-
Original Articles
Perfusion index for assessing microvascular reactivity in septic shock after fluid resuscitation
Rev Bras Ter Intensiva. 2018;30(2):135-143
Abstract
Original ArticlesPerfusion index for assessing microvascular reactivity in septic shock after fluid resuscitation
Rev Bras Ter Intensiva. 2018;30(2):135-143
DOI 10.5935/0103-507X.20180027
Views0See moreABSTRACT
Objective:
Microcirculation disturbances are implicated in the prognosis of septic shock. Microvascular hyporesponsiveness can be assessed by an oximetry-derived perfusion index and reactive hyperemia. Using this perfusion index, we investigated reactive hyperemia and its relationship with peripheral perfusion and clinical-hemodynamic parameters in septic shock.
Methods:
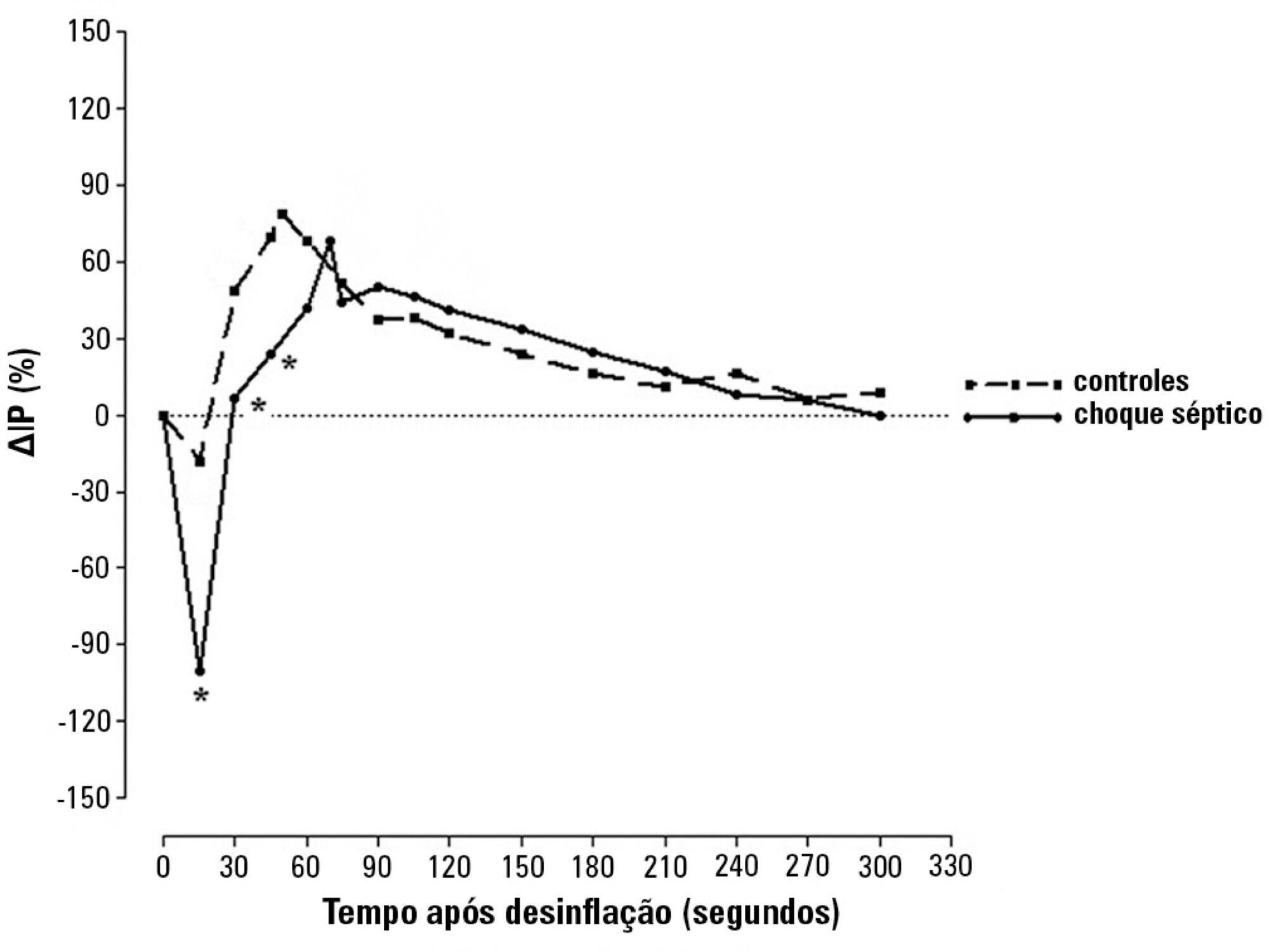
Eighty-two patients were evaluated: 47 with septic shock and 35 controls. Tests were performed within 24 hours after admission. The perfusion index was evaluated before and after a 3-min blood flow occlusion using a time-response analysis for 5 min. The perfusion index was also evaluated in the hyperemic phases and was mainly derived by mechanosensitive (ΔPI0-60) and metabolic mechanisms (ΔPI60-120). Correlation tests were performed between reactive hyperemia and clinical-hemodynamic data.
