-
Commentary
Mortality due to sepsis in Brazil in a real scenario: the Brazilian ICUs project
Rev Bras Ter Intensiva. 2019;31(1):1-4
Abstract
CommentaryMortality due to sepsis in Brazil in a real scenario: the Brazilian ICUs project
Rev Bras Ter Intensiva. 2019;31(1):1-4
DOI 10.5935/0103-507X.20190008
Views1Worldwide, the number of sepsis patients per year is estimated at 15 to 17 million, contributing to more than 5 million deaths annually.(–) In Brazil, recent publications have indicated an increase in the number of cases of this syndrome in late years.() Many factors have contributed to this trend, such as population growth and rising […]See moreViews1

Abstract
CommentaryMortality due to sepsis in Brazil in a real scenario: the Brazilian ICUs project
Rev Bras Ter Intensiva. 2019;31(1):1-4
DOI 10.5935/0103-507X.20190008
Views1Worldwide, the number of sepsis patients per year is estimated at 15 to 17 million, contributing to more than 5 million deaths annually.(–) In Brazil, recent publications have indicated an increase in the number of cases of this syndrome in late years.() Many factors have contributed to this trend, such as population growth and rising […]See more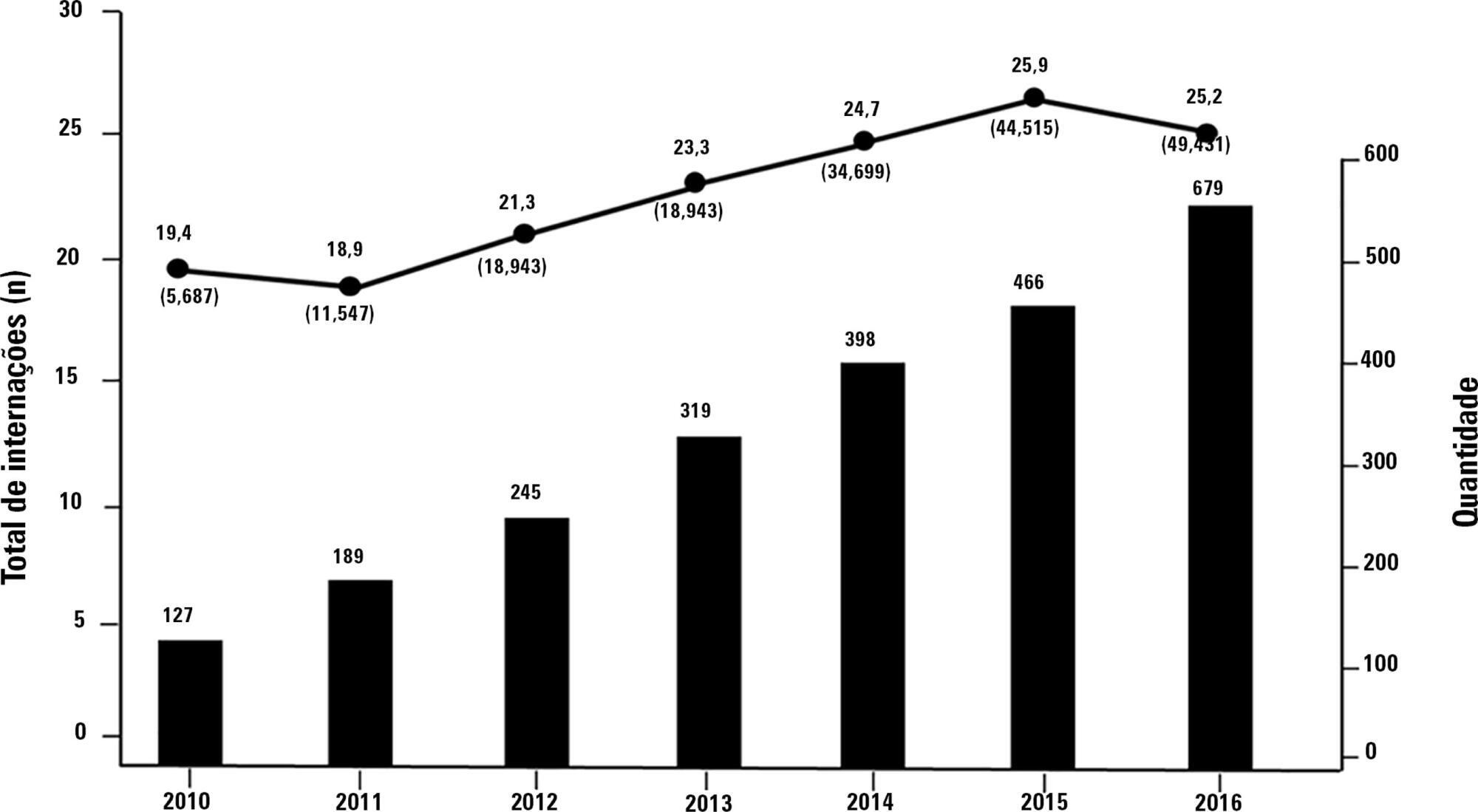
-
Special Article
Sociedade Portuguesa de Cuidados Intensivos guidelines for stress ulcer prophylaxis in the intensive care unit
Rev Bras Ter Intensiva. 2019;31(1):5-14
Abstract
Special ArticleSociedade Portuguesa de Cuidados Intensivos guidelines for stress ulcer prophylaxis in the intensive care unit
Rev Bras Ter Intensiva. 2019;31(1):5-14
DOI 10.5935/0103-507X.20190002
Views0See moreABSTRACT
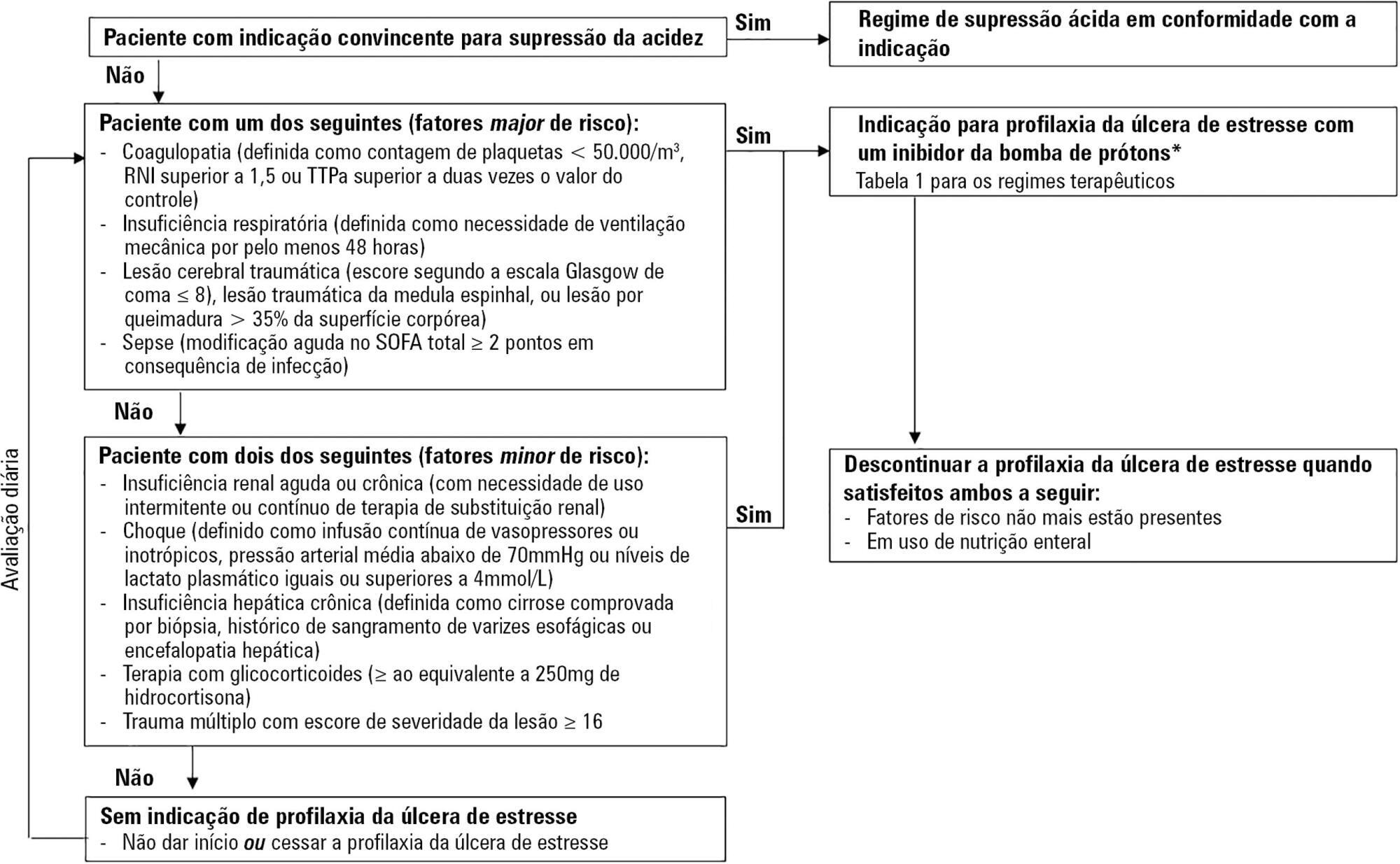
Critically ill patients are at risk of developing stress ulcers in the upper digestive tract. Agents that suppress gastric acid are commonly prescribed to reduce the incidence of clinically important stress ulcer-related gastrointestinal bleeding. However, the indiscriminate use of stress ulcer prophylaxis in all patients admitted to the intensive care unit is not warranted and can have potential adverse clinical effects and cost implications. The present guidelines from the Sociedade Portuguesa de Cuidados Intensivos summarizes the current evidence and gives six clinical statements and an algorithm aiming to provide a standardized prescribing policy for the use of stress ulcer prophylaxis in the intensive care unit.
