-
Commentary
Sepsis is an important healthcare burden in Latin America: a call to action!
Rev Bras Ter Intensiva. 2018;30(4):402-404
Abstract
CommentarySepsis is an important healthcare burden in Latin America: a call to action!
Rev Bras Ter Intensiva. 2018;30(4):402-404
DOI 10.5935/0103-507X.20180061
Views0Sepsis is a life-threatening organ dysfunction caused by a dysregulated host response to infection. The precise incidence of sepsis is unknown and there is a lack of populational studies on the disease, especially from low and middle-income countries. However, extrapolations of populational data from high-income countries suggest a number of 30 million sepsis cases annually […]See moreViews0

Abstract
CommentarySepsis is an important healthcare burden in Latin America: a call to action!
Rev Bras Ter Intensiva. 2018;30(4):402-404
DOI 10.5935/0103-507X.20180061
Views0Sepsis is a life-threatening organ dysfunction caused by a dysregulated host response to infection. The precise incidence of sepsis is unknown and there is a lack of populational studies on the disease, especially from low and middle-income countries. However, extrapolations of populational data from high-income countries suggest a number of 30 million sepsis cases annually […]See more -
Original Article
Quality of life after intensive care unit: a multicenter cohort study protocol for assessment of long-term outcomes among intensive care survivors in Brazil
Rev Bras Ter Intensiva. 2018;30(4):405-413
Abstract
Original ArticleQuality of life after intensive care unit: a multicenter cohort study protocol for assessment of long-term outcomes among intensive care survivors in Brazil
Rev Bras Ter Intensiva. 2018;30(4):405-413
DOI 10.5935/0103-507X.20180063
Views0ABSTRACT
Objective:
To establish the prevalence of physical, cognitive and psychiatric disabilities, associated factors and their relationship with the qualities of life of intensive care survivors in Brazil.
Methods:
A prospective multicenter cohort study is currently being conducted at 10 adult medical-surgical intensive care units representative of the 5 Brazilian geopolitical regions. Patients aged ≥ 18 years who are discharged from the participating intensive care units and stay 72 hours or more in the intensive care unit for medical or emergency surgery admissions or 120 hours or more for elective surgery admissions are consecutively included. Patients are followed up for a period of one year by means of structured telephone interviews conducted at 3, 6 and 12 months after discharge from the intensive care unit. The outcomes are functional dependence, cognitive dysfunction, anxiety and depression symptoms, posttraumatic stress symptoms, health-related quality of life, rehospitalization and long-term mortality.
Discussion:
The present study has the potential to contribute to current knowledge of the prevalence and factors associated with postintensive care syndrome among adult intensive care survivors in Brazil. In addition, an association might be established between postintensive care syndrome and health-related quality of life.
Keywords:AnxietyCognitive dysfunctionCritical care outcomesDepressionDisabled personsQuality of lifeStress disorders, PosttraumaticSee moreViews0Abstract
Original ArticleQuality of life after intensive care unit: a multicenter cohort study protocol for assessment of long-term outcomes among intensive care survivors in Brazil
Rev Bras Ter Intensiva. 2018;30(4):405-413
DOI 10.5935/0103-507X.20180063
Views0ABSTRACT
Objective:
To establish the prevalence of physical, cognitive and psychiatric disabilities, associated factors and their relationship with the qualities of life of intensive care survivors in Brazil.
Methods:
A prospective multicenter cohort study is currently being conducted at 10 adult medical-surgical intensive care units representative of the 5 Brazilian geopolitical regions. Patients aged ≥ 18 years who are discharged from the participating intensive care units and stay 72 hours or more in the intensive care unit for medical or emergency surgery admissions or 120 hours or more for elective surgery admissions are consecutively included. Patients are followed up for a period of one year by means of structured telephone interviews conducted at 3, 6 and 12 months after discharge from the intensive care unit. The outcomes are functional dependence, cognitive dysfunction, anxiety and depression symptoms, posttraumatic stress symptoms, health-related quality of life, rehospitalization and long-term mortality.
Discussion:
The present study has the potential to contribute to current knowledge of the prevalence and factors associated with postintensive care syndrome among adult intensive care survivors in Brazil. In addition, an association might be established between postintensive care syndrome and health-related quality of life.
Keywords:AnxietyCognitive dysfunctionCritical care outcomesDepressionDisabled personsQuality of lifeStress disorders, PosttraumaticSee more
-
Original Article
An electronic warning system helps reduce the time to diagnosis of sepsis
Rev Bras Ter Intensiva. 2018;30(4):414-422
Abstract
Original ArticleAn electronic warning system helps reduce the time to diagnosis of sepsis
Rev Bras Ter Intensiva. 2018;30(4):414-422
DOI 10.5935/0103-507X.20180059
Views0See moreABSTRACT
Objective:
To describe the improvements of an early warning system for the identification of septic patients on the time to diagnosis, antibiotic delivery, and mortality.
Methods:
This was an observational cohort study that describes the successive improvements made over a period of 10 years using an early warning system to detect sepsis, including systematic active manual surveillance, electronic alerts via a telephonist, and alerts sent directly to the mobile devices of nurses. For all periods, after an alert was triggered, early treatment was instituted according to the institutional sepsis guidelines.
Results:
In total, 637 patients with sepsis were detected over the study period. The median triage-to-diagnosis time was reduced from 19:20 (9:10 – 38:15) hours to 12:40 (2:50 – 23:45) hours when the manual surveillance method was used (p = 0.14), to 2:10 (1:25 – 2:20) hours when the alert was sent automatically to the hospital telephone service (p = 0.014), and to 1:00 (0:30 – 1:10) hour when the alert was sent directly to the nurse’s mobile phone (p = 0.016). The diagnosis-to-antibiotic time was reduced to 1:00 (0:55 – 1:30) hours when the alert was sent to the telephonist and to 0:45 (0:30 – 1:00) minutes when the alert was sent directly to the nurse’s mobile phone (p = 0.02), with the maintenance of similar values over the following years. There was no difference in the time of treatment between survivors and non-survivors.
Conclusion:
Electronic systems help reduce the triage-to-diagnosis time and diagnosis-to-antibiotic time in patients with sepsis.
Views0Abstract
Original ArticleAn electronic warning system helps reduce the time to diagnosis of sepsis
Rev Bras Ter Intensiva. 2018;30(4):414-422
DOI 10.5935/0103-507X.20180059
Views0See moreABSTRACT
Objective:
To describe the improvements of an early warning system for the identification of septic patients on the time to diagnosis, antibiotic delivery, and mortality.
Methods:
This was an observational cohort study that describes the successive improvements made over a period of 10 years using an early warning system to detect sepsis, including systematic active manual surveillance, electronic alerts via a telephonist, and alerts sent directly to the mobile devices of nurses. For all periods, after an alert was triggered, early treatment was instituted according to the institutional sepsis guidelines.
Results:
In total, 637 patients with sepsis were detected over the study period. The median triage-to-diagnosis time was reduced from 19:20 (9:10 – 38:15) hours to 12:40 (2:50 – 23:45) hours when the manual surveillance method was used (p = 0.14), to 2:10 (1:25 – 2:20) hours when the alert was sent automatically to the hospital telephone service (p = 0.014), and to 1:00 (0:30 – 1:10) hour when the alert was sent directly to the nurse’s mobile phone (p = 0.016). The diagnosis-to-antibiotic time was reduced to 1:00 (0:55 – 1:30) hours when the alert was sent to the telephonist and to 0:45 (0:30 – 1:00) minutes when the alert was sent directly to the nurse’s mobile phone (p = 0.02), with the maintenance of similar values over the following years. There was no difference in the time of treatment between survivors and non-survivors.
Conclusion:
Electronic systems help reduce the triage-to-diagnosis time and diagnosis-to-antibiotic time in patients with sepsis.
-
Original Article
Use of vasopressin in the treatment of refractory septic shock
Rev Bras Ter Intensiva. 2018;30(4):423-428
Abstract
Original ArticleUse of vasopressin in the treatment of refractory septic shock
Rev Bras Ter Intensiva. 2018;30(4):423-428
DOI 10.5935/0103-507X.20180060
Views1See moreABSTRACT
Objective:
To evaluate the short-term evolution of patients with septic shock refractory to norepinephrine treated with vasopressin in an intensive care unit of a university hospital.
Methods:
An unmatched retrospective study (case series) was performed. Clinical, laboratory, and anthropometric data were collected from patients who received vasopressin infusion for treatment of catecholamine-refractory shock from December 2014 to June 2016. For the assessment of severity, APACHE II and SOFA scores were used. The main outcome was mortality at 3 and 30 days.
Results:
A total of 80 patients were included, of which 60% were male. In 86.3% of the cases, APACHE II was observed in the highest ranges (> 20). The 30-day mortality was 86.2%, and 75% of the patients died within 72 hours after starting vasopressin.
