-
Original Article
Statistical analysis plan for early goal-directed therapy using a physiological holistic view – the ANDROMEDA-SHOCK: a randomized controlled trial
Rev Bras Ter Intensiva. 2018;30(3):253-263
Abstract
Original ArticleStatistical analysis plan for early goal-directed therapy using a physiological holistic view – the ANDROMEDA-SHOCK: a randomized controlled trial
Rev Bras Ter Intensiva. 2018;30(3):253-263
DOI 10.5935/0103-507X.20180041
Views0See moreABSTRACT
Background:
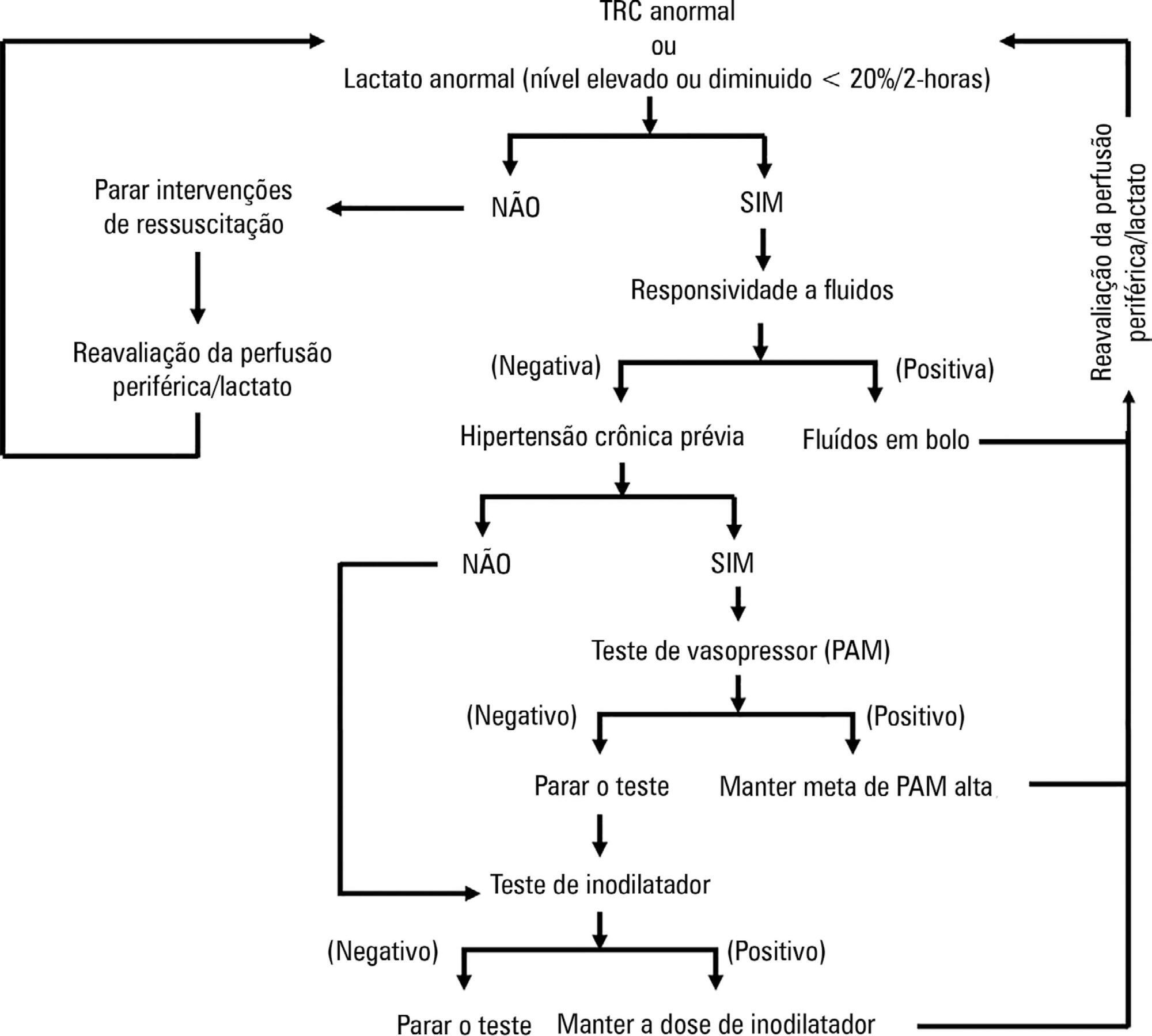
ANDROMEDA-SHOCK is an international, multicenter, randomized controlled trial comparing peripheral perfusion-targeted resuscitation to lactate-targeted resuscitation in patients with septic shock in order to test the hypothesis that resuscitation targeting peripheral perfusion will be associated with lower morbidity and mortality.
Objective:
To report the statistical analysis plan for the ANDROMEDA-SHOCK trial.
Methods:
We describe the trial design, primary and secondary objectives, patients, methods of randomization, interventions, outcomes, and sample size. We describe our planned statistical analysis for the primary, secondary and tertiary outcomes. We also describe the subgroup and sensitivity analyses. Finally, we provide details for presenting our results, including mock tables showing baseline characteristics, the evolution of hemodynamic and perfusion variables, and the effects of treatments on outcomes.
Conclusion:
According to the best trial practice, we report our statistical analysis plan and data management plan prior to locking the database and initiating the analyses. We anticipate that this procedure will prevent analysis bias and enhance the utility of the reported results.
Views0

Abstract
Original ArticleStatistical analysis plan for early goal-directed therapy using a physiological holistic view – the ANDROMEDA-SHOCK: a randomized controlled trial
Rev Bras Ter Intensiva. 2018;30(3):253-263
DOI 10.5935/0103-507X.20180041
Views0See moreABSTRACT
Background:
ANDROMEDA-SHOCK is an international, multicenter, randomized controlled trial comparing peripheral perfusion-targeted resuscitation to lactate-targeted resuscitation in patients with septic shock in order to test the hypothesis that resuscitation targeting peripheral perfusion will be associated with lower morbidity and mortality.
Objective:
To report the statistical analysis plan for the ANDROMEDA-SHOCK trial.
Methods:
We describe the trial design, primary and secondary objectives, patients, methods of randomization, interventions, outcomes, and sample size. We describe our planned statistical analysis for the primary, secondary and tertiary outcomes. We also describe the subgroup and sensitivity analyses. Finally, we provide details for presenting our results, including mock tables showing baseline characteristics, the evolution of hemodynamic and perfusion variables, and the effects of treatments on outcomes.
Conclusion:
According to the best trial practice, we report our statistical analysis plan and data management plan prior to locking the database and initiating the analyses. We anticipate that this procedure will prevent analysis bias and enhance the utility of the reported results.
-
Original Article
Existing capacity for renal replacement therapy and site-specific practices for managing acute kidney injury at centers participating in the BaSICS trial
Rev Bras Ter Intensiva. 2018;30(3):264-285
Abstract
Original ArticleExisting capacity for renal replacement therapy and site-specific practices for managing acute kidney injury at centers participating in the BaSICS trial
Rev Bras Ter Intensiva. 2018;30(3):264-285
DOI 10.5935/0103-507X.20180058
Views0See moreABSTRACT
Objective:
To investigate the existing capacity for renal replacement therapy and site-specific practices for managing acute kidney injury at centers participating in the BaSICS trial.
Methods:
A questionnaire was provided to the chairs of 61 intensive care units enrolled in a randomized clinical trial in Brazil. A total of 124 physicians completed the questionnaire.
Results:
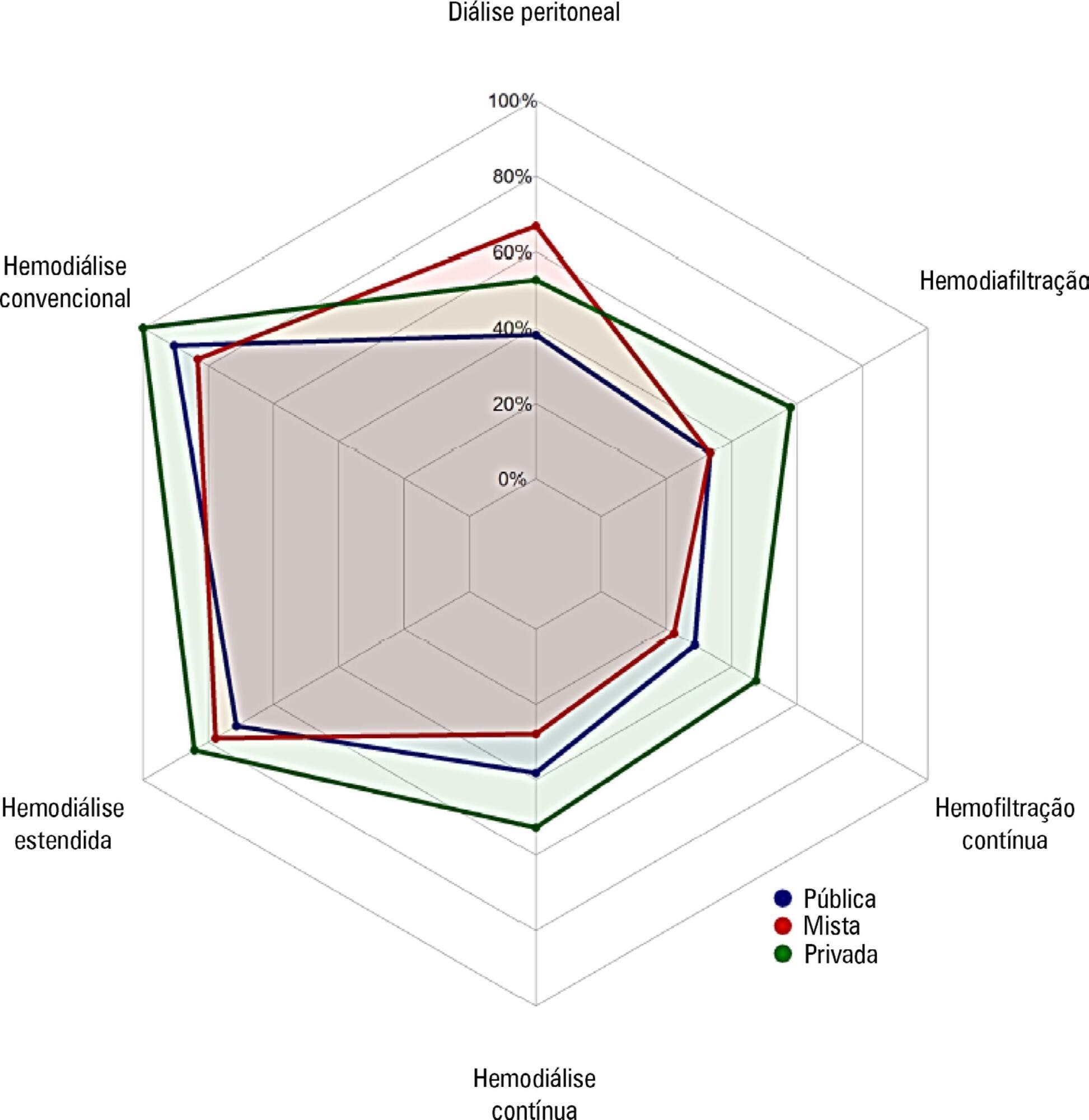
Approximately 15% of the patients admitted to the analyzed intensive care units received renal replacement therapy at the time of data collection. At least one renal replacement method was available in all of the analyzed units. Continuous methods were available more frequently at the private units than at the public units. The time from indication to onset of treatment was longer at the public units than at private units. The main obstacles to treatment initiation at public intensive care units were related to the availability of equipment and personnel, while the main bottleneck at private units was the nephrologist assessment. A considerable proportion of the participants stated that they would change their approach to renal replacement therapy if there were no limitations on the availability of methods in their units.
Conclusion:
There was wide variation in the availability of resources for renal replacement therapy and in the management of acute kidney injury in Brazilian intensive care units. This information should be taken into account when planning clinical trials focused on this topic in Brazil.
Views0Abstract
Original ArticleExisting capacity for renal replacement therapy and site-specific practices for managing acute kidney injury at centers participating in the BaSICS trial
Rev Bras Ter Intensiva. 2018;30(3):264-285
DOI 10.5935/0103-507X.20180058
Views0See moreABSTRACT
Objective:
To investigate the existing capacity for renal replacement therapy and site-specific practices for managing acute kidney injury at centers participating in the BaSICS trial.
Methods:
A questionnaire was provided to the chairs of 61 intensive care units enrolled in a randomized clinical trial in Brazil. A total of 124 physicians completed the questionnaire.