Views0Abstract
Special ArticleSociedade Portuguesa de Cuidados Intensivos guidelines for stress ulcer prophylaxis in the intensive care unit
Rev Bras Ter Intensiva. 2019;31(1):5-14
DOI 10.5935/0103-507X.20190002
Views0See moreABSTRACT
Critically ill patients are at risk of developing stress ulcers in the upper digestive tract. Agents that suppress gastric acid are commonly prescribed to reduce the incidence of clinically important stress ulcer-related gastrointestinal bleeding. However, the indiscriminate use of stress ulcer prophylaxis in all patients admitted to the intensive care unit is not warranted and can have potential adverse clinical effects and cost implications. The present guidelines from the Sociedade Portuguesa de Cuidados Intensivos summarizes the current evidence and gives six clinical statements and an algorithm aiming to provide a standardized prescribing policy for the use of stress ulcer prophylaxis in the intensive care unit.
-
Original Article
Adverse events during intrahospital transport of critically ill patients in a large hospital
Rev Bras Ter Intensiva. 2019;31(1):15-20
Abstract
Original ArticleAdverse events during intrahospital transport of critically ill patients in a large hospital
Rev Bras Ter Intensiva. 2019;31(1):15-20
DOI 10.5935/0103-507X.20190003
Views1See moreABSTRACT
Objective:
To describe the incidence of clinical and non-clinical events during intrahospital transport of critically ill patients and to analyze the associated risk factors.
Methods:
Cohort study with retrospective data collected from October 2016 to October 2017. All cases of intrahospital transport for diagnostic and therapeutic purposes in a large hospital with six adult intensive care units were analyzed, and the adverse events and related risk factors were evaluated.
Results:
During the study period, 1,559 intrahospital transports were performed with 1,348 patients, with a mean age of 66 ± 17 years and a mean transport time of 43 ± 34 minutes. During transport, 19.8% of the patients were using vasoactive drugs; 13.7% were under sedation; and 10.6% were under mechanical ventilation. Clinical events occurred in 117 transports (7.5%), and non-clinical events occurred in 125 (8.0%) transports. Communication failures were prevalent; however, the multivariate analysis showed that the use of sedatives, noradrenaline and nitroprusside and a transport time greater than 36.5 minutes were associated with adverse clinical events. The use of dobutamine and a transport time greater than 36.5 minutes were associated with non-clinical events. At the end of transport, 98.1% of the patients presented unchanged clinical conditions compared with baseline.
Conclusion:
Intrahospital transport is related to a high incidence of adverse events, and transport time and the use of sedatives and vasoactive drugs were related to these events.
Views1Abstract
Original ArticleAdverse events during intrahospital transport of critically ill patients in a large hospital
Rev Bras Ter Intensiva. 2019;31(1):15-20
DOI 10.5935/0103-507X.20190003
Views1See moreABSTRACT
Objective:
To describe the incidence of clinical and non-clinical events during intrahospital transport of critically ill patients and to analyze the associated risk factors.
Methods:
Cohort study with retrospective data collected from October 2016 to October 2017. All cases of intrahospital transport for diagnostic and therapeutic purposes in a large hospital with six adult intensive care units were analyzed, and the adverse events and related risk factors were evaluated.
Results:
During the study period, 1,559 intrahospital transports were performed with 1,348 patients, with a mean age of 66 ± 17 years and a mean transport time of 43 ± 34 minutes. During transport, 19.8% of the patients were using vasoactive drugs; 13.7% were under sedation; and 10.6% were under mechanical ventilation. Clinical events occurred in 117 transports (7.5%), and non-clinical events occurred in 125 (8.0%) transports. Communication failures were prevalent; however, the multivariate analysis showed that the use of sedatives, noradrenaline and nitroprusside and a transport time greater than 36.5 minutes were associated with adverse clinical events. The use of dobutamine and a transport time greater than 36.5 minutes were associated with non-clinical events. At the end of transport, 98.1% of the patients presented unchanged clinical conditions compared with baseline.
Conclusion:
Intrahospital transport is related to a high incidence of adverse events, and transport time and the use of sedatives and vasoactive drugs were related to these events.
-
Original Article
Pharmacological and nonpharmacological measures of pain management and treatment among neonates
Rev Bras Ter Intensiva. 2019;31(1):21-26
Abstract
Original ArticlePharmacological and nonpharmacological measures of pain management and treatment among neonates
Rev Bras Ter Intensiva. 2019;31(1):21-26
DOI 10.5935/0103-507X.20190007
Views0ABSTRACT
Objective:
This study sought to describe and quantify the pharmacological and nonpharmacological strategies used to relieve the pain/stress of neonates during hospitalization in neonatal intensive care units.
Methods:
This quantitative, longitudinal, and descriptive study examined 50 neonates from neonatal intensive care unit admission to discharge.
Results:
A total of 9,948 painful/stressful procedures were recorded (mean = 11.25 ± 6.3) per day per neonate. A total of 11,722 pain-management and relief interventions were performed, of which 11,495 (98.1%) were nonpharmacological strategies, and 227 (1.9%) were pharmacological interventions. On average, each neonate received 235 pain-management and treatment interventions during hospitalization, 13 nonpharmacological interventions per day, and one pharmacological intervention every 2 days.
Conclusion:
Neonates receive few specific measures for pain relief given the high number of painful and stressful procedures performed during hospitalization. Thus, it is essential to implement effective pain-relief protocols.
Keywords:analgesiadrug therapyInfant, newbornIntensive care units, neonatalNeonatal nursingPain managementPain/prevention & controlSee moreViews0Abstract
Original ArticlePharmacological and nonpharmacological measures of pain management and treatment among neonates
Rev Bras Ter Intensiva. 2019;31(1):21-26
DOI 10.5935/0103-507X.20190007
Views0ABSTRACT
Objective:
This study sought to describe and quantify the pharmacological and nonpharmacological strategies used to relieve the pain/stress of neonates during hospitalization in neonatal intensive care units.
Methods:
This quantitative, longitudinal, and descriptive study examined 50 neonates from neonatal intensive care unit admission to discharge.
Results:
A total of 9,948 painful/stressful procedures were recorded (mean = 11.25 ± 6.3) per day per neonate. A total of 11,722 pain-management and relief interventions were performed, of which 11,495 (98.1%) were nonpharmacological strategies, and 227 (1.9%) were pharmacological interventions. On average, each neonate received 235 pain-management and treatment interventions during hospitalization, 13 nonpharmacological interventions per day, and one pharmacological intervention every 2 days.
Conclusion:
Neonates receive few specific measures for pain relief given the high number of painful and stressful procedures performed during hospitalization. Thus, it is essential to implement effective pain-relief protocols.
Keywords:analgesiadrug therapyInfant, newbornIntensive care units, neonatalNeonatal nursingPain managementPain/prevention & controlSee more -
Original Article
The Five Times Sit-to-Stand Test: safety and reliability with older intensive care unit patients at discharge
Rev Bras Ter Intensiva. 2019;31(1):27-33
Abstract
Original ArticleThe Five Times Sit-to-Stand Test: safety and reliability with older intensive care unit patients at discharge
Rev Bras Ter Intensiva. 2019;31(1):27-33
DOI 10.5935/0103-507X.20190006
Views1ABSTRACT
Objective:
Assess the Five Times Sit-to-Stand Test safety and clinimetric properties in older patients hospitalized in an intensive care unit.
Methods:
Test safety was assessed according to the incidence of adverse events and through hemodynamic and respiratory data. Additionally, reliability properties were investigated using the intraclass correlation coefficients, standard error of measurement, standard error percentage change, Altman-Bland plot and a survival agreement plot.
Results:
The overall suitability of the Five Times Sit-to-Stand Test was found to be low, with 29.8% meeting the inclusion criteria. Only 44% of the hospitalized patients who met the inclusion criteria performed the test, with no need for discontinuation in any patient. Heart rate (79.7 ± 10.2bpm/86.6 ± 9.7bpm; p = 0.001) and systolic blood pressure (118 ± 21.4mmHg/129 ± 21.5mmHg; p = 0.031) were the only variables that presented a significant statistical increase, with no evidence of exacerbated response to the test. Additionally, no adverse events were reported from participating and both test-retest and interrater reliability were high (intraclass correlation coefficient ≥ 0.99).
Conclusion:
The Five Times Sit-to-Stand Test was proven to be safe and to have excellent reliability. Its clinical use, however, may be restricted to high-functioning older adults in hospital settings.
Keywords:Accidental falls/prevention & controlAgedHospitalizationIntensive care unitsPatient dischargePhysical therapy modalitiesRehabilitationRisk assessmentSee moreViews1Abstract
Original ArticleThe Five Times Sit-to-Stand Test: safety and reliability with older intensive care unit patients at discharge
Rev Bras Ter Intensiva. 2019;31(1):27-33
DOI 10.5935/0103-507X.20190006
Views1ABSTRACT
Objective:
Assess the Five Times Sit-to-Stand Test safety and clinimetric properties in older patients hospitalized in an intensive care unit.
Methods:
Test safety was assessed according to the incidence of adverse events and through hemodynamic and respiratory data. Additionally, reliability properties were investigated using the intraclass correlation coefficients, standard error of measurement, standard error percentage change, Altman-Bland plot and a survival agreement plot.