Conclusion:
The series evaluated had high mortality in the first 72 hours of treatment with vasopressin. The use of vasopressin in patients who are refractory to norepinephrine had little or no impact on mortality. It was not possible to exclude the possibility that the high mortality in the present study was linked to the relatively late onset (after established refractoriness of norepinephrine) of vasopressin; this hypothesis should be further evaluated in a randomized study.
Views1Abstract
Original ArticleUse of vasopressin in the treatment of refractory septic shock
Rev Bras Ter Intensiva. 2018;30(4):423-428
DOI 10.5935/0103-507X.20180060
Views1See moreABSTRACT
Objective:
To evaluate the short-term evolution of patients with septic shock refractory to norepinephrine treated with vasopressin in an intensive care unit of a university hospital.
Methods:
An unmatched retrospective study (case series) was performed. Clinical, laboratory, and anthropometric data were collected from patients who received vasopressin infusion for treatment of catecholamine-refractory shock from December 2014 to June 2016. For the assessment of severity, APACHE II and SOFA scores were used. The main outcome was mortality at 3 and 30 days.
Results:
A total of 80 patients were included, of which 60% were male. In 86.3% of the cases, APACHE II was observed in the highest ranges (> 20). The 30-day mortality was 86.2%, and 75% of the patients died within 72 hours after starting vasopressin.
Conclusion:
The series evaluated had high mortality in the first 72 hours of treatment with vasopressin. The use of vasopressin in patients who are refractory to norepinephrine had little or no impact on mortality. It was not possible to exclude the possibility that the high mortality in the present study was linked to the relatively late onset (after established refractoriness of norepinephrine) of vasopressin; this hypothesis should be further evaluated in a randomized study.
-
Original Article
Association between pediatric Risk, Injury, Failure, Loss and End Stage Renal Disease score and mortality in a pediatric intensive care unit: a retrospective study
Rev Bras Ter Intensiva. 2018;30(4):429-435
Abstract
Original ArticleAssociation between pediatric Risk, Injury, Failure, Loss and End Stage Renal Disease score and mortality in a pediatric intensive care unit: a retrospective study
Rev Bras Ter Intensiva. 2018;30(4):429-435
DOI 10.5935/0103-507X.20180065
Views0See moreABSTRACT
Objective:
To evaluate the association between acute kidney injury through the pediatric Risk, Injury, Failure, Loss and End Stage Renal Disease score and mortality in a pediatric intensive care unit.
Methods:
This retrospective cohort study assessed all children admitted to the pediatric intensive care unit of a reference hospital in Brazil from January to December 2016. Patients were screened for the presence of acute kidney injury through the pediatric Risk, Injury, Failure, Loss and End Stage Renal Disease score. Patients were subdivided into the stages of Risk, Injury and Kidney Failure.
Results:
The sample comprised 192 children, of whom 45.8% developed acute kidney injury, with 79.5% of the cases identified up to 72 hours after admission. Patients with acute kidney injury showed a 3.74 increase risk of death (p = 0.01) than the control group. Patients with kidney failure had a mortality rate that was 8.56 times greater than that of the remaining sample (p < 0.001). The variables that were associated with the stages of acute kidney injury were nephrotoxic drugs (p = 0.025), renal replacement therapy (p < 0.001), vasoactive drugs (p < 0.001), pediatric risk of mortality 2 score (p = 0.023), fluid overload (p = 0.005), pediatric intensive care unit length of stay (p = 0.001) and death (p < 0.001).
Conclusion:
In this study, the pediatric Risk, Injury, Failure, Loss and End Stage Renal Disease score proved to be a useful tool for the early identification of severely ill children with acute kidney injury, showing an association with mortality. We thus suggest its use for pediatric intensive care unit patient admission.
Views0Abstract
Original ArticleAssociation between pediatric Risk, Injury, Failure, Loss and End Stage Renal Disease score and mortality in a pediatric intensive care unit: a retrospective study
Rev Bras Ter Intensiva. 2018;30(4):429-435
DOI 10.5935/0103-507X.20180065
Views0See moreABSTRACT
Objective:
To evaluate the association between acute kidney injury through the pediatric Risk, Injury, Failure, Loss and End Stage Renal Disease score and mortality in a pediatric intensive care unit.
Methods:
This retrospective cohort study assessed all children admitted to the pediatric intensive care unit of a reference hospital in Brazil from January to December 2016. Patients were screened for the presence of acute kidney injury through the pediatric Risk, Injury, Failure, Loss and End Stage Renal Disease score. Patients were subdivided into the stages of Risk, Injury and Kidney Failure.
Results:
The sample comprised 192 children, of whom 45.8% developed acute kidney injury, with 79.5% of the cases identified up to 72 hours after admission. Patients with acute kidney injury showed a 3.74 increase risk of death (p = 0.01) than the control group. Patients with kidney failure had a mortality rate that was 8.56 times greater than that of the remaining sample (p < 0.001). The variables that were associated with the stages of acute kidney injury were nephrotoxic drugs (p = 0.025), renal replacement therapy (p < 0.001), vasoactive drugs (p < 0.001), pediatric risk of mortality 2 score (p = 0.023), fluid overload (p = 0.005), pediatric intensive care unit length of stay (p = 0.001) and death (p < 0.001).
Conclusion:
In this study, the pediatric Risk, Injury, Failure, Loss and End Stage Renal Disease score proved to be a useful tool for the early identification of severely ill children with acute kidney injury, showing an association with mortality. We thus suggest its use for pediatric intensive care unit patient admission.
-
Original Article
Risk factors for vascular catheter-related bloodstream infections in pediatric intensive care units
Rev Bras Ter Intensiva. 2018;30(4):436-442
Abstract
Original ArticleRisk factors for vascular catheter-related bloodstream infections in pediatric intensive care units
Rev Bras Ter Intensiva. 2018;30(4):436-442
DOI 10.5935/0103-507X.20180066
Views1ABSTRACT
Objectives:
To determine the risk factors for acquiring central line-associated blood stream infections (CLABSI) in pediatric intensive care units and to investigate the incidence and etiology of CLABSI in pediatric intensive care units with different profiles.
Methods:
The study was a prospective cohort study in three hospitals. One of the hospitals is a large metropolitan public hospital with two pediatric intensive care units and a total of nineteen pediatric intensive care unit beds, another is a regional hospital with eight pediatric intensive care unit beds, and the third is a private hospital with fifteen beds. Patients between the ages of 1 month old and 18 years old who used a central venous catheter for over 24 hours were included. We recorded patients’ daily progress. General patient and catheter-related data were collected and used as variables. All the data were analyzed using Statistical Package for Social Science (SPSS), version 13.0, to compare patients with CLABSI with or without risk factors.
Results:
A total of 728 patients were admitted to the pediatric intensive care units, and 170 had a central line in place for at least 24 hours. The median age was 32 months, and 97 (57%) of the patients were males. The CLABSI incidence rate was 3.9/1000 central venous catheter-days. The incidence among hospitals varied from 1.6 to 6.6. The overall mortality rate was 11.1%, and the CLABSI and non-CLABSI mortality rates were 12.9% and 10.7%, respectively. In multivariate analysis, independent risk factors for CLABSI were a longer duration of central venous catheter use (OR: 1.07; 95%CI 1.00 – 1.14; p = 0.019) and the use of more than one central venous catheter at once (OR: 2.59; 95%CI 1.17 – 5.73; p = 0.048).
Conclusion:
A longer duration of central venous catheter use and the use of more than one central venous catheter at once were the main risk factors for CLABSI in pediatric intensive care units.
Keywords:Catheter-related infectionsCatheterization, central venous/adverse effectscross infectionIntensive care units, pediatricrisk factorsSee moreViews1Abstract
Original ArticleRisk factors for vascular catheter-related bloodstream infections in pediatric intensive care units
Rev Bras Ter Intensiva. 2018;30(4):436-442
DOI 10.5935/0103-507X.20180066
Views1ABSTRACT
Objectives:
To determine the risk factors for acquiring central line-associated blood stream infections (CLABSI) in pediatric intensive care units and to investigate the incidence and etiology of CLABSI in pediatric intensive care units with different profiles.
Methods:
The study was a prospective cohort study in three hospitals. One of the hospitals is a large metropolitan public hospital with two pediatric intensive care units and a total of nineteen pediatric intensive care unit beds, another is a regional hospital with eight pediatric intensive care unit beds, and the third is a private hospital with fifteen beds. Patients between the ages of 1 month old and 18 years old who used a central venous catheter for over 24 hours were included. We recorded patients’ daily progress. General patient and catheter-related data were collected and used as variables. All the data were analyzed using Statistical Package for Social Science (SPSS), version 13.0, to compare patients with CLABSI with or without risk factors.