Results:
Approximately 15% of the patients admitted to the analyzed intensive care units received renal replacement therapy at the time of data collection. At least one renal replacement method was available in all of the analyzed units. Continuous methods were available more frequently at the private units than at the public units. The time from indication to onset of treatment was longer at the public units than at private units. The main obstacles to treatment initiation at public intensive care units were related to the availability of equipment and personnel, while the main bottleneck at private units was the nephrologist assessment. A considerable proportion of the participants stated that they would change their approach to renal replacement therapy if there were no limitations on the availability of methods in their units.
Conclusion:
There was wide variation in the availability of resources for renal replacement therapy and in the management of acute kidney injury in Brazilian intensive care units. This information should be taken into account when planning clinical trials focused on this topic in Brazil.
-
Original Article
Etiology of hyperglycemia in critically ill children and the impact of organ dysfunction
Rev Bras Ter Intensiva. 2018;30(3):286-293
Abstract
Original ArticleEtiology of hyperglycemia in critically ill children and the impact of organ dysfunction
Rev Bras Ter Intensiva. 2018;30(3):286-293
DOI 10.5935/0103-507X.20180051
Views0See moreABSTRACT
Objective:
This study aimed to study the incidence of stress hyperglycemia in critically ill children and to investigate the etiological basis of the hyperglycemia based on homeostasis model assessment.
Methods:
This was a prospective cohort study in one of the pediatric intensive care units of Cairo University, including 60 critically ill children and 21 healthy controls. Serum blood glucose, insulin, and C-peptide levels were measured within 24 hours of admission. Homeostasis model assessment was used to assess β-cell function and insulin sensitivity.
Results:
Hyperglycemia was estimated in 70% of patients. Blood glucose values ≥ 180mg/dL were associated with a poor outcome. Blood glucose levels were positively correlated with Pediatric Risk for Mortality (PRISM III) score and number of organ dysfunctions (p = 0.019 and p = 0.022, respectively), while insulin levels were negatively correlated with number of organ dysfunctions (r = −0.33, p = 0.01). Homeostasis model assessment revealed that 26 (43.3%) of the critically ill patients had low β-cell function, and 18 (30%) had low insulin sensitivity. Combined pathology was detected in 2 (3.3%) patients only. Low β-cell function was significantly associated with the presence of multi-organ dysfunction; respiratory, cardiovascular, and hematological dysfunctions; and the presence of sepsis.
Conclusions:
β-Cell dysfunction appeared to be prevalent in our cohort and was associated with multi-organ dysfunction.
Views0Abstract
Original ArticleEtiology of hyperglycemia in critically ill children and the impact of organ dysfunction
Rev Bras Ter Intensiva. 2018;30(3):286-293
DOI 10.5935/0103-507X.20180051
Views0See moreABSTRACT
Objective:
This study aimed to study the incidence of stress hyperglycemia in critically ill children and to investigate the etiological basis of the hyperglycemia based on homeostasis model assessment.
Methods:
This was a prospective cohort study in one of the pediatric intensive care units of Cairo University, including 60 critically ill children and 21 healthy controls. Serum blood glucose, insulin, and C-peptide levels were measured within 24 hours of admission. Homeostasis model assessment was used to assess β-cell function and insulin sensitivity.
Results:
Hyperglycemia was estimated in 70% of patients. Blood glucose values ≥ 180mg/dL were associated with a poor outcome. Blood glucose levels were positively correlated with Pediatric Risk for Mortality (PRISM III) score and number of organ dysfunctions (p = 0.019 and p = 0.022, respectively), while insulin levels were negatively correlated with number of organ dysfunctions (r = −0.33, p = 0.01). Homeostasis model assessment revealed that 26 (43.3%) of the critically ill patients had low β-cell function, and 18 (30%) had low insulin sensitivity. Combined pathology was detected in 2 (3.3%) patients only. Low β-cell function was significantly associated with the presence of multi-organ dysfunction; respiratory, cardiovascular, and hematological dysfunctions; and the presence of sepsis.
Conclusions:
β-Cell dysfunction appeared to be prevalent in our cohort and was associated with multi-organ dysfunction.
-
Original Article
Risk factors for extubation failure in the intensive care unit
Rev Bras Ter Intensiva. 2018;30(3):294-300
Abstract
Original ArticleRisk factors for extubation failure in the intensive care unit
Rev Bras Ter Intensiva. 2018;30(3):294-300
DOI 10.5935/0103-507X.20180046
Views0See moreABSTRACT
Objective:
To determine the risk factors for extubation failure in the intensive care unit.
Methods:
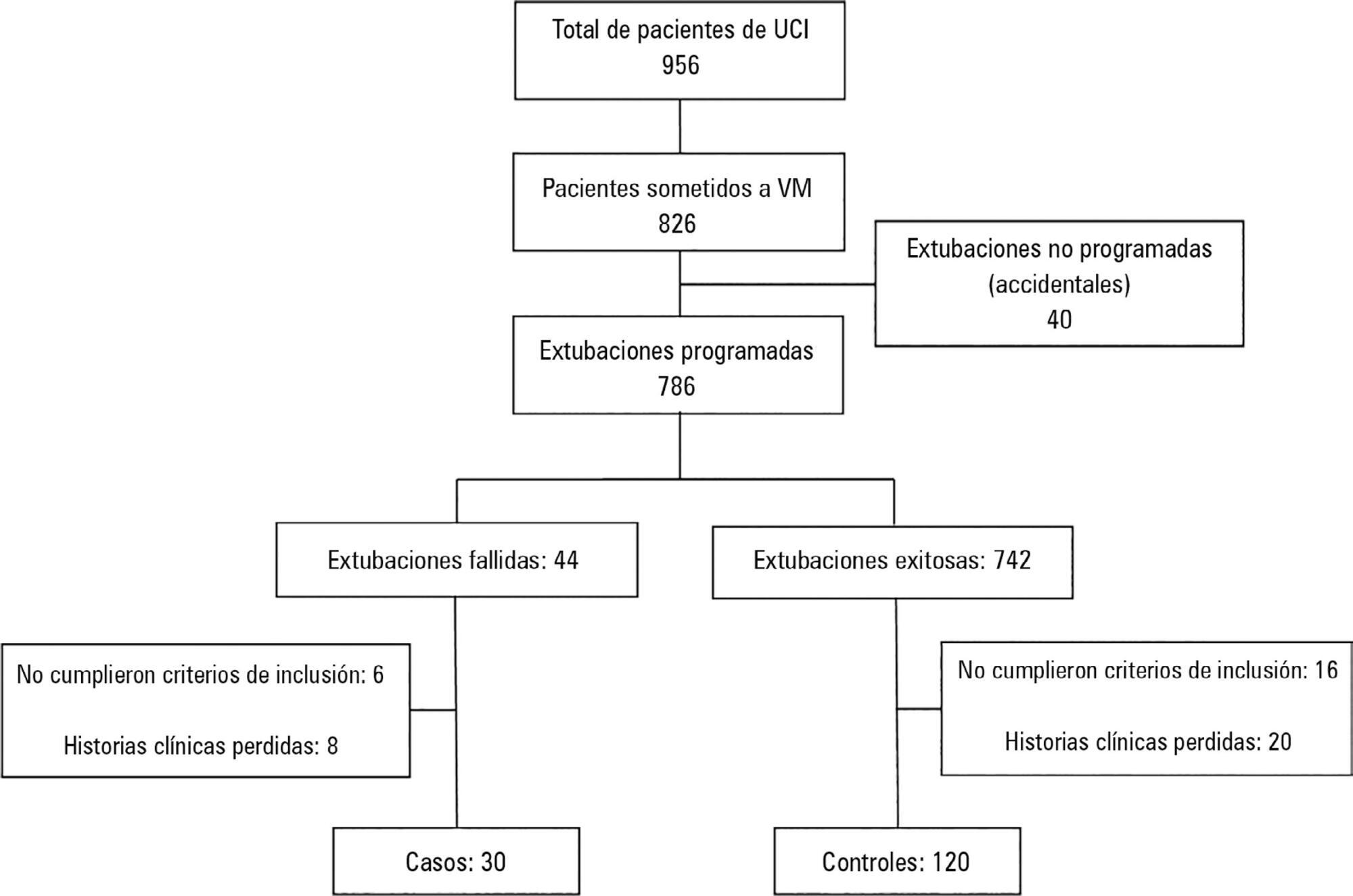
The present case-control study was conducted in an intensive care unit. Failed extubations were used as cases, while successful extubations were used as controls. Extubation failure was defined as reintubation being required within the first 48 hours of extubation.
Results:
Out of a total of 956 patients who were admitted to the intensive care unit, 826 were subjected to mechanical ventilation (86%). There were 30 failed extubations and 120 successful extubations. The proportion of failed extubations was 5.32%. The risk factors found for failed extubations were a prolonged length of mechanical ventilation of greater than 7 days (OR = 3.84, 95%CI = 1.01 – 14.56, p = 0.04), time in the intensive care unit (OR = 1.04, 95%CI = 1.00 – 1.09, p = 0.03) and the use of sedatives for longer than 5 days (OR = 4.81, 95%CI = 1.28 – 18.02; p = 0.02).
Conclusion:
Pediatric patients on mechanical ventilation were at greater risk of failed extubation if they spent more time in the intensive care unit and if they were subjected to prolonged mechanical ventilation (longer than 7 days) or greater amounts of sedative use.
Views0Abstract
Original ArticleRisk factors for extubation failure in the intensive care unit
Rev Bras Ter Intensiva. 2018;30(3):294-300
DOI 10.5935/0103-507X.20180046
Views0See moreABSTRACT
Objective:
To determine the risk factors for extubation failure in the intensive care unit.
Methods:
The present case-control study was conducted in an intensive care unit. Failed extubations were used as cases, while successful extubations were used as controls. Extubation failure was defined as reintubation being required within the first 48 hours of extubation.
Results:
Out of a total of 956 patients who were admitted to the intensive care unit, 826 were subjected to mechanical ventilation (86%). There were 30 failed extubations and 120 successful extubations. The proportion of failed extubations was 5.32%. The risk factors found for failed extubations were a prolonged length of mechanical ventilation of greater than 7 days (OR = 3.84, 95%CI = 1.01 – 14.56, p = 0.04), time in the intensive care unit (OR = 1.04, 95%CI = 1.00 – 1.09, p = 0.03) and the use of sedatives for longer than 5 days (OR = 4.81, 95%CI = 1.28 – 18.02; p = 0.02).
Conclusion:
Pediatric patients on mechanical ventilation were at greater risk of failed extubation if they spent more time in the intensive care unit and if they were subjected to prolonged mechanical ventilation (longer than 7 days) or greater amounts of sedative use.
-
Original Article
Brazilian version of the Pediatric Functional Status Scale: translation and cross-cultural adaptation
Rev Bras Ter Intensiva. 2018;30(3):301-307
Abstract
Original ArticleBrazilian version of the Pediatric Functional Status Scale: translation and cross-cultural adaptation
Rev Bras Ter Intensiva. 2018;30(3):301-307
DOI 10.5935/0103-507X.20180043
Views0ABSTRACT
Objective:
To translate and cross-culturally adapt the Functional Status Scale for hospitalized children into Brazilian Portuguese.
Methods:
A methodological study of the translation and cross-cultural adaptation of the Functional Status Scale was conducted, according to the stages of translation, synthesis of translations, back-translation, synthesis of back-translations, expert committee analysis and pre-test with a sample of the target population. During the evaluation by the committee of experts, semantic, content and item analyses were performed.
Results:
The semantic, idiomatic, cultural and conceptual equivalences between the translated version and the original version were obtained, resulting in the Brazilian version of the Functional Status Scale. After the analysis by the expert committee, there were no problems regarding the cultural or conceptual equivalences because the items were pertinent to the Brazilian culture and few terms were modified. In the pre-test stage, the scale was applied by two evaluators to a sample of 25 children. Clarity and ease in answering the scale items were observed. Good inter-observer reliability was obtained, with an intraclass correlation coefficient of 0.85 (0.59 – 0.95).
Conclusions:
The Functional Status Scale for pediatric use was translated and culturally adapted into Portuguese spoken in Brazil. The translated items were pertinent to the Brazilian culture and evaluated the dimensions proposed by the original instrument. Validation studies of this instrument are suggested to make it feasible for use in different regions of Brazil.
