The rate of nonresponders was 13.3% (4 subjects), of whom one needed and accepted noninvasive mechanical ventilation and three required intubation. Intensive care unit mortality was 3.3% (1 subject), and a patient died after discharge to the ward (hospital mortality of 6.6%).
Conclusion:
High-flow nasal cannula oxygen therapy is effective for moderate hypercapnic respiratory failure as it helps normalize clinical and gas exchange levels with an acceptable rate of nonresponders who require ventilatory support.
Keywords:Cannula/utilizationIntensive care unitsOxygen inhalation therapy/methodsOxygen/therapeutic useRespiration, artificialRespiratory insufficiency/therapySee moreViews1Abstract
Original ArticleEfficacy and safety of high-flow nasal cannula oxygen therapy in moderate acute hypercapnic respiratory failure
Rev Bras Ter Intensiva. 2019;31(2):156-163
DOI 10.5935/0103-507X.20190026
Views1ABSTRACT
Objective:
To assess the efficacy and safety of high-flow nasal cannula oxygen therapy in treating moderate hypercapnic respiratory failure in patients who cannot tolerate or have contraindications to noninvasive mechanical ventilation.
Methods:
A prospective observational 13-month study involving subjects admitted to an intensive care unit with or developing moderate hypercapnic respiratory failure. Clinical and gas exchange parameters were recorded at regular intervals during the first 24 hours. The endpoints were a oxygen saturation between 88 and 92% along with a reduction in breathing effort (respiratory rate) and pH normalization (≥ 7.35). Subjects were considered nonresponders if they required ventilatory support.
Results:
Thirty subjects were treated with high-flow nasal cannula oxygen therapy. They consisted of a mixed population with chronic obstructive pulmonary disease exacerbation, acute cardiogenic pulmonary edema, and postoperative and postextubation respiratory failure. A nonsignificant improvement was observed in respiratory rate (28.0 ± 0.9 versus 24.3 ± 1.5, p = 0.22), which was apparent in the first four hours of treatment. The pH improved, although normal levels were only reached after 24 hours on high-flow nasal cannula therapy (7.28 ± 0.02 versus 7.37 ± 0.01, p = 0.02). The rate of nonresponders was 13.3% (4 subjects), of whom one needed and accepted noninvasive mechanical ventilation and three required intubation. Intensive care unit mortality was 3.3% (1 subject), and a patient died after discharge to the ward (hospital mortality of 6.6%).
Conclusion:
High-flow nasal cannula oxygen therapy is effective for moderate hypercapnic respiratory failure as it helps normalize clinical and gas exchange levels with an acceptable rate of nonresponders who require ventilatory support.
Keywords:Cannula/utilizationIntensive care unitsOxygen inhalation therapy/methodsOxygen/therapeutic useRespiration, artificialRespiratory insufficiency/therapySee more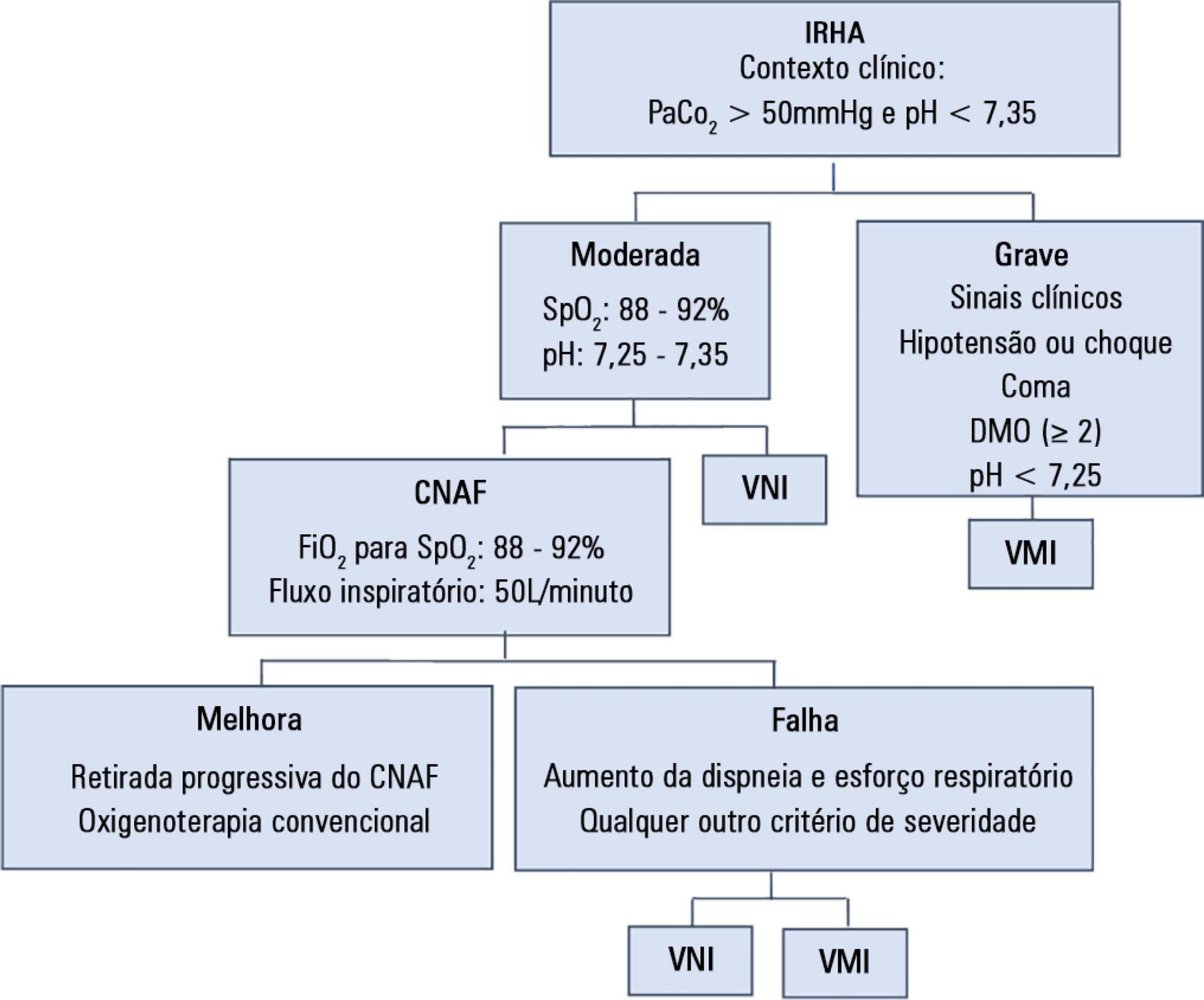
-
Original Article
Assessment of patient satisfaction and preferences with an intensive care diary
Rev Bras Ter Intensiva. 2019;31(2):164-170
Abstract
Original ArticleAssessment of patient satisfaction and preferences with an intensive care diary
Rev Bras Ter Intensiva. 2019;31(2):164-170
DOI 10.5935/0103-507X.20190028
Views0See moreABSTRACT
Objectives:
To evaluate the satisfaction of patients admitted to the intensive care unit using a diary and analyze possible points for improving this instrument.
Methods:
This was an observational, retrospective study, conducted between March 2014 and July 2017, in a multidisciplinary intensive care unit of a district hospital. The diary was implemented in patients sedated for 3 or more days. Three months after discharge, their satisfaction was assessed using a questionnaire. A patient who agreed with the 5 statements assessing the diary’s help in clarifying the intensive care unit stay, in filling memory gaps, in recovery, in reassurance, and in the recommendation of this intervention was defined as satisfied.
Results:
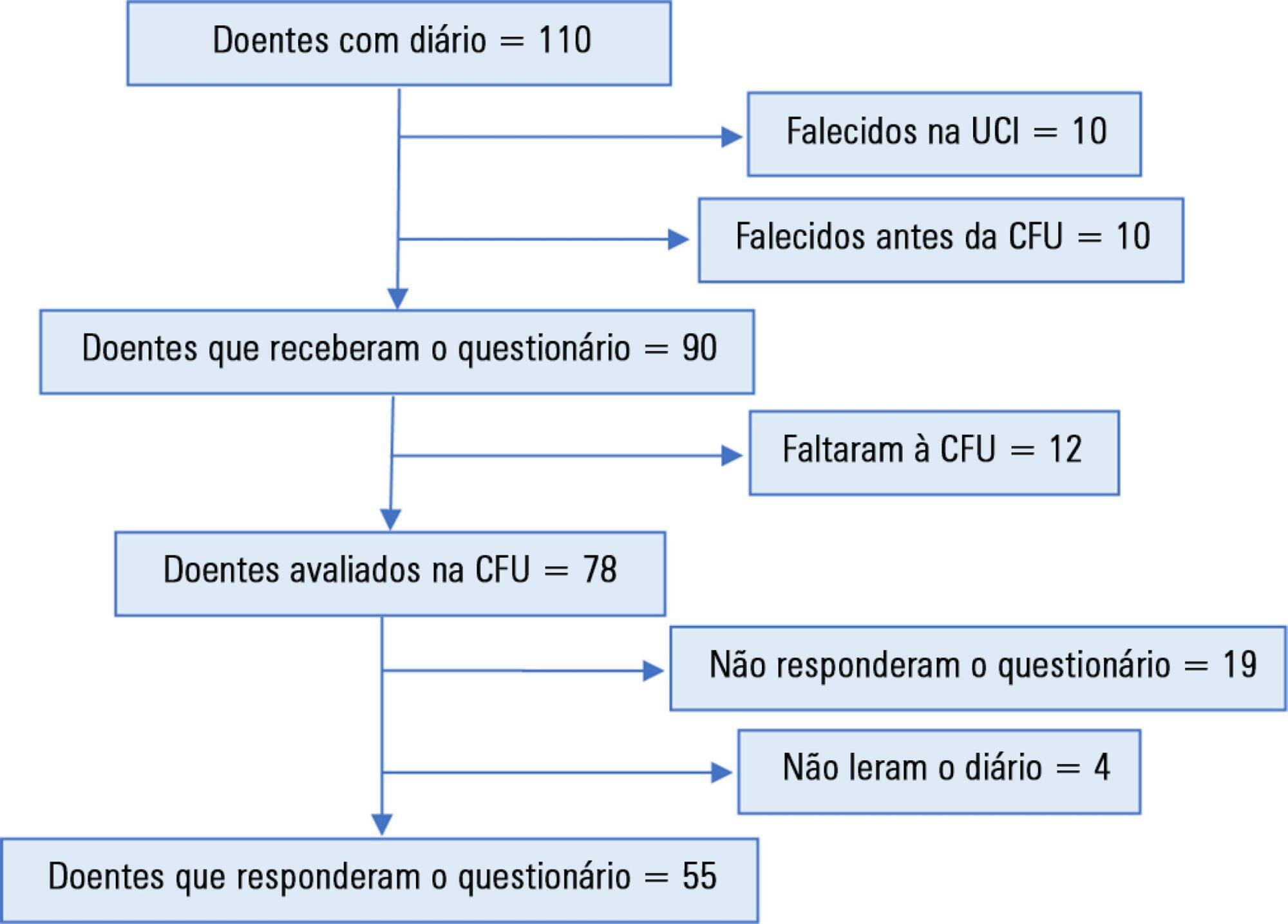
A total of 110 patients were included, of whom 55 answered the questionnaire. Of these, 36 (65.5%) were classified as satisfied. Each item had a positive response in more than 74% of cases. A total of 60% of the participants suggested increasing the number of photographs. No significant differences were found in the subgroup analysis (age, sex, duration of sedation and ventilation, length of diary keeping, severity on admission, or delirium, depression, or anxiety in the intensive care unit).
Conclusions:
Most patients were satisfied with the diary but suggested an increase in the number of photographs.