Results:
A total of 728 patients were admitted to the pediatric intensive care units, and 170 had a central line in place for at least 24 hours. The median age was 32 months, and 97 (57%) of the patients were males. The CLABSI incidence rate was 3.9/1000 central venous catheter-days. The incidence among hospitals varied from 1.6 to 6.6. The overall mortality rate was 11.1%, and the CLABSI and non-CLABSI mortality rates were 12.9% and 10.7%, respectively. In multivariate analysis, independent risk factors for CLABSI were a longer duration of central venous catheter use (OR: 1.07; 95%CI 1.00 – 1.14; p = 0.019) and the use of more than one central venous catheter at once (OR: 2.59; 95%CI 1.17 – 5.73; p = 0.048).
Conclusion:
A longer duration of central venous catheter use and the use of more than one central venous catheter at once were the main risk factors for CLABSI in pediatric intensive care units.
Keywords:Catheter-related infectionsCatheterization, central venous/adverse effectscross infectionIntensive care units, pediatricrisk factorsSee more -
Original Article
Role of interleukin-3 as a prognostic marker in septic patients
Rev Bras Ter Intensiva. 2018;30(4):443-452
Abstract
Original ArticleRole of interleukin-3 as a prognostic marker in septic patients
Rev Bras Ter Intensiva. 2018;30(4):443-452
DOI 10.5935/0103-507X.20180064
Views0See moreABSTRACT
Objective:
To evaluate the accuracy of IL-3 to predict the outcome of septic patients.
Methods:
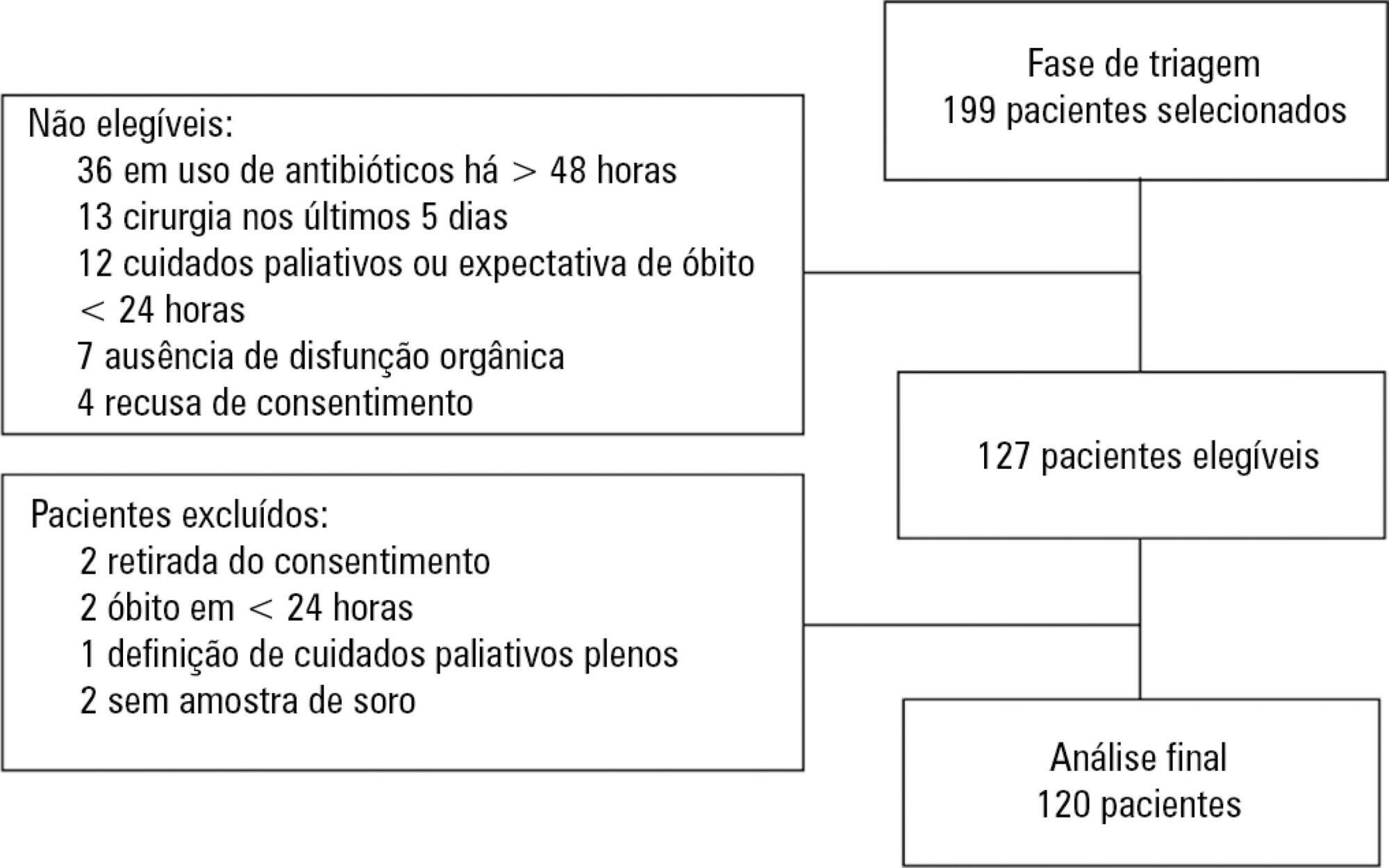
Prospective cohort study with adult patients in an intensive care unit with sepsis or septic shock diagnosed within the previous 48 hours. Circulating IL-3 levels were measured upon inclusion (day 1) and on days 3 and 7. The primary outcome was hospital mortality.
Results:
One hundred and twenty patients were included. Serum levels of IL-3 on day 1 were significantly higher among patients who died than among patients who survived the hospital stay (91.2pg/mL versus 36pg/mL, p = 0.024). In a Cox survival model considering the IL-3 levels at inclusion, age and sequential SOFA, IL-3 values remained independently associated with mortality (HR 1.032; 95%CI 1.010 – 1.055; p = 0.005). An receiver operating characteristic curve was built to further investigate the accuracy of IL-3, with an area under the curve of 0.62 (95%CI 0.51 – 0.73; p = 0.024) for hospital mortality. A cutoff initial IL-3 value above 127.5pg/mL was associated with hospital mortality (OR 2.97; 95%CI: 1.27 – 6.97; p = 0.0019) but with a low performance (82% for specificity, 39% for sensibility, 53% for the positive predictive value, 72% for the negative predictive value, 0.73 for the negative likelihood and 2.16 for the positive likelihood ratio).
Conclusion:
Higher levels of IL-3 are shown to be independently associated with hospital mortality in septic patients but with poor clinical performance.
Views0Abstract
Original ArticleRole of interleukin-3 as a prognostic marker in septic patients
Rev Bras Ter Intensiva. 2018;30(4):443-452
DOI 10.5935/0103-507X.20180064
Views0See moreABSTRACT
Objective:
To evaluate the accuracy of IL-3 to predict the outcome of septic patients.
Methods:
Prospective cohort study with adult patients in an intensive care unit with sepsis or septic shock diagnosed within the previous 48 hours. Circulating IL-3 levels were measured upon inclusion (day 1) and on days 3 and 7. The primary outcome was hospital mortality.
Results:
One hundred and twenty patients were included. Serum levels of IL-3 on day 1 were significantly higher among patients who died than among patients who survived the hospital stay (91.2pg/mL versus 36pg/mL, p = 0.024). In a Cox survival model considering the IL-3 levels at inclusion, age and sequential SOFA, IL-3 values remained independently associated with mortality (HR 1.032; 95%CI 1.010 – 1.055; p = 0.005). An receiver operating characteristic curve was built to further investigate the accuracy of IL-3, with an area under the curve of 0.62 (95%CI 0.51 – 0.73; p = 0.024) for hospital mortality. A cutoff initial IL-3 value above 127.5pg/mL was associated with hospital mortality (OR 2.97; 95%CI: 1.27 – 6.97; p = 0.0019) but with a low performance (82% for specificity, 39% for sensibility, 53% for the positive predictive value, 72% for the negative predictive value, 0.73 for the negative likelihood and 2.16 for the positive likelihood ratio).
Conclusion:
Higher levels of IL-3 are shown to be independently associated with hospital mortality in septic patients but with poor clinical performance.
-
Original Article
suPAR in the assessment of post intensive care unit prognosis: a pilot study
Rev Bras Ter Intensiva. 2018;30(4):453-459
Abstract
Original ArticlesuPAR in the assessment of post intensive care unit prognosis: a pilot study
Rev Bras Ter Intensiva. 2018;30(4):453-459
DOI 10.5935/0103-507X.20180062
Views0See moreABSTRACT
Objective:
To determine the performance of soluble urokinase-type plasminogen activator receptor upon intensive care unit discharge to predict post intensive care unit mortality.
Methods:
A prospective observational cohort study was conducted during a 24-month period in an 8-bed polyvalent intensive care unit. APACHE II, SOFA, C-reactive protein, white cell count and soluble urokinase-type plasminogen activator receptor on the day of intensive care unit discharge were collected from patients who survived intensive care unit admission.