Results:
The overall suitability of the Five Times Sit-to-Stand Test was found to be low, with 29.8% meeting the inclusion criteria. Only 44% of the hospitalized patients who met the inclusion criteria performed the test, with no need for discontinuation in any patient. Heart rate (79.7 ± 10.2bpm/86.6 ± 9.7bpm; p = 0.001) and systolic blood pressure (118 ± 21.4mmHg/129 ± 21.5mmHg; p = 0.031) were the only variables that presented a significant statistical increase, with no evidence of exacerbated response to the test. Additionally, no adverse events were reported from participating and both test-retest and interrater reliability were high (intraclass correlation coefficient ≥ 0.99).
Conclusion:
The Five Times Sit-to-Stand Test was proven to be safe and to have excellent reliability. Its clinical use, however, may be restricted to high-functioning older adults in hospital settings.
Keywords:Accidental falls/prevention & controlAgedHospitalizationIntensive care unitsPatient dischargePhysical therapy modalitiesRehabilitationRisk assessmentSee more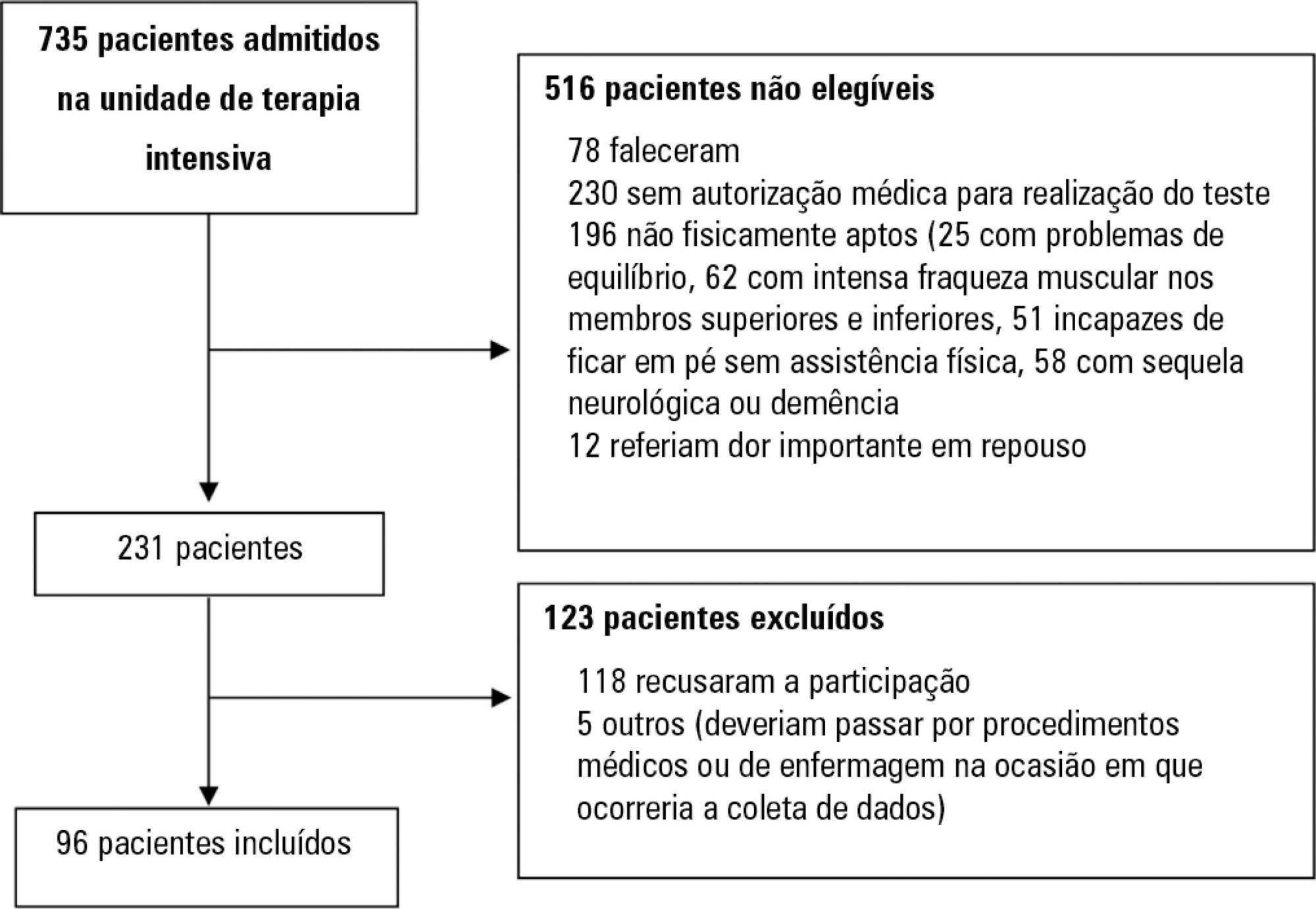
-
Original Article
Adequacy of enteral nutritional support in intensive care units does not affect the short- and long-term prognosis of mechanically ventilated patients: a pilot study
Rev Bras Ter Intensiva. 2019;31(1):34-38
Abstract
Original ArticleAdequacy of enteral nutritional support in intensive care units does not affect the short- and long-term prognosis of mechanically ventilated patients: a pilot study
Rev Bras Ter Intensiva. 2019;31(1):34-38
DOI 10.5935/0103-507X.20190004
Views0ABSTRACT
Objective:
To correlate short-term (duration of mechanical ventilation and length of intensive care unit stay) and long-term (functional capacity) clinical outcomes of patients who reached nutritional adequacy ≥ 70% of predicted in the first 72 hours of hospitalization in the intensive care unit.
Methods:
This was a prospective observational pilot study conducted in an 18-bed intensive care unit. A total of 100 mechanically ventilated patients receiving exclusive enteral nutritional support and receiving intensive care for more than 72 hours were included. Patients who never received enteral nutrition, those with spinal cord trauma, pregnant women, organ donors and cases of family refusal were excluded. The variables studied were nutritional adequacy ≥ 70% of predicted in the first 72 hours of hospitalization, length of intensive care unit stay, duration of mechanical ventilation and the ability to perform activities of daily living after 12 months, assessed via telephone contact using the Lawton Activities of Daily Living Scale.
Results:
The mean duration of mechanical ventilation was 18 ± 9 days, and the mean intensive care unit length of stay was 19 ± 8 days. Only 45% of the patients received more than 70% of the target nutrition in 72 hours. There was no association between nutritional adequacy and short-term (duration of mechanical ventilation, length of stay in the intensive care unit and mortality) or long-term (functional capacity and mortality) clinical outcomes.
Conclusion:
Critically ill patients receiving caloric intake ≥ 70% in the first 72 hours of hospitalization did not present better outcomes in the short term or after 1 year.
Keywords:Activities of daily livingCritical careCritical illnessEnergy requiremententeral nutritionIntensive care unitsNutritional supportRespiration, artificialSee moreViews0Abstract
Original ArticleAdequacy of enteral nutritional support in intensive care units does not affect the short- and long-term prognosis of mechanically ventilated patients: a pilot study
Rev Bras Ter Intensiva. 2019;31(1):34-38
DOI 10.5935/0103-507X.20190004
Views0ABSTRACT
Objective:
To correlate short-term (duration of mechanical ventilation and length of intensive care unit stay) and long-term (functional capacity) clinical outcomes of patients who reached nutritional adequacy ≥ 70% of predicted in the first 72 hours of hospitalization in the intensive care unit.
Methods:
This was a prospective observational pilot study conducted in an 18-bed intensive care unit. A total of 100 mechanically ventilated patients receiving exclusive enteral nutritional support and receiving intensive care for more than 72 hours were included. Patients who never received enteral nutrition, those with spinal cord trauma, pregnant women, organ donors and cases of family refusal were excluded. The variables studied were nutritional adequacy ≥ 70% of predicted in the first 72 hours of hospitalization, length of intensive care unit stay, duration of mechanical ventilation and the ability to perform activities of daily living after 12 months, assessed via telephone contact using the Lawton Activities of Daily Living Scale.
Results:
The mean duration of mechanical ventilation was 18 ± 9 days, and the mean intensive care unit length of stay was 19 ± 8 days. Only 45% of the patients received more than 70% of the target nutrition in 72 hours. There was no association between nutritional adequacy and short-term (duration of mechanical ventilation, length of stay in the intensive care unit and mortality) or long-term (functional capacity and mortality) clinical outcomes.
Conclusion:
Critically ill patients receiving caloric intake ≥ 70% in the first 72 hours of hospitalization did not present better outcomes in the short term or after 1 year.