Results:
Reactive hyperemia measured by the perfusion index was significantly lower in patients with septic shock, but this was only observed for the first 45 seconds after cuff-deflation. In the remaining period, there were no statistical differences between the groups. The peaks in the perfusion index were similar between groups, although the peak was reached more slowly in the septic group. Values of ΔPI0-60 were lower in shock [01% (-19% – -40%) versus 39% (6% – 75%); p = 0.001]. However, ΔPI60-120 was similar between the groups [43% (18% – 93%) versus 48% (18% – 98%); p = 0.58]. The time-to-peak of the perfusion index was correlated positively with the SOFA scores and negatively with C-reactive protein; the peak of the perfusion index was positively correlated with vasopressor doses; and the ΔPI60-120 values were positively correlated with C-reactive protein and vasopressor doses. No other significant correlations occurred.
Conclusions:
This perfusion index-based study suggests that septic shock promotes initial peripheral vascular hyporesponsiveness and preserves posterior vascular reactivity to a considerable degree. These results demonstrate a time-dependent peripheral hyperemic response and a significant ischemic reserve in septic shock.
Views0

Abstract
Original ArticlesPerfusion index for assessing microvascular reactivity in septic shock after fluid resuscitation
Rev Bras Ter Intensiva. 2018;30(2):135-143
DOI 10.5935/0103-507X.20180027
Views0See moreABSTRACT
Objective:
Microcirculation disturbances are implicated in the prognosis of septic shock. Microvascular hyporesponsiveness can be assessed by an oximetry-derived perfusion index and reactive hyperemia. Using this perfusion index, we investigated reactive hyperemia and its relationship with peripheral perfusion and clinical-hemodynamic parameters in septic shock.
Methods:
Eighty-two patients were evaluated: 47 with septic shock and 35 controls. Tests were performed within 24 hours after admission. The perfusion index was evaluated before and after a 3-min blood flow occlusion using a time-response analysis for 5 min. The perfusion index was also evaluated in the hyperemic phases and was mainly derived by mechanosensitive (ΔPI0-60) and metabolic mechanisms (ΔPI60-120). Correlation tests were performed between reactive hyperemia and clinical-hemodynamic data.
Results:
Reactive hyperemia measured by the perfusion index was significantly lower in patients with septic shock, but this was only observed for the first 45 seconds after cuff-deflation. In the remaining period, there were no statistical differences between the groups. The peaks in the perfusion index were similar between groups, although the peak was reached more slowly in the septic group. Values of ΔPI0-60 were lower in shock [01% (-19% – -40%) versus 39% (6% – 75%); p = 0.001]. However, ΔPI60-120 was similar between the groups [43% (18% – 93%) versus 48% (18% – 98%); p = 0.58]. The time-to-peak of the perfusion index was correlated positively with the SOFA scores and negatively with C-reactive protein; the peak of the perfusion index was positively correlated with vasopressor doses; and the ΔPI60-120 values were positively correlated with C-reactive protein and vasopressor doses. No other significant correlations occurred.
Conclusions:
This perfusion index-based study suggests that septic shock promotes initial peripheral vascular hyporesponsiveness and preserves posterior vascular reactivity to a considerable degree. These results demonstrate a time-dependent peripheral hyperemic response and a significant ischemic reserve in septic shock.