Keywords:ChildIntensive care unitsintensive therapySemanticsSurveys and questionnairesTranslationsValidation studiesSee moreViews0Abstract
Original ArticleBrazilian version of the Pediatric Functional Status Scale: translation and cross-cultural adaptation
Rev Bras Ter Intensiva. 2018;30(3):301-307
DOI 10.5935/0103-507X.20180043
Views0ABSTRACT
Objective:
To translate and cross-culturally adapt the Functional Status Scale for hospitalized children into Brazilian Portuguese.
Methods:
A methodological study of the translation and cross-cultural adaptation of the Functional Status Scale was conducted, according to the stages of translation, synthesis of translations, back-translation, synthesis of back-translations, expert committee analysis and pre-test with a sample of the target population. During the evaluation by the committee of experts, semantic, content and item analyses were performed.
Results:
The semantic, idiomatic, cultural and conceptual equivalences between the translated version and the original version were obtained, resulting in the Brazilian version of the Functional Status Scale. After the analysis by the expert committee, there were no problems regarding the cultural or conceptual equivalences because the items were pertinent to the Brazilian culture and few terms were modified. In the pre-test stage, the scale was applied by two evaluators to a sample of 25 children. Clarity and ease in answering the scale items were observed. Good inter-observer reliability was obtained, with an intraclass correlation coefficient of 0.85 (0.59 – 0.95).
Conclusions:
The Functional Status Scale for pediatric use was translated and culturally adapted into Portuguese spoken in Brazil. The translated items were pertinent to the Brazilian culture and evaluated the dimensions proposed by the original instrument. Validation studies of this instrument are suggested to make it feasible for use in different regions of Brazil.
Keywords:ChildIntensive care unitsintensive therapySemanticsSurveys and questionnairesTranslationsValidation studiesSee more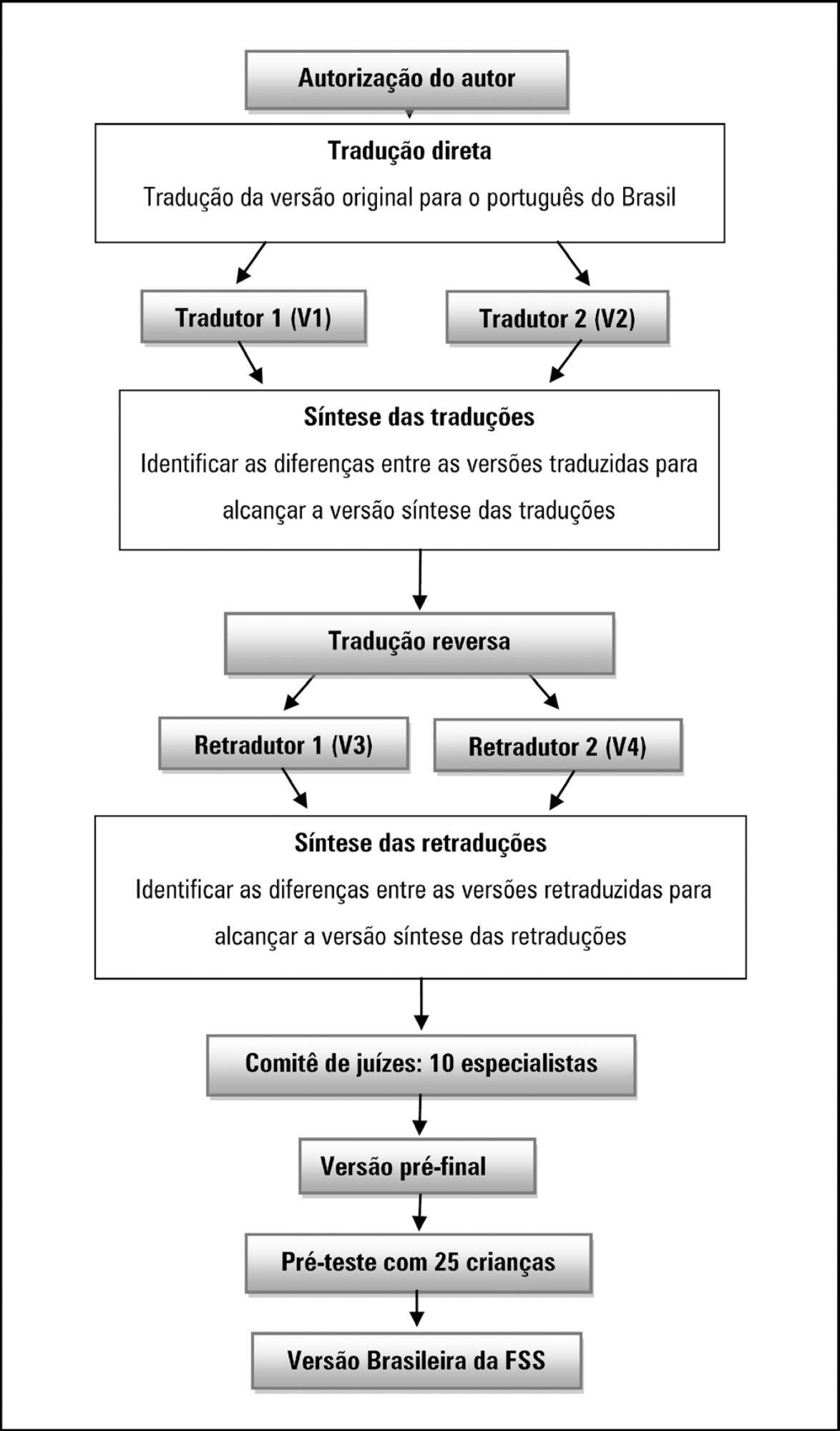
-
Original Article
Effect of a palliative care program on trends in intensive care unit utilization and do-not-resuscitate orders during terminal hospitalizations. An interrupted time series analysis
Rev Bras Ter Intensiva. 2018;30(3):308-316
Abstract
Original ArticleEffect of a palliative care program on trends in intensive care unit utilization and do-not-resuscitate orders during terminal hospitalizations. An interrupted time series analysis
Rev Bras Ter Intensiva. 2018;30(3):308-316
DOI 10.5935/0103-507X.20180042
Views2ABSTRACT
Objective:
To assess the effect of the implementation of a palliative care program on do-not-resuscitate orders and intensive care unit utilization during terminal hospitalizations.
Methods:
Data were retrospectively collected for all patients who died in a tertiary hospital in Brazil from May 2014 to September 2016. We analyzed the frequency of do-not-resuscitate orders and intensive care unit admissions among in-hospital deaths. Interrupted time series analyses were used to evaluate differences in trends of do-not-resuscitate orders and intensive care unit admissions before (17 months) and after (12 months) the implementation of a palliative care program.
Results:
We analyzed 48,372 hospital admissions and 1,071 in-hospital deaths. Deaths were preceded by do-not-resuscitate orders in 276 (25.8%) cases and admissions to the intensive care unit occurred in 814 (76%) cases. Do-not-resuscitate orders increased from 125 (20.4%) to 151 (33%) cases in the pre-implementation and post-implementation periods, respectively (p < 0.001). Intensive care unit admissions occurred in 469 (76.5%) and 345 (75.3%) cases in the pre-implementation and post-implementation periods, respectively (p = 0.654). Interrupted time series analyses confirmed a trend of increased do-not-resuscitate order registrations, from an increase of 0.5% per month pre-implementation to an increase of 2.9% per month post-implementation (p < 0.001), and demonstrated a trend of decreased intensive care unit utilization, from an increase of 0.6% per month pre-implementation to a decrease of -0.9% per month in the post-implementation period (p = 0.001).
Conclusion:
The implementation of a palliative care program was associated with a trend of increased registration of do-not-resuscitate orders and a trend of decreased intensive care unit utilization during terminal hospitalizations.
Keywords:Intensive care unitsInterrupted time series analysisPalliative CarePatient care planningResuscitation OrdersSee moreViews2Abstract
Original ArticleEffect of a palliative care program on trends in intensive care unit utilization and do-not-resuscitate orders during terminal hospitalizations. An interrupted time series analysis
Rev Bras Ter Intensiva. 2018;30(3):308-316
DOI 10.5935/0103-507X.20180042
Views2ABSTRACT
Objective:
To assess the effect of the implementation of a palliative care program on do-not-resuscitate orders and intensive care unit utilization during terminal hospitalizations.
Methods:
Data were retrospectively collected for all patients who died in a tertiary hospital in Brazil from May 2014 to September 2016. We analyzed the frequency of do-not-resuscitate orders and intensive care unit admissions among in-hospital deaths. Interrupted time series analyses were used to evaluate differences in trends of do-not-resuscitate orders and intensive care unit admissions before (17 months) and after (12 months) the implementation of a palliative care program.
Results:
We analyzed 48,372 hospital admissions and 1,071 in-hospital deaths. Deaths were preceded by do-not-resuscitate orders in 276 (25.8%) cases and admissions to the intensive care unit occurred in 814 (76%) cases. Do-not-resuscitate orders increased from 125 (20.4%) to 151 (33%) cases in the pre-implementation and post-implementation periods, respectively (p < 0.001). Intensive care unit admissions occurred in 469 (76.5%) and 345 (75.3%) cases in the pre-implementation and post-implementation periods, respectively (p = 0.654). Interrupted time series analyses confirmed a trend of increased do-not-resuscitate order registrations, from an increase of 0.5% per month pre-implementation to an increase of 2.9% per month post-implementation (p < 0.001), and demonstrated a trend of decreased intensive care unit utilization, from an increase of 0.6% per month pre-implementation to a decrease of -0.9% per month in the post-implementation period (p = 0.001).
Conclusion:
The implementation of a palliative care program was associated with a trend of increased registration of do-not-resuscitate orders and a trend of decreased intensive care unit utilization during terminal hospitalizations.
Keywords:Intensive care unitsInterrupted time series analysisPalliative CarePatient care planningResuscitation OrdersSee more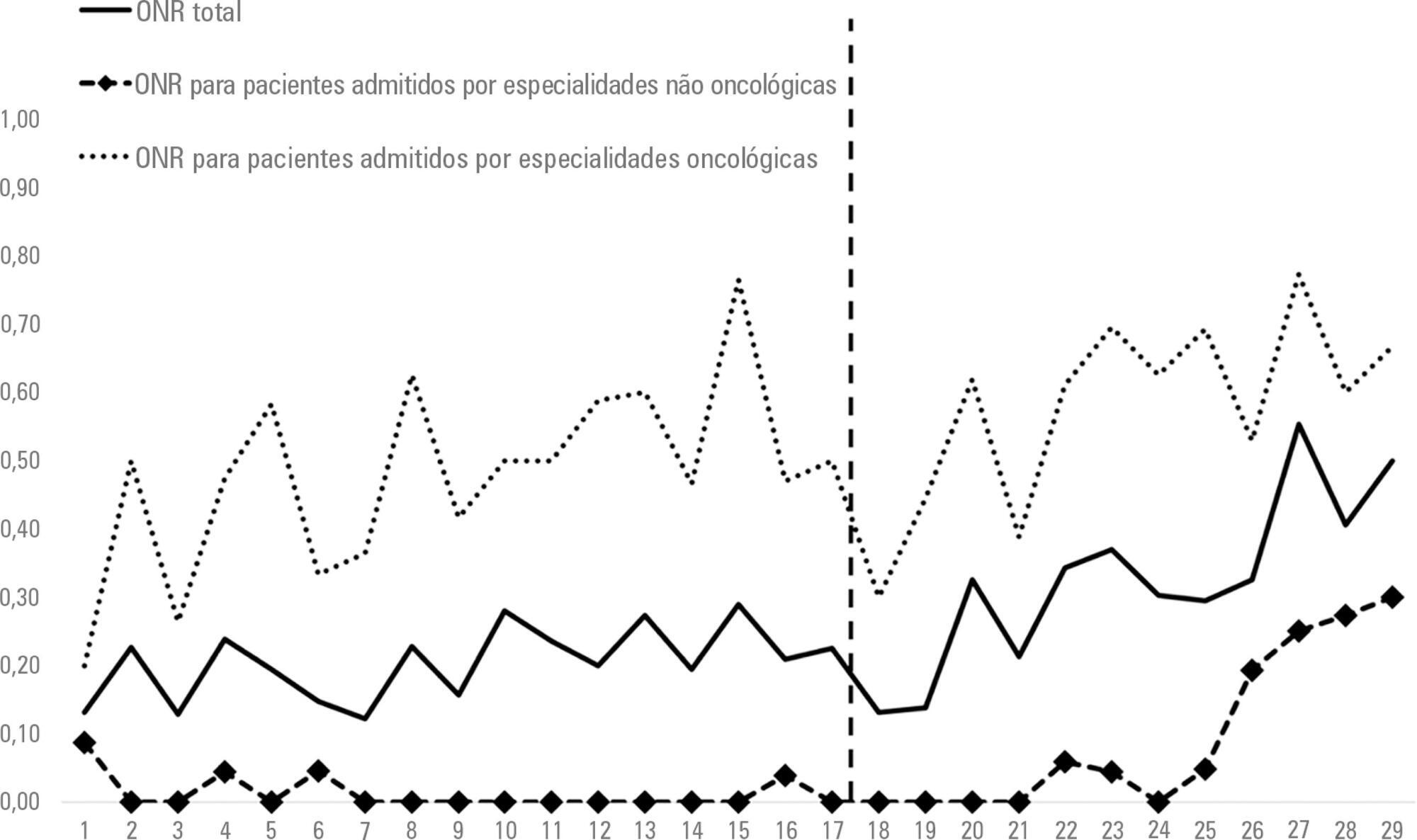
-
Original Article
Characterization of patients transported with extracorporeal respiratory and/or cardiovascular support in the State of São Paulo, Brazil
Rev Bras Ter Intensiva. 2018;30(3):317-326
Abstract
Original ArticleCharacterization of patients transported with extracorporeal respiratory and/or cardiovascular support in the State of São Paulo, Brazil
Rev Bras Ter Intensiva. 2018;30(3):317-326
DOI 10.5935/0103-507X.20180052
Views0ABSTRACT
Objective:
To characterize the transport of severely ill patients with extracorporeal respiratory or cardiovascular support.