Views0Abstract
Original ArticleAssessment of patient satisfaction and preferences with an intensive care diary
Rev Bras Ter Intensiva. 2019;31(2):164-170
DOI 10.5935/0103-507X.20190028
Views0See moreABSTRACT
Objectives:
To evaluate the satisfaction of patients admitted to the intensive care unit using a diary and analyze possible points for improving this instrument.
Methods:
This was an observational, retrospective study, conducted between March 2014 and July 2017, in a multidisciplinary intensive care unit of a district hospital. The diary was implemented in patients sedated for 3 or more days. Three months after discharge, their satisfaction was assessed using a questionnaire. A patient who agreed with the 5 statements assessing the diary’s help in clarifying the intensive care unit stay, in filling memory gaps, in recovery, in reassurance, and in the recommendation of this intervention was defined as satisfied.
Results:
A total of 110 patients were included, of whom 55 answered the questionnaire. Of these, 36 (65.5%) were classified as satisfied. Each item had a positive response in more than 74% of cases. A total of 60% of the participants suggested increasing the number of photographs. No significant differences were found in the subgroup analysis (age, sex, duration of sedation and ventilation, length of diary keeping, severity on admission, or delirium, depression, or anxiety in the intensive care unit).
Conclusions:
Most patients were satisfied with the diary but suggested an increase in the number of photographs.
-
Original Article
Optimized calorie and high protein intake versus recommended caloric-protein intake in critically ill patients: a prospective, randomized, controlled phase II clinical trial
Rev Bras Ter Intensiva. 2019;31(2):171-179
Abstract
Original ArticleOptimized calorie and high protein intake versus recommended caloric-protein intake in critically ill patients: a prospective, randomized, controlled phase II clinical trial
Rev Bras Ter Intensiva. 2019;31(2):171-179
DOI 10.5935/0103-507X.20190025
Views0See moreABSTRACT
Objective:
To evaluate differences in outcomes for an optimized calorie and high protein nutrition therapy versus standard nutrition care in critically ill adult patients.
Methods:
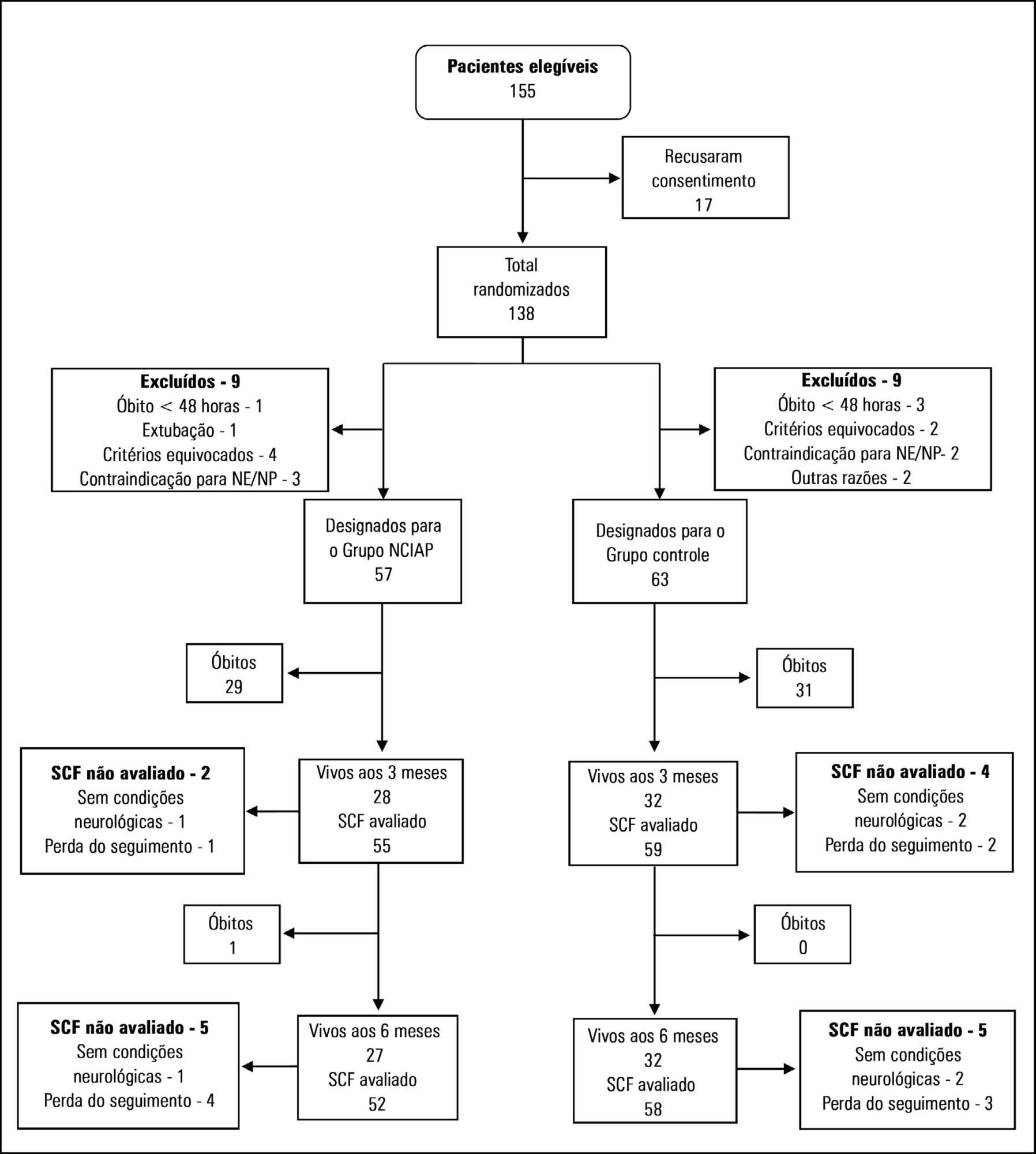
We randomized patients expected to stay in the intensive care unit for at least 3 days. In the optimized calorie and high protein nutrition group, caloric intake was determined by indirect calorimetry, and protein intake was established at 2.0 to 2.2g/kg/day. The control group received 25kcal/kg/day of calories and 1.4 to 1.5g/kg/day protein. The primary outcome was the physical component summary score obtained at 3 and 6 months. Secondary outcomes included handgrip strength at intensive care unit discharge, duration of mechanical ventilation and hospital mortality.
Results:
In total, 120 patients were included in the analysis. There was no significant difference between the two groups in calories received. However, the amount of protein received by the optimized calorie and high protein nutrition group was significantly higher compared with the control group. The physical component summary score at 3 and 6 months did not differ between the two groups nor did secondary outcomes. However, after adjusting for covariates, a negative delta protein (protein received minus predetermined protein requirement) was associated with a lower physical component summary score at 3 and 6 months postrandomization.
Conclusion:
In this study optimized calorie and high protein strategy did not appear to improve physical quality of life compared with standard nutrition care. However, after adjusting for covariates, a negative delta protein was associated with a lower physical component summary score at 3 and 6 months postrandomization. This association exists independently of the method of calculation of protein target.
Views0Abstract
Original ArticleOptimized calorie and high protein intake versus recommended caloric-protein intake in critically ill patients: a prospective, randomized, controlled phase II clinical trial
Rev Bras Ter Intensiva. 2019;31(2):171-179
DOI 10.5935/0103-507X.20190025
Views0See moreABSTRACT
Objective:
To evaluate differences in outcomes for an optimized calorie and high protein nutrition therapy versus standard nutrition care in critically ill adult patients.
Methods:
We randomized patients expected to stay in the intensive care unit for at least 3 days. In the optimized calorie and high protein nutrition group, caloric intake was determined by indirect calorimetry, and protein intake was established at 2.0 to 2.2g/kg/day. The control group received 25kcal/kg/day of calories and 1.4 to 1.5g/kg/day protein. The primary outcome was the physical component summary score obtained at 3 and 6 months. Secondary outcomes included handgrip strength at intensive care unit discharge, duration of mechanical ventilation and hospital mortality.
Results:
In total, 120 patients were included in the analysis. There was no significant difference between the two groups in calories received. However, the amount of protein received by the optimized calorie and high protein nutrition group was significantly higher compared with the control group. The physical component summary score at 3 and 6 months did not differ between the two groups nor did secondary outcomes. However, after adjusting for covariates, a negative delta protein (protein received minus predetermined protein requirement) was associated with a lower physical component summary score at 3 and 6 months postrandomization.
Conclusion:
In this study optimized calorie and high protein strategy did not appear to improve physical quality of life compared with standard nutrition care. However, after adjusting for covariates, a negative delta protein was associated with a lower physical component summary score at 3 and 6 months postrandomization. This association exists independently of the method of calculation of protein target.
-
Original Article
Survey on the extubation procedure in intensive care units in Buenos Aires, Argentina
Rev Bras Ter Intensiva. 2019;31(2):180-185
Abstract
Original ArticleSurvey on the extubation procedure in intensive care units in Buenos Aires, Argentina
Rev Bras Ter Intensiva. 2019;31(2):180-185
DOI 10.5935/0103-507X.20190027
Views0ABSTRACT
Objective:
To examine the usual practice of airway management during the extubation procedure through an online survey to professionals working in intensive care units in the Autonomous City of Buenos Aires and in the Province of Buenos Aires, Argentina.
Methods:
A cross-sectional descriptive study online survey was conducted from February 11 to March 11, 2013. A database was generated, and a voluntary and anonymous invitation to access the survey was sent by email to 500 participants.
Results:
Out of a total of 500 participants, 217 (44%) responded to the survey, of whom 59.4% were physical therapists. One hundred ninety-five (89.9%) professionals were working in adult care. Regarding the cuff deflation procedure and extubation, 203 (93.5%) performe endotracheal suctioning, and 27 (12.5%) use positive pressure. Approximately 53.5% of participants reported having experienced immediate complications with this procedure in the last three months. In all, 163 complications were reported, and stridor was the most prevalent (52.7%).
Conclusion:
Most professionals working in intensive care units in the Autonomous City of Buenos Aires and in the Province of Buenos Aires, Argentina, use endotracheal suctioning without applying positive pressure during extubation.
Keywords:Airway extubation/adverse effectsIntermittent positive-pressure ventilationSurvey and questionnairesSee moreViews0Abstract
Original ArticleSurvey on the extubation procedure in intensive care units in Buenos Aires, Argentina
Rev Bras Ter Intensiva. 2019;31(2):180-185
DOI 10.5935/0103-507X.20190027
Views0ABSTRACT
Objective:
To examine the usual practice of airway management during the extubation procedure through an online survey to professionals working in intensive care units in the Autonomous City of Buenos Aires and in the Province of Buenos Aires, Argentina.
Methods:
A cross-sectional descriptive study online survey was conducted from February 11 to March 11, 2013. A database was generated, and a voluntary and anonymous invitation to access the survey was sent by email to 500 participants.
Results:
Out of a total of 500 participants, 217 (44%) responded to the survey, of whom 59.4% were physical therapists. One hundred ninety-five (89.9%) professionals were working in adult care. Regarding the cuff deflation procedure and extubation, 203 (93.5%) performe endotracheal suctioning, and 27 (12.5%) use positive pressure. Approximately 53.5% of participants reported having experienced immediate complications with this procedure in the last three months. In all, 163 complications were reported, and stridor was the most prevalent (52.7%).
Conclusion:
Most professionals working in intensive care units in the Autonomous City of Buenos Aires and in the Province of Buenos Aires, Argentina, use endotracheal suctioning without applying positive pressure during extubation.