-
Original Articles
Sizing the lung in dogs: the inspiratory capacity defines the tidal volume
Rev Bras Ter Intensiva. 2018;30(2):144-152
Abstract
Original ArticlesSizing the lung in dogs: the inspiratory capacity defines the tidal volume
Rev Bras Ter Intensiva. 2018;30(2):144-152
DOI 10.5935/0103-507X.20180028
Views0See moreABSTRACT
Objective:
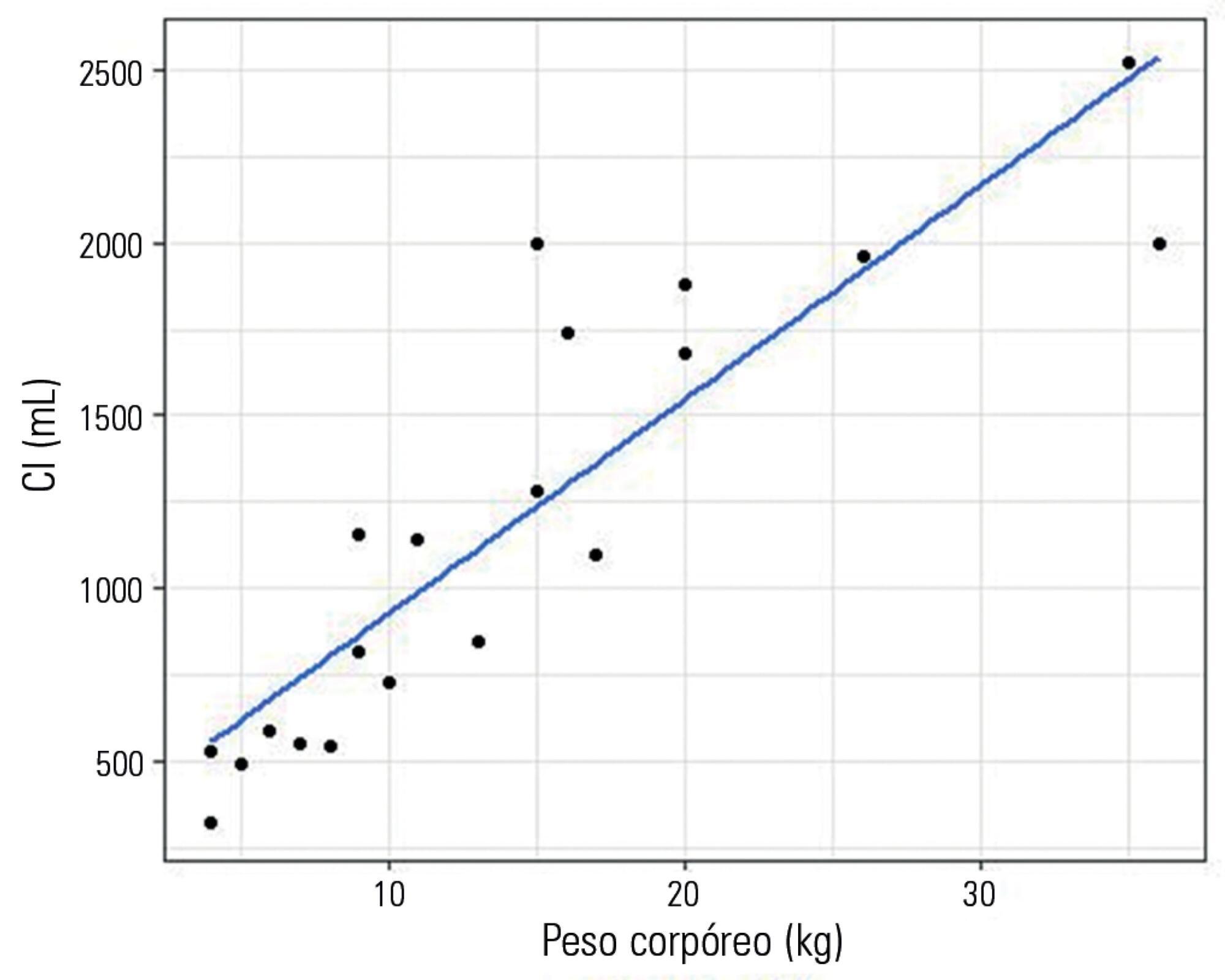
To evaluate a novel physiological approach for setting the tidal volume in mechanical ventilation according to inspiratory capacity, and to determine if it results in an appropriate mechanical and gas exchange measurements in healthy and critically ill dogs.