Methods:
A series of 18 patients in the state of São Paulo, Brazil is described. All patients were consecutively evaluated by a multidisciplinary team at the hospital of origin. The patients were rescued, and extracorporeal membrane oxygenation support was provided on site. The patients were then transported to referral hospitals for extracorporeal membrane oxygenation support. Data were retrieved from a prospectively collected database.
Results:
From 2011 to 2017, 18 patients aged 29 (25 – 31) years with a SAPS 3 of 84 (68 – 92) and main primary diagnosis of leptospirosis and influenza A (H1N1) virus were transported to three referral hospitals in São Paulo. A median distance of 39 (15 – 82) km was traveled on each rescue mission during a period of 360 (308 – 431) min. A median of one (0 – 2) nurse, three (2 – 3) physicians, and one (0 – 1) physical therapist was present per rescue. Seventeen rescues were made by ambulance, and one rescue was made by helicopter. The observed complications were interruption in the energy supply to the pump in two cases (11%) and oxygen saturation < 70% in two cases. Thirteen patients (72%) survived and were discharged from the hospital. Among the nonsurvivors, there were two cases of brain death, two cases of multiple organ dysfunction syndrome, and one case of irreversible pulmonary fibrosis.
Conclusions:
Transportation with extracorporeal support occurred without serious complications, and the hospital survival rate was high.
Keywords:artificial respirationCritical illnessExtracorporeal membrane oxygenationIntensive care unitsRespiratory insufficiencyTransportation of patientsSee moreViews0Abstract
Original ArticleCharacterization of patients transported with extracorporeal respiratory and/or cardiovascular support in the State of São Paulo, Brazil
Rev Bras Ter Intensiva. 2018;30(3):317-326
DOI 10.5935/0103-507X.20180052
Views0ABSTRACT
Objective:
To characterize the transport of severely ill patients with extracorporeal respiratory or cardiovascular support.
Methods:
A series of 18 patients in the state of São Paulo, Brazil is described. All patients were consecutively evaluated by a multidisciplinary team at the hospital of origin. The patients were rescued, and extracorporeal membrane oxygenation support was provided on site. The patients were then transported to referral hospitals for extracorporeal membrane oxygenation support. Data were retrieved from a prospectively collected database.
Results:
From 2011 to 2017, 18 patients aged 29 (25 – 31) years with a SAPS 3 of 84 (68 – 92) and main primary diagnosis of leptospirosis and influenza A (H1N1) virus were transported to three referral hospitals in São Paulo. A median distance of 39 (15 – 82) km was traveled on each rescue mission during a period of 360 (308 – 431) min. A median of one (0 – 2) nurse, three (2 – 3) physicians, and one (0 – 1) physical therapist was present per rescue. Seventeen rescues were made by ambulance, and one rescue was made by helicopter. The observed complications were interruption in the energy supply to the pump in two cases (11%) and oxygen saturation < 70% in two cases. Thirteen patients (72%) survived and were discharged from the hospital. Among the nonsurvivors, there were two cases of brain death, two cases of multiple organ dysfunction syndrome, and one case of irreversible pulmonary fibrosis.
Conclusions:
Transportation with extracorporeal support occurred without serious complications, and the hospital survival rate was high.
Keywords:artificial respirationCritical illnessExtracorporeal membrane oxygenationIntensive care unitsRespiratory insufficiencyTransportation of patientsSee more -
Original Article
The practice of dentistry in intensive care units in Brazil
Rev Bras Ter Intensiva. 2018;30(3):327-332
Abstract
Original ArticleThe practice of dentistry in intensive care units in Brazil
Rev Bras Ter Intensiva. 2018;30(3):327-332
DOI 10.5935/0103-507X.20180044
Views0See moreABSTRACT
Objective:
To evaluate the practice of dentistry in intensive care units.
Methods:
An observational survey study was conducted in which questionnaires were sent via the online platform for collaboration in intensive care research in Brazil (AMIBnet). The study was carried out from June to October 2017. The questionnaires, which contained 26 closed questions about hospitals and dentistry practices in the intensive care units, were sent to 4,569 professionals from different specialties practicing in the units.
Results:
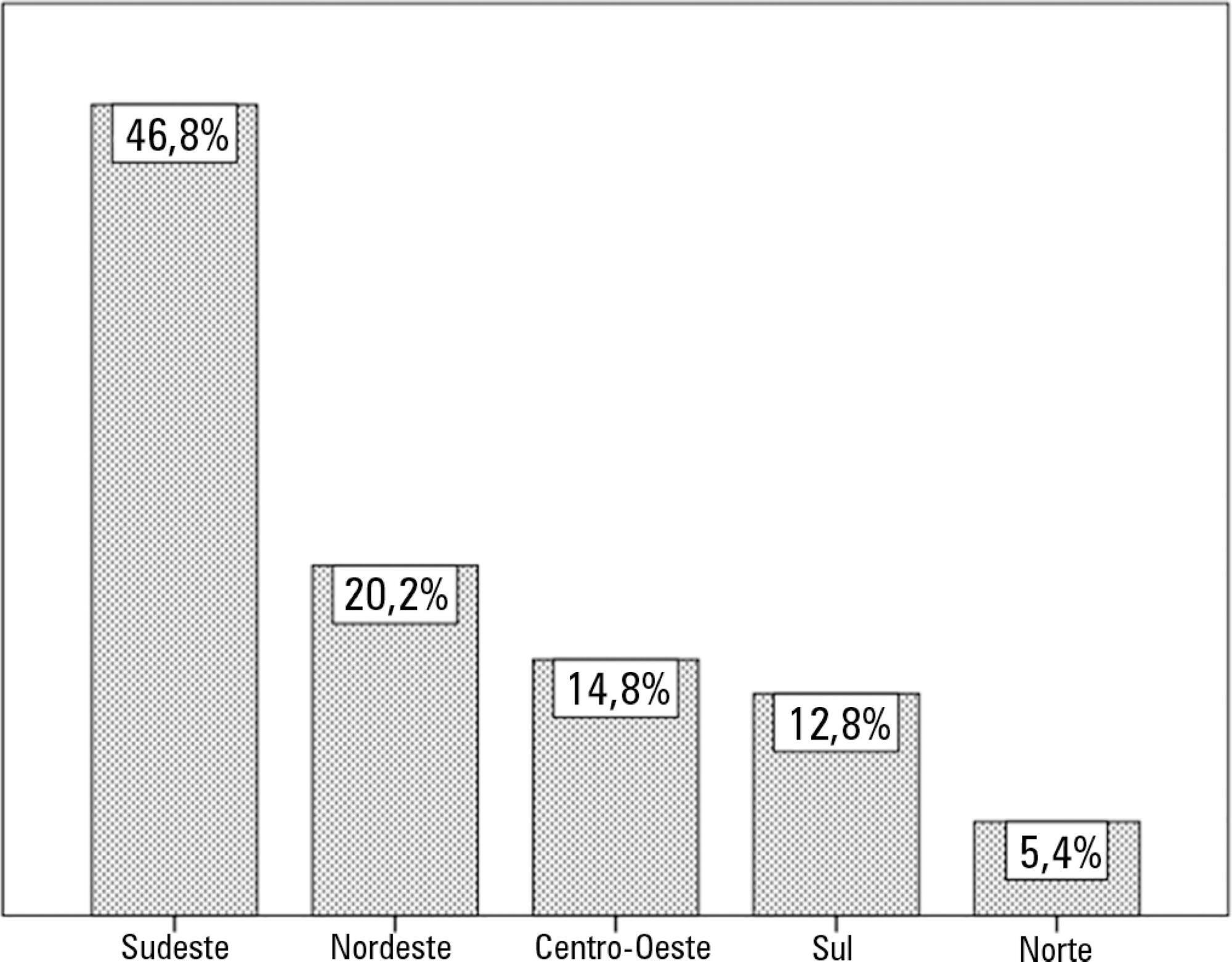
In total, 203 questionnaires were returned, resulting in a response rate of 4.44%. Most of the responses were from intensive care units in the Southeast region of the country (46.8%). Public hospitals (37.9%) and private hospitals (36.4%) had similar participation rates. Of the respondents, 55% indicated that a bedside dentistry service was present, and they were provided in different ways.
Conclusion:
The presence of dentistry services and oral health service delivery training and protocols were correlated. The oral care methods varied greatly among the intensive care units surveyed.
Views0Abstract
Original ArticleThe practice of dentistry in intensive care units in Brazil
Rev Bras Ter Intensiva. 2018;30(3):327-332
DOI 10.5935/0103-507X.20180044
Views0See moreABSTRACT
Objective:
To evaluate the practice of dentistry in intensive care units.
Methods:
An observational survey study was conducted in which questionnaires were sent via the online platform for collaboration in intensive care research in Brazil (AMIBnet). The study was carried out from June to October 2017. The questionnaires, which contained 26 closed questions about hospitals and dentistry practices in the intensive care units, were sent to 4,569 professionals from different specialties practicing in the units.
Results:
In total, 203 questionnaires were returned, resulting in a response rate of 4.44%. Most of the responses were from intensive care units in the Southeast region of the country (46.8%). Public hospitals (37.9%) and private hospitals (36.4%) had similar participation rates. Of the respondents, 55% indicated that a bedside dentistry service was present, and they were provided in different ways.
Conclusion:
The presence of dentistry services and oral health service delivery training and protocols were correlated. The oral care methods varied greatly among the intensive care units surveyed.
-
Original Article
Characteristics and outcome of burned children admitted to a pediatric intensive care unit
Rev Bras Ter Intensiva. 2018;30(3):333-337
Abstract
Original ArticleCharacteristics and outcome of burned children admitted to a pediatric intensive care unit
Rev Bras Ter Intensiva. 2018;30(3):333-337
DOI 10.5935/0103-507X.20180045
Views2See moreABSTRACT
Objective:
To analyze the characteristics and outcomes of children hospitalized for burns in a pediatric trauma intensive care unit for burn patients.
Methods:
An observational study was conducted through the retrospective analysis of children (< 16 years) admitted to the pediatric trauma intensive care unit for burn victims between January 2013 and December 2015. Sociodemographic and clinical variables were analyzed including the causal agent, burned body surface, presence of inhalation injury, length of hospital stay and mortality.
Results:
The study analyzed a sum of 140 patients; 61.8% were male, with a median age of 24 months and an overall mortality of 5%. The main cause of burns was scalding (51.4%), followed by accidents involving fire (38.6%) and electric shock (6.4%). Mechanical ventilation was used in 20.7% of the cases. Associated inhalation injury presented a relative risk of 6.1 (3.5 – 10.7) of needing ventilatory support and a relative risk of mortality of 14.1 (2.9 – 68.3) compared to patients without this associated injury. A significant connection was found between burned body surface and mortality (p < 0.002), reaching 80% in patients with a burned area greater than 50%. Patients who died had a significantly higher Tobiasen Abbreviated Burn Severity Index than survivors (9.6 ± 2.2 versus 4.4 ± 1.1; p < 0.001). A Tobiasen Abbreviated Burn Severity Index ≥ 7 represented a relative risk of death of 68.4 (95%CI 9.1 - 513.5).