Results:
Two hundred and two patients were included in this study, 29 patients (18.6%) of whom died after intensive care unit discharge. Nonsurvivors were older and more seriously ill upon intensive care unit admission with higher severity scores, and nonsurvivors required extended use of vasopressors than did survivors. The area under the receiver operating characteristics curves of SOFA, APACHE II, C-reactive protein, white cell count, and soluble urokinase-type plasminogen activator receptor at intensive care unit discharge as prognostic markers of hospital death were 0.78 (95%CI 0.70 – 0.86); 0.70 (95%CI 0.61 – 0.79); 0.54 (95%CI 0.42 – 0.65); 0.48 (95%CI 0.36 – 0.58); and 0.68 (95%CI 0.58 – 0.78), respectively. SOFA was independently associated with a higher risk of in-hospital mortality (OR 1.673; 95%CI 1.252 – 2.234), 28-day mortality (OR 1.861; 95%CI 1.856 – 2.555) and 90-day mortality (OR 1.584; 95%CI 1.241 – 2.022).
Conclusion:
At intensive care unit discharge, soluble urokinase-type plasminogen activator receptor is a poor predictor of post intensive care unit prognosis.
Views0Abstract
Original ArticlesuPAR in the assessment of post intensive care unit prognosis: a pilot study
Rev Bras Ter Intensiva. 2018;30(4):453-459
DOI 10.5935/0103-507X.20180062
Views0See moreABSTRACT
Objective:
To determine the performance of soluble urokinase-type plasminogen activator receptor upon intensive care unit discharge to predict post intensive care unit mortality.
Methods:
A prospective observational cohort study was conducted during a 24-month period in an 8-bed polyvalent intensive care unit. APACHE II, SOFA, C-reactive protein, white cell count and soluble urokinase-type plasminogen activator receptor on the day of intensive care unit discharge were collected from patients who survived intensive care unit admission.
Results:
Two hundred and two patients were included in this study, 29 patients (18.6%) of whom died after intensive care unit discharge. Nonsurvivors were older and more seriously ill upon intensive care unit admission with higher severity scores, and nonsurvivors required extended use of vasopressors than did survivors. The area under the receiver operating characteristics curves of SOFA, APACHE II, C-reactive protein, white cell count, and soluble urokinase-type plasminogen activator receptor at intensive care unit discharge as prognostic markers of hospital death were 0.78 (95%CI 0.70 – 0.86); 0.70 (95%CI 0.61 – 0.79); 0.54 (95%CI 0.42 – 0.65); 0.48 (95%CI 0.36 – 0.58); and 0.68 (95%CI 0.58 – 0.78), respectively. SOFA was independently associated with a higher risk of in-hospital mortality (OR 1.673; 95%CI 1.252 – 2.234), 28-day mortality (OR 1.861; 95%CI 1.856 – 2.555) and 90-day mortality (OR 1.584; 95%CI 1.241 – 2.022).
Conclusion:
At intensive care unit discharge, soluble urokinase-type plasminogen activator receptor is a poor predictor of post intensive care unit prognosis.
-
Original Article
The use of bedside echocardiography for measuring cardiac index and systemic vascular resistance in pediatric patients with septic shock
Rev Bras Ter Intensiva. 2018;30(4):460-470
Abstract
Original ArticleThe use of bedside echocardiography for measuring cardiac index and systemic vascular resistance in pediatric patients with septic shock
Rev Bras Ter Intensiva. 2018;30(4):460-470
DOI 10.5935/0103-507X.20180067
Views0See moreABSTRACT
Objective:
Follow-up of cardiac index and systemic vascular resistance index by bedside echocardiography until resuscitation.
Methods:
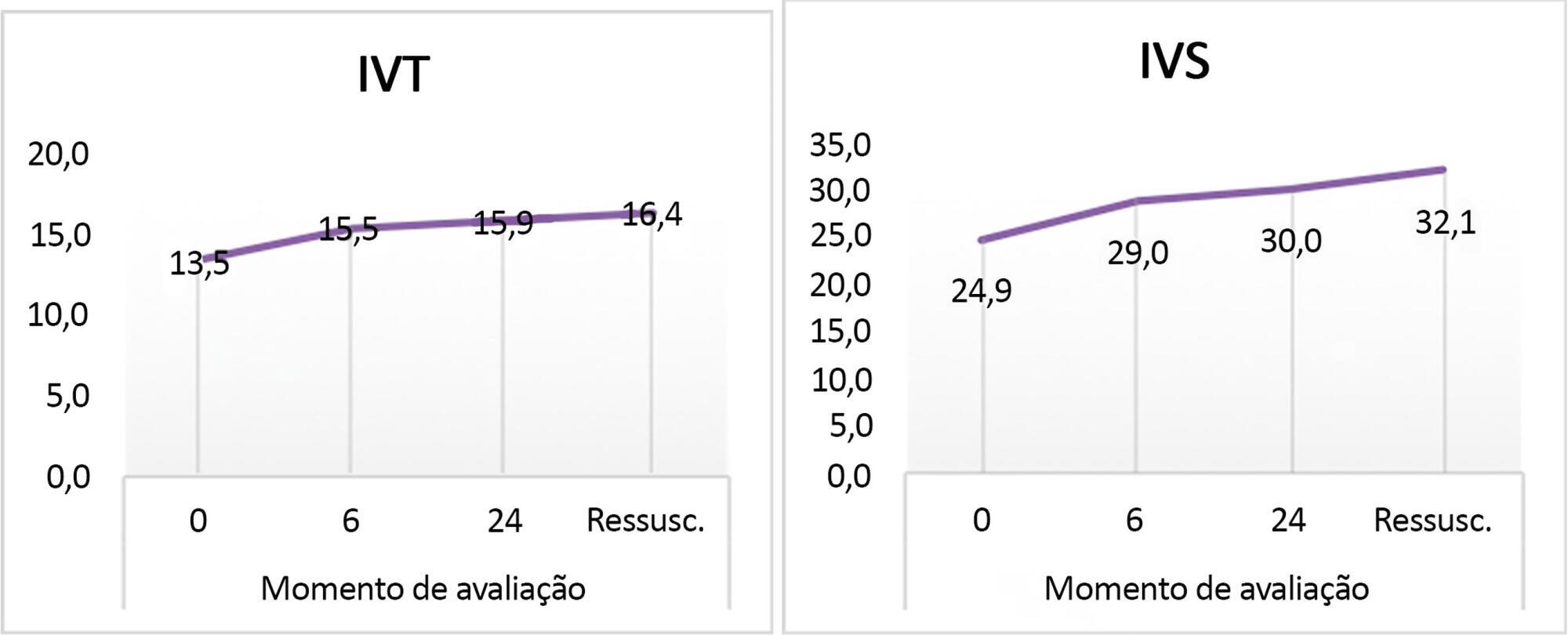
A set of hemodynamic parameters was obtained, including cardiac output, stroke volume, cardiac index, systemic vascular resistance index, velocity time integral, myocardial performance index, capillary refill time, and heart rate at 0 hours after fluid boluses before the start of inotropes, and followed up after 6 hours and 24 hours.
Results:
Included were 45 patients with community-acquired septic shock. Septic foci were gastroenteritis (24%), intestinal perforation requiring emergency surgery (24%), pneumonia (20%), central nervous system infection (22%) and soft tissue infection (8%). Klebsiella and Enterobacter were the most frequent isolates. We estimated the factors affecting the cardiac index: high central venous pressure at zero time (r = 0.33, p = 0.024) and persistently high heart rate at hour 6 (r = 0.33, p = 0.03). The systemic vascular resistance index was high in most patients at 0 and 24 hours and at the time of resuscitation and inversely affected the cardiac index as well as affecting the velocity time integral (r = -0.416, -0.61, 0.55 and -0.295). Prolonged capillary refill time was a clinical predictor of the low velocity time integral at 24 hours (r = -0.4). The mortality was 27%. Lower systemic vascular resistance index and higher cardiac output were observed in nonsurviving patients.
Conclusion:
There was a persistently high systemic vascular resistance index in cold shock patients that influenced the stroke volume index, cardiac index, and velocity time integral. The use of echocardiograms for hemodynamic measurements is important in pediatric septic shock patients to adjust dilators, and vasopressor doses and achieve resuscitation targets in a timely manner.
Views0Abstract
Original ArticleThe use of bedside echocardiography for measuring cardiac index and systemic vascular resistance in pediatric patients with septic shock
Rev Bras Ter Intensiva. 2018;30(4):460-470
DOI 10.5935/0103-507X.20180067
Views0See moreABSTRACT
Objective:
Follow-up of cardiac index and systemic vascular resistance index by bedside echocardiography until resuscitation.