Keywords:Airway extubation/adverse effectsIntermittent positive-pressure ventilationSurvey and questionnairesSee more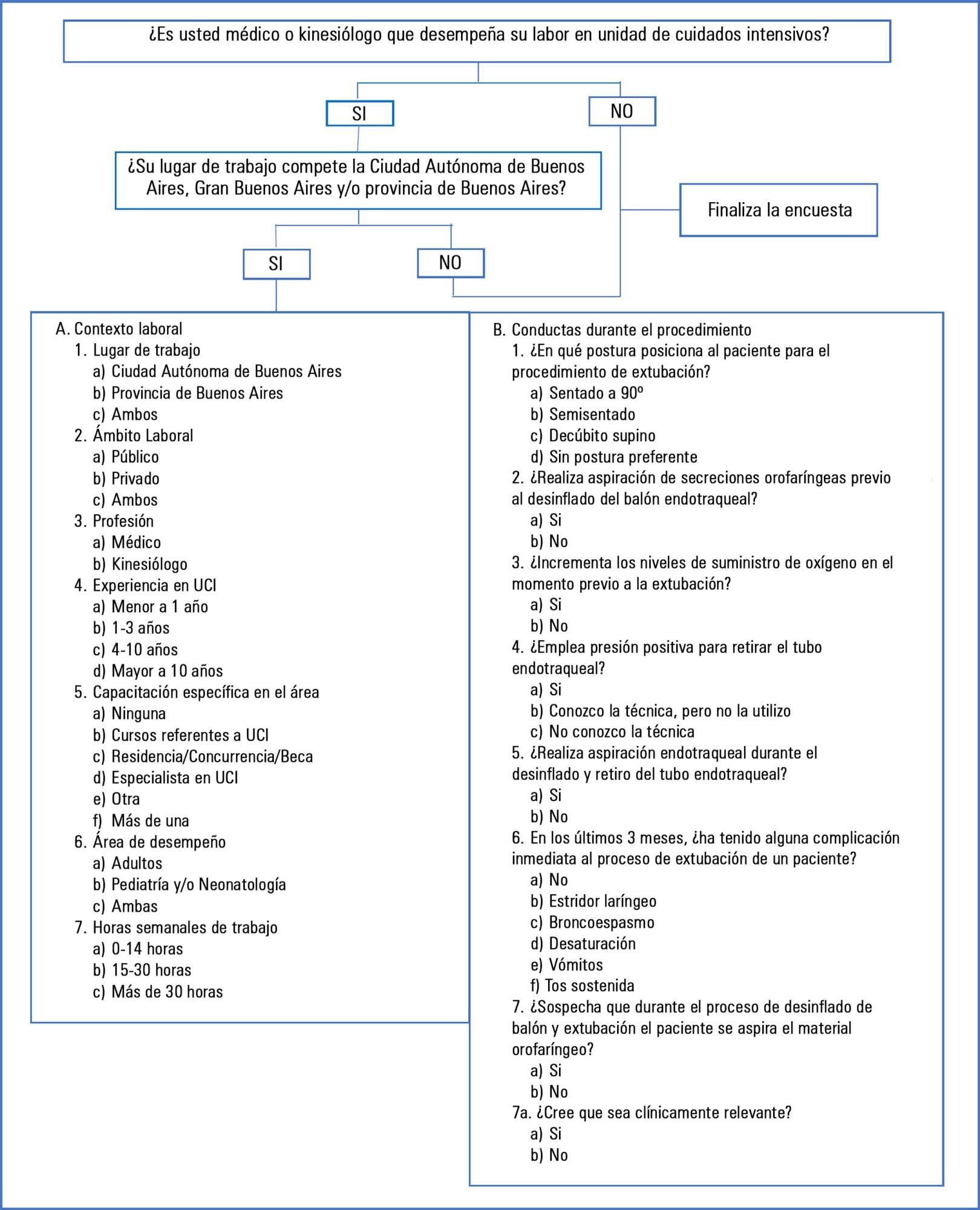
-
Original Article
Heel prick test: maternal-fetal conditions that may have an effect on the test results in newborns admitted to the intensive care unit
Rev Bras Ter Intensiva. 2019;31(2):186-192
Abstract
Original ArticleHeel prick test: maternal-fetal conditions that may have an effect on the test results in newborns admitted to the intensive care unit
Rev Bras Ter Intensiva. 2019;31(2):186-192
DOI 10.5935/0103-507X.20190030
Views0ABSTRACT
Objective:
To describe the characteristics of the heel prick test in newborns admitted to the intensive care unit of a university hospital as well as to determine whether maternal and fetal conditions could have affected the results of this test.
Methods:
Retrospective longitudinal study with a quantitative approach that evaluated 240 medical records. The data collected were analyzed by descriptive statistical analysis.
Results:
There was a predominance of pregnant women aged 20 to 34 years who had a complete secondary education and who had more than six prenatal care visits. Maternal complications or pathologies occurred in 60% of the mothers, and most (67.5%) did not present any condition that could have affected the heel prick test results. Most newborns were premature and exhibited low birth weight. Approximately 90% of newborns exhibited conditions that could have influenced the test, especially prematurity, parenteral nutrition and blood transfusion. Of the 240 newborns, 25% had abnormal heel prick test results, especially for cystic fibrosis and congenital adrenal hyperplasia.
Conclusion:
There are maternal and neonatal conditions that can affect heel prick test results, and therefore, their investigation is essential, aiming to guide measures that promote mother and child health and consolidate neonatal screening in this population.
Keywords:Infant, newbornInfant, prematureIntensive care unitsIntensive care, neonatalMetabolism, inborn errorsMother and child healthNeonatal screeningSee moreViews0Abstract
Original ArticleHeel prick test: maternal-fetal conditions that may have an effect on the test results in newborns admitted to the intensive care unit
Rev Bras Ter Intensiva. 2019;31(2):186-192
DOI 10.5935/0103-507X.20190030
Views0ABSTRACT
Objective:
To describe the characteristics of the heel prick test in newborns admitted to the intensive care unit of a university hospital as well as to determine whether maternal and fetal conditions could have affected the results of this test.
Methods:
Retrospective longitudinal study with a quantitative approach that evaluated 240 medical records. The data collected were analyzed by descriptive statistical analysis.
Results:
There was a predominance of pregnant women aged 20 to 34 years who had a complete secondary education and who had more than six prenatal care visits. Maternal complications or pathologies occurred in 60% of the mothers, and most (67.5%) did not present any condition that could have affected the heel prick test results. Most newborns were premature and exhibited low birth weight. Approximately 90% of newborns exhibited conditions that could have influenced the test, especially prematurity, parenteral nutrition and blood transfusion. Of the 240 newborns, 25% had abnormal heel prick test results, especially for cystic fibrosis and congenital adrenal hyperplasia.
Conclusion:
There are maternal and neonatal conditions that can affect heel prick test results, and therefore, their investigation is essential, aiming to guide measures that promote mother and child health and consolidate neonatal screening in this population.
Keywords:Infant, newbornInfant, prematureIntensive care unitsIntensive care, neonatalMetabolism, inborn errorsMother and child healthNeonatal screeningSee more -
Original Article
Availability of resources to treat sepsis in Brazil: a random sample of Brazilian institutions
Rev Bras Ter Intensiva. 2019;31(2):193-201
Abstract
Original ArticleAvailability of resources to treat sepsis in Brazil: a random sample of Brazilian institutions
Rev Bras Ter Intensiva. 2019;31(2):193-201
DOI 10.5935/0103-507X.20190033
Views1ABSTRACT
Objective:
To characterize resource availability from a nationally representative random sample of intensive care units in Brazil.
Methods:
A structured online survey of participating units in the Sepsis PREvalence Assessment Database (SPREAD) study, a nationwide 1-day point prevalence survey to assess the burden of sepsis in Brazil, was sent to the medical director of each unit.
Results:
A representative sample of 277 of the 317 invited units responded to the resources survey. Most of the hospitals had fewer than 500 beds (94.6%) with a median of 14 beds in the intensive care unit. Providing care for public-insured patients was the main source of income in two-thirds of the surveyed units. Own microbiology laboratory was not available for 26.8% of the surveyed intensive care units, and 10.5% did not always have access to blood cultures. Broad spectrum antibiotics were not always available in 10.5% of surveyed units, and 21.3% could not always measure lactate within three hours. Those institutions with a high resource availability (158 units, 57%) were usually larger and preferentially served patients from the private health system compared to institutions without high resource availability. Otherwise, those without high resource availability did not always have broad-spectrum antibiotics (24.4%), vasopressors (4.2%) or crystalloids (7.6%).
Conclusion:
Our study indicates that a relevant number of units cannot perform basic monitoring and therapeutic interventions in septic patients. Our results highlight major opportunities for improvement to adhere to simple but effective interventions in Brazil.
Keywords:Brazil/epidemiologyCritical careDeveloping countriesEpidemiological monitoringHealth resourcesIntensive care unitsSepsis/epidemiologyTherapeuticsSee moreViews1Abstract
Original ArticleAvailability of resources to treat sepsis in Brazil: a random sample of Brazilian institutions
Rev Bras Ter Intensiva. 2019;31(2):193-201
DOI 10.5935/0103-507X.20190033
Views1ABSTRACT
Objective:
To characterize resource availability from a nationally representative random sample of intensive care units in Brazil.
Methods:
A structured online survey of participating units in the Sepsis PREvalence Assessment Database (SPREAD) study, a nationwide 1-day point prevalence survey to assess the burden of sepsis in Brazil, was sent to the medical director of each unit.
Results:
A representative sample of 277 of the 317 invited units responded to the resources survey. Most of the hospitals had fewer than 500 beds (94.6%) with a median of 14 beds in the intensive care unit. Providing care for public-insured patients was the main source of income in two-thirds of the surveyed units. Own microbiology laboratory was not available for 26.8% of the surveyed intensive care units, and 10.5% did not always have access to blood cultures. Broad spectrum antibiotics were not always available in 10.5% of surveyed units, and 21.3% could not always measure lactate within three hours. Those institutions with a high resource availability (158 units, 57%) were usually larger and preferentially served patients from the private health system compared to institutions without high resource availability. Otherwise, those without high resource availability did not always have broad-spectrum antibiotics (24.4%), vasopressors (4.2%) or crystalloids (7.6%).
Conclusion:
Our study indicates that a relevant number of units cannot perform basic monitoring and therapeutic interventions in septic patients. Our results highlight major opportunities for improvement to adhere to simple but effective interventions in Brazil.
Keywords:Brazil/epidemiologyCritical careDeveloping countriesEpidemiological monitoringHealth resourcesIntensive care unitsSepsis/epidemiologyTherapeuticsSee more -
Original Article
Intravenous overload of fluids and sodium may contribute to the lower infusion of enteral nutrition in critically ill patients
Rev Bras Ter Intensiva. 2019;31(2):202-209
Abstract
Original ArticleIntravenous overload of fluids and sodium may contribute to the lower infusion of enteral nutrition in critically ill patients
Rev Bras Ter Intensiva. 2019;31(2):202-209
DOI 10.5935/0103-507X.20190032
Views0See moreABSTRACT
Objective:
To evaluate the effects of intravenous infusion of fluids and sodium on the first day of admission on infusion of enteral nutrition in the first 5 days in intensive care patients.
Methods:
A prospective cohort study was conducted with critical nonsurgical patients admitted for at least 5 days who were on mechanical ventilation and receiving enteral nutrition. The amount of intravenous fluids and sodium infused on the first day and the volume of enteral nutrition infused in the first 5 days were investigated. The volume of intravenous fluids > 35mL/kg or ≤ 35mL/kg of body weight and sodium (above or below the 25th percentile) infused on the first day was compared with infused enteral nutrition.