Conclusion:
Scalding burns are quite frequent and are associated with high morbidity. Mortality is associated with the amount of burned body surface and the presence of inhalation injury. Special emphasis should be given to accidents involving fire, reinforcing proper diagnosis and treatment of inhalation injury.
Views2Abstract
Original ArticleCharacteristics and outcome of burned children admitted to a pediatric intensive care unit
Rev Bras Ter Intensiva. 2018;30(3):333-337
DOI 10.5935/0103-507X.20180045
Views2See moreABSTRACT
Objective:
To analyze the characteristics and outcomes of children hospitalized for burns in a pediatric trauma intensive care unit for burn patients.
Methods:
An observational study was conducted through the retrospective analysis of children (< 16 years) admitted to the pediatric trauma intensive care unit for burn victims between January 2013 and December 2015. Sociodemographic and clinical variables were analyzed including the causal agent, burned body surface, presence of inhalation injury, length of hospital stay and mortality.
Results:
The study analyzed a sum of 140 patients; 61.8% were male, with a median age of 24 months and an overall mortality of 5%. The main cause of burns was scalding (51.4%), followed by accidents involving fire (38.6%) and electric shock (6.4%). Mechanical ventilation was used in 20.7% of the cases. Associated inhalation injury presented a relative risk of 6.1 (3.5 – 10.7) of needing ventilatory support and a relative risk of mortality of 14.1 (2.9 – 68.3) compared to patients without this associated injury. A significant connection was found between burned body surface and mortality (p < 0.002), reaching 80% in patients with a burned area greater than 50%. Patients who died had a significantly higher Tobiasen Abbreviated Burn Severity Index than survivors (9.6 ± 2.2 versus 4.4 ± 1.1; p < 0.001). A Tobiasen Abbreviated Burn Severity Index ≥ 7 represented a relative risk of death of 68.4 (95%CI 9.1 - 513.5).
Conclusion:
Scalding burns are quite frequent and are associated with high morbidity. Mortality is associated with the amount of burned body surface and the presence of inhalation injury. Special emphasis should be given to accidents involving fire, reinforcing proper diagnosis and treatment of inhalation injury.
-
Original Article
Evaluation of the use of electronic medical record systems in Brazilian intensive care units
Rev Bras Ter Intensiva. 2018;30(3):338-346
Abstract
Original ArticleEvaluation of the use of electronic medical record systems in Brazilian intensive care units
Rev Bras Ter Intensiva. 2018;30(3):338-346
DOI 10.5935/0103-507X.20180057
Views0ABSTRACT
Objective:
To examine the prevalence of the use of electronic medical record systems in Brazilian intensive care units and the perceptions of intensive care physicians regarding the contribution of electronic medical record systems toward improving safety and quality in clinical practice.
Methods:
Using an online questionnaire, physicians working in Brazilian intensive care units answered questions about the use of electronic medical record systems in the hospitals in which they worked. They were asked about the types of electronic medical record systems used and their levels of satisfaction with these systems in terms of improving quality and safety.
Results:
Of the 4,772 invitations sent, 204 physicians responded to the questionnaire. Most used electronic medical record and prescription systems (92.6%), worked in private hospitals (43.1%), worked in general adult intensive care units (66.7%) and used Private System A (39.2%); most systems had been used for between 2 and 4 years (25.5%). Furthermore, the majority (84.6%) believed that the electronic system provided better quality than a paper system, and 76.7% believed that electronic systems provided greater safety than paper systems.
Conclusion:
Electronic medical record systems seem to be widely used by the Brazilian intensive care physicians who responded to the questionnaire and, according to the data, seem to provide greater quality and safety than do paper records.
Keywords:BrazilElectronic health recordsHealth information systemHealth information technologyHealth surveysIntensive care unitsMedical informaticsSee moreViews0Abstract
Original ArticleEvaluation of the use of electronic medical record systems in Brazilian intensive care units
Rev Bras Ter Intensiva. 2018;30(3):338-346
DOI 10.5935/0103-507X.20180057
Views0ABSTRACT
Objective:
To examine the prevalence of the use of electronic medical record systems in Brazilian intensive care units and the perceptions of intensive care physicians regarding the contribution of electronic medical record systems toward improving safety and quality in clinical practice.
Methods:
Using an online questionnaire, physicians working in Brazilian intensive care units answered questions about the use of electronic medical record systems in the hospitals in which they worked. They were asked about the types of electronic medical record systems used and their levels of satisfaction with these systems in terms of improving quality and safety.
Results:
Of the 4,772 invitations sent, 204 physicians responded to the questionnaire. Most used electronic medical record and prescription systems (92.6%), worked in private hospitals (43.1%), worked in general adult intensive care units (66.7%) and used Private System A (39.2%); most systems had been used for between 2 and 4 years (25.5%). Furthermore, the majority (84.6%) believed that the electronic system provided better quality than a paper system, and 76.7% believed that electronic systems provided greater safety than paper systems.
Conclusion:
Electronic medical record systems seem to be widely used by the Brazilian intensive care physicians who responded to the questionnaire and, according to the data, seem to provide greater quality and safety than do paper records.
Keywords:BrazilElectronic health recordsHealth information systemHealth information technologyHealth surveysIntensive care unitsMedical informaticsSee more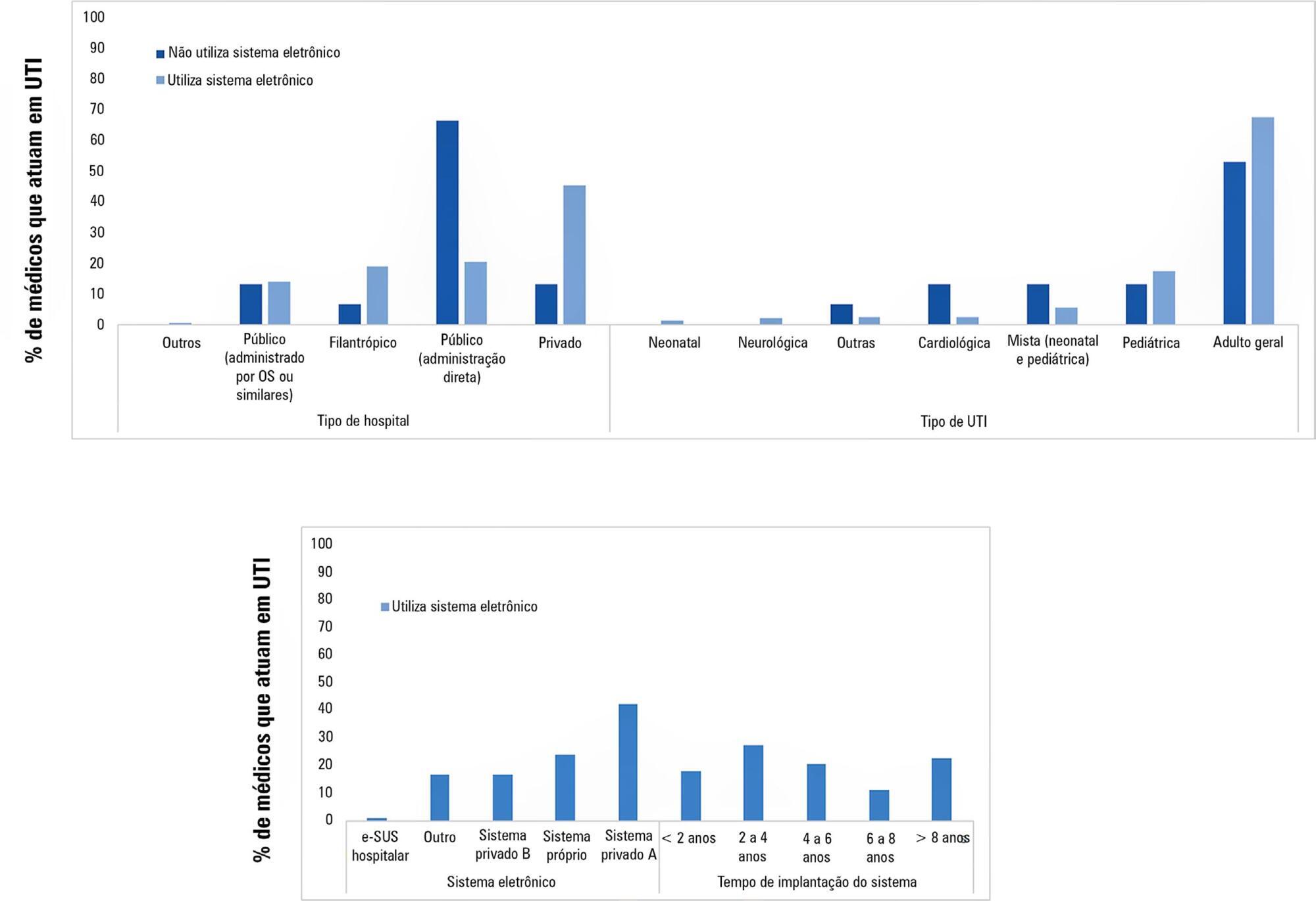
-
Original Article
Planning and understanding the intensive care network in the State of Rio de Janeiro (RJ), Brazil: a complex societal problem
Rev Bras Ter Intensiva. 2018;30(3):347-357
Abstract
Original ArticlePlanning and understanding the intensive care network in the State of Rio de Janeiro (RJ), Brazil: a complex societal problem
Rev Bras Ter Intensiva. 2018;30(3):347-357
DOI 10.5935/0103-507X.20180053
Views0ABSTRACT
Objectives:
To determine the optimal number of adult intensive care unit beds to reduce patient’s queue waiting time and to propose policy strategies.
Methods:
Multimethodological approach: (a) quantitative time series and queueing theory were used to predict the demand and estimate intensive care unit beds in different scenarios; (b) qualitative focus group and content analysis were used to explore physicians’ attitudes and provide insights into their behaviors and belief-driven healthcare delivery changes.
Results:
A total of 33,101 requests for 268 regulated intensive care unit beds in one year resulted in 25% admissions, 55% queue abandonment and 20% deaths. Maintaining current intensive care unit arrival and exit rates, there would need 628 beds to ensure a maximum wait time of six hours. A reduction of the current abandonment rates due to clinical improvement or the average intensive care unit length of stay would decrease the number of beds to 471 and 366, respectively. If both were reduced, the number would reach 275 beds. The interviews generated 3 main themes: (1) the doctor’s conflict: fair, legal, ethical and shared priorities in the decision-making process; (2) a failure of access: invisible queues and a lack of infrastructure; and (3) societal drama: deterioration of public policies and health care networks.
Conclusion:
The queue should be treated as a complex societal problem with a multifactorial origin requiring integrated solutions. Improving intensive care unit protocols and reengineering the general wards may decrease the length of stay. It is essential to redefine and consolidate the regulatory centers to organize the queue and provide available resources in a timely manner, by using priority criteria, working with stakeholders to guarantee clinical governance and network organization.
Keywords:Health policy, planning and managementHealth services accessibilityHospital bed capacityIntensive care unit organization & administrationManagementQualitative researchUnified Health SystemSee moreViews0Abstract
Original ArticlePlanning and understanding the intensive care network in the State of Rio de Janeiro (RJ), Brazil: a complex societal problem
Rev Bras Ter Intensiva. 2018;30(3):347-357
DOI 10.5935/0103-507X.20180053
Views0ABSTRACT
Objectives:
To determine the optimal number of adult intensive care unit beds to reduce patient’s queue waiting time and to propose policy strategies.
Methods:
Multimethodological approach: (a) quantitative time series and queueing theory were used to predict the demand and estimate intensive care unit beds in different scenarios; (b) qualitative focus group and content analysis were used to explore physicians’ attitudes and provide insights into their behaviors and belief-driven healthcare delivery changes.
Results:
A total of 33,101 requests for 268 regulated intensive care unit beds in one year resulted in 25% admissions, 55% queue abandonment and 20% deaths. Maintaining current intensive care unit arrival and exit rates, there would need 628 beds to ensure a maximum wait time of six hours. A reduction of the current abandonment rates due to clinical improvement or the average intensive care unit length of stay would decrease the number of beds to 471 and 366, respectively. If both were reduced, the number would reach 275 beds. The interviews generated 3 main themes: (1) the doctor’s conflict: fair, legal, ethical and shared priorities in the decision-making process; (2) a failure of access: invisible queues and a lack of infrastructure; and (3) societal drama: deterioration of public policies and health care networks.
Conclusion:
The queue should be treated as a complex societal problem with a multifactorial origin requiring integrated solutions. Improving intensive care unit protocols and reengineering the general wards may decrease the length of stay. It is essential to redefine and consolidate the regulatory centers to organize the queue and provide available resources in a timely manner, by using priority criteria, working with stakeholders to guarantee clinical governance and network organization.