Keywords:Activities of daily livingCritical careCritical illnessEnergy requiremententeral nutritionIntensive care unitsNutritional supportRespiration, artificialSee more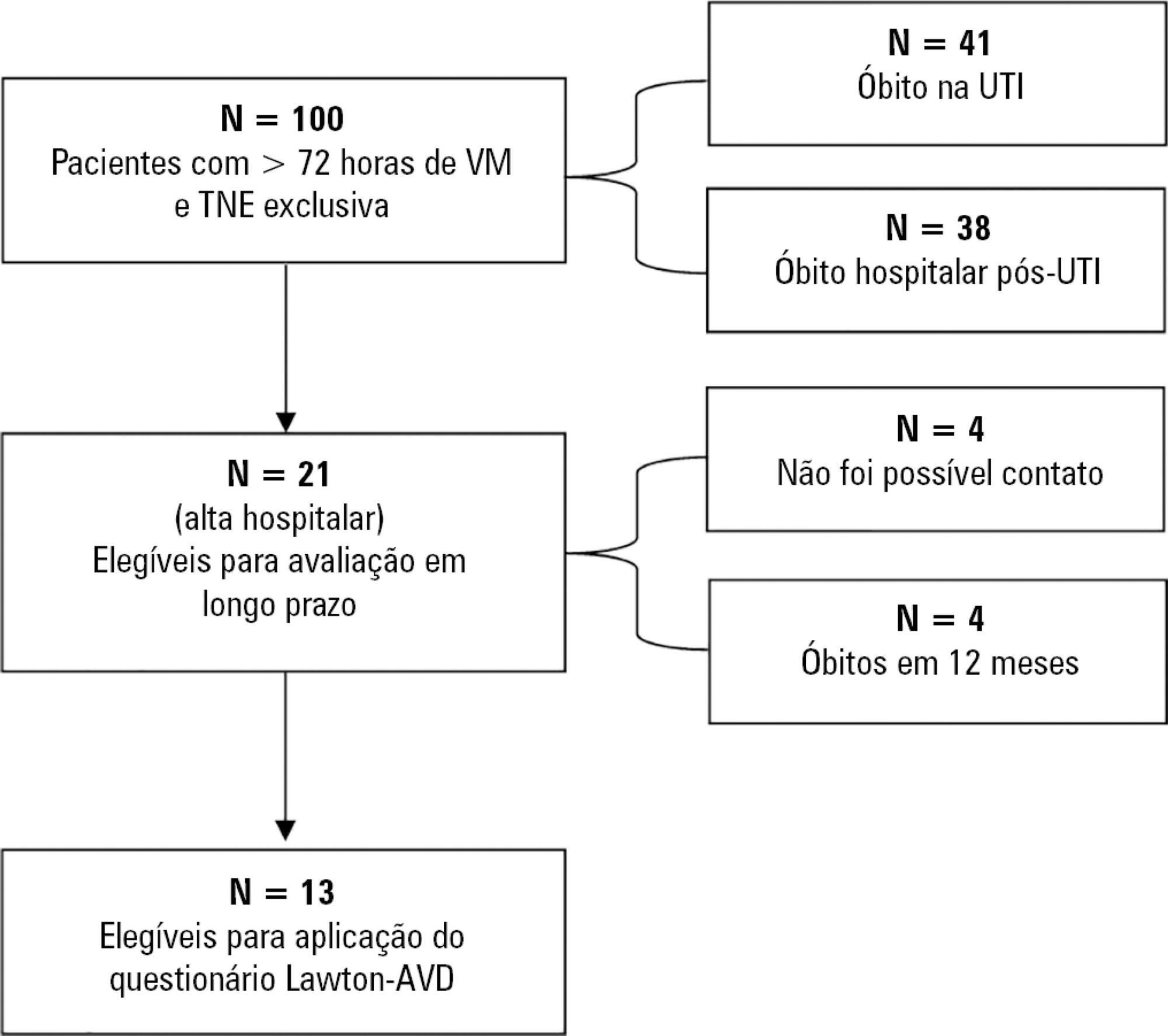
-
Original Article
Comparison of bronchial hygiene techniques in mechanically ventilated patients: a randomized clinical trial
Rev Bras Ter Intensiva. 2019;31(1):39-46
Abstract
Original ArticleComparison of bronchial hygiene techniques in mechanically ventilated patients: a randomized clinical trial
Rev Bras Ter Intensiva. 2019;31(1):39-46
DOI 10.5935/0103-507X.20190005
Views1ABSTRACT
Objective:
To compare the effects of vibrocompression and hyperinflation with mechanical ventilator techniques alone and in combination (hyperinflation with mechanical ventilator + vibrocompression) on the amount of aspirated secretion and the change in hemodynamic and pulmonary parameters.
Methods:
A randomized clinical trial with critically ill patients on mechanical ventilation conducted in the intensive care unit of a university hospital. The patients were randomly allocated to receive one of the bronchial hygiene techniques for 10 minutes (vibrocompression or hyperinflation with mechanical ventilator or hyperinflation with mechanical ventilator + vibrocompression). Afterwards, the patients were again randomly allocated to receive either the previous randomly allocated technique or only tracheal aspiration. The weight of aspirated secretions (in grams), ventilatory mechanics and cardiopulmonary data before and after the application of the techniques were analyzed. The tracheal reintubation frequency and time and mortality on mechanical ventilation were also evaluated.
Results:
A total of 93 patients (29 vibrocompression, 32 hyperinflation with mechanical ventilator and 32 hyperinflation with mechanical ventilator + vibrocompression) on mechanical ventilation for more than 24 hours were included. The hyperinflation with mechanical ventilator + vibrocompression group was the only one that presented a significant increase in aspirated secretions compared to tracheal aspiration alone [0.7g (0.1 – 2.5g) versus 0.2g (0.0 – 0.6g), p value = 0.006].
Conclusion:
Compared to tracheal aspiration alone, the combination of hyperinflation with mechanical ventilator + vibrocompression techniques was most efficient for increasing the amount of aspirated secretions.
Keywords:Bronchoalveolar lavageHygieneInsufflationPhysical therapy modalitiesRespiratory aspirationVentilators, mechanicalSee moreViews1Abstract
Original ArticleComparison of bronchial hygiene techniques in mechanically ventilated patients: a randomized clinical trial
Rev Bras Ter Intensiva. 2019;31(1):39-46
DOI 10.5935/0103-507X.20190005
Views1ABSTRACT
Objective:
To compare the effects of vibrocompression and hyperinflation with mechanical ventilator techniques alone and in combination (hyperinflation with mechanical ventilator + vibrocompression) on the amount of aspirated secretion and the change in hemodynamic and pulmonary parameters.
Methods:
A randomized clinical trial with critically ill patients on mechanical ventilation conducted in the intensive care unit of a university hospital. The patients were randomly allocated to receive one of the bronchial hygiene techniques for 10 minutes (vibrocompression or hyperinflation with mechanical ventilator or hyperinflation with mechanical ventilator + vibrocompression). Afterwards, the patients were again randomly allocated to receive either the previous randomly allocated technique or only tracheal aspiration. The weight of aspirated secretions (in grams), ventilatory mechanics and cardiopulmonary data before and after the application of the techniques were analyzed. The tracheal reintubation frequency and time and mortality on mechanical ventilation were also evaluated.
Results:
A total of 93 patients (29 vibrocompression, 32 hyperinflation with mechanical ventilator and 32 hyperinflation with mechanical ventilator + vibrocompression) on mechanical ventilation for more than 24 hours were included. The hyperinflation with mechanical ventilator + vibrocompression group was the only one that presented a significant increase in aspirated secretions compared to tracheal aspiration alone [0.7g (0.1 – 2.5g) versus 0.2g (0.0 – 0.6g), p value = 0.006].
Conclusion:
Compared to tracheal aspiration alone, the combination of hyperinflation with mechanical ventilator + vibrocompression techniques was most efficient for increasing the amount of aspirated secretions.
Keywords:Bronchoalveolar lavageHygieneInsufflationPhysical therapy modalitiesRespiratory aspirationVentilators, mechanicalSee more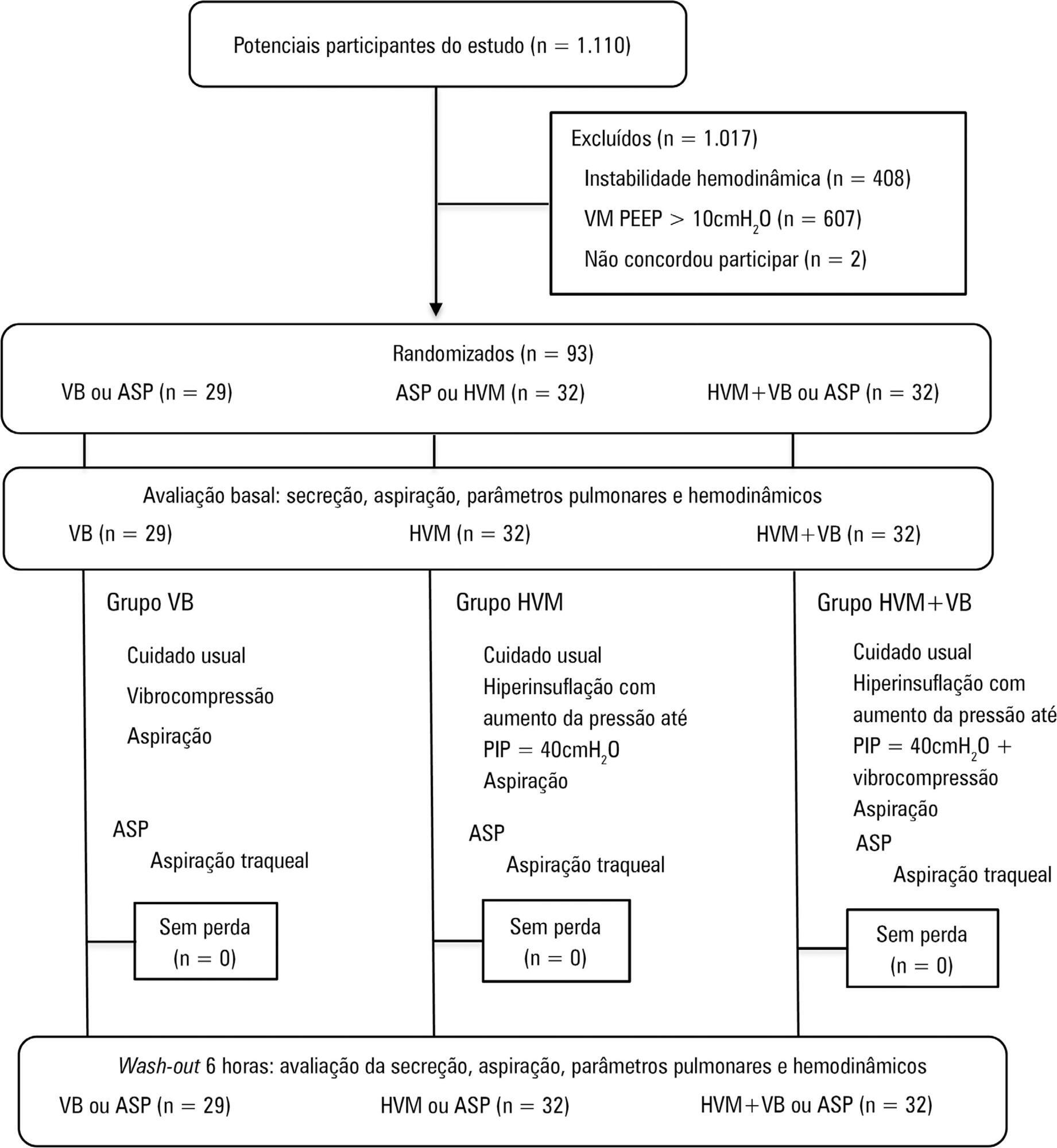
-
Original Articles
Association between site of infection and in-hospital mortality in patients with sepsis admitted to emergency departments of tertiary hospitals in Medellin, Colombia
Rev Bras Ter Intensiva. 2019;31(1):47-56
Abstract
Original ArticlesAssociation between site of infection and in-hospital mortality in patients with sepsis admitted to emergency departments of tertiary hospitals in Medellin, Colombia
Rev Bras Ter Intensiva. 2019;31(1):47-56
DOI 10.5935/0103-507X.20190011
Views1See moreABSTRACT
Objective:
To determine the association between the primary site of infection and in-hospital mortality as the main outcome, or the need for admission to the intensive care unit as a secondary outcome, in patients with sepsis admitted to the emergency department.