Results:
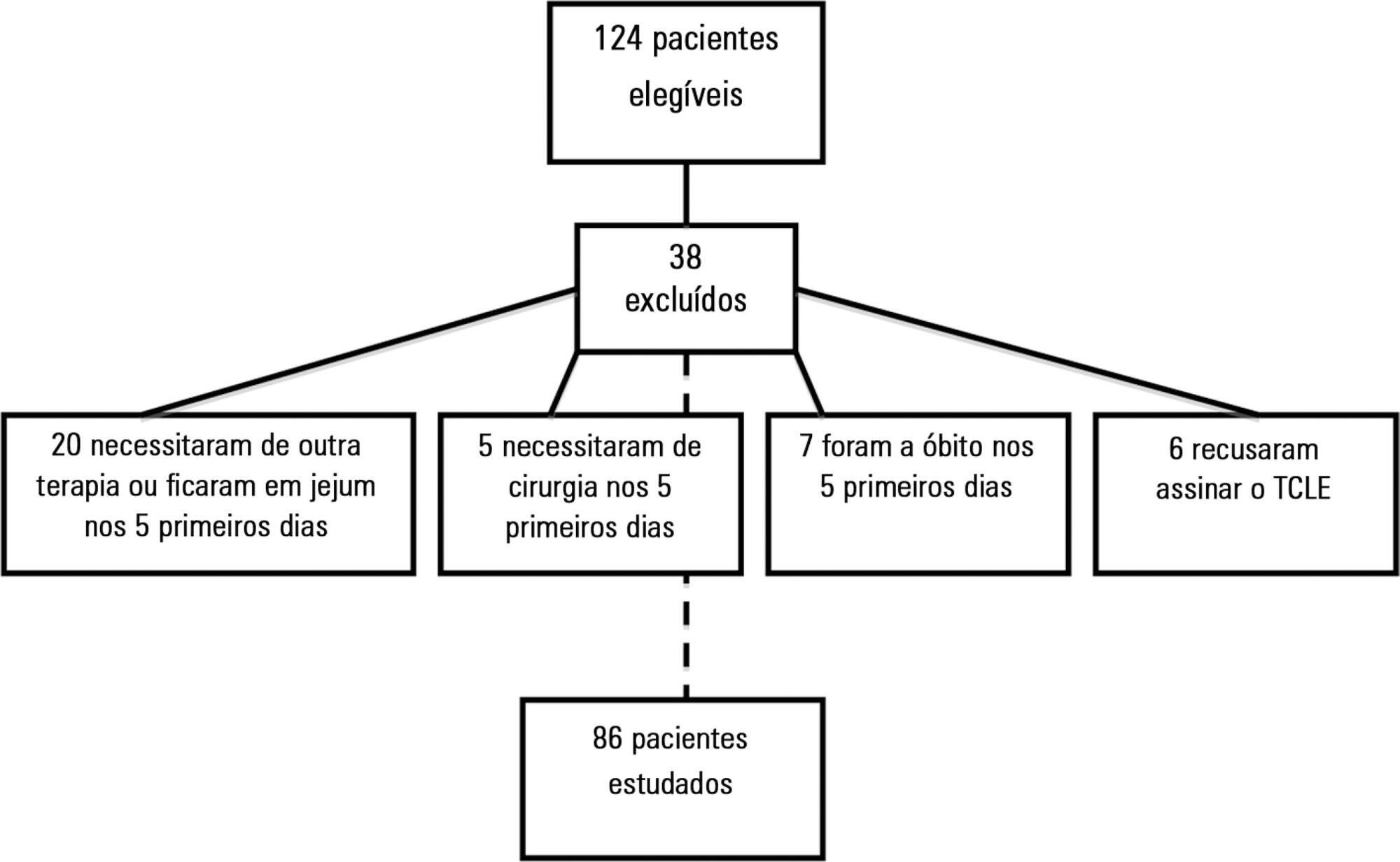
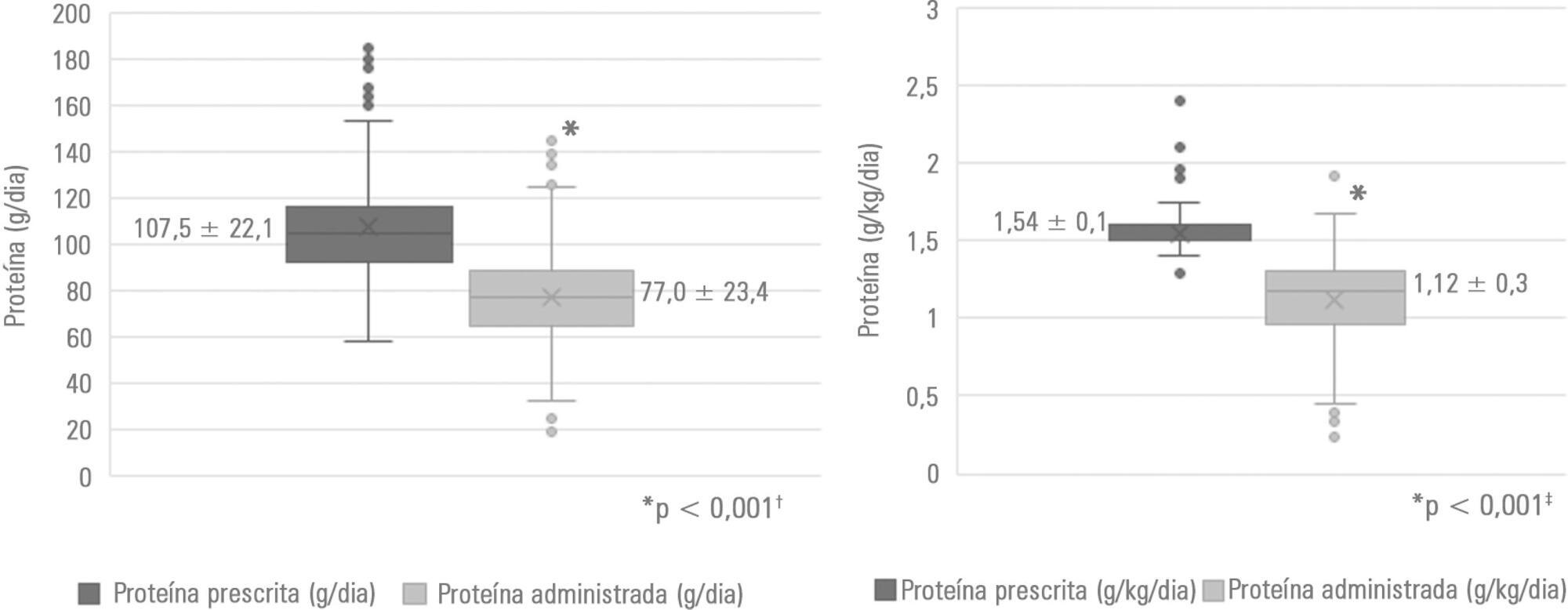
A total of 86 patients were studied, with a mean (± standard deviation) of 65 ± 17 years, of which 54.7% were female. On the first day, 3,393.7 ± 1,417.0mL of fluid (48.2 ± 23.0mL/kg) and 12.2 ± 5.1g of sodium were administered. Fifty-eight (67.4%) patients received more than 35mL/kg of fluids. In 5 days, 67 ± 19.8% (2,993.8 ± 1,324.4mL) of the prescribed enteral nutrition was received. Patients who received > 35mL/kg of intravenous fluids also received less enteral nutrition in 5 days (2,781.4 ± 1,337.9 versus 3,433.6 ± 1,202.2mL; p = 0.03) versus those who received ≤ 35mL/kg. Patients with intravenous sodium infusion above the 25th percentile (≥ 8.73g) on the first day received less enteral nutrition volume in 5 days (2,827.2 ± 1,398.0 versus 3,509.3 ± 911.9mL; p = 0.02).
Conclusion:
The results of this study support the assumption that the administration of intravenous fluids > 35mL/kg and sodium ≥ 8.73g on the first day of hospitalization may contribute to the lower infusion of enteral nutrition in critically ill patients.
Views0Abstract
Original ArticleIntravenous overload of fluids and sodium may contribute to the lower infusion of enteral nutrition in critically ill patients
Rev Bras Ter Intensiva. 2019;31(2):202-209
DOI 10.5935/0103-507X.20190032
Views0See moreABSTRACT
Objective:
To evaluate the effects of intravenous infusion of fluids and sodium on the first day of admission on infusion of enteral nutrition in the first 5 days in intensive care patients.
Methods:
A prospective cohort study was conducted with critical nonsurgical patients admitted for at least 5 days who were on mechanical ventilation and receiving enteral nutrition. The amount of intravenous fluids and sodium infused on the first day and the volume of enteral nutrition infused in the first 5 days were investigated. The volume of intravenous fluids > 35mL/kg or ≤ 35mL/kg of body weight and sodium (above or below the 25th percentile) infused on the first day was compared with infused enteral nutrition.
Results:
A total of 86 patients were studied, with a mean (± standard deviation) of 65 ± 17 years, of which 54.7% were female. On the first day, 3,393.7 ± 1,417.0mL of fluid (48.2 ± 23.0mL/kg) and 12.2 ± 5.1g of sodium were administered. Fifty-eight (67.4%) patients received more than 35mL/kg of fluids. In 5 days, 67 ± 19.8% (2,993.8 ± 1,324.4mL) of the prescribed enteral nutrition was received. Patients who received > 35mL/kg of intravenous fluids also received less enteral nutrition in 5 days (2,781.4 ± 1,337.9 versus 3,433.6 ± 1,202.2mL; p = 0.03) versus those who received ≤ 35mL/kg. Patients with intravenous sodium infusion above the 25th percentile (≥ 8.73g) on the first day received less enteral nutrition volume in 5 days (2,827.2 ± 1,398.0 versus 3,509.3 ± 911.9mL; p = 0.02).
Conclusion:
The results of this study support the assumption that the administration of intravenous fluids > 35mL/kg and sodium ≥ 8.73g on the first day of hospitalization may contribute to the lower infusion of enteral nutrition in critically ill patients.
-
Original Article
Impact of protein intake and nutritional status on the clinical outcome of critically ill patients
Rev Bras Ter Intensiva. 2019;31(2):210-216
Abstract
Original ArticleImpact of protein intake and nutritional status on the clinical outcome of critically ill patients
Rev Bras Ter Intensiva. 2019;31(2):210-216
DOI 10.5935/0103-507X.20190035
Views1See moreABSTRACT
Objective:
To evaluate the association of nutritional status and protein intake with the clinical outcomes of critically ill patients receiving enteral nutrition therapy in an intensive care unit.
Methods:
A retrospective observational analytical study was performed by collecting secondary data recorded in medical records of patients ≥ 18 years of age who were admitted to the intensive care unit and who received exclusive enteral nutrition therapy for at least 72 hours in 2017. Nutritional status was assessed by body mass index and arm circumference. For the estimation of protein requirements, the recommendation of the American Society for Parenteral and Enteral Nutrition was considered. Nutritional adequacy was assessed by the daily collection of prescribed and administered enteral formula. In the analyses, parametric and nonparametric tests were used, and significance was set at p <0.05.
Results:
Of the 188 patients evaluated, 71.3% were male. The median age of the patients was 48.5 years (31.0 – 63.75). The main clinical diagnosis was trauma (46.3%), and eutrophic was the most frequent nutritional status (54.8% according to body mass index and 46.4% according to arm circumference). Protein adequacy was not attained in 56.4% of patients, and only 46.8% reached the minimum protein recommendation. The occurrence of mortality was associated with nutritional diagnosis, body mass index (p = 0.023), arm circumference (p = 0.041) and protein adequacy (p = 0.012).
Conclusion:
Nutritional status and protein intake were significantly associated with the clinical outcomes of critically ill patients.
Views1Abstract
Original ArticleImpact of protein intake and nutritional status on the clinical outcome of critically ill patients
Rev Bras Ter Intensiva. 2019;31(2):210-216
DOI 10.5935/0103-507X.20190035
Views1See moreABSTRACT
Objective:
To evaluate the association of nutritional status and protein intake with the clinical outcomes of critically ill patients receiving enteral nutrition therapy in an intensive care unit.