Keywords:Health policy, planning and managementHealth services accessibilityHospital bed capacityIntensive care unit organization & administrationManagementQualitative researchUnified Health SystemSee more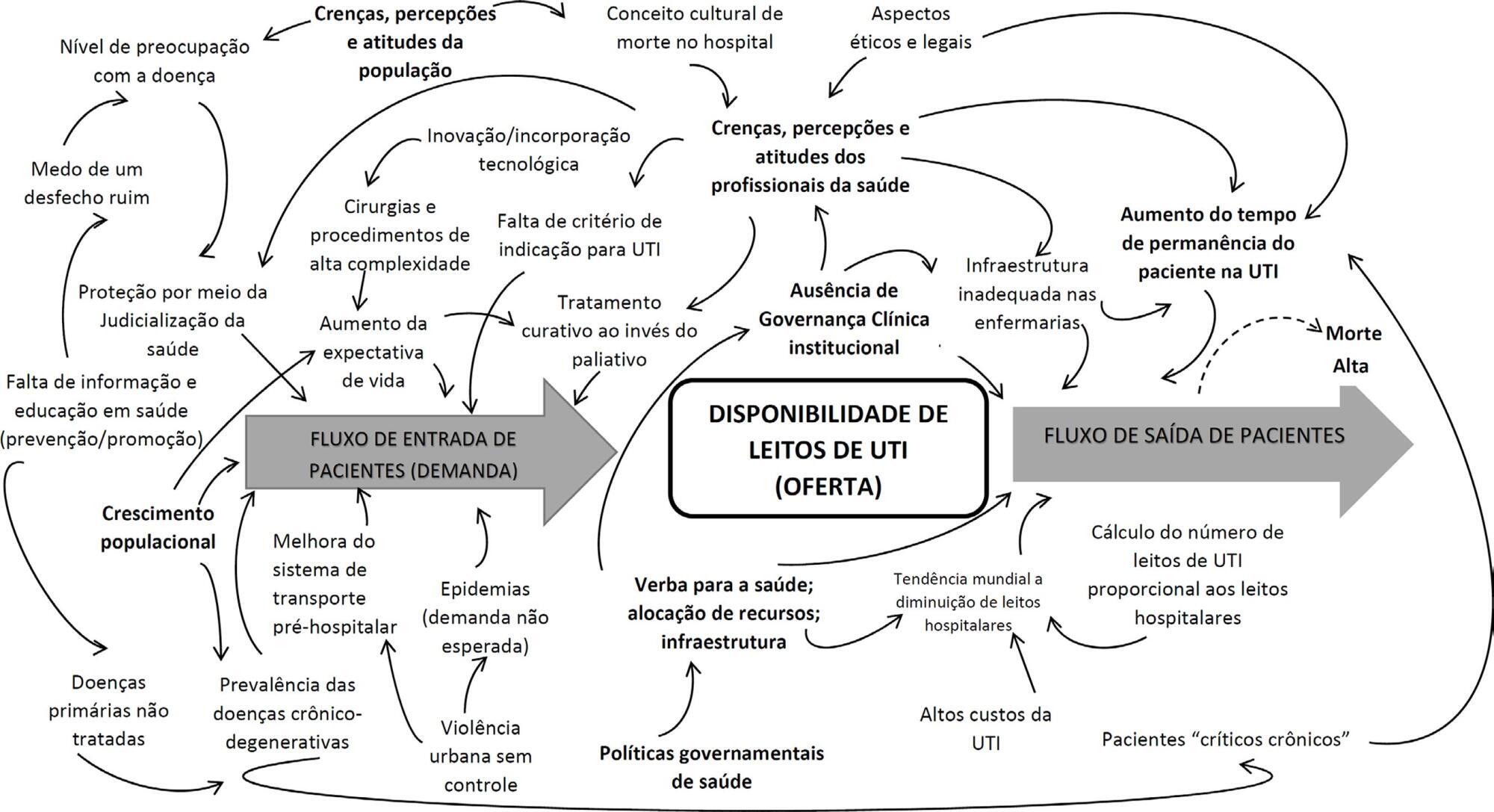
-
Review Article
Use of dietary fibers in enteral nutrition of critically ill patients: a systematic review
Rev Bras Ter Intensiva. 2018;30(3):358-365
Abstract
Review ArticleUse of dietary fibers in enteral nutrition of critically ill patients: a systematic review
Rev Bras Ter Intensiva. 2018;30(3):358-365
DOI 10.5935/0103-507X.20180050
Views0See moreABSTRACT
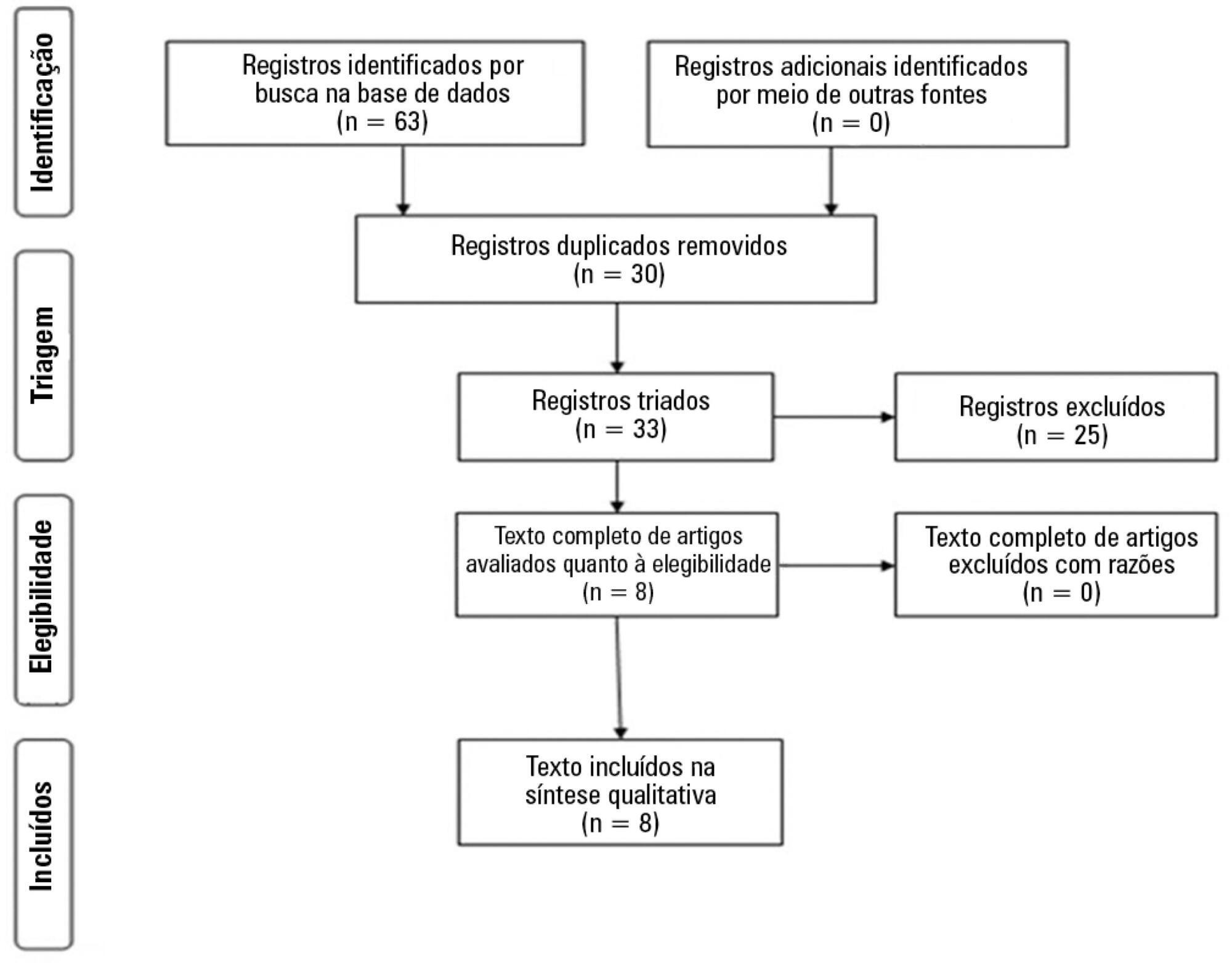
To meet the nutritional requirements of patients admitted to intensive care units, it is necessary to establish a diet schedule. Complications associated with enteral nutrition by tube feeding are not uncommon and may reduce the delivery of required nutrient to patients in intensive care units. Research on the osmolality, fat content, caloric intensity and fiber content of formulas are under way, and a substantial number of studies have focused on fiber content tolerability or symptom reduction. We conducted a systematic review of dietary fiber use and safety in critically ill patients in 8 studies based on diarrhea, other gastrointestinal symptoms (abdominal distension, gastric residual volume, vomiting and constipation), intestinal microbiota, length of stay in the intensive care unit and death. We discussed the results reported in the scientific literature and current recommendations. This contemporary approach demonstrated that the use of soluble fiber in all hemodynamically stable, critically ill patients is safe and should be considered beneficial for reducing the incidence of diarrhea in this population.
Views0Abstract
Review ArticleUse of dietary fibers in enteral nutrition of critically ill patients: a systematic review
Rev Bras Ter Intensiva. 2018;30(3):358-365
DOI 10.5935/0103-507X.20180050
Views0See moreABSTRACT
To meet the nutritional requirements of patients admitted to intensive care units, it is necessary to establish a diet schedule. Complications associated with enteral nutrition by tube feeding are not uncommon and may reduce the delivery of required nutrient to patients in intensive care units. Research on the osmolality, fat content, caloric intensity and fiber content of formulas are under way, and a substantial number of studies have focused on fiber content tolerability or symptom reduction. We conducted a systematic review of dietary fiber use and safety in critically ill patients in 8 studies based on diarrhea, other gastrointestinal symptoms (abdominal distension, gastric residual volume, vomiting and constipation), intestinal microbiota, length of stay in the intensive care unit and death. We discussed the results reported in the scientific literature and current recommendations. This contemporary approach demonstrated that the use of soluble fiber in all hemodynamically stable, critically ill patients is safe and should be considered beneficial for reducing the incidence of diarrhea in this population.
-
Review Article
Effectiveness of rapid response teams in reducing intrahospital cardiac arrests and deaths: a systematic review and meta-analysis
Rev Bras Ter Intensiva. 2018;30(3):366-375
Abstract
Review ArticleEffectiveness of rapid response teams in reducing intrahospital cardiac arrests and deaths: a systematic review and meta-analysis
Rev Bras Ter Intensiva. 2018;30(3):366-375
DOI 10.5935/0103-507X.20180049
Views0ABSTRACT
Objective:
To evaluate the effectiveness of rapid response teams using early identification of clinical deterioration in reducing the occurrence of in-hospital mortality and cardiorespiratory arrest.
Data sources:
The MEDLINE, LILACS, Cochrane Library, Center for Reviews and Dissemination databases were searched.
Study selection:
We included studies that evaluated the effectiveness of rapid response teams in adult hospital units, published in English, Portuguese, or Spanish, from 2000 to 2016; systematic reviews, clinical trials, cohort studies, and prepost ecological studies were eligible for inclusion. The quality of studies was independently assessed by two researchers using the Newcastle-Ottawa, modified Jadad, and Assessment of Multiple Systematic Reviews scales.
Data extractions:
The results were synthesized and tabulated. When risk measures were reported by the authors of the included studies, we estimated effectiveness as 1-RR or 1-OR. In pre-post studies, we estimated effectiveness as the percent decrease in rates following the intervention.
Results:
Overall, 278 studies were identified, 256 of which were excluded after abstract evaluation, and two of which were excluded after full text evaluation. In the meta-analysis of the studies reporting mortality data, we calculated a risk ratio of 0.85 (95%CI 0.76 – 0.94); and for studies reporting cardiac arrest data the estimated risk ratio was 0.65 (95%CI 0.49 – 0.87). Evidence was assessed as low quality due to the high heterogeneity and risk of bias in primary studies.
Conclusion:
We conclude that rapid response teams may reduce in-hospital mortality and cardiac arrests, although the quality of evidence for both outcomes is low.