Methods:
Twenty healthy animals were included in the study to assess the tidal volume expressed as a percentage of inspiratory capacity. For inspiratory capacity measurement, the mechanical ventilator was set as follows: pressure control mode with 35cmH2O of inspired pressure and zero end-expiratory pressure for 5 seconds. Subsequently, the animals were randomized into four groups and ventilated with a tidal volume corresponding to the different percentages of inspiratory capacity. Subsequently, ten critically ill dogs were studied.
Results:
Healthy dogs ventilated with a tidal volume of 17% of the inspiratory capacity showed normal respiratory mechanics and presented expected PaCO2 values more frequently than the other groups. The respiratory system and transpulmonary driving pressure were significantly higher among the critically ill dogs but below 15 cmH2O in all cases.
Conclusions:
The tidal volume based on the inspiratory capacity of each animal has proven to be a useful and simple tool when setting ventilator parameters. A similar approach should also be evaluated in other species, including human beings, if we consider the potential limitations of tidal volume titration based on the calculated ideal body weight.
Views0Abstract
Original ArticlesSizing the lung in dogs: the inspiratory capacity defines the tidal volume
Rev Bras Ter Intensiva. 2018;30(2):144-152
DOI 10.5935/0103-507X.20180028
Views0See moreABSTRACT
Objective:
To evaluate a novel physiological approach for setting the tidal volume in mechanical ventilation according to inspiratory capacity, and to determine if it results in an appropriate mechanical and gas exchange measurements in healthy and critically ill dogs.
Methods:
Twenty healthy animals were included in the study to assess the tidal volume expressed as a percentage of inspiratory capacity. For inspiratory capacity measurement, the mechanical ventilator was set as follows: pressure control mode with 35cmH2O of inspired pressure and zero end-expiratory pressure for 5 seconds. Subsequently, the animals were randomized into four groups and ventilated with a tidal volume corresponding to the different percentages of inspiratory capacity. Subsequently, ten critically ill dogs were studied.
Results:
Healthy dogs ventilated with a tidal volume of 17% of the inspiratory capacity showed normal respiratory mechanics and presented expected PaCO2 values more frequently than the other groups. The respiratory system and transpulmonary driving pressure were significantly higher among the critically ill dogs but below 15 cmH2O in all cases.
Conclusions:
The tidal volume based on the inspiratory capacity of each animal has proven to be a useful and simple tool when setting ventilator parameters. A similar approach should also be evaluated in other species, including human beings, if we consider the potential limitations of tidal volume titration based on the calculated ideal body weight.
-
Original Articles
Prognostic factors among critically ill patients with community-acquired acute bacterial meningitis and acute kidney injury
Rev Bras Ter Intensiva. 2018;30(2):153-159
Abstract
Original ArticlesPrognostic factors among critically ill patients with community-acquired acute bacterial meningitis and acute kidney injury
Rev Bras Ter Intensiva. 2018;30(2):153-159
DOI 10.5935/0103-507X.20180030
Views0See moreABSTRACT
Objective:
To investigate prognostic factors among critically ill patients with community-acquired bacterial meningitis and acute kidney injury.
Methods:
A retrospective study including patients admitted to a tertiary infectious disease hospital in Fortaleza, Brazil diagnosed with community-acquired bacterial meningitis complicated with acute kidney injury. Factors associated with death, mechanical ventilation and use of vasopressors were investigated.
Results:
Forty-one patients were included, with a mean age of 41.6 ± 15.5 years; 56% were males. Mean time between intensive care unit admission and acute kidney injury diagnosis was 5.8 ± 10.6 days. Overall mortality was 53.7%. According to KDIGO criteria, 10 patients were classified as stage 1 (24.4%), 18 as stage 2 (43.9%) and 13 as stage 3 (31.7%). KDIGO 3 significantly increased mortality (OR = 6.67; 95%CI = 1.23 – 36.23; p = 0.028). Thrombocytopenia was not associated with higher mortality, but it was a risk factor for KDIGO 3 (OR = 5.67; 95%CI = 1.25 – 25.61; p = 0.024) and for mechanical ventilation (OR = 6.25; 95%CI = 1.33 – 29.37; p = 0.02). Patients who needed mechanical ventilation by 48 hours from acute kidney injury diagnosis had higher urea (44.6 versus 74mg/dL, p = 0.039) and sodium (138.6 versus 144.1mEq/L; p = 0.036).