Methods:
A set of hemodynamic parameters was obtained, including cardiac output, stroke volume, cardiac index, systemic vascular resistance index, velocity time integral, myocardial performance index, capillary refill time, and heart rate at 0 hours after fluid boluses before the start of inotropes, and followed up after 6 hours and 24 hours.
Results:
Included were 45 patients with community-acquired septic shock. Septic foci were gastroenteritis (24%), intestinal perforation requiring emergency surgery (24%), pneumonia (20%), central nervous system infection (22%) and soft tissue infection (8%). Klebsiella and Enterobacter were the most frequent isolates. We estimated the factors affecting the cardiac index: high central venous pressure at zero time (r = 0.33, p = 0.024) and persistently high heart rate at hour 6 (r = 0.33, p = 0.03). The systemic vascular resistance index was high in most patients at 0 and 24 hours and at the time of resuscitation and inversely affected the cardiac index as well as affecting the velocity time integral (r = -0.416, -0.61, 0.55 and -0.295). Prolonged capillary refill time was a clinical predictor of the low velocity time integral at 24 hours (r = -0.4). The mortality was 27%. Lower systemic vascular resistance index and higher cardiac output were observed in nonsurviving patients.
Conclusion:
There was a persistently high systemic vascular resistance index in cold shock patients that influenced the stroke volume index, cardiac index, and velocity time integral. The use of echocardiograms for hemodynamic measurements is important in pediatric septic shock patients to adjust dilators, and vasopressor doses and achieve resuscitation targets in a timely manner.
-
Original Article
Glycemia upon admission and mortality in a pediatric intensive care unit
Rev Bras Ter Intensiva. 2018;30(4):471-478
Abstract
Original ArticleGlycemia upon admission and mortality in a pediatric intensive care unit
Rev Bras Ter Intensiva. 2018;30(4):471-478
DOI 10.5935/0103-507X.20180068
Views0See moreABSTRACT
Objectives:
To analyze the association between glycemia levels upon pediatric intensive care unit admission and mortality in patients hospitalized.
Methods:
A retrospective cohort of pediatric intensive care unit patients admitted to the Instituto Nacional de Salud del Niño between 2012 and 2013. A Poisson regression model with robust variance was used to quantify the association. Diagnostic test performance evaluation was used to describe the sensitivity, specificity, positive predictive value, negative predictive value and likelihood ratios for each range of glycemia.
Results:
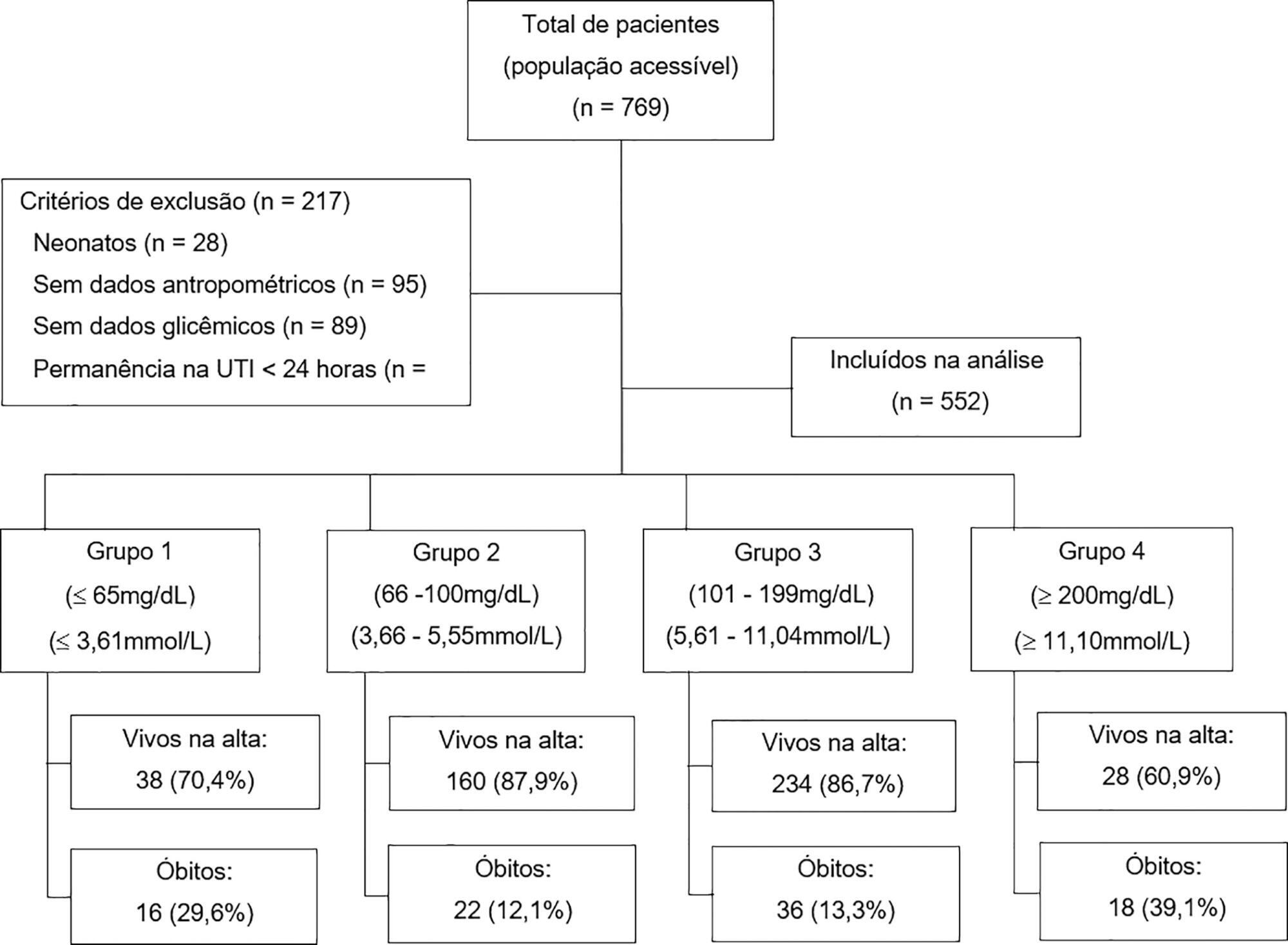
In total, 552 patients were included (median age 23 months, age range 5 months to 79.8 months). The mean glycemia level upon admission was 121.3mg/dL (6.73mmol/L). Ninety-two (16.6%) patients died during hospitalization. In multivariable analyses, significant associations were found between glycemia < 65mg/dL (3.61mmol/L) (RR: 2.01, 95%CI 1.14 - 3.53), glycemia > 200mg/dL (> 11.1mmol/L) (RR: 2.91, 95%CI 1.71 – 4.55), malnutrition (RR: 1.53, 95%CI 1.04 – 2.25), mechanical ventilation (RR: 3.71, 95%CI 1.17 – 11.76) and mortality at discharge. There was low sensitivity (between 17.39% and 39.13%) and high specificity (between 49.13% and 91.74%) for different glucose cut-off levels.
Conclusion:
There was an increased risk of death at discharge in patients who developed hypoglycemia and hyperglycemia upon admission to the pediatric intensive care unit. Certain glucose ranges (> 200mg/dL (> 11.1mmol/L) and < 65mg/dL (3.61mmol/L)) have high specificity as predictors of death at discharge.
Views0Abstract
Original ArticleGlycemia upon admission and mortality in a pediatric intensive care unit
Rev Bras Ter Intensiva. 2018;30(4):471-478
DOI 10.5935/0103-507X.20180068
Views0See moreABSTRACT
Objectives:
To analyze the association between glycemia levels upon pediatric intensive care unit admission and mortality in patients hospitalized.
Methods:
A retrospective cohort of pediatric intensive care unit patients admitted to the Instituto Nacional de Salud del Niño between 2012 and 2013. A Poisson regression model with robust variance was used to quantify the association. Diagnostic test performance evaluation was used to describe the sensitivity, specificity, positive predictive value, negative predictive value and likelihood ratios for each range of glycemia.
Results:
In total, 552 patients were included (median age 23 months, age range 5 months to 79.8 months). The mean glycemia level upon admission was 121.3mg/dL (6.73mmol/L). Ninety-two (16.6%) patients died during hospitalization. In multivariable analyses, significant associations were found between glycemia < 65mg/dL (3.61mmol/L) (RR: 2.01, 95%CI 1.14 - 3.53), glycemia > 200mg/dL (> 11.1mmol/L) (RR: 2.91, 95%CI 1.71 – 4.55), malnutrition (RR: 1.53, 95%CI 1.04 – 2.25), mechanical ventilation (RR: 3.71, 95%CI 1.17 – 11.76) and mortality at discharge. There was low sensitivity (between 17.39% and 39.13%) and high specificity (between 49.13% and 91.74%) for different glucose cut-off levels.