Methods:
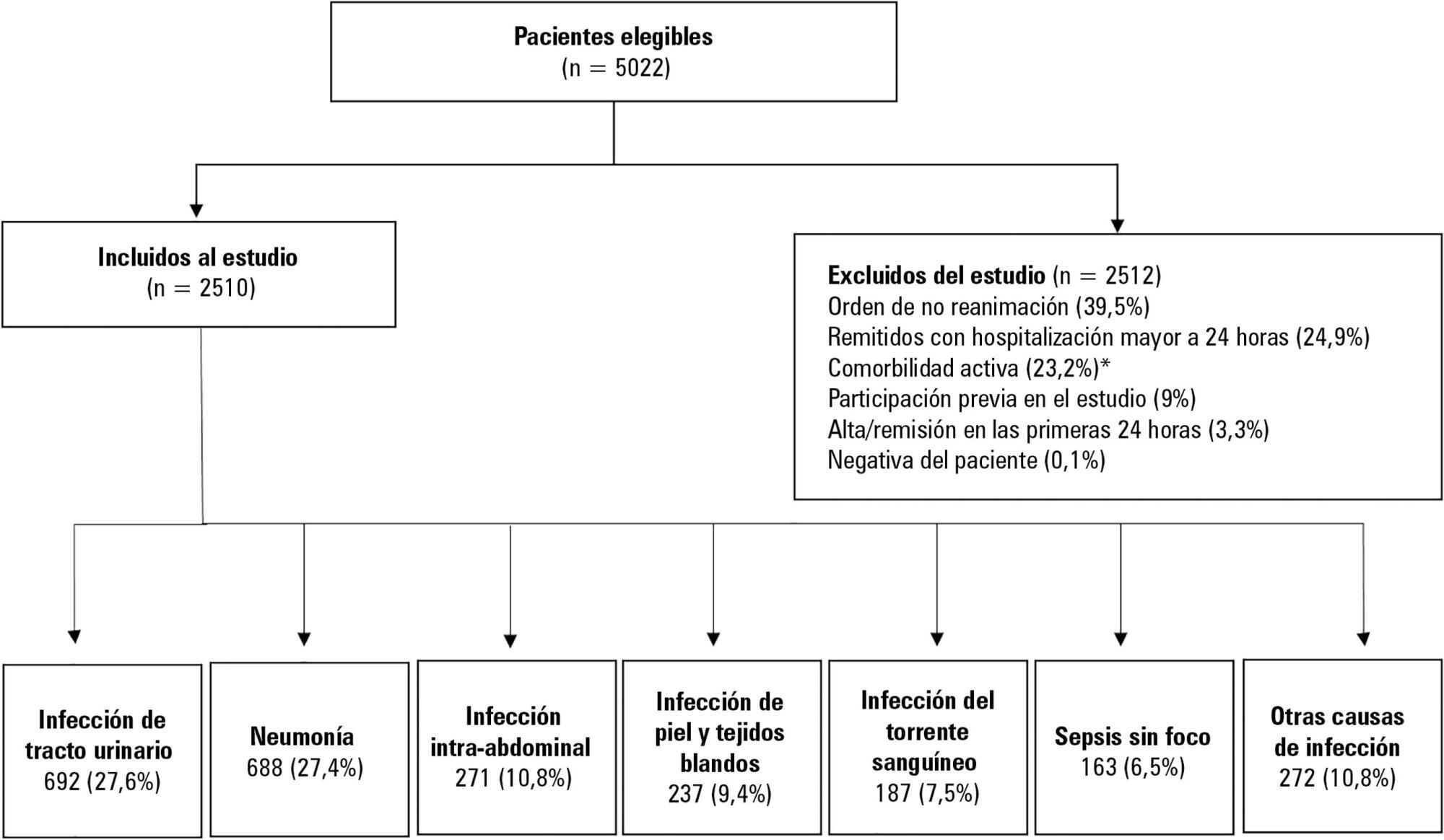
This was a secondary analysis of a multicenter prospective cohort. Patients included in the study were older than 18 years with a diagnosis of severe sepsis or septic shock who were admitted to the emergency departments of three tertiary care hospitals. Of the 5022 eligible participants, 2510 were included. Multiple logistic regression analysis was performed for mortality.
Results:
The most common site of infection was the urinary tract, present in 27.8% of the cases, followed by pneumonia (27.5%) and intra-abdominal focus (10.8%). In 5.4% of the cases, no definite site of infection was identified on admission. Logistic regression revealed a significant association between the following sites of infection and in-hospital mortality when using the urinary infection group as a reference: pneumonia (OR 3.4; 95%CI, 2.2 – 5.2; p < 0.001), skin and soft tissues (OR 2.6; 95%CI, 1.4 - 5.0; p = 0.003), bloodstream (OR 2.0; 95%CI, 1.1 - 3.6; p = 0.018), without specific focus (OR 2.0; 95%CI, 1.1 - 3.8; p = 0.028), and intra-abdominal focus (OR 1.9; 95%CI, 1.1 - 3.3; p = 0.024).
Conclusions:
There is a significant association between the different sites of infection and in-hospital mortality or the need for admission to an intensive care unit in patients with sepsis or septic shock. Urinary tract infection shows the lowest risk, which should be considered in prognostic models of these conditions.
Views1Abstract
Original ArticlesAssociation between site of infection and in-hospital mortality in patients with sepsis admitted to emergency departments of tertiary hospitals in Medellin, Colombia
Rev Bras Ter Intensiva. 2019;31(1):47-56
DOI 10.5935/0103-507X.20190011
Views1See moreABSTRACT
Objective:
To determine the association between the primary site of infection and in-hospital mortality as the main outcome, or the need for admission to the intensive care unit as a secondary outcome, in patients with sepsis admitted to the emergency department.
Methods:
This was a secondary analysis of a multicenter prospective cohort. Patients included in the study were older than 18 years with a diagnosis of severe sepsis or septic shock who were admitted to the emergency departments of three tertiary care hospitals. Of the 5022 eligible participants, 2510 were included. Multiple logistic regression analysis was performed for mortality.
Results:
The most common site of infection was the urinary tract, present in 27.8% of the cases, followed by pneumonia (27.5%) and intra-abdominal focus (10.8%). In 5.4% of the cases, no definite site of infection was identified on admission. Logistic regression revealed a significant association between the following sites of infection and in-hospital mortality when using the urinary infection group as a reference: pneumonia (OR 3.4; 95%CI, 2.2 – 5.2; p < 0.001), skin and soft tissues (OR 2.6; 95%CI, 1.4 - 5.0; p = 0.003), bloodstream (OR 2.0; 95%CI, 1.1 - 3.6; p = 0.018), without specific focus (OR 2.0; 95%CI, 1.1 - 3.8; p = 0.028), and intra-abdominal focus (OR 1.9; 95%CI, 1.1 - 3.3; p = 0.024).
Conclusions:
There is a significant association between the different sites of infection and in-hospital mortality or the need for admission to an intensive care unit in patients with sepsis or septic shock. Urinary tract infection shows the lowest risk, which should be considered in prognostic models of these conditions.
-
Original Articles
The Perme scale score as a predictor of functional status and complications after discharge from the intensive care unit in patients undergoing liver transplantation
Rev Bras Ter Intensiva. 2019;31(1):57-62
Abstract
Original ArticlesThe Perme scale score as a predictor of functional status and complications after discharge from the intensive care unit in patients undergoing liver transplantation
Rev Bras Ter Intensiva. 2019;31(1):57-62
DOI 10.5935/0103-507X.20190016
Views1ABSTRACT
Objective:
To assess the Perme mobility scale score as a predictor of functional status and complications in the postoperative period in patients undergoing liver transplantation.
Methods:
The sample consisted of 30 patients who underwent liver transplantation. The patients were evaluated at two time points to determine their perception of pain, degree of dyspnea, peripheral muscle strength, and functional status according to the Perme scale. The collected data were analyzed by descriptive and inferential statistics. To compare the means between the evaluations, Student’s t test for paired samples was applied. In case of asymmetry, the Wilcoxon test was used. In the evaluation of the association between the quantitative variables, the Pearson or Spearman correlation tests were applied.