Conclusion:
Mortality among critically ill patients with community-acquired bacterial meningitis and acute kidney injury is high. Acute kidney injury severity was associated with even higher mortality. Thrombocytopenia was associated with severer acute kidney injury. Higher urea was an earlier predictor of severer acute kidney injury than was creatinine.
Views0Abstract
Original ArticlesPrognostic factors among critically ill patients with community-acquired acute bacterial meningitis and acute kidney injury
Rev Bras Ter Intensiva. 2018;30(2):153-159
DOI 10.5935/0103-507X.20180030
Views0See moreABSTRACT
Objective:
To investigate prognostic factors among critically ill patients with community-acquired bacterial meningitis and acute kidney injury.
Methods:
A retrospective study including patients admitted to a tertiary infectious disease hospital in Fortaleza, Brazil diagnosed with community-acquired bacterial meningitis complicated with acute kidney injury. Factors associated with death, mechanical ventilation and use of vasopressors were investigated.
Results:
Forty-one patients were included, with a mean age of 41.6 ± 15.5 years; 56% were males. Mean time between intensive care unit admission and acute kidney injury diagnosis was 5.8 ± 10.6 days. Overall mortality was 53.7%. According to KDIGO criteria, 10 patients were classified as stage 1 (24.4%), 18 as stage 2 (43.9%) and 13 as stage 3 (31.7%). KDIGO 3 significantly increased mortality (OR = 6.67; 95%CI = 1.23 – 36.23; p = 0.028). Thrombocytopenia was not associated with higher mortality, but it was a risk factor for KDIGO 3 (OR = 5.67; 95%CI = 1.25 – 25.61; p = 0.024) and for mechanical ventilation (OR = 6.25; 95%CI = 1.33 – 29.37; p = 0.02). Patients who needed mechanical ventilation by 48 hours from acute kidney injury diagnosis had higher urea (44.6 versus 74mg/dL, p = 0.039) and sodium (138.6 versus 144.1mEq/L; p = 0.036).
Conclusion:
Mortality among critically ill patients with community-acquired bacterial meningitis and acute kidney injury is high. Acute kidney injury severity was associated with even higher mortality. Thrombocytopenia was associated with severer acute kidney injury. Higher urea was an earlier predictor of severer acute kidney injury than was creatinine.
-
Original Articles
Reducing malnutrition in critically ill pediatric patients
Rev Bras Ter Intensiva. 2018;30(2):160-165
Abstract
Original ArticlesReducing malnutrition in critically ill pediatric patients
Rev Bras Ter Intensiva. 2018;30(2):160-165
DOI 10.5935/0103-507X.20180034
Views1See moreABSTRACT
Objective:
To compare the prevalence of malnutrition during two time periods in a pediatric intensive care unit.