Methods:
A retrospective observational analytical study was performed by collecting secondary data recorded in medical records of patients ≥ 18 years of age who were admitted to the intensive care unit and who received exclusive enteral nutrition therapy for at least 72 hours in 2017. Nutritional status was assessed by body mass index and arm circumference. For the estimation of protein requirements, the recommendation of the American Society for Parenteral and Enteral Nutrition was considered. Nutritional adequacy was assessed by the daily collection of prescribed and administered enteral formula. In the analyses, parametric and nonparametric tests were used, and significance was set at p <0.05.
Results:
Of the 188 patients evaluated, 71.3% were male. The median age of the patients was 48.5 years (31.0 – 63.75). The main clinical diagnosis was trauma (46.3%), and eutrophic was the most frequent nutritional status (54.8% according to body mass index and 46.4% according to arm circumference). Protein adequacy was not attained in 56.4% of patients, and only 46.8% reached the minimum protein recommendation. The occurrence of mortality was associated with nutritional diagnosis, body mass index (p = 0.023), arm circumference (p = 0.041) and protein adequacy (p = 0.012).
Conclusion:
Nutritional status and protein intake were significantly associated with the clinical outcomes of critically ill patients.
-
Original Article
Implementation of a rapid response team in a large nonprofit Brazilian hospital: improving the quality of emergency care through Plan-Do-Study-Act
Rev Bras Ter Intensiva. 2019;31(2):217-226
Abstract
Original ArticleImplementation of a rapid response team in a large nonprofit Brazilian hospital: improving the quality of emergency care through Plan-Do-Study-Act
Rev Bras Ter Intensiva. 2019;31(2):217-226
DOI 10.5935/0103-507X.20190036
Views1ABSTRACT
Objective:
To describe the implementation of a rapid response team in a large nonprofit hospital, indicating relevant issues for other initiatives in similar contexts, particularly in Latin America.
Methods:
In general terms, the intervention consisted of three major components: (1) a tool to detect aggravation of clinical conditions in general wards; (2) the structuring of a rapid response team to attend to all patients at risk; and (3) the monitoring of indicators regarding the intervention. This work employed four half-year Plan-Do-Study-Act cycles to test and adjust the intervention from January 2013 to December 2014.
Results:
Between 2013 and 2014, the rapid response team attended to 2,296 patients. This study showed a nonsignificant reduction in mortality from 8.3% in cycle 1 to 5.0% in cycle 4; however, death rates remained stable in cycles 3 and 4, with frequencies of 5.2% and 5.0%, respectively. Regarding patient flow and continuum of critical care, which is a premise of the rapid response system, there was a reduction in waiting time for intensive care unit beds with a decrease from 45.9% to 19.0% in the frequency of inpatients who could not be admitted immediately after indication (p < 0.001), representing improved patient flow in the hospital. In addition, an increase in the recognition of palliative care patients from 2.8% to 10.3% was noted (p = 0.005).
Conclusion:
Implementing a rapid response team in contexts where there are structural restrictions, such as lack of intensive care unit beds, may be very beneficial, but a strategy of adjustment is needed.
Keywords:Emergency medical servicesHospital careHospital rapid response teamLatin AmericaOrganizational innovationQuality assurance health careQuality of health careSee moreViews1Abstract
Original ArticleImplementation of a rapid response team in a large nonprofit Brazilian hospital: improving the quality of emergency care through Plan-Do-Study-Act
Rev Bras Ter Intensiva. 2019;31(2):217-226
DOI 10.5935/0103-507X.20190036
Views1ABSTRACT
Objective:
To describe the implementation of a rapid response team in a large nonprofit hospital, indicating relevant issues for other initiatives in similar contexts, particularly in Latin America.
Methods:
In general terms, the intervention consisted of three major components: (1) a tool to detect aggravation of clinical conditions in general wards; (2) the structuring of a rapid response team to attend to all patients at risk; and (3) the monitoring of indicators regarding the intervention. This work employed four half-year Plan-Do-Study-Act cycles to test and adjust the intervention from January 2013 to December 2014.
Results:
Between 2013 and 2014, the rapid response team attended to 2,296 patients. This study showed a nonsignificant reduction in mortality from 8.3% in cycle 1 to 5.0% in cycle 4; however, death rates remained stable in cycles 3 and 4, with frequencies of 5.2% and 5.0%, respectively. Regarding patient flow and continuum of critical care, which is a premise of the rapid response system, there was a reduction in waiting time for intensive care unit beds with a decrease from 45.9% to 19.0% in the frequency of inpatients who could not be admitted immediately after indication (p < 0.001), representing improved patient flow in the hospital. In addition, an increase in the recognition of palliative care patients from 2.8% to 10.3% was noted (p = 0.005).
Conclusion:
Implementing a rapid response team in contexts where there are structural restrictions, such as lack of intensive care unit beds, may be very beneficial, but a strategy of adjustment is needed.
Keywords:Emergency medical servicesHospital careHospital rapid response teamLatin AmericaOrganizational innovationQuality assurance health careQuality of health careSee more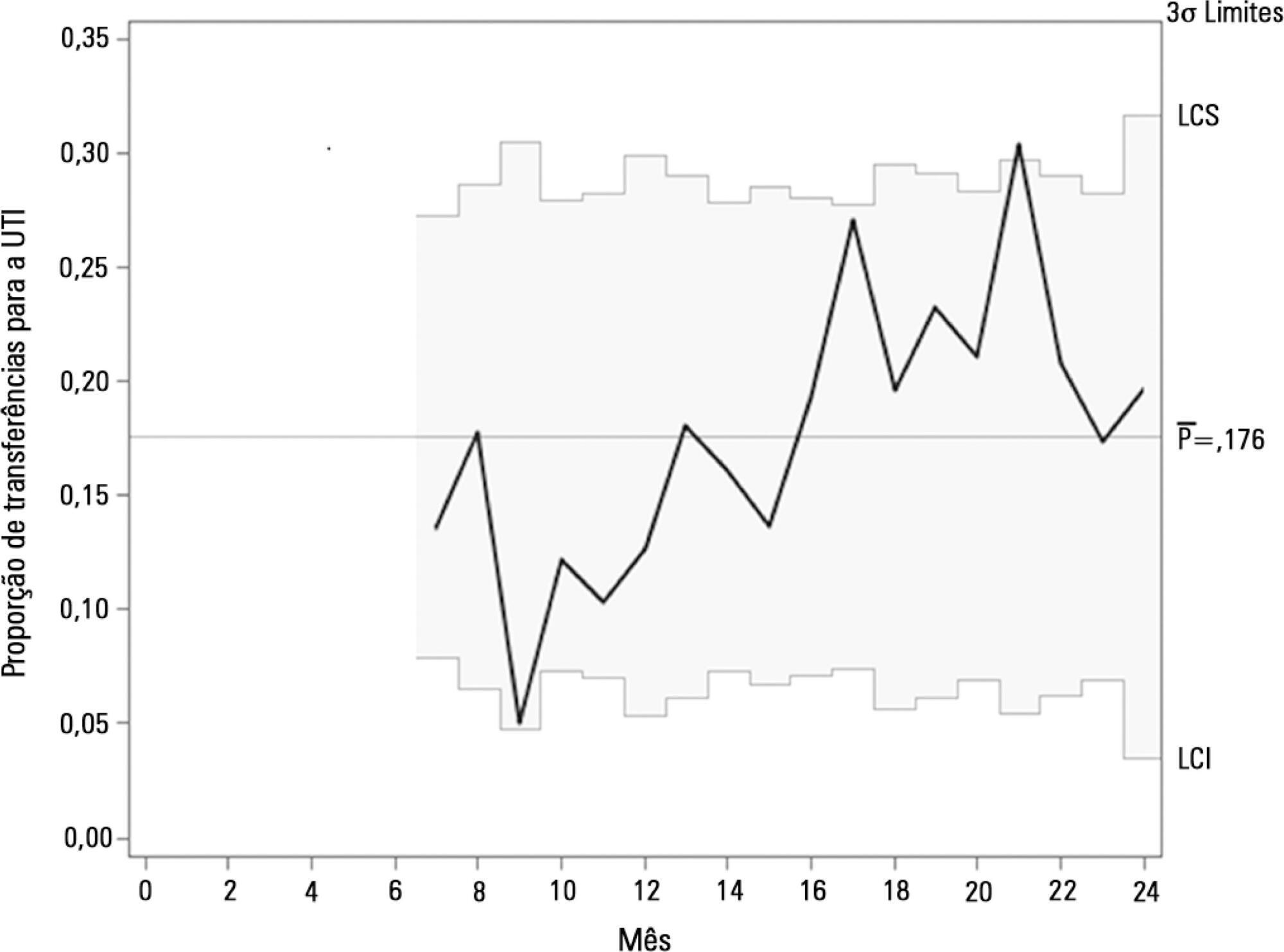
-
Review Article
Safety and potential benefits of physical therapy in adult patients on extracorporeal membrane oxygenation support: a systematic review
Rev Bras Ter Intensiva. 2019;31(2):227-239
Abstract
Review ArticleSafety and potential benefits of physical therapy in adult patients on extracorporeal membrane oxygenation support: a systematic review
Rev Bras Ter Intensiva. 2019;31(2):227-239
DOI 10.5935/0103-507X.20190017
Views0Abstract
Scientific and technological advances, coupled with the work of multidisciplinary teams in intensive care units, have increased the survival of critically ill patients. An essential life support resource used in intensive care is extracorporeal membrane oxygenation. Despite the increased number of studies involving critically ill patients, few studies to date have demonstrated the safety and benefits of physical therapy combined with extracorporeal membrane oxygenation support. This review identified the clinical outcomes of physical therapy in adult patients on extracorporeal membrane oxygenation support by searching the MEDLINE®, PEDro, Cochrane CENTRAL, LILACS, and EMBASE databases and by manually searching the references of the articles published until September 2017. The database search retrieved 1,213 studies. Of these studies, 20 were included in this review, with data on 317 subjects (58 in the control group). Twelve studies reported that there were no complications during physical therapy. Cannula fracture during ambulation (one case), thrombus in the return cannula (one case), and leg swelling (one case) were reported in two studies, and desaturation and mild vertigo were reported in two studies. In contrast, improvements in respiratory/pulmonary function, functional capacity, muscle strength (with reduced muscle mass loss), incidence of myopathy, length of hospitalization, and mortality in patients who underwent physical therapy were reported. The analysis of the available data indicates that physical therapy, including early progressive mobilization, standing, ambulation, and breathing techniques, together with extracorporeal membrane oxygenation, is feasible, relatively safe, and potentially beneficial for critically ill adult patients.
Keywords:Early ambulationExtracorporeal membrane oxygenationPhysical therapy modalitiesPhysical therapy specialtyRehabilitationSee moreViews0Abstract
Review ArticleSafety and potential benefits of physical therapy in adult patients on extracorporeal membrane oxygenation support: a systematic review
Rev Bras Ter Intensiva. 2019;31(2):227-239
DOI 10.5935/0103-507X.20190017
Views0Abstract
Scientific and technological advances, coupled with the work of multidisciplinary teams in intensive care units, have increased the survival of critically ill patients. An essential life support resource used in intensive care is extracorporeal membrane oxygenation. Despite the increased number of studies involving critically ill patients, few studies to date have demonstrated the safety and benefits of physical therapy combined with extracorporeal membrane oxygenation support. This review identified the clinical outcomes of physical therapy in adult patients on extracorporeal membrane oxygenation support by searching the MEDLINE®, PEDro, Cochrane CENTRAL, LILACS, and EMBASE databases and by manually searching the references of the articles published until September 2017. The database search retrieved 1,213 studies. Of these studies, 20 were included in this review, with data on 317 subjects (58 in the control group). Twelve studies reported that there were no complications during physical therapy. Cannula fracture during ambulation (one case), thrombus in the return cannula (one case), and leg swelling (one case) were reported in two studies, and desaturation and mild vertigo were reported in two studies. In contrast, improvements in respiratory/pulmonary function, functional capacity, muscle strength (with reduced muscle mass loss), incidence of myopathy, length of hospitalization, and mortality in patients who underwent physical therapy were reported. The analysis of the available data indicates that physical therapy, including early progressive mobilization, standing, ambulation, and breathing techniques, together with extracorporeal membrane oxygenation, is feasible, relatively safe, and potentially beneficial for critically ill adult patients.