Results:
A total of 30 individuals who underwent liver transplantation were included. The patients were predominantly male, and the mean age was 58.4 ± 9.9 years. The most prevalent underlying pathology was cirrhosis C virus (23.3%). Significant associations of the time on mechanical ventilation with the Perme scale score at discharge from the intensive care unit (r = -0.374; p = 0.042) and the number of physical therapy treatments (r = -0.578; p = 0.001) were recorded. When comparing the results of the initial evaluation and the evaluation at hospital discharge, there was a significant improvement in functional status (p < 0.001).
Conclusion:
Functional mobility, peripheral muscle strength, pain perception, and dyspnea are significantly improved at hospital discharge compared with those at inpatient unit admission.
Keywords:DyspneaLiver transplantationMobility limitationMuscle strengthPain measurementPostoperative complicationsSee moreViews1Abstract
Original ArticlesThe Perme scale score as a predictor of functional status and complications after discharge from the intensive care unit in patients undergoing liver transplantation
Rev Bras Ter Intensiva. 2019;31(1):57-62
DOI 10.5935/0103-507X.20190016
Views1ABSTRACT
Objective:
To assess the Perme mobility scale score as a predictor of functional status and complications in the postoperative period in patients undergoing liver transplantation.
Methods:
The sample consisted of 30 patients who underwent liver transplantation. The patients were evaluated at two time points to determine their perception of pain, degree of dyspnea, peripheral muscle strength, and functional status according to the Perme scale. The collected data were analyzed by descriptive and inferential statistics. To compare the means between the evaluations, Student’s t test for paired samples was applied. In case of asymmetry, the Wilcoxon test was used. In the evaluation of the association between the quantitative variables, the Pearson or Spearman correlation tests were applied.
Results:
A total of 30 individuals who underwent liver transplantation were included. The patients were predominantly male, and the mean age was 58.4 ± 9.9 years. The most prevalent underlying pathology was cirrhosis C virus (23.3%). Significant associations of the time on mechanical ventilation with the Perme scale score at discharge from the intensive care unit (r = -0.374; p = 0.042) and the number of physical therapy treatments (r = -0.578; p = 0.001) were recorded. When comparing the results of the initial evaluation and the evaluation at hospital discharge, there was a significant improvement in functional status (p < 0.001).
Conclusion:
Functional mobility, peripheral muscle strength, pain perception, and dyspnea are significantly improved at hospital discharge compared with those at inpatient unit admission.
Keywords:DyspneaLiver transplantationMobility limitationMuscle strengthPain measurementPostoperative complicationsSee more -
Original Article
Neutrophil-lymphocyte ratio in the early diagnosis of sepsis in an intensive care unit: a case-control study
Rev Bras Ter Intensiva. 2019;31(1):64-70
Abstract
Original ArticleNeutrophil-lymphocyte ratio in the early diagnosis of sepsis in an intensive care unit: a case-control study
Rev Bras Ter Intensiva. 2019;31(1):64-70
DOI 10.5935/0103-507X.20190010
Views0ABSTRACT
Objective:
To evaluate the neutrophil-lymphocyte ratio as a predictor of sepsis and mortality in patients admitted to an intensive care unit.
Methods:
Case-control study of adult patients admitted to an intensive care unit. Patients who had sepsis as the reason for admission and who had a previous complete blood count examination were included as case patients. The following statistical analyses were performed: ROC curves, binary logistic regression, and Mann-Whitney and Pearson’s chi-square tests. p < 0.05 was considered significant.
Results:
The ROC curve values were 0.62 for neutrophil-lymphocyte ratio, 0.98 for band neutrophils and 0.51 for total leukocytes. The presence of a neutrophil-lymphocyte ratio greater than 5.0, leukocyte count above 12,000mm3/mL and band neutrophil percentage above 10% were risk factors for sepsis; however, only the SAPS 3 and SOFA score were related to patient mortality.
Conclusion:
The neutrophil-lymphocyte ratio and band neutrophils in combination with other parameters may be markers for the early detection of sepsis in intensive care units.
Keywords:Blood cell countClinical laboratory techniquesIntensive care unitsLymphocyte count/methodsNeutrophilsSepsis/diagnosisSee moreViews0Abstract
Original ArticleNeutrophil-lymphocyte ratio in the early diagnosis of sepsis in an intensive care unit: a case-control study
Rev Bras Ter Intensiva. 2019;31(1):64-70
DOI 10.5935/0103-507X.20190010
Views0ABSTRACT
Objective:
To evaluate the neutrophil-lymphocyte ratio as a predictor of sepsis and mortality in patients admitted to an intensive care unit.
Methods:
Case-control study of adult patients admitted to an intensive care unit. Patients who had sepsis as the reason for admission and who had a previous complete blood count examination were included as case patients. The following statistical analyses were performed: ROC curves, binary logistic regression, and Mann-Whitney and Pearson’s chi-square tests. p < 0.05 was considered significant.
Results:
The ROC curve values were 0.62 for neutrophil-lymphocyte ratio, 0.98 for band neutrophils and 0.51 for total leukocytes. The presence of a neutrophil-lymphocyte ratio greater than 5.0, leukocyte count above 12,000mm3/mL and band neutrophil percentage above 10% were risk factors for sepsis; however, only the SAPS 3 and SOFA score were related to patient mortality.
Conclusion:
The neutrophil-lymphocyte ratio and band neutrophils in combination with other parameters may be markers for the early detection of sepsis in intensive care units.
Keywords:Blood cell countClinical laboratory techniquesIntensive care unitsLymphocyte count/methodsNeutrophilsSepsis/diagnosisSee more -
Original Articles
Characteristics and outcomes of patients with community-acquired and hospital-acquired sepsis
Rev Bras Ter Intensiva. 2019;31(1):71-78
Abstract
Original ArticlesCharacteristics and outcomes of patients with community-acquired and hospital-acquired sepsis
Rev Bras Ter Intensiva. 2019;31(1):71-78
DOI 10.5935/0103-507X.20190013
Views1See moreABSTRACT
Objective:
To compare the clinical characteristics and outcomes of patients with community-acquired and hospital-acquired sepsis.
Methods:
This is a retrospective cohort study that included all patients with a diagnosis of sepsis detected between January 2010 and December 2015 at a private hospital in southern Brazil. Outcomes (mortality, intensive care unit and hospital lengths of stay) were measured by analyzing electronic records.
Results:
There were 543 hospitalized patients with a diagnosis of sepsis, with a frequency of 90.5 (85 to 105) cases/year. Of these, 319 (58%) cases were classified as hospital-acquired sepsis. This group exhibited more severe disease and had a larger number of organ dysfunctions, with higher hospital [8 (8 – 10) versus 23 (20 – 27) days; p < 0.001] and intensive care unit [5 (4 - 7) versus 8.5 (7 – 10); p < 0.001] lengths of stay and higher in-hospital mortality (30.7% versus 15.6%; p < 0.001) than those with community-acquired sepsis. After adjusting for age, APACHE II scores, and hemodynamic and respiratory dysfunction, hospital-acquired sepsis remained associated with increased mortality (OR 1.96; 95%CI 1.15 - 3.32, p = 0.013).
Conclusion:
The present results contribute to the definition of the epidemiological profile of sepsis in the sample studied, in which hospital-acquired sepsis was more severe and was associated with higher mortality.
Views1Abstract
Original ArticlesCharacteristics and outcomes of patients with community-acquired and hospital-acquired sepsis
Rev Bras Ter Intensiva. 2019;31(1):71-78
DOI 10.5935/0103-507X.20190013
Views1See moreABSTRACT
Objective:
To compare the clinical characteristics and outcomes of patients with community-acquired and hospital-acquired sepsis.
Methods:
This is a retrospective cohort study that included all patients with a diagnosis of sepsis detected between January 2010 and December 2015 at a private hospital in southern Brazil. Outcomes (mortality, intensive care unit and hospital lengths of stay) were measured by analyzing electronic records.
Results:
There were 543 hospitalized patients with a diagnosis of sepsis, with a frequency of 90.5 (85 to 105) cases/year. Of these, 319 (58%) cases were classified as hospital-acquired sepsis. This group exhibited more severe disease and had a larger number of organ dysfunctions, with higher hospital [8 (8 – 10) versus 23 (20 – 27) days; p < 0.001] and intensive care unit [5 (4 - 7) versus 8.5 (7 – 10); p < 0.001] lengths of stay and higher in-hospital mortality (30.7% versus 15.6%; p < 0.001) than those with community-acquired sepsis. After adjusting for age, APACHE II scores, and hemodynamic and respiratory dysfunction, hospital-acquired sepsis remained associated with increased mortality (OR 1.96; 95%CI 1.15 - 3.32, p = 0.013).
Conclusion:
The present results contribute to the definition of the epidemiological profile of sepsis in the sample studied, in which hospital-acquired sepsis was more severe and was associated with higher mortality.
-
Original Articles
Incidence, risk factors, and outcomes of unplanned extubation in adult patients in a resource-limited teaching hospital in the Philippines: a cohort study
Rev Bras Ter Intensiva. 2019;31(1):79-85
Abstract
Original ArticlesIncidence, risk factors, and outcomes of unplanned extubation in adult patients in a resource-limited teaching hospital in the Philippines: a cohort study
Rev Bras Ter Intensiva. 2019;31(1):79-85
DOI 10.5935/0103-507X.20190012
Views0See moreABSTRACT
Objective:
We aimed to determine the incidence, risk factors, and outcomes of unplanned extubation among adult patients.
Methods:
We conducted a prospective cohort study of adult intubated patients admitted to the charity wards of a government tertiary teaching hospital in the Philippines. Patients managed in both intensive care and nonintensive care settings were included. Patients were followed-up until discharge or until seven days postextubation.
