Hospital care Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2022;34(4):499-506
DOI 10.5935/0103-507X.20220080-en
To evaluate the prevalence and factors associated with depression in family members of people hospitalized in intensive care units.
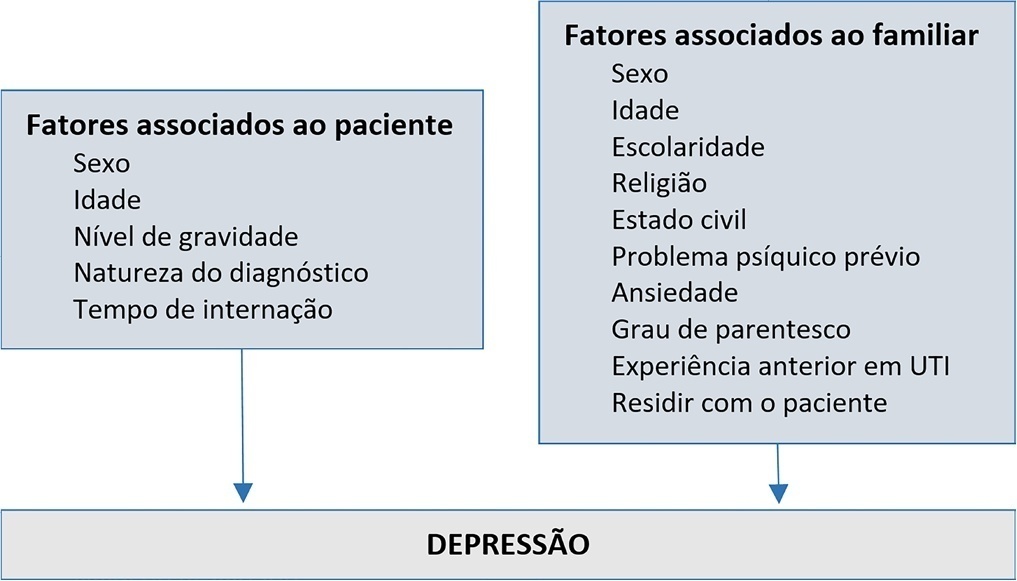
A cross-sectional study was conducted with 980 family members of patients admitted to the intensive care units of a large public hospital in the interior of Bahia. Depression was measured using the Patient Health Questionnaire-8. The multivariate model consisted of the following variables: sex and age of the patient, sex and age of the family member, education level, religion, living with the family member, previous mental illness and anxiety.
Depression had a prevalence of 43.5%. In the multivariate analysis, the model with the best representativeness indicated that factors associated with a higher prevalence of depression were being female (39%), age younger than 40 years (26%) and previous mental illness (38%). A higher education level was associated with a 19% lower prevalence of depression in family members.
The increase in the prevalence of depression was associated with female sex, age younger than 40 years and previous psychological problems. Such elements should be valued in actions aimed at family members of people hospitalized in intensive care.
Abstract
Rev Bras Ter Intensiva. 2022;34(4):499-506
DOI 10.5935/0103-507X.20220080-en
To evaluate the prevalence and factors associated with depression in family members of people hospitalized in intensive care units.
A cross-sectional study was conducted with 980 family members of patients admitted to the intensive care units of a large public hospital in the interior of Bahia. Depression was measured using the Patient Health Questionnaire-8. The multivariate model consisted of the following variables: sex and age of the patient, sex and age of the family member, education level, religion, living with the family member, previous mental illness and anxiety.
Depression had a prevalence of 43.5%. In the multivariate analysis, the model with the best representativeness indicated that factors associated with a higher prevalence of depression were being female (39%), age younger than 40 years (26%) and previous mental illness (38%). A higher education level was associated with a 19% lower prevalence of depression in family members.
The increase in the prevalence of depression was associated with female sex, age younger than 40 years and previous psychological problems. Such elements should be valued in actions aimed at family members of people hospitalized in intensive care.
Abstract
Rev Bras Ter Intensiva. 2019;31(2):217-226
DOI 10.5935/0103-507X.20190036
To describe the implementation of a rapid response team in a large nonprofit hospital, indicating relevant issues for other initiatives in similar contexts, particularly in Latin America.