Keywords:Early ambulationExtracorporeal membrane oxygenationPhysical therapy modalitiesPhysical therapy specialtyRehabilitationSee more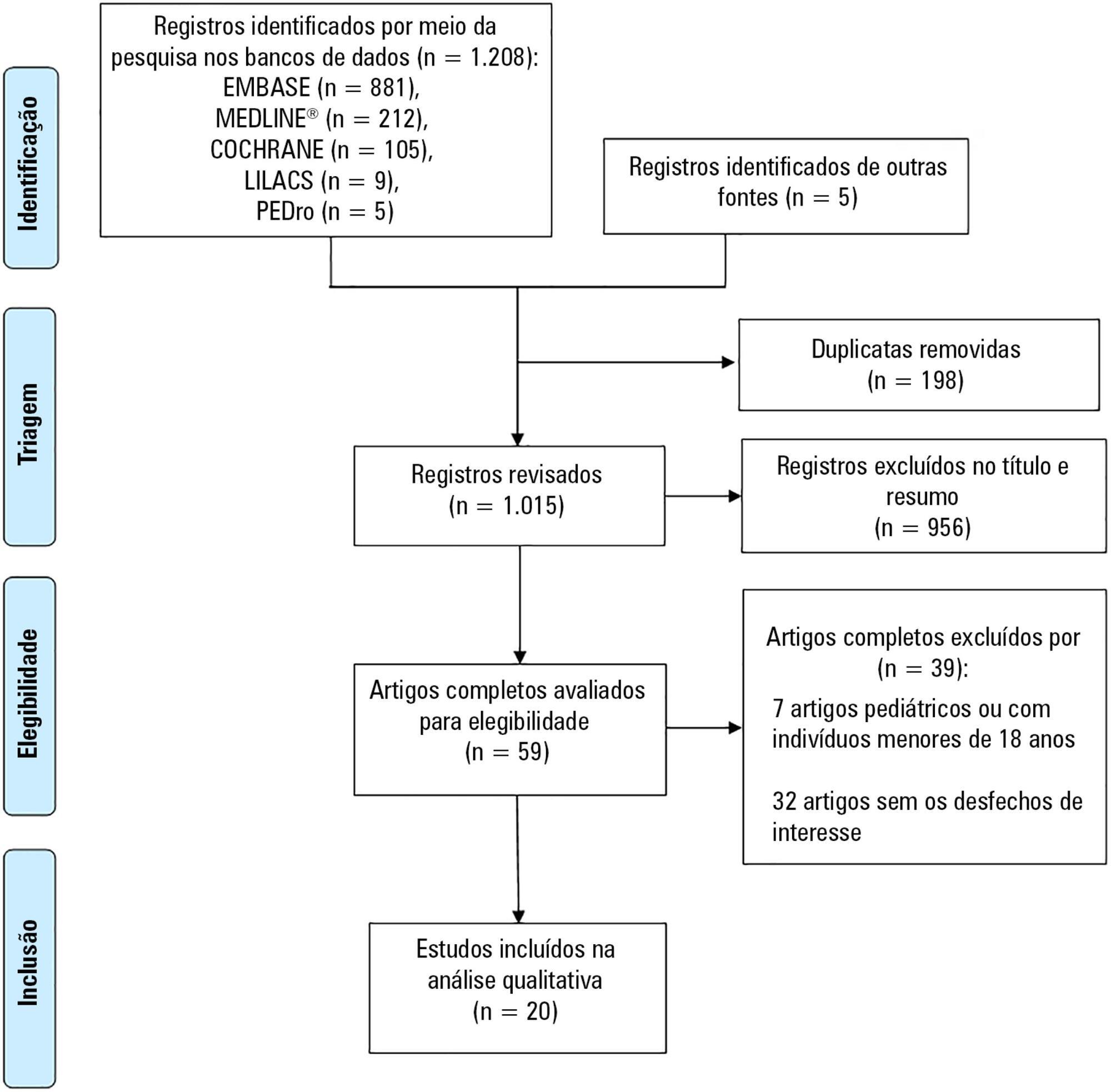
-
Review Article
Inferior vena cava evaluation in fluid therapy decision making in intensive care: practical implications
Rev Bras Ter Intensiva. 2019;31(2):240-247
Abstract
Review ArticleInferior vena cava evaluation in fluid therapy decision making in intensive care: practical implications
Rev Bras Ter Intensiva. 2019;31(2):240-247
DOI 10.5935/0103-507X.20190039
Views0See moreABSTRACT
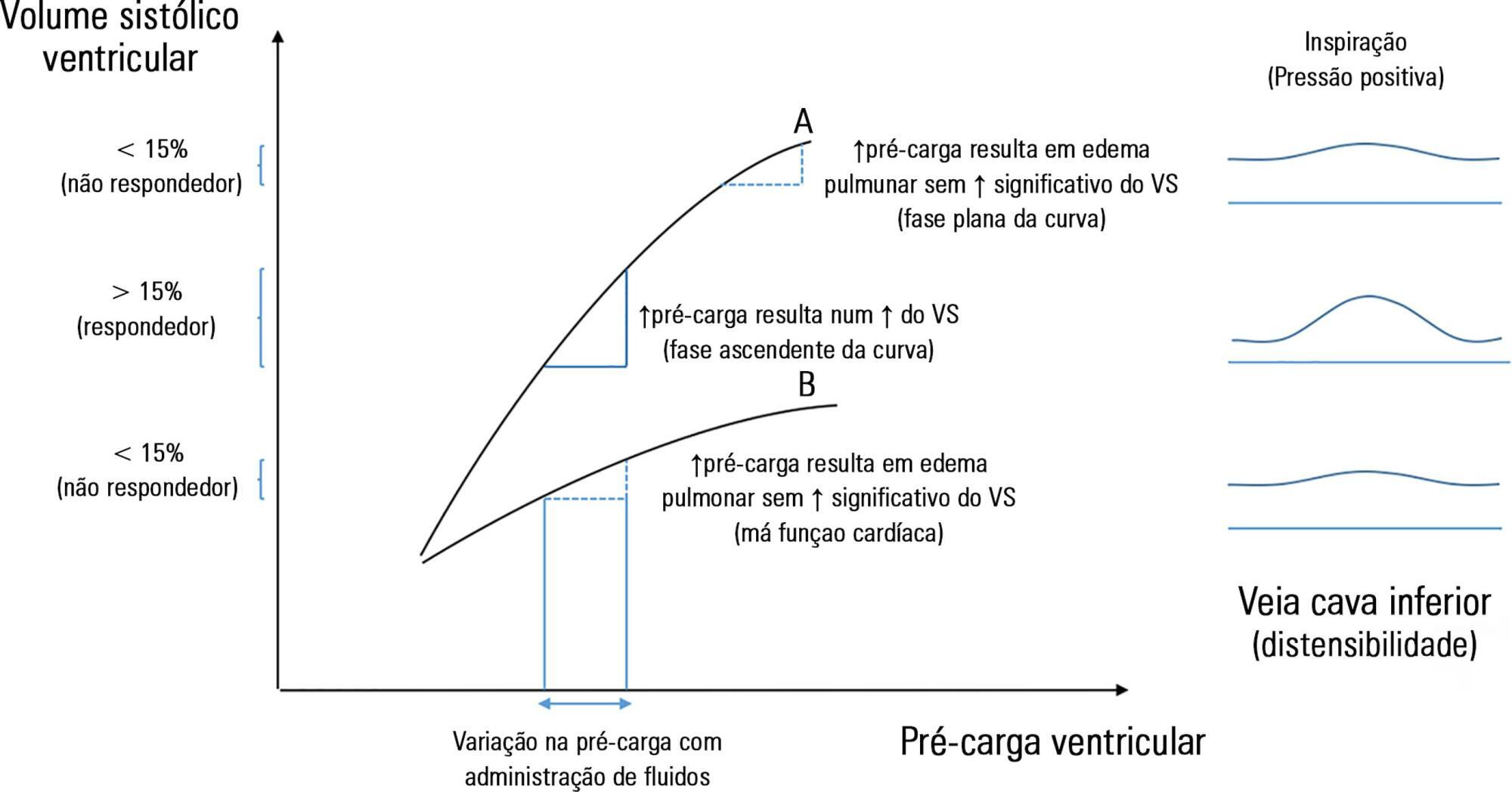
The fluid resuscitation of patients with acute circulatory failure aims to increase systolic volume and consequently improve cardiac output for better tissue oxygenation. However, this effect does not always occur because approximately half of patients do not respond to fluids. The evaluation of fluid responsiveness before their administration may help to identify patients who would benefit from fluid resuscitation and avoid the risk of fluid overload in the others. The dynamic parameters of fluid responsiveness evaluation are promising predictive factors. Of these, the echocardiographic measurement of the respiratory variation in the inferior vena cava diameter is easy to apply and has been used in the hemodynamic evaluation of intensive care unit patients. However, the applicability of this technique has many limitations, and the present studies are heterogeneous and inconsistent across specific groups of patients. We review the use of the inferior vena cava diameter respiratory variation, measured via transthoracic echocardiography, to decide whether to administer fluids to patients with acute circulatory failure in the intensive care unit. We explore the benefits and limitations of this technique, its current use, and the existing evidence.
Views0Abstract
Review ArticleInferior vena cava evaluation in fluid therapy decision making in intensive care: practical implications
Rev Bras Ter Intensiva. 2019;31(2):240-247
DOI 10.5935/0103-507X.20190039
Views0See moreABSTRACT
The fluid resuscitation of patients with acute circulatory failure aims to increase systolic volume and consequently improve cardiac output for better tissue oxygenation. However, this effect does not always occur because approximately half of patients do not respond to fluids. The evaluation of fluid responsiveness before their administration may help to identify patients who would benefit from fluid resuscitation and avoid the risk of fluid overload in the others. The dynamic parameters of fluid responsiveness evaluation are promising predictive factors. Of these, the echocardiographic measurement of the respiratory variation in the inferior vena cava diameter is easy to apply and has been used in the hemodynamic evaluation of intensive care unit patients. However, the applicability of this technique has many limitations, and the present studies are heterogeneous and inconsistent across specific groups of patients. We review the use of the inferior vena cava diameter respiratory variation, measured via transthoracic echocardiography, to decide whether to administer fluids to patients with acute circulatory failure in the intensive care unit. We explore the benefits and limitations of this technique, its current use, and the existing evidence.
-
Review Article
Early mobilization protocols for critically ill pediatric patients: systematic review
Rev Bras Ter Intensiva. 2019;31(2):248-257
Abstract
Review ArticleEarly mobilization protocols for critically ill pediatric patients: systematic review
Rev Bras Ter Intensiva. 2019;31(2):248-257
DOI 10.5935/0103-507X.20190038
Views0See moreABSTRACT
Objective:
To describe the existing early mobilization protocols in pediatric intensive care units.