Conclusion:
There was an increased risk of death at discharge in patients who developed hypoglycemia and hyperglycemia upon admission to the pediatric intensive care unit. Certain glucose ranges (> 200mg/dL (> 11.1mmol/L) and < 65mg/dL (3.61mmol/L)) have high specificity as predictors of death at discharge.
-
Original Article
Comparisons and correlations of pain intensity and respiratory and peripheral muscle strength in the pre- and postoperative periods of cardiac surgery
Rev Bras Ter Intensiva. 2018;30(4):479-486
Abstract
Original ArticleComparisons and correlations of pain intensity and respiratory and peripheral muscle strength in the pre- and postoperative periods of cardiac surgery
Rev Bras Ter Intensiva. 2018;30(4):479-486
DOI 10.5935/0103-507X.20180069
Views0See moreABSTRACT
Objective:
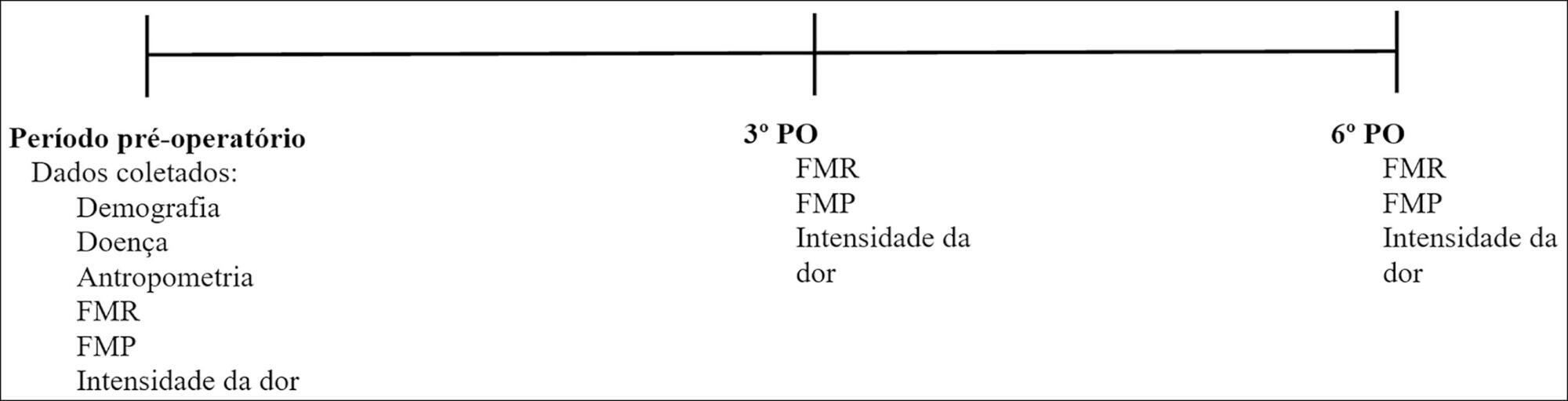
To evaluate respiratory and peripheral muscle strength after cardiac surgery. Additionally, we compared the changes in these variables on the third and sixth postoperative days.
Methods:
Forty-six patients were recruited, including 17 women and 29 men, with a mean age of 60.50 years (SD = 9.20). Myocardial revascularization surgery was performed in 36 patients, replacement of the aortic valve in 5 patients, and replacement of the mitral valve in 5 patients.
Results:
A significant reduction in respiratory and peripheral muscle strength and a significant increase in pain intensity were observed on the third and sixth postoperative days (p < 0.05), except for the variable maximal inspiratory pressure; on the sixth postoperative day, maximal inspiratory pressure values were already similar to the preoperative and predicted values (p > 0.05). There was an association between peripheral muscle strength, specifically between maximal expiratory pressure preoperatively (rs = 0.383; p = 0.009), on the third postoperative day (rs = 0.468; p = 0.001) and on the sixth postoperative day (rs = 0.311; p = 0.037). The effect sizes were consistently moderate-to-large for respiratory muscle strength, the Medical Research Council scale and the visual analog scale, in particular between preoperative assessment and the sixth postoperative day.
Conclusion:
There is a decrease in respiratory and peripheral muscle strength after cardiac surgery. In addition, maximal expiratory pressure is the variable that is most associated with peripheral muscle strength. These variables, especially respiratory and peripheral muscle strength, should be considered by professionals working in the intensive care setting.
Views0Abstract
Original ArticleComparisons and correlations of pain intensity and respiratory and peripheral muscle strength in the pre- and postoperative periods of cardiac surgery
Rev Bras Ter Intensiva. 2018;30(4):479-486
DOI 10.5935/0103-507X.20180069
Views0See moreABSTRACT
Objective:
To evaluate respiratory and peripheral muscle strength after cardiac surgery. Additionally, we compared the changes in these variables on the third and sixth postoperative days.
Methods:
Forty-six patients were recruited, including 17 women and 29 men, with a mean age of 60.50 years (SD = 9.20). Myocardial revascularization surgery was performed in 36 patients, replacement of the aortic valve in 5 patients, and replacement of the mitral valve in 5 patients.
Results:
A significant reduction in respiratory and peripheral muscle strength and a significant increase in pain intensity were observed on the third and sixth postoperative days (p < 0.05), except for the variable maximal inspiratory pressure; on the sixth postoperative day, maximal inspiratory pressure values were already similar to the preoperative and predicted values (p > 0.05). There was an association between peripheral muscle strength, specifically between maximal expiratory pressure preoperatively (rs = 0.383; p = 0.009), on the third postoperative day (rs = 0.468; p = 0.001) and on the sixth postoperative day (rs = 0.311; p = 0.037). The effect sizes were consistently moderate-to-large for respiratory muscle strength, the Medical Research Council scale and the visual analog scale, in particular between preoperative assessment and the sixth postoperative day.
Conclusion:
There is a decrease in respiratory and peripheral muscle strength after cardiac surgery. In addition, maximal expiratory pressure is the variable that is most associated with peripheral muscle strength. These variables, especially respiratory and peripheral muscle strength, should be considered by professionals working in the intensive care setting.
-
Review Article
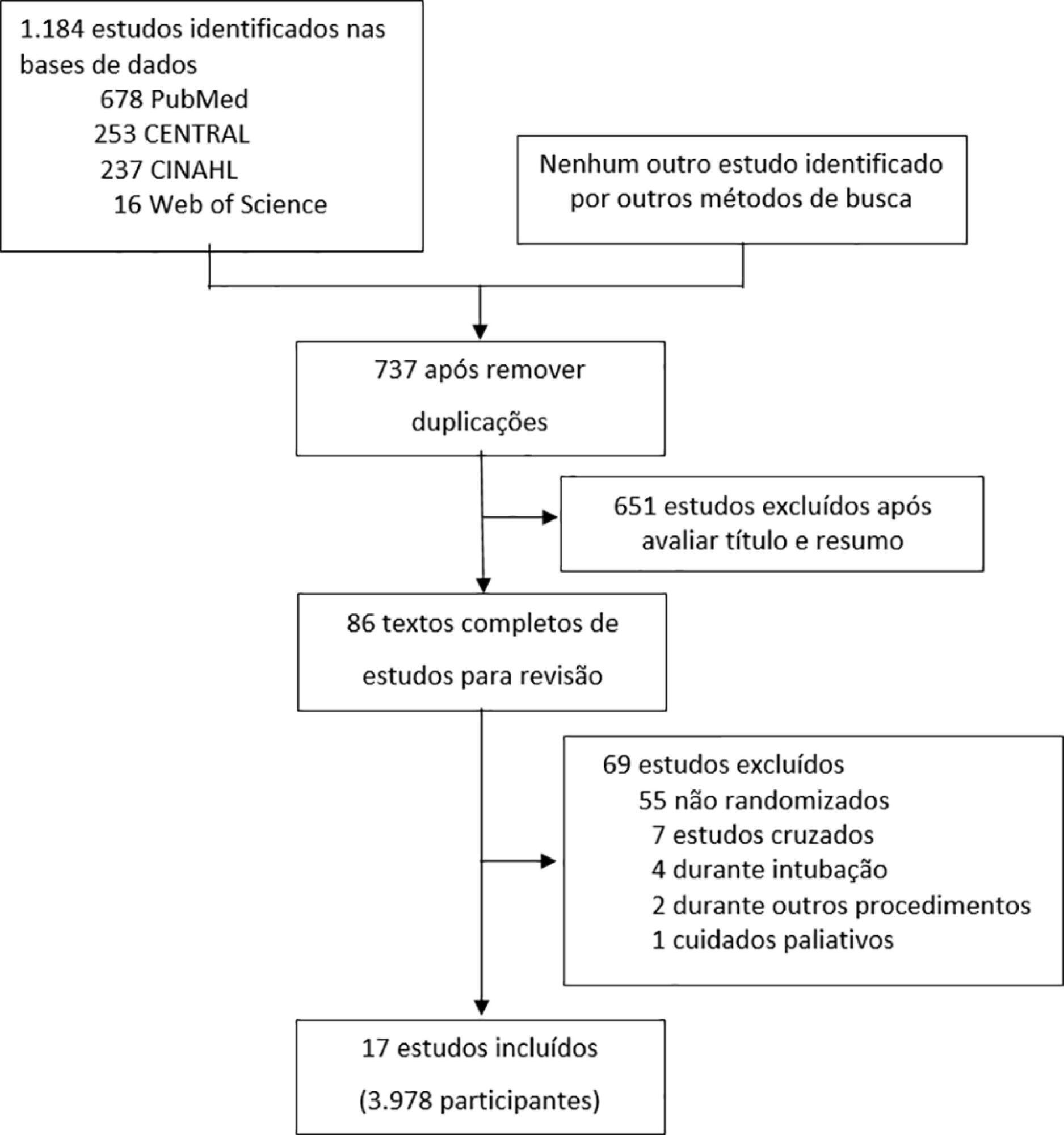
The effects of high-flow nasal cannula on intubation and re-intubation in critically ill patients: a systematic review, meta-analysis and trial sequential analysis
Rev Bras Ter Intensiva. 2018;30(4):487-495
Abstract
Review ArticleThe effects of high-flow nasal cannula on intubation and re-intubation in critically ill patients: a systematic review, meta-analysis and trial sequential analysis
Rev Bras Ter Intensiva. 2018;30(4):487-495
DOI 10.5935/0103-507X.20180070
Views0See moreABSTRACT
Objective:
To evaluate the efficacy of high-flow nasal cannula in the prevention of intubation and re-intubation in critically ill patients compared to conventional oxygen therapy or noninvasive ventilation.