Results:
The outcomes of the 191 included patients were planned extubation (35%), unplanned extubation (19%), death (39%), and discharge against advice (7%). Competing risk regression showed that male sex (Crude OR: 2.25, 95%CI: 1.10 – 4.63) and age (Crude OR 0.976, 95%CI: 0.957 – 0.996) were significant baseline factors. The night shift (Crude OR: 24.6, 95%CI: 2.87 – 211) was also consistently associated with more unplanned extubations. Among postextubation outcomes, reintubation (unplanned extubation: 61.1% versus planned extubation: 25.4%), acute respiratory failure (unplanned extubation: 38.9% versus planned extubation: 17.5%), and cardiovascular events (unplanned extubation: 8.33% versus planned extubation: 1.49%) occurred significantly more often among the unplanned extubation patients. Admission in an intensive care unit was not associated with a lower risk of unplanned extubation (Crude OR 1.15, 95%CI: 0.594 – 2.21).
Conclusion:
Many intubated patients had unplanned extubation. Patients admitted in nonintensive care unit settings did not have significantly higher odds of unplanned extubation.
Views0Abstract
Original ArticlesIncidence, risk factors, and outcomes of unplanned extubation in adult patients in a resource-limited teaching hospital in the Philippines: a cohort study
Rev Bras Ter Intensiva. 2019;31(1):79-85
DOI 10.5935/0103-507X.20190012
Views0See moreABSTRACT
Objective:
We aimed to determine the incidence, risk factors, and outcomes of unplanned extubation among adult patients.
Methods:
We conducted a prospective cohort study of adult intubated patients admitted to the charity wards of a government tertiary teaching hospital in the Philippines. Patients managed in both intensive care and nonintensive care settings were included. Patients were followed-up until discharge or until seven days postextubation.
Results:
The outcomes of the 191 included patients were planned extubation (35%), unplanned extubation (19%), death (39%), and discharge against advice (7%). Competing risk regression showed that male sex (Crude OR: 2.25, 95%CI: 1.10 – 4.63) and age (Crude OR 0.976, 95%CI: 0.957 – 0.996) were significant baseline factors. The night shift (Crude OR: 24.6, 95%CI: 2.87 – 211) was also consistently associated with more unplanned extubations. Among postextubation outcomes, reintubation (unplanned extubation: 61.1% versus planned extubation: 25.4%), acute respiratory failure (unplanned extubation: 38.9% versus planned extubation: 17.5%), and cardiovascular events (unplanned extubation: 8.33% versus planned extubation: 1.49%) occurred significantly more often among the unplanned extubation patients. Admission in an intensive care unit was not associated with a lower risk of unplanned extubation (Crude OR 1.15, 95%CI: 0.594 – 2.21).
Conclusion:
Many intubated patients had unplanned extubation. Patients admitted in nonintensive care unit settings did not have significantly higher odds of unplanned extubation.
-
Original Article
Brain death-induced cytokine release is not associated with primary graft dysfunction: a cohort study
Rev Bras Ter Intensiva. 2019;31(1):86-92
Abstract
Original ArticleBrain death-induced cytokine release is not associated with primary graft dysfunction: a cohort study
Rev Bras Ter Intensiva. 2019;31(1):86-92
DOI 10.5935/0103-507X.20190009
Views1See moreABSTRACT
Objective:
To examine the association between donor plasma cytokine levels and the development of primary graft dysfunction of organs transplanted from deceased donors.
Methods:
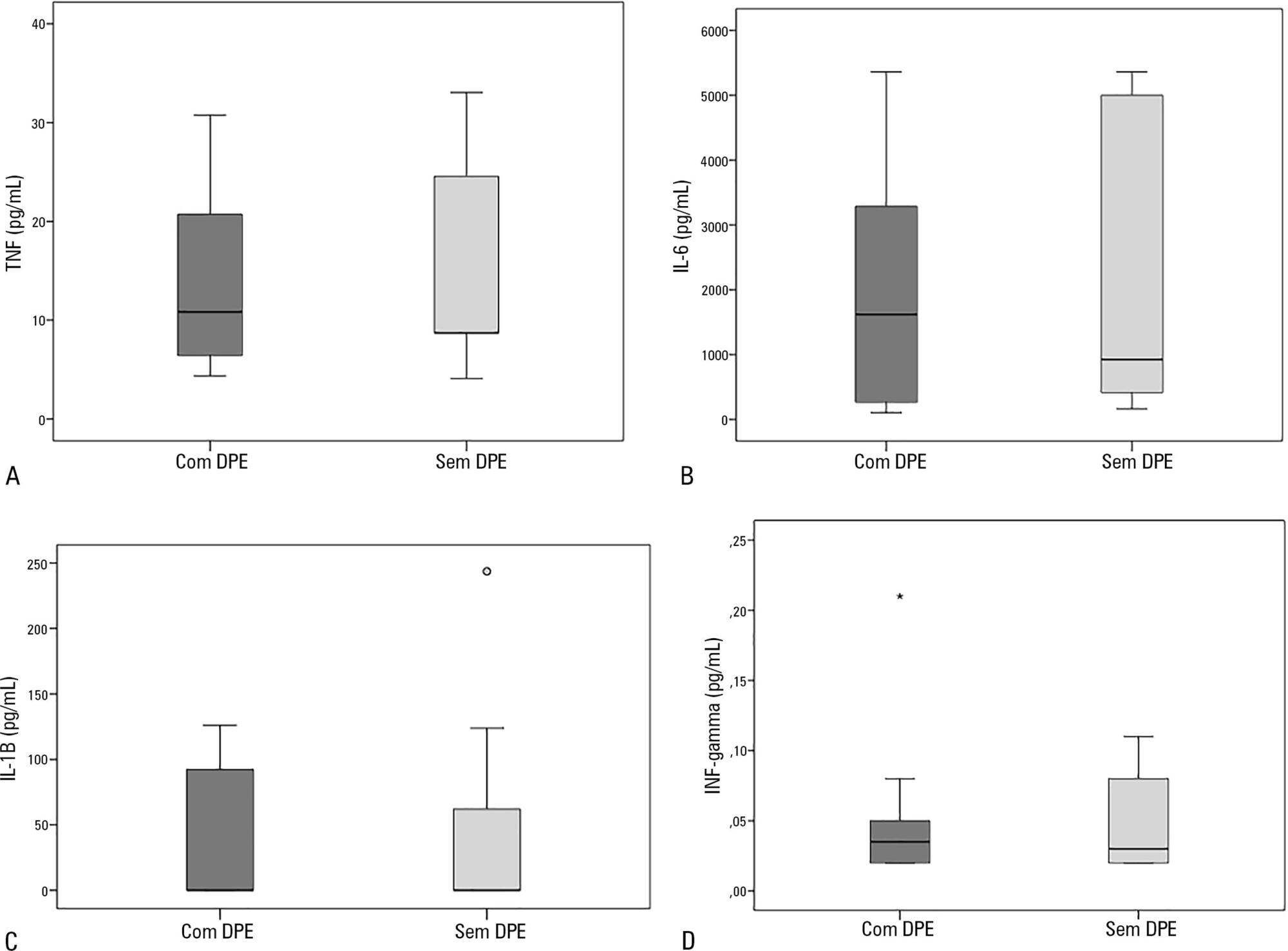
Seventeen deceased donors and the respective 47 transplant recipients were prospectively included in the study. Recipients were divided into two groups: group 1, patients who developed primary graft dysfunction; and group 2, patients who did not develop primary graft dysfunction. Donor plasma levels of TNF, IL-6, IL-1β, and IFN-γ assessed by ELISA were compared between groups.
Results:
Sixty-nine organs were retrieved, and 48 transplants were performed. Donor plasma cytokine levels did not differ between groups (in pg/mL): TNF, group 1: 10.8 (4.3 – 30.8) versus group 2: 8.7 (4.1 – 33.1), p = 0.63; IL-6, group 1: 1617.8 (106.7 – 5361.7) versus group 2: 922.9 (161.7 – 5361.7), p = 0.56; IL-1β, group 1: 0.1 (0.1 – 126.1) versus group 2: 0.1 (0.1 – 243.6), p = 0.60; and IFN-γ, group 1: 0.03 (0.02 – 0.2) versus group 2: 0.03 (0.02 – 0.1), p = 0.93). Similar findings were obtained when kidney transplants were analyzed separately.
Conclusion:
In this sample of transplant recipients, deceased donor plasma cytokines TNF, IL-6, IL-1β, and IFN-γ were not associated with the development of primary graft dysfunction.
Views1Abstract
Original ArticleBrain death-induced cytokine release is not associated with primary graft dysfunction: a cohort study
Rev Bras Ter Intensiva. 2019;31(1):86-92
DOI 10.5935/0103-507X.20190009
Views1See moreABSTRACT
Objective:
To examine the association between donor plasma cytokine levels and the development of primary graft dysfunction of organs transplanted from deceased donors.
Methods:
Seventeen deceased donors and the respective 47 transplant recipients were prospectively included in the study. Recipients were divided into two groups: group 1, patients who developed primary graft dysfunction; and group 2, patients who did not develop primary graft dysfunction. Donor plasma levels of TNF, IL-6, IL-1β, and IFN-γ assessed by ELISA were compared between groups.
Results:
Sixty-nine organs were retrieved, and 48 transplants were performed. Donor plasma cytokine levels did not differ between groups (in pg/mL): TNF, group 1: 10.8 (4.3 – 30.8) versus group 2: 8.7 (4.1 – 33.1), p = 0.63; IL-6, group 1: 1617.8 (106.7 – 5361.7) versus group 2: 922.9 (161.7 – 5361.7), p = 0.56; IL-1β, group 1: 0.1 (0.1 – 126.1) versus group 2: 0.1 (0.1 – 243.6), p = 0.60; and IFN-γ, group 1: 0.03 (0.02 – 0.2) versus group 2: 0.03 (0.02 – 0.1), p = 0.93). Similar findings were obtained when kidney transplants were analyzed separately.