Methods:
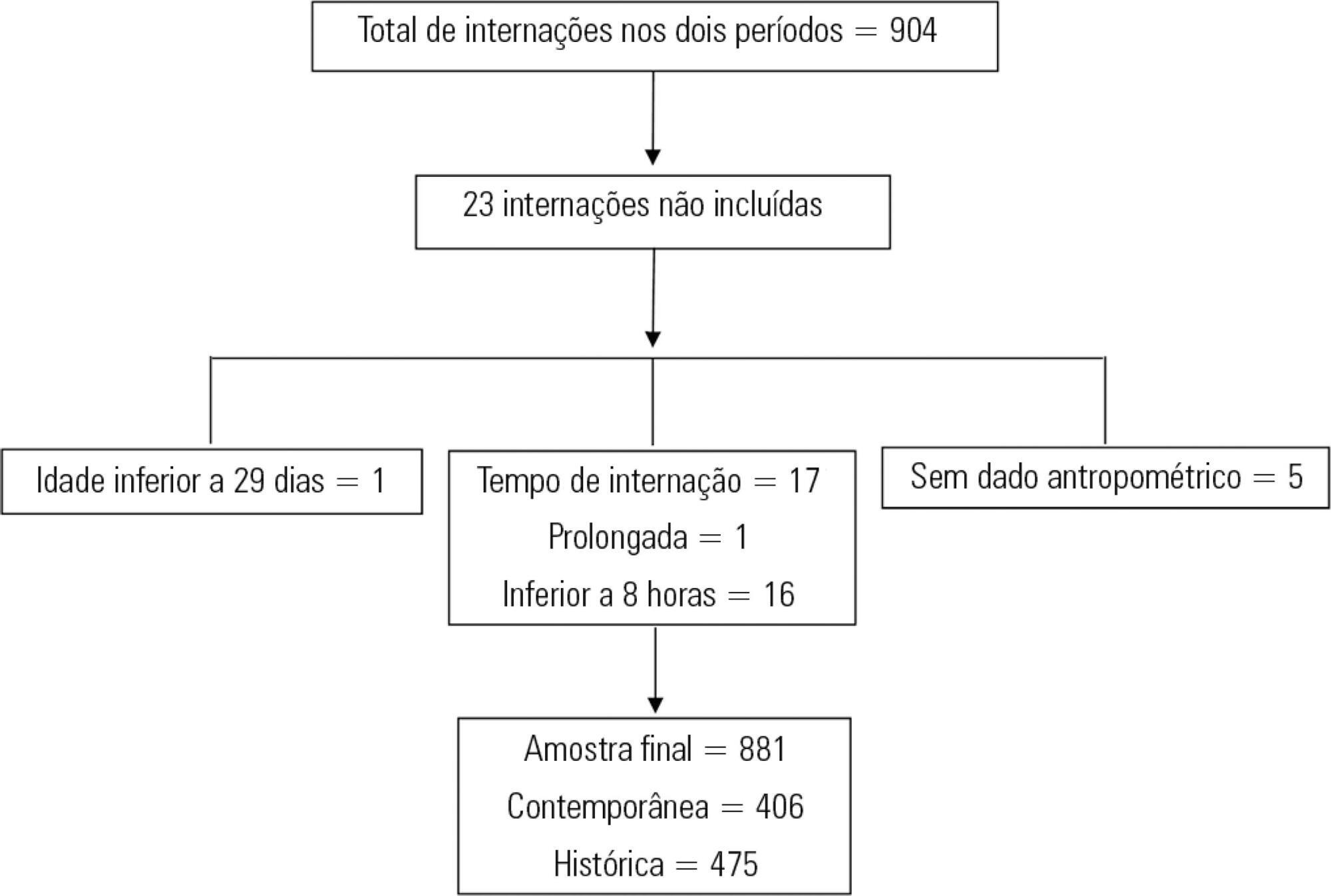
This was a retrospective cross-sectional study of patients admitted to the pediatric intensive care unit of a university hospital during two one-year periods with an interval of four years between them. Nutritional evaluation was conducted based on weight and height measured at admission. The body mass index-for-age was the parameter chosen to evaluate nutritional status, as classified according to the World Health Organization, according to age group.
Results:
The total sample size was 881 (406 in the contemporary sample and 475 in the historical sample). There was a significant reduction in malnutrition in the contemporary sample (p = 0.03). Malnourishment in patients in the historical sample was significantly associated with mortality and length of stay, while malnourishment in patients in the contemporary sample was not associated with worse outcomes.
Conclusion:
There was a significant reduction in malnutrition among patients in the same pediatric intensive care unit when comparing the two time periods. Our findings of a change in nutritional profile in critically ill patients corroborate the nutritional status data of children and adolescents worldwide.
Views1Abstract
Original ArticlesReducing malnutrition in critically ill pediatric patients
Rev Bras Ter Intensiva. 2018;30(2):160-165
DOI 10.5935/0103-507X.20180034
Views1See moreABSTRACT
Objective:
To compare the prevalence of malnutrition during two time periods in a pediatric intensive care unit.