Methods:
This systematic review was performed through an electronic database search of articles published from 1966 to April 2018. The primary outcome was the need for intubation or re-intubation. The secondary outcomes were therapy escalation, mortality at the longest follow-up, hospital mortality and the need for noninvasive ventilation.
Results:
Seventeen studies involving 3,978 patients were included. There was no reduction in the need for intubation or re-intubation with high-flow nasal cannula (OR 0.72; 95%CI 0.52 – 1.01; p = 0.056). There was no difference in the need for therapy escalation (OR 0.80, 95% CI 0.59 – 1.08, p = 0.144), mortality at the longest follow-up (OR 0.94; 95%CI 0.70 – 1.25; p = 0.667), hospital mortality (OR 0.84; 95%CI 0.56 – 1.26; p = 0.391) or noninvasive ventilation (OR 0.64, 95%CI 0.39 – 1.05, p = 0.075). In the trial sequential analysis, the number of events included was lower than the optimal information size with a global type I error > 0.05.
Conclusion:
In the present study and setting, high-flow nasal cannula was not associated with a reduction of the need for intubation or re-intubation in critically ill patients.
Views0Abstract
Review ArticleThe effects of high-flow nasal cannula on intubation and re-intubation in critically ill patients: a systematic review, meta-analysis and trial sequential analysis
Rev Bras Ter Intensiva. 2018;30(4):487-495
DOI 10.5935/0103-507X.20180070
Views0See moreABSTRACT
Objective:
To evaluate the efficacy of high-flow nasal cannula in the prevention of intubation and re-intubation in critically ill patients compared to conventional oxygen therapy or noninvasive ventilation.
Methods:
This systematic review was performed through an electronic database search of articles published from 1966 to April 2018. The primary outcome was the need for intubation or re-intubation. The secondary outcomes were therapy escalation, mortality at the longest follow-up, hospital mortality and the need for noninvasive ventilation.
Results:
Seventeen studies involving 3,978 patients were included. There was no reduction in the need for intubation or re-intubation with high-flow nasal cannula (OR 0.72; 95%CI 0.52 – 1.01; p = 0.056). There was no difference in the need for therapy escalation (OR 0.80, 95% CI 0.59 – 1.08, p = 0.144), mortality at the longest follow-up (OR 0.94; 95%CI 0.70 – 1.25; p = 0.667), hospital mortality (OR 0.84; 95%CI 0.56 – 1.26; p = 0.391) or noninvasive ventilation (OR 0.64, 95%CI 0.39 – 1.05, p = 0.075). In the trial sequential analysis, the number of events included was lower than the optimal information size with a global type I error > 0.05.
Conclusion:
In the present study and setting, high-flow nasal cannula was not associated with a reduction of the need for intubation or re-intubation in critically ill patients.
-
Review Article
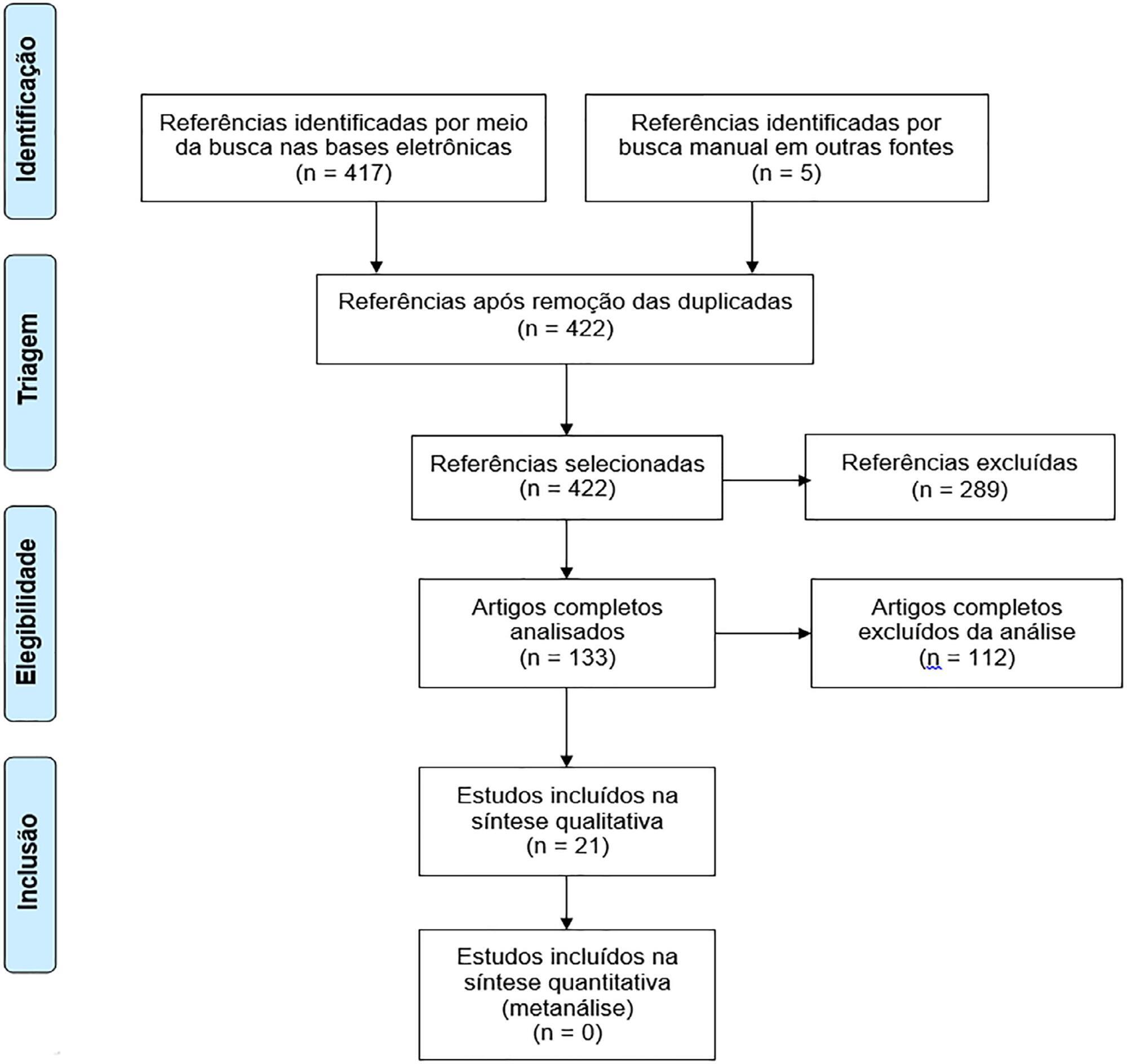
Quality of life in survivors after a period of hospitalization in the intensive care unit: a systematic review
Rev Bras Ter Intensiva. 2018;30(4):496-507
Abstract
Review ArticleQuality of life in survivors after a period of hospitalization in the intensive care unit: a systematic review
Rev Bras Ter Intensiva. 2018;30(4):496-507
DOI 10.5935/0103-507X.20180071
Views0See moreABSTRACT
Objective:
To assess the long-term, health-related quality of life of intensive care unit survivors by systematic review.