Keywords:Heart arrestMortalityPatient care teamQuality of health careRapid response teamssystematic reviewSee moreViews0Abstract
Review ArticleEffectiveness of rapid response teams in reducing intrahospital cardiac arrests and deaths: a systematic review and meta-analysis
Rev Bras Ter Intensiva. 2018;30(3):366-375
DOI 10.5935/0103-507X.20180049
Views0ABSTRACT
Objective:
To evaluate the effectiveness of rapid response teams using early identification of clinical deterioration in reducing the occurrence of in-hospital mortality and cardiorespiratory arrest.
Data sources:
The MEDLINE, LILACS, Cochrane Library, Center for Reviews and Dissemination databases were searched.
Study selection:
We included studies that evaluated the effectiveness of rapid response teams in adult hospital units, published in English, Portuguese, or Spanish, from 2000 to 2016; systematic reviews, clinical trials, cohort studies, and prepost ecological studies were eligible for inclusion. The quality of studies was independently assessed by two researchers using the Newcastle-Ottawa, modified Jadad, and Assessment of Multiple Systematic Reviews scales.
Data extractions:
The results were synthesized and tabulated. When risk measures were reported by the authors of the included studies, we estimated effectiveness as 1-RR or 1-OR. In pre-post studies, we estimated effectiveness as the percent decrease in rates following the intervention.
Results:
Overall, 278 studies were identified, 256 of which were excluded after abstract evaluation, and two of which were excluded after full text evaluation. In the meta-analysis of the studies reporting mortality data, we calculated a risk ratio of 0.85 (95%CI 0.76 – 0.94); and for studies reporting cardiac arrest data the estimated risk ratio was 0.65 (95%CI 0.49 – 0.87). Evidence was assessed as low quality due to the high heterogeneity and risk of bias in primary studies.
Conclusion:
We conclude that rapid response teams may reduce in-hospital mortality and cardiac arrests, although the quality of evidence for both outcomes is low.
Keywords:Heart arrestMortalityPatient care teamQuality of health careRapid response teamssystematic reviewSee more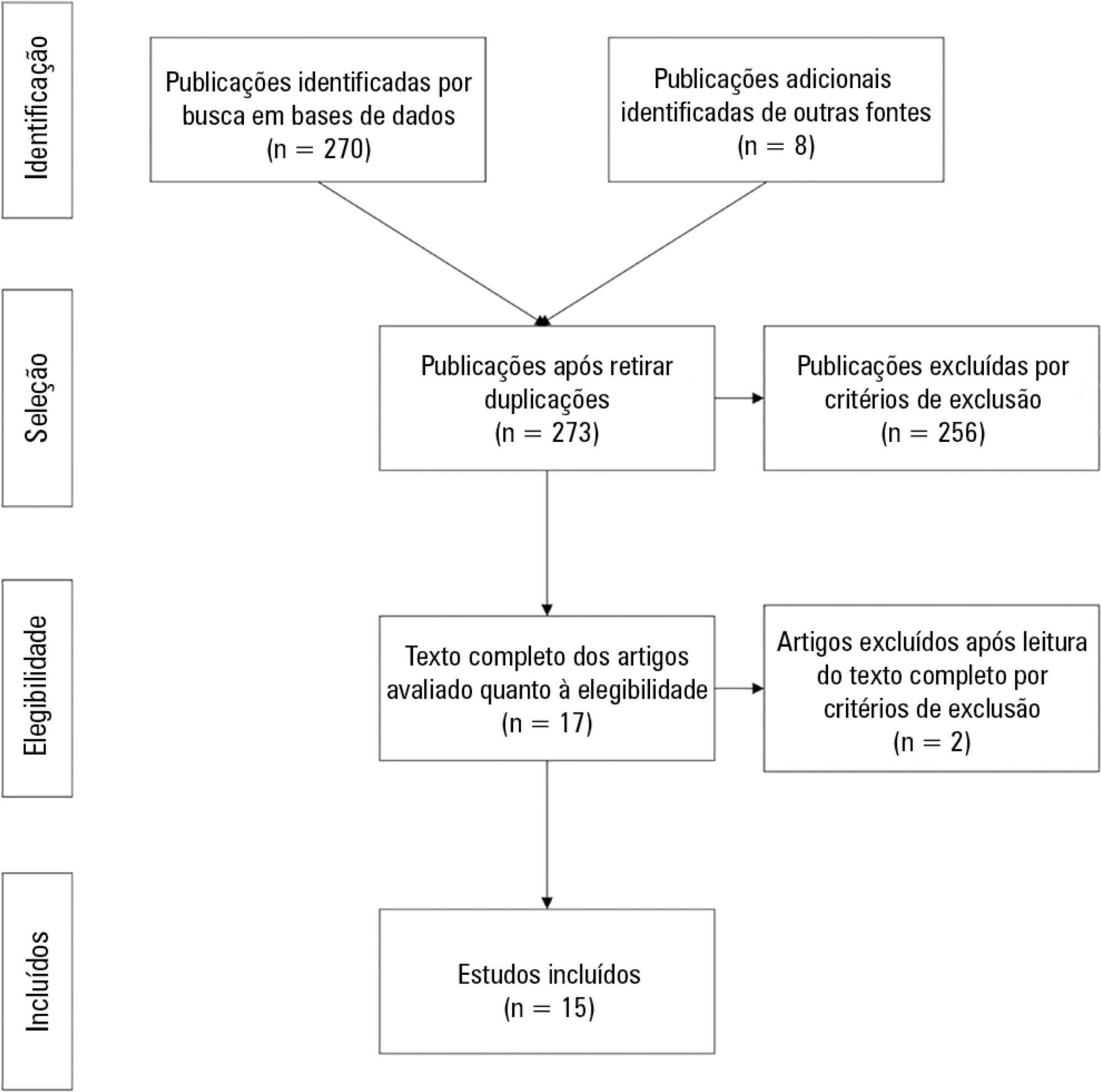
-
Review Article
Early versus delayed initiation of renal replacement therapy for acute kidney injury: an updated systematic review, meta-analysis, meta-regression and trial sequential analysis of randomized controlled trials
Rev Bras Ter Intensiva. 2018;30(3):376-384
Abstract
Review ArticleEarly versus delayed initiation of renal replacement therapy for acute kidney injury: an updated systematic review, meta-analysis, meta-regression and trial sequential analysis of randomized controlled trials
Rev Bras Ter Intensiva. 2018;30(3):376-384
DOI 10.5935/0103-507X.20180054
Views0ABSTRACT
Objective:
To evaluate whether early initiation of renal replacement therapy is associated with lower mortality in patients with acute kidney injury compared to delayed initiation.
Methods:
We performed a systematic review and meta-analysis of randomized controlled trials comparing early versus delayed initiation of renal replacement therapy in patients with acute kidney injury without the life-threatening acute kidney injury-related symptoms of fluid overload or metabolic disorders. Two investigators extracted the data from the selected studies. The Cochrane Risk of Bias Tool was used to assess the quality of the studies, and the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach was used to test the overall quality of the evidence.
Results:
Six randomized controlled trials (1,292 patients) were included. There was no statistically significant difference between early and delayed initiation of renal replacement therapy regarding the primary outcome (OR 0.82; 95%CI, 0.48 – 1.42; p = 0.488), but there was an increased risk of catheter-related bloodstream infection when renal replacement therapy was initiated early (OR 1.77; 95%CI, 1.01 – 3.11; p = 0.047). The quality of evidence generated by our meta-analysis for the primary outcome was considered low due to the risk of bias of the included studies and the heterogeneity among them.
Conclusion:
Early initiation of renal replacement therapy is not associated with improved survival. However, the quality of the current evidence is low, and the criteria used for -early- and -delayed- initiation of renal replacement therapy are too heterogeneous among studies.
Keywords:Acute kidney injuryCritically illMeta-analysisRandomized controlled trialRenal replacement therapysystematic reviewSee moreViews0Abstract
Review ArticleEarly versus delayed initiation of renal replacement therapy for acute kidney injury: an updated systematic review, meta-analysis, meta-regression and trial sequential analysis of randomized controlled trials
Rev Bras Ter Intensiva. 2018;30(3):376-384
DOI 10.5935/0103-507X.20180054
Views0ABSTRACT
Objective:
To evaluate whether early initiation of renal replacement therapy is associated with lower mortality in patients with acute kidney injury compared to delayed initiation.
Methods:
We performed a systematic review and meta-analysis of randomized controlled trials comparing early versus delayed initiation of renal replacement therapy in patients with acute kidney injury without the life-threatening acute kidney injury-related symptoms of fluid overload or metabolic disorders. Two investigators extracted the data from the selected studies. The Cochrane Risk of Bias Tool was used to assess the quality of the studies, and the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach was used to test the overall quality of the evidence.
Results:
Six randomized controlled trials (1,292 patients) were included. There was no statistically significant difference between early and delayed initiation of renal replacement therapy regarding the primary outcome (OR 0.82; 95%CI, 0.48 – 1.42; p = 0.488), but there was an increased risk of catheter-related bloodstream infection when renal replacement therapy was initiated early (OR 1.77; 95%CI, 1.01 – 3.11; p = 0.047). The quality of evidence generated by our meta-analysis for the primary outcome was considered low due to the risk of bias of the included studies and the heterogeneity among them.
Conclusion:
Early initiation of renal replacement therapy is not associated with improved survival. However, the quality of the current evidence is low, and the criteria used for -early- and -delayed- initiation of renal replacement therapy are too heterogeneous among studies.
Keywords:Acute kidney injuryCritically illMeta-analysisRandomized controlled trialRenal replacement therapysystematic reviewSee more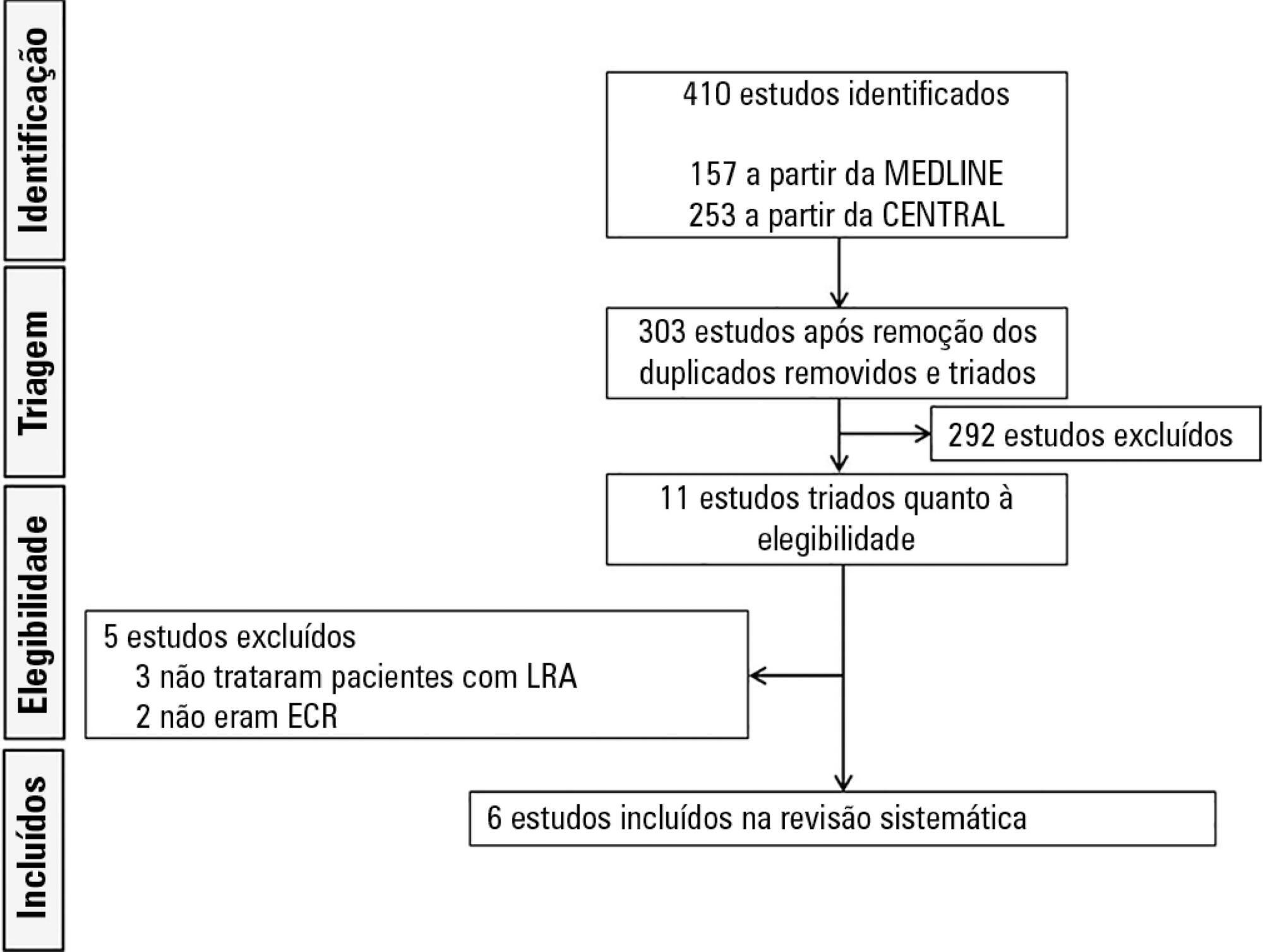
-
Review Article
Non-invasive hemodynamic evaluation by Doppler echocardiography
Rev Bras Ter Intensiva. 2018;30(3):385-393
Abstract
Review ArticleNon-invasive hemodynamic evaluation by Doppler echocardiography
Rev Bras Ter Intensiva. 2018;30(3):385-393
DOI 10.5935/0103-507X.20180055
Views0ABSTRACT
The approach for treating a hemodynamically unstable patient remains a diagnostic and therapeutic challenge. Stabilization of the patient should be rapid and effective, but there is not much room for error. This narrow window of intervention makes it necessary to use rapid and accurate hemodynamic evaluation methods. Echocardiography is the method of choice for the bedside evaluation of patients in circulatory shock. In fact, it was intensive care physicians who recognized the potential of Doppler echocardiography for the initial approach to patients in circulatory failure. An echocardiogram allows rapid anatomical and functional cardiac evaluation, which may include non-invasive hemodynamic evaluation using a Doppler study. Such an integrated study may provide data of extreme importance for understanding the mechanisms underlying the hemodynamic instability of the patient to allow the rapid institution of appropriate therapeutic measures. In the present article, we describe the most relevant echocardiographic findings using a practical approach for critical patients with hemodynamic instability.