Methods:
A systematic literature review was performed using the databases MEDLINE®, Embase, SciELO, LILACS and PeDRO, without restrictions of date and language. Observational and randomized and nonrandomized clinical trials that described an early mobilization program in patients aged between 29 days and 18 years admitted to the pediatric intensive care unit were included. The methodological quality of the studies was evaluated using the Newcastle-Ottawa Scale, Methodological Index for Non-Randomized Studies and the Cochrane Collaboration.
Results:
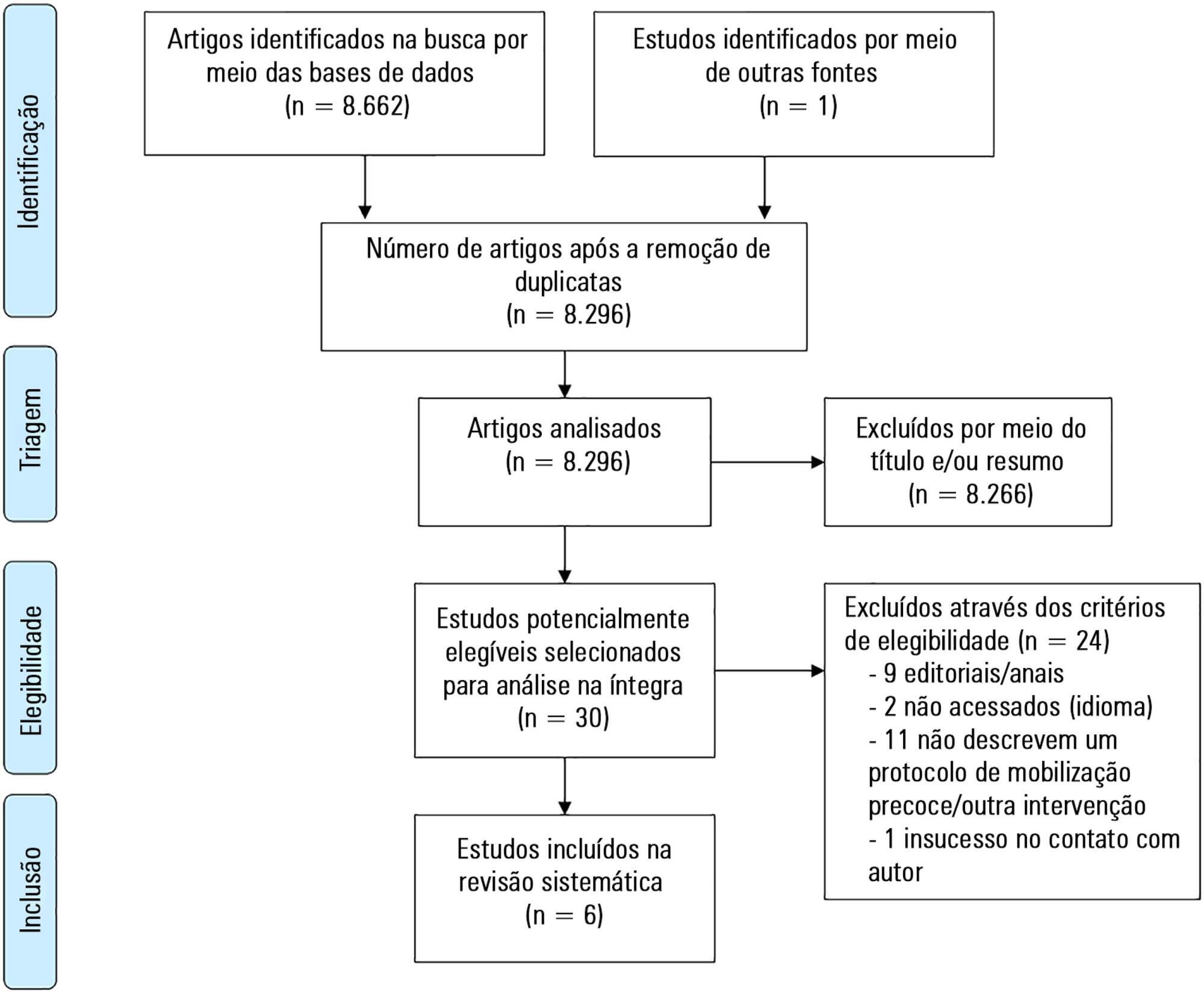
A total of 8,663 studies were identified, of which 6 were included in this review. Three studies described the implementation of an early mobilization program, including activities such as progressive passive mobilization, positioning, and discussion of mobilization goals with the team, in addition to contraindications and interruption criteria. Cycle ergometer and virtual reality games were also used as resources for mobilization. Four studies considered the importance of the participation of the multidisciplinary team in the implementation of early mobilization protocols.
Conclusion:
In general, early mobilization protocols are based on individualized interventions, depending on the child’s development. In addition, the use of a cycle ergometer may be feasible and safe in this population. The implementation of institutional and multidisciplinary protocols may contribute to the use of early mobilization in pediatric intensive care units; however, studies demonstrating the efficacy of such intervention are needed.
Views0Abstract
Review ArticleEarly mobilization protocols for critically ill pediatric patients: systematic review
Rev Bras Ter Intensiva. 2019;31(2):248-257
DOI 10.5935/0103-507X.20190038
Views0See moreABSTRACT
Objective:
To describe the existing early mobilization protocols in pediatric intensive care units.
Methods:
A systematic literature review was performed using the databases MEDLINE®, Embase, SciELO, LILACS and PeDRO, without restrictions of date and language. Observational and randomized and nonrandomized clinical trials that described an early mobilization program in patients aged between 29 days and 18 years admitted to the pediatric intensive care unit were included. The methodological quality of the studies was evaluated using the Newcastle-Ottawa Scale, Methodological Index for Non-Randomized Studies and the Cochrane Collaboration.
Results:
A total of 8,663 studies were identified, of which 6 were included in this review. Three studies described the implementation of an early mobilization program, including activities such as progressive passive mobilization, positioning, and discussion of mobilization goals with the team, in addition to contraindications and interruption criteria. Cycle ergometer and virtual reality games were also used as resources for mobilization. Four studies considered the importance of the participation of the multidisciplinary team in the implementation of early mobilization protocols.
Conclusion:
In general, early mobilization protocols are based on individualized interventions, depending on the child’s development. In addition, the use of a cycle ergometer may be feasible and safe in this population. The implementation of institutional and multidisciplinary protocols may contribute to the use of early mobilization in pediatric intensive care units; however, studies demonstrating the efficacy of such intervention are needed.
-
Case Report
Rituximab use for lymphoplasmacytic lymphoma during continuous renal replacement therapy
Rev Bras Ter Intensiva. 2019;31(2):258-261
Abstract
Case ReportRituximab use for lymphoplasmacytic lymphoma during continuous renal replacement therapy
Rev Bras Ter Intensiva. 2019;31(2):258-261
DOI 10.5935/0103-507X.20190040
Views0ABSTRACT
Rituximab safety and efficacy in patients with renal impairment have not been established, nor have the effects of hemodialysis on serum rituximab level. There are only a few published case reports assessing serum rituximab level pre- and postdialysis. No data have been published regarding the usage of rituximab in patients with continuous renal replacement therapy. The authors present a case of a 59-year-old female patient who presented with paraneoplastic tetraparesis. She was admitted to the intensive care unit due to alveolar hemorrhage with respiratory failure and acute kidney injury requiring continuous renal replacement therapy. After a diagnostic workup, the diagnosis of lymphoplasmacytic lymphoma was established. Therapy with rituximab and cyclophosphamide was started. Rituximab levels were determined in serum and dialysate. No rituximab was found in the dialysate. The patient died after 2 months in the intensive care unit from nosocomial pneumonia due to multidrug-resistant Pseudomonas aeruginosa.
Keywords:Critical careLymphomaPolyradiculoneuropathyRenal insufficiencyRenal replacement therapyRituximabSee moreViews0Abstract
Case ReportRituximab use for lymphoplasmacytic lymphoma during continuous renal replacement therapy
Rev Bras Ter Intensiva. 2019;31(2):258-261
DOI 10.5935/0103-507X.20190040
Views0ABSTRACT
Rituximab safety and efficacy in patients with renal impairment have not been established, nor have the effects of hemodialysis on serum rituximab level. There are only a few published case reports assessing serum rituximab level pre- and postdialysis. No data have been published regarding the usage of rituximab in patients with continuous renal replacement therapy. The authors present a case of a 59-year-old female patient who presented with paraneoplastic tetraparesis. She was admitted to the intensive care unit due to alveolar hemorrhage with respiratory failure and acute kidney injury requiring continuous renal replacement therapy. After a diagnostic workup, the diagnosis of lymphoplasmacytic lymphoma was established. Therapy with rituximab and cyclophosphamide was started. Rituximab levels were determined in serum and dialysate. No rituximab was found in the dialysate. The patient died after 2 months in the intensive care unit from nosocomial pneumonia due to multidrug-resistant Pseudomonas aeruginosa.
Keywords:Critical careLymphomaPolyradiculoneuropathyRenal insufficiencyRenal replacement therapyRituximabSee more -
Case Report
Traumatic tricuspid valve papillary muscle case with concomitant acquired patent foramen ovale and covert right atrial rupture
Rev Bras Ter Intensiva. 2019;31(2):262-265
Abstract
Case ReportTraumatic tricuspid valve papillary muscle case with concomitant acquired patent foramen ovale and covert right atrial rupture
Rev Bras Ter Intensiva. 2019;31(2):262-265
DOI 10.5935/0103-507X.20190034
Views0See moreABSTRACT
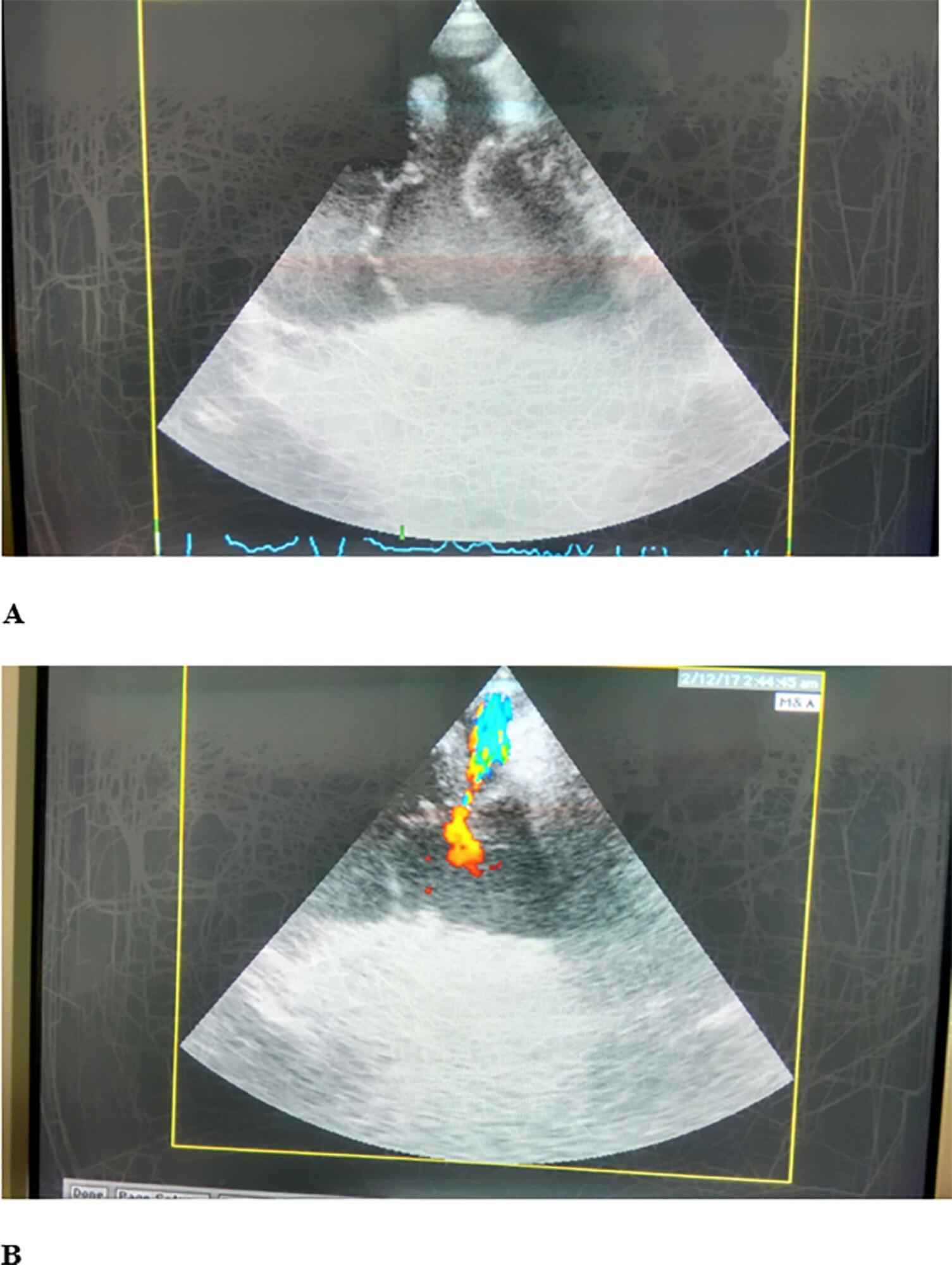
Cardiac trauma often occurs in motor vehicle accidents. A 50-year-old female driver was transported to our hospital with multiple trauma after a high-speed car accident. After admission to the intensive care unit, cardiac ultrasound examination revealed traumatic tricuspid valve papillary muscle rupture and patent foramen ovale, while Lancisi’s sign was noted on physical examination. Surgical treatment was performed with valve annuloplasty and closure of the patent foramen ovale and a covert right atrial defect that was detected intraoperatively.