Methods:
The search for, and selection and analysis of, observational studies that assessed the health-related quality of life of intensive care unit survivors in the electronic databases LILACS and MEDLINE® (accessed through PubMed) was performed using the indexed MESH terms “quality of life [MeSH Terms]” AND “critically illness [MeSH Terms]”. Studies on adult patients without specific prior diseases published in English in the last 5 years were included in this systematic review. The citations were independently selected by three reviewers. Data were standardly and independently retrieved by two reviewers, and the quality of the studies was assessed using the Newcastle-Ottawa scale.
Results:
In total, 19 observational cohort and 2 case-control studies of 57,712 critically ill patients were included. The follow-up time of the studies ranged from 6 months to 6 years, and most studies had a 6-month or 1-year follow up. The health-related quality of life was assessed using two generic tools, the EuroQol and the Short Form Health Survey. The overall quality of the studies was low.
Conclusions:
Long-term, health-related quality of life is compromised among intensive care unit survivors compared with the corresponding general population. However, it is not significantly affected by the occurrence of sepsis, delirium, and acute kidney injury during intensive care unit admission when compared with that of critically ill patient control groups. High-quality studies are necessary to quantify the health-related quality of life among intensive care unit survivors.
Views0Abstract
Review ArticleQuality of life in survivors after a period of hospitalization in the intensive care unit: a systematic review
Rev Bras Ter Intensiva. 2018;30(4):496-507
DOI 10.5935/0103-507X.20180071
Views0See moreABSTRACT
Objective:
To assess the long-term, health-related quality of life of intensive care unit survivors by systematic review.
Methods:
The search for, and selection and analysis of, observational studies that assessed the health-related quality of life of intensive care unit survivors in the electronic databases LILACS and MEDLINE® (accessed through PubMed) was performed using the indexed MESH terms “quality of life [MeSH Terms]” AND “critically illness [MeSH Terms]”. Studies on adult patients without specific prior diseases published in English in the last 5 years were included in this systematic review. The citations were independently selected by three reviewers. Data were standardly and independently retrieved by two reviewers, and the quality of the studies was assessed using the Newcastle-Ottawa scale.
Results:
In total, 19 observational cohort and 2 case-control studies of 57,712 critically ill patients were included. The follow-up time of the studies ranged from 6 months to 6 years, and most studies had a 6-month or 1-year follow up. The health-related quality of life was assessed using two generic tools, the EuroQol and the Short Form Health Survey. The overall quality of the studies was low.
Conclusions:
Long-term, health-related quality of life is compromised among intensive care unit survivors compared with the corresponding general population. However, it is not significantly affected by the occurrence of sepsis, delirium, and acute kidney injury during intensive care unit admission when compared with that of critically ill patient control groups. High-quality studies are necessary to quantify the health-related quality of life among intensive care unit survivors.
-
Case Report
High-flow nasal cannula in the treatment of acute hypoxemic respiratory failure in a pregnant patient: case report
Rev Bras Ter Intensiva. 2018;30(4):508-511
Abstract
Case ReportHigh-flow nasal cannula in the treatment of acute hypoxemic respiratory failure in a pregnant patient: case report
Rev Bras Ter Intensiva. 2018;30(4):508-511
DOI 10.5935/0103-507X.20180072
Views0ABSTRACT
Little evidence exists to support the use of noninvasive mechanical ventilation for acute hypoxemic respiratory failure. However, considering the complications associated with endotracheal intubation, we attempted to implement noninvasive mechanical ventilation in a 24-year-old patient who was 32 weeks pregnant and was admitted to the intensive care unit with acute hypoxemic respiratory failure and sepsis secondary to a urinary tract infection. Lack of tolerance to noninvasive mechanical ventilation led us to use an alternative method to avoid endotracheal intubation. The use of high-flow nasal cannula allowed to overcome this situation, wich supports this technique as a treatment option for critical obstetric patients that is safe for both the mother and fetus.
Keywords:acute respiratory failureHigh flow nasal cannulaIntensive Care UnitOxygen inhalation therapypregnancySee moreViews0Abstract
Case ReportHigh-flow nasal cannula in the treatment of acute hypoxemic respiratory failure in a pregnant patient: case report
Rev Bras Ter Intensiva. 2018;30(4):508-511
DOI 10.5935/0103-507X.20180072
Views0ABSTRACT
Little evidence exists to support the use of noninvasive mechanical ventilation for acute hypoxemic respiratory failure. However, considering the complications associated with endotracheal intubation, we attempted to implement noninvasive mechanical ventilation in a 24-year-old patient who was 32 weeks pregnant and was admitted to the intensive care unit with acute hypoxemic respiratory failure and sepsis secondary to a urinary tract infection. Lack of tolerance to noninvasive mechanical ventilation led us to use an alternative method to avoid endotracheal intubation. The use of high-flow nasal cannula allowed to overcome this situation, wich supports this technique as a treatment option for critical obstetric patients that is safe for both the mother and fetus.
Keywords:acute respiratory failureHigh flow nasal cannulaIntensive Care UnitOxygen inhalation therapypregnancySee more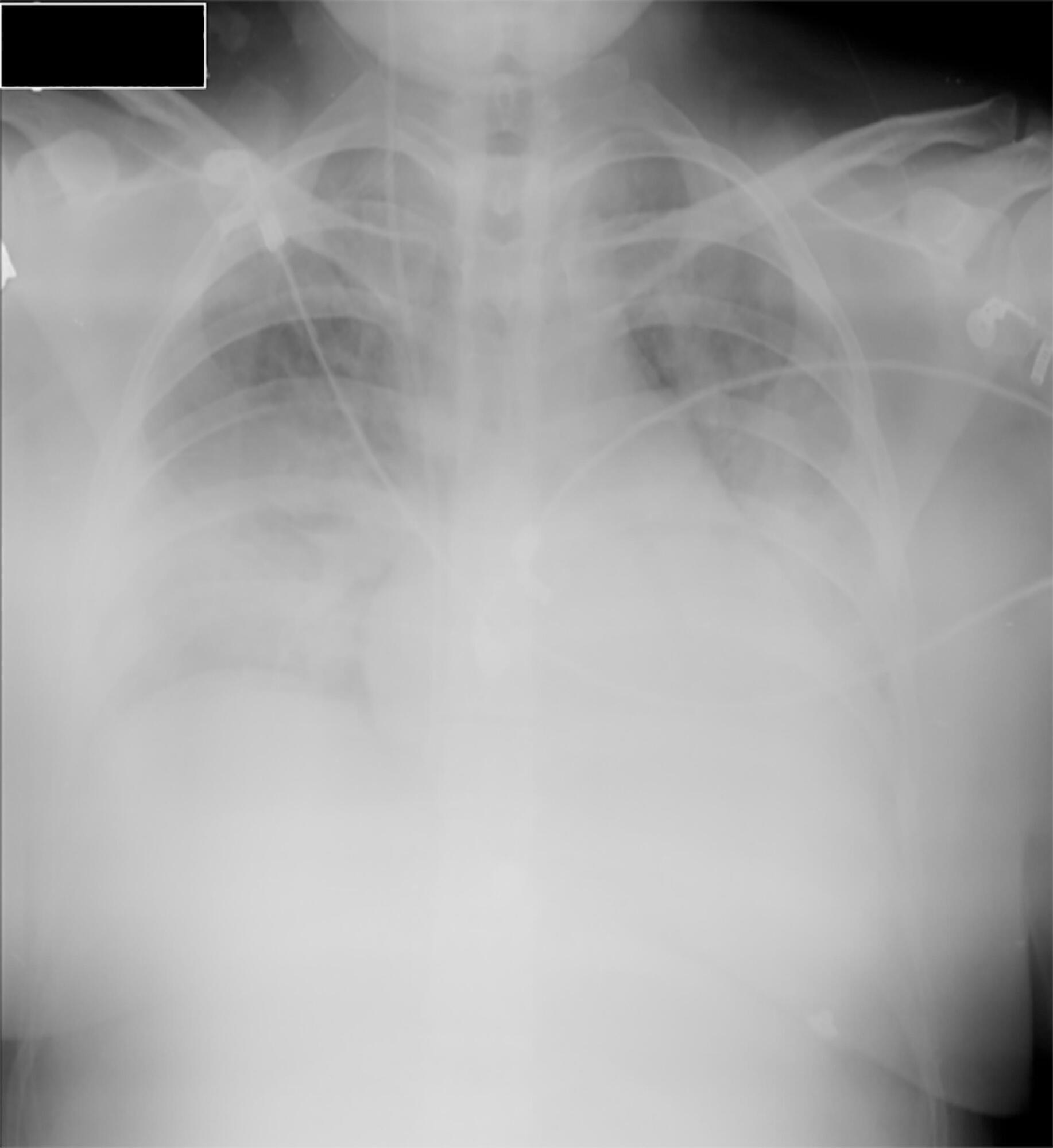
Volume Articles - Critical Care Science (CCS)