Conclusion:
In this sample of transplant recipients, deceased donor plasma cytokines TNF, IL-6, IL-1β, and IFN-γ were not associated with the development of primary graft dysfunction.
-
Review Article
Challenges in high-sensitive troponin assay interpretation for intensive therapy
Rev Bras Ter Intensiva. 2019;31(1):93-105
Abstract
Review ArticleChallenges in high-sensitive troponin assay interpretation for intensive therapy
Rev Bras Ter Intensiva. 2019;31(1):93-105
DOI 10.5935/0103-507X.20190001
Views0See moreABSTRACT
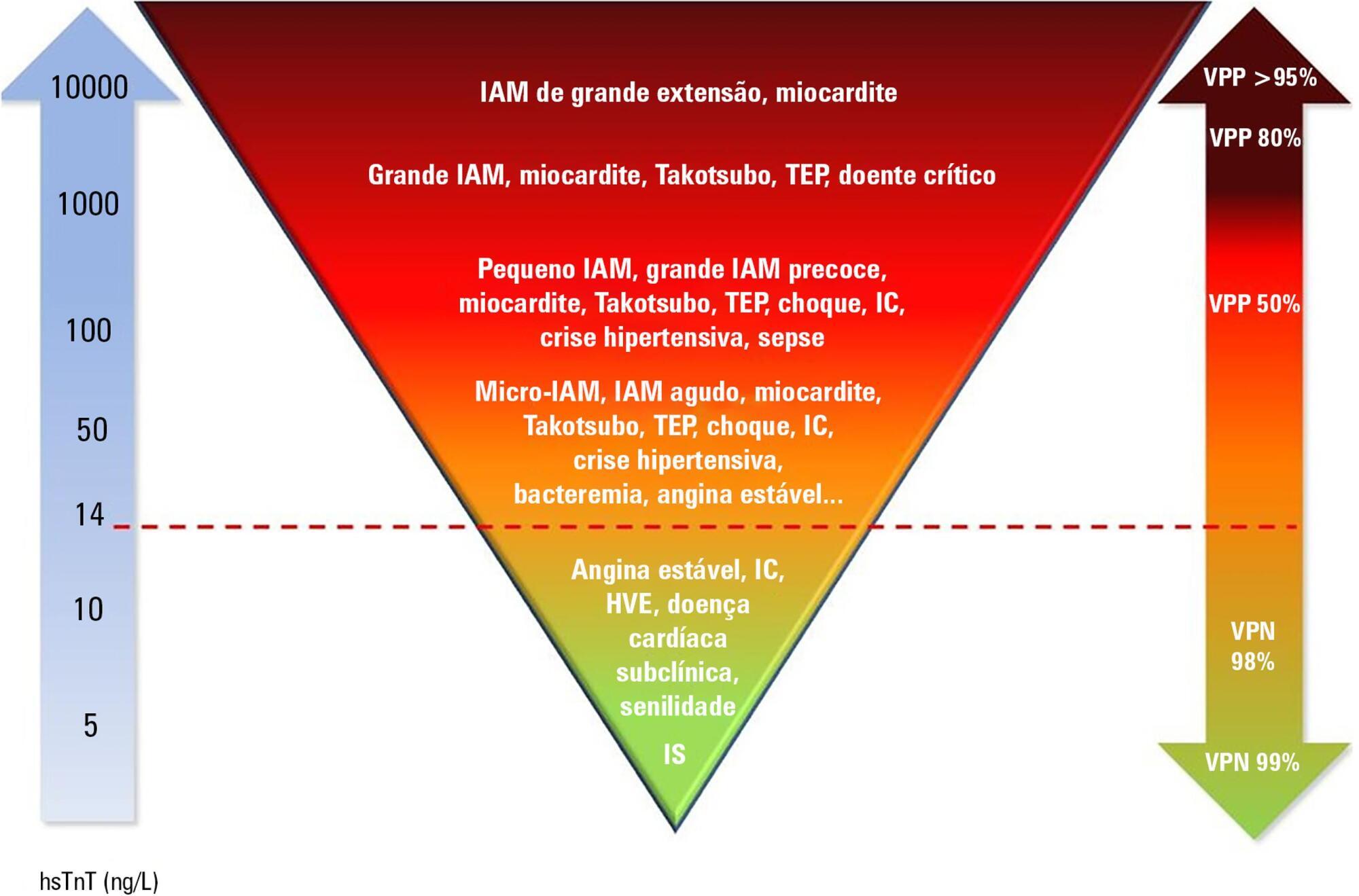
Cardiac troponins T and I are considered highly sensitive and specific markers for the diagnosis of acute myocardial infarction. Currently, a series of nonprimary cardiac abnormalities may manifest as an elevation in high-sensitive assays. The reduction in their detection limits has allowed earlier diagnosis and the use of evidence-based therapeutic measures; however, this characteristic has increased the spectrum of detectable noncoronary heart diseases, which poses challenges for characterizing acute coronary syndromes and creates a new role for these tests in known disorders in intensive care units, especially sepsis. Management of patients through a greater understanding of how these markers behave should be re-evaluated to ensure their correct interpretation.
Views0Abstract
Review ArticleChallenges in high-sensitive troponin assay interpretation for intensive therapy
Rev Bras Ter Intensiva. 2019;31(1):93-105
DOI 10.5935/0103-507X.20190001
Views0See moreABSTRACT
Cardiac troponins T and I are considered highly sensitive and specific markers for the diagnosis of acute myocardial infarction. Currently, a series of nonprimary cardiac abnormalities may manifest as an elevation in high-sensitive assays. The reduction in their detection limits has allowed earlier diagnosis and the use of evidence-based therapeutic measures; however, this characteristic has increased the spectrum of detectable noncoronary heart diseases, which poses challenges for characterizing acute coronary syndromes and creates a new role for these tests in known disorders in intensive care units, especially sepsis. Management of patients through a greater understanding of how these markers behave should be re-evaluated to ensure their correct interpretation.
-
Case Report
Optimization of conditions for apnea testing in a hypoxemic brain dead patient
Rev Bras Ter Intensiva. 2019;31(1):106-110
Abstract
Case ReportOptimization of conditions for apnea testing in a hypoxemic brain dead patient
Rev Bras Ter Intensiva. 2019;31(1):106-110
DOI 10.5935/0103-507X.20190015
Views0See moreABSTRACT
We report the case of a patient in whom brain death was suspected and associated with atelectasis and moderate to severe hypoxemia even though the patient was subjected to protective ventilation, a closed tracheal suction system, positive end-expiratory pressure, and recruitment maneuvers. Faced with the failure to obtain an adequate partial pressure of oxygen for the apnea test, we elected to place the patient in a prone position, use higher positive end-expiratory pressure, perform a new recruitment maneuver, and ventilate with a higher tidal volume (8mL/kg) without exceeding the plateau pressure of 30cmH2O. The apnea test was performed with the patient in a prone position, with continuous positive airway pressure coupled with a T-piece. The delay in diagnosis was 10 hours, and organ donation was not possible due to circulatory arrest. This report demonstrates the difficulties in obtaining higher levels of the partial pressure of oxygen for the apnea test. The delays in the diagnosis of brain death and in the organ donation process are discussed, as well as potential strategies to optimize the partial pressure of oxygen to perform the apnea test according to the current recommendations.
Views0Abstract
Case ReportOptimization of conditions for apnea testing in a hypoxemic brain dead patient
Rev Bras Ter Intensiva. 2019;31(1):106-110
DOI 10.5935/0103-507X.20190015
Views0See moreABSTRACT
We report the case of a patient in whom brain death was suspected and associated with atelectasis and moderate to severe hypoxemia even though the patient was subjected to protective ventilation, a closed tracheal suction system, positive end-expiratory pressure, and recruitment maneuvers. Faced with the failure to obtain an adequate partial pressure of oxygen for the apnea test, we elected to place the patient in a prone position, use higher positive end-expiratory pressure, perform a new recruitment maneuver, and ventilate with a higher tidal volume (8mL/kg) without exceeding the plateau pressure of 30cmH2O. The apnea test was performed with the patient in a prone position, with continuous positive airway pressure coupled with a T-piece. The delay in diagnosis was 10 hours, and organ donation was not possible due to circulatory arrest. This report demonstrates the difficulties in obtaining higher levels of the partial pressure of oxygen for the apnea test. The delays in the diagnosis of brain death and in the organ donation process are discussed, as well as potential strategies to optimize the partial pressure of oxygen to perform the apnea test according to the current recommendations.
-
Letter to the Editor
To: Long-term psychological outcome after discharge from intensive care
Rev Bras Ter Intensiva. 2019;31(1):111-112
Abstract
Letter to the EditorTo: Long-term psychological outcome after discharge from intensive care
Rev Bras Ter Intensiva. 2019;31(1):111-112
DOI 10.5935/0103-507X.20190014
Views1To the Editor,We read with great interest the article “Long-term psychological outcome after discharge from intensive care”, by Pereira et al. The authors performed a follow-up study of patients admitted to an intensive care unit (ICU) and evaluated the prevalence of long-term mental health outcomes as well as possible predictors during hospitalization.() The importance of […]See moreViews1Abstract
Letter to the EditorTo: Long-term psychological outcome after discharge from intensive care
Rev Bras Ter Intensiva. 2019;31(1):111-112
DOI 10.5935/0103-507X.20190014
Views1To the Editor,We read with great interest the article “Long-term psychological outcome after discharge from intensive care”, by Pereira et al. The authors performed a follow-up study of patients admitted to an intensive care unit (ICU) and evaluated the prevalence of long-term mental health outcomes as well as possible predictors during hospitalization.() The importance of […]See more
Volume Articles - Critical Care Science (CCS)