Views0Abstract
Case ReportTraumatic tricuspid valve papillary muscle case with concomitant acquired patent foramen ovale and covert right atrial rupture
Rev Bras Ter Intensiva. 2019;31(2):262-265
DOI 10.5935/0103-507X.20190034
Views0See moreABSTRACT
Cardiac trauma often occurs in motor vehicle accidents. A 50-year-old female driver was transported to our hospital with multiple trauma after a high-speed car accident. After admission to the intensive care unit, cardiac ultrasound examination revealed traumatic tricuspid valve papillary muscle rupture and patent foramen ovale, while Lancisi’s sign was noted on physical examination. Surgical treatment was performed with valve annuloplasty and closure of the patent foramen ovale and a covert right atrial defect that was detected intraoperatively.
-
Letter to the Editor
Extensive oral ulcer in a patient with lupus erythematosus
Rev Bras Ter Intensiva. 2019;31(2):266-268
Abstract
Letter to the EditorExtensive oral ulcer in a patient with lupus erythematosus
Rev Bras Ter Intensiva. 2019;31(2):266-268
DOI 10.5935/0103-507X.20190020
Views0To the editor, Systemic lupus erythematosus (SLE) is a heterogeneous and multisystemic autoimmune disease characterized by the production of autoantibodies against various cellular constituents.() Systemic lupus erythematosus presents with varied clinical manifestations and periods of exacerbation and remission.() Systemic lupus erythematosus may present as intraoral lesions that occur primarily in the tongue, buccal mucosa, clips […]See moreViews0Abstract
Letter to the EditorExtensive oral ulcer in a patient with lupus erythematosus
Rev Bras Ter Intensiva. 2019;31(2):266-268
DOI 10.5935/0103-507X.20190020
Views0To the editor, Systemic lupus erythematosus (SLE) is a heterogeneous and multisystemic autoimmune disease characterized by the production of autoantibodies against various cellular constituents.() Systemic lupus erythematosus presents with varied clinical manifestations and periods of exacerbation and remission.() Systemic lupus erythematosus may present as intraoral lesions that occur primarily in the tongue, buccal mucosa, clips […]See more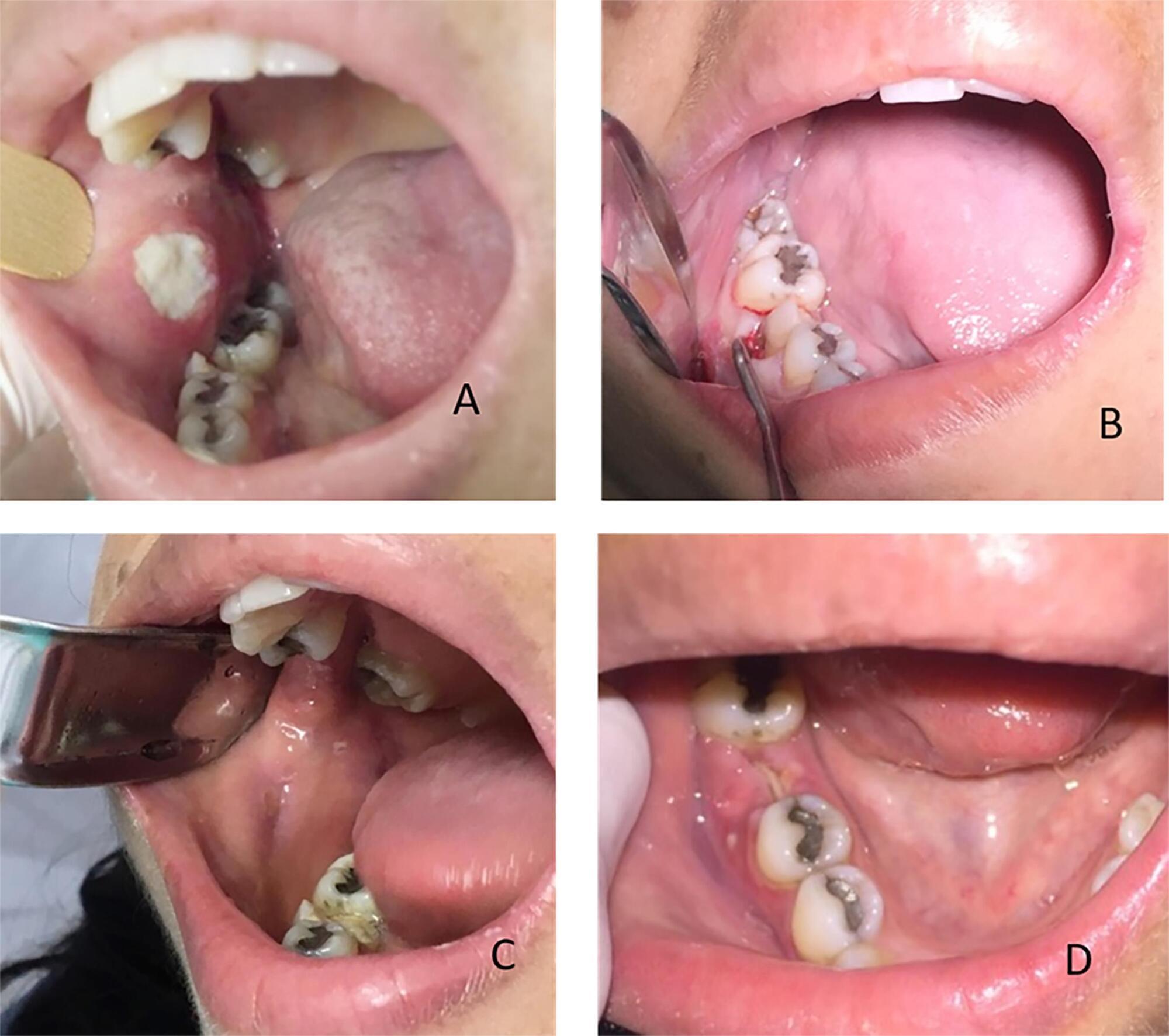
-
Letter to the Editor
Multiple organ dysfunction – we must take a closer look at muscle wasting!
Rev Bras Ter Intensiva. 2019;31(2):269-270
Abstract
Letter to the EditorMultiple organ dysfunction – we must take a closer look at muscle wasting!
Rev Bras Ter Intensiva. 2019;31(2):269-270
DOI 10.5935/0103-507X.20190021
Views1To the editor Organ dysfunction is quantified routinely by scores such as: the Sequential Organ Failure Assessment (SOFA) score, the Multiple Organ Dysfunction Score (MODS), and the Logistic Organ Dysfunction Score (LODS).() Once the number of organs failure is associated with intensive care unit (ICU) and hospital-mortality, these scores are helpful to only predict acute […]See moreViews1Abstract
Letter to the EditorMultiple organ dysfunction – we must take a closer look at muscle wasting!
Rev Bras Ter Intensiva. 2019;31(2):269-270
DOI 10.5935/0103-507X.20190021
Views1To the editor Organ dysfunction is quantified routinely by scores such as: the Sequential Organ Failure Assessment (SOFA) score, the Multiple Organ Dysfunction Score (MODS), and the Logistic Organ Dysfunction Score (LODS).() Once the number of organs failure is associated with intensive care unit (ICU) and hospital-mortality, these scores are helpful to only predict acute […]See more -
Letter to the Editor
To: Acute kidney injury and intra-abdominal hypertension in burn patients in intensive care
Rev Bras Ter Intensiva. 2019;31(2):271-272
Abstract
Letter to the EditorTo: Acute kidney injury and intra-abdominal hypertension in burn patients in intensive care
Rev Bras Ter Intensiva. 2019;31(2):271-272
DOI 10.5935/0103-507X.20190022
Views0To the Editor The difficulty of managing fluid in severely burned patients and the fact that monitoring intra-abdominal pressure (IAP) is not yet a routine intensive care therapy makes the article by Talizin et al.() mandatory reading, especially for professionals working with this group of patients.[…]See moreViews0Abstract
Letter to the EditorTo: Acute kidney injury and intra-abdominal hypertension in burn patients in intensive care
Rev Bras Ter Intensiva. 2019;31(2):271-272
DOI 10.5935/0103-507X.20190022
Views0To the Editor The difficulty of managing fluid in severely burned patients and the fact that monitoring intra-abdominal pressure (IAP) is not yet a routine intensive care therapy makes the article by Talizin et al.() mandatory reading, especially for professionals working with this group of patients.[…]See more -
Letter to the Editor
To: Perfusion index for assessing microvascular reactivity in septic shock after fluid resuscitation
Rev Bras Ter Intensiva. 2019;31(2):273-274
Abstract
Letter to the EditorTo: Perfusion index for assessing microvascular reactivity in septic shock after fluid resuscitation
Rev Bras Ter Intensiva. 2019;31(2):273-274
DOI 10.5935/0103-507X.20190019
Views0Dear Editor, In a recent issue of your journal, Menezes et al.() presented a superb evaluation of the perfusion index in septic shock patients following fluid resuscitation. In a novel and fascinating piece of research, the authors seem to successfully evaluate microvascular reactivity byoximetry-derived perfusion index and reactive hyperemia. However, as already mentioned by the […]See moreViews0Abstract
Letter to the EditorTo: Perfusion index for assessing microvascular reactivity in septic shock after fluid resuscitation
Rev Bras Ter Intensiva. 2019;31(2):273-274
DOI 10.5935/0103-507X.20190019
Views0Dear Editor, In a recent issue of your journal, Menezes et al.() presented a superb evaluation of the perfusion index in septic shock patients following fluid resuscitation. In a novel and fascinating piece of research, the authors seem to successfully evaluate microvascular reactivity byoximetry-derived perfusion index and reactive hyperemia. However, as already mentioned by the […]See more
Volume Articles - Critical Care Science (CCS)