Keywords:Echocardiography, DopplerHemodynamicSee moreViews0Abstract
Review ArticleNon-invasive hemodynamic evaluation by Doppler echocardiography
Rev Bras Ter Intensiva. 2018;30(3):385-393
DOI 10.5935/0103-507X.20180055
Views0ABSTRACT
The approach for treating a hemodynamically unstable patient remains a diagnostic and therapeutic challenge. Stabilization of the patient should be rapid and effective, but there is not much room for error. This narrow window of intervention makes it necessary to use rapid and accurate hemodynamic evaluation methods. Echocardiography is the method of choice for the bedside evaluation of patients in circulatory shock. In fact, it was intensive care physicians who recognized the potential of Doppler echocardiography for the initial approach to patients in circulatory failure. An echocardiogram allows rapid anatomical and functional cardiac evaluation, which may include non-invasive hemodynamic evaluation using a Doppler study. Such an integrated study may provide data of extreme importance for understanding the mechanisms underlying the hemodynamic instability of the patient to allow the rapid institution of appropriate therapeutic measures. In the present article, we describe the most relevant echocardiographic findings using a practical approach for critical patients with hemodynamic instability.
Keywords:Echocardiography, DopplerHemodynamicSee more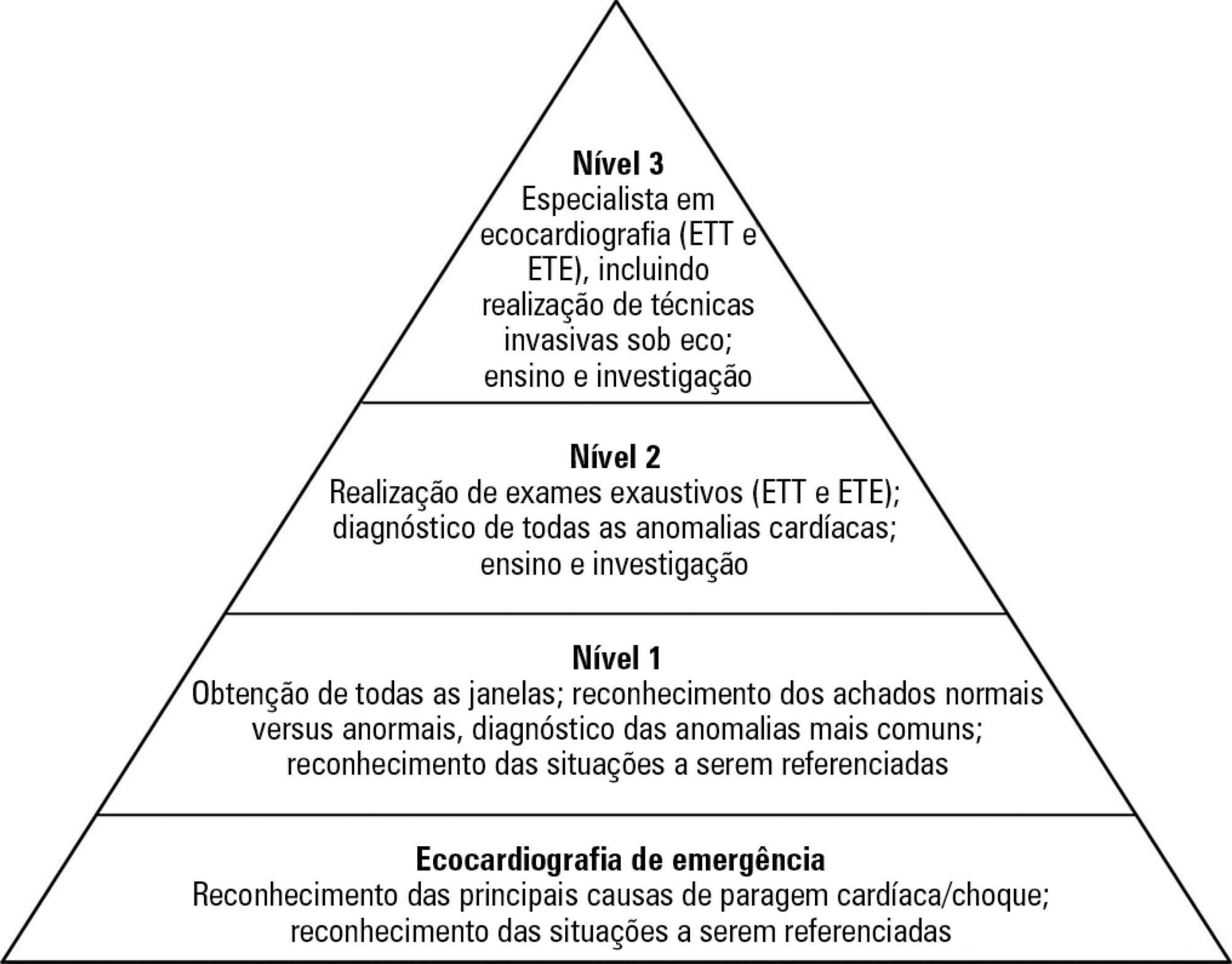
-
Case Report
Compensatory effect of fibrinogen in a patient with bone marrow aplasia, septic shock, and severe thrombocytopenia guided by thromboelastometry: a case report
Rev Bras Ter Intensiva. 2018;30(3):394-397
Abstract
Case ReportCompensatory effect of fibrinogen in a patient with bone marrow aplasia, septic shock, and severe thrombocytopenia guided by thromboelastometry: a case report
Rev Bras Ter Intensiva. 2018;30(3):394-397
DOI 10.5935/0103-507X.20180056
Views0ABSTRACT
Platelet transfusion is a common practice to prevent spontaneous bleeding or bleeding due to invasive procedures. Transfusion of allogeneic blood components is associated with increased mortality and a worse clinical outcome. The clot strength is assessed by thromboelastometry and determined by the interaction between platelets and fibrinogen. The compensatory effect of high levels of fibrinogen on clot strength in patients with thrombocytopenia has been demonstrated in different clinical settings including sepsis. We report the case of a patient with severe thrombocytopenia whose thromboelastometry showed clot strength that was compensated for by the increase in plasma fibrinogen levels as an acute phase reactant of septic patients. Here, we report a case of a 62-year-old female diagnosed with bone marrow aplasia admitted in the intensive care unit with septic shock and severe thrombocytopenia. During the first 24 hours in the intensive care unit, she presented acute respiratory insufficiency and circulatory shock. The use of invasive mechanical ventilation and norepinephrine was required. Her chest X-ray showed bilateral lung injury. Thus, bronchoscopy with bronchoalveolar lavage was requested. Thromboelastometry was performed and resulted in a normal coagulable profile. Despite severe thrombocytopenia (1,000/mm3), fibrinogen levels were increased (1,050mg/dL) due to septic shock. Bronchoscopy was performed without any active or further bleeding. Here, we report the use of thromboelastometry in the diagnosis of coagulation disorders, preventing unnecessary prophylactic platelet transfusion.
Keywords:Bone marrow diseasesBone marrow/abnormalitiesFibrinogenSeptic shockThrombocytopeniaThromboelastographySee moreViews0Abstract
Case ReportCompensatory effect of fibrinogen in a patient with bone marrow aplasia, septic shock, and severe thrombocytopenia guided by thromboelastometry: a case report
Rev Bras Ter Intensiva. 2018;30(3):394-397
DOI 10.5935/0103-507X.20180056
Views0ABSTRACT
Platelet transfusion is a common practice to prevent spontaneous bleeding or bleeding due to invasive procedures. Transfusion of allogeneic blood components is associated with increased mortality and a worse clinical outcome. The clot strength is assessed by thromboelastometry and determined by the interaction between platelets and fibrinogen. The compensatory effect of high levels of fibrinogen on clot strength in patients with thrombocytopenia has been demonstrated in different clinical settings including sepsis. We report the case of a patient with severe thrombocytopenia whose thromboelastometry showed clot strength that was compensated for by the increase in plasma fibrinogen levels as an acute phase reactant of septic patients. Here, we report a case of a 62-year-old female diagnosed with bone marrow aplasia admitted in the intensive care unit with septic shock and severe thrombocytopenia. During the first 24 hours in the intensive care unit, she presented acute respiratory insufficiency and circulatory shock. The use of invasive mechanical ventilation and norepinephrine was required. Her chest X-ray showed bilateral lung injury. Thus, bronchoscopy with bronchoalveolar lavage was requested. Thromboelastometry was performed and resulted in a normal coagulable profile. Despite severe thrombocytopenia (1,000/mm3), fibrinogen levels were increased (1,050mg/dL) due to septic shock. Bronchoscopy was performed without any active or further bleeding. Here, we report the use of thromboelastometry in the diagnosis of coagulation disorders, preventing unnecessary prophylactic platelet transfusion.
Keywords:Bone marrow diseasesBone marrow/abnormalitiesFibrinogenSeptic shockThrombocytopeniaThromboelastographySee more
-
Letter to the Editor
Reply to: The Epimed Monitor ICU Database®: a cloud-based national registry for adult intensive care unit patients in Brazil
Rev Bras Ter Intensiva. 2018;30(3):398-398
Abstract
Letter to the EditorReply to: The Epimed Monitor ICU Database®: a cloud-based national registry for adult intensive care unit patients in Brazil
Rev Bras Ter Intensiva. 2018;30(3):398-398
Views0Abstract
Letter to the EditorReply to: The Epimed Monitor ICU Database®: a cloud-based national registry for adult intensive care unit patients in Brazil
Rev Bras Ter Intensiva. 2018;30(3):398-398
-
Letter to the Editor
Use of topical glutamine as an adjuvant for the treatment of oral ulcers
Rev Bras Ter Intensiva. 2018;30(3):399-399
Abstract
Letter to the EditorUse of topical glutamine as an adjuvant for the treatment of oral ulcers
Rev Bras Ter Intensiva. 2018;30(3):399-399
DOI 10.5935/0103-507X.20180047
Views1To the Editor Glutamine is the most commonly found free amino acid in the human body. When applied to clinical lesions, glutamine can aid in the recovery of severe presentations, reduce infections and even decrease the length of hospital stay because it causes symptom remission. For patients with severe systemic presentations, this amino acid is […]See moreViews1Abstract
Letter to the EditorUse of topical glutamine as an adjuvant for the treatment of oral ulcers
Rev Bras Ter Intensiva. 2018;30(3):399-399
DOI 10.5935/0103-507X.20180047
Views1To the Editor Glutamine is the most commonly found free amino acid in the human body. When applied to clinical lesions, glutamine can aid in the recovery of severe presentations, reduce infections and even decrease the length of hospital stay because it causes symptom remission. For patients with severe systemic presentations, this amino acid is […]See more
Volume Articles - Critical Care Science (CCS)