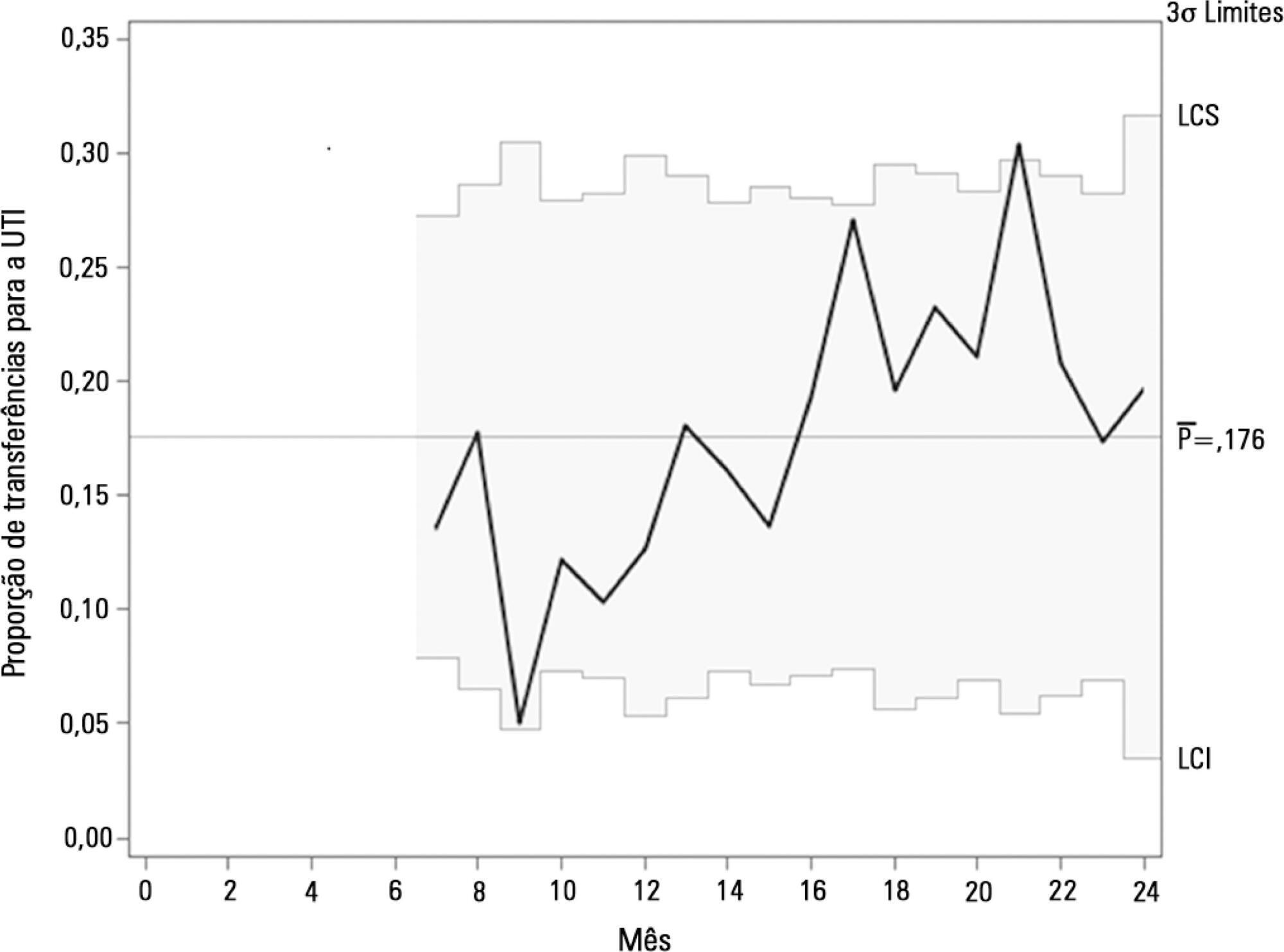
In general terms, the intervention consisted of three major components: (1) a tool to detect aggravation of clinical conditions in general wards; (2) the structuring of a rapid response team to attend to all patients at risk; and (3) the monitoring of indicators regarding the intervention. This work employed four half-year Plan-Do-Study-Act cycles to test and adjust the intervention from January 2013 to December 2014.
Between 2013 and 2014, the rapid response team attended to 2,296 patients. This study showed a nonsignificant reduction in mortality from 8.3% in cycle 1 to 5.0% in cycle 4; however, death rates remained stable in cycles 3 and 4, with frequencies of 5.2% and 5.0%, respectively. Regarding patient flow and continuum of critical care, which is a premise of the rapid response system, there was a reduction in waiting time for intensive care unit beds with a decrease from 45.9% to 19.0% in the frequency of inpatients who could not be admitted immediately after indication (p < 0.001), representing improved patient flow in the hospital. In addition, an increase in the recognition of palliative care patients from 2.8% to 10.3% was noted (p = 0.005).
Implementing a rapid response team in contexts where there are structural restrictions, such as lack of intensive care unit beds, may be very beneficial, but a strategy of adjustment is needed.
Abstract
Rev Bras Ter Intensiva. 2019;31(2):217-226
DOI 10.5935/0103-507X.20190036
To describe the implementation of a rapid response team in a large nonprofit hospital, indicating relevant issues for other initiatives in similar contexts, particularly in Latin America.
In general terms, the intervention consisted of three major components: (1) a tool to detect aggravation of clinical conditions in general wards; (2) the structuring of a rapid response team to attend to all patients at risk; and (3) the monitoring of indicators regarding the intervention. This work employed four half-year Plan-Do-Study-Act cycles to test and adjust the intervention from January 2013 to December 2014.
Between 2013 and 2014, the rapid response team attended to 2,296 patients. This study showed a nonsignificant reduction in mortality from 8.3% in cycle 1 to 5.0% in cycle 4; however, death rates remained stable in cycles 3 and 4, with frequencies of 5.2% and 5.0%, respectively. Regarding patient flow and continuum of critical care, which is a premise of the rapid response system, there was a reduction in waiting time for intensive care unit beds with a decrease from 45.9% to 19.0% in the frequency of inpatients who could not be admitted immediately after indication (p < 0.001), representing improved patient flow in the hospital. In addition, an increase in the recognition of palliative care patients from 2.8% to 10.3% was noted (p = 0.005).
Implementing a rapid response team in contexts where there are structural restrictions, such as lack of intensive care unit beds, may be very beneficial, but a strategy of adjustment is needed.