Methods:
This was a retrospective cross-sectional study of patients admitted to the pediatric intensive care unit of a university hospital during two one-year periods with an interval of four years between them. Nutritional evaluation was conducted based on weight and height measured at admission. The body mass index-for-age was the parameter chosen to evaluate nutritional status, as classified according to the World Health Organization, according to age group.
Results:
The total sample size was 881 (406 in the contemporary sample and 475 in the historical sample). There was a significant reduction in malnutrition in the contemporary sample (p = 0.03). Malnourishment in patients in the historical sample was significantly associated with mortality and length of stay, while malnourishment in patients in the contemporary sample was not associated with worse outcomes.
Conclusion:
There was a significant reduction in malnutrition among patients in the same pediatric intensive care unit when comparing the two time periods. Our findings of a change in nutritional profile in critically ill patients corroborate the nutritional status data of children and adolescents worldwide.
-
Original Articles
Predictors of de novo atrial fibrillation in a non-cardiac intensive care unit
Rev Bras Ter Intensiva. 2018;30(2):166-173
Abstract
Original ArticlesPredictors of de novo atrial fibrillation in a non-cardiac intensive care unit
Rev Bras Ter Intensiva. 2018;30(2):166-173
DOI 10.5935/0103-507X.20180022
Views1See moreABSTRACT
Objective:
To assess the predictors of de novo atrial fibrillation in patients in a non-cardiac intensive care unit.
Methods:
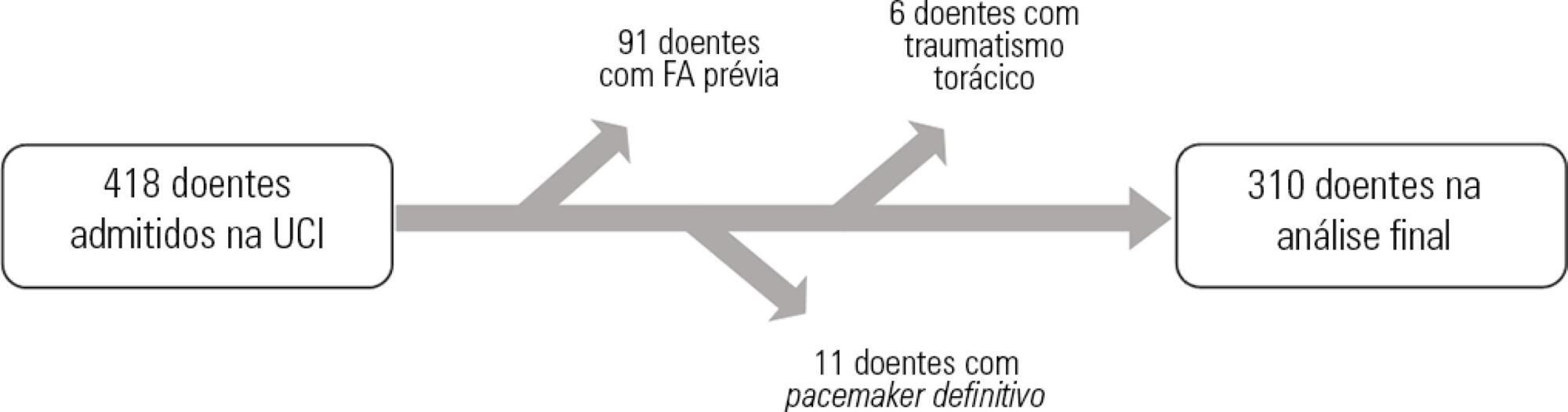
A total of 418 hospitalized patients were analyzed between January and September 2016 in a non-cardiac intensive care unit. Clinical characteristics, interventions, and biochemical markers were recorded during hospitalization. In-hospital mortality and length of hospital stay in the intensive care unit were also evaluated.
Results:
A total of 310 patients were included. The mean age of the patients was 61.0 ± 18.3 years, 49.4% were male, and 23.5% presented de novo atrial fibrillation. The multivariate model identified previous stroke (OR = 10.09; p = 0.016) and elevated levels of pro-B type natriuretic peptide (proBNP, OR = 1.28 for each 1,000pg/mL increment; p = 0.004) as independent predictors of de novo atrial fibrillation. Analysis of the proBNP receiver operating characteristic curve for prediction of de novo atrial fibrillation revealed an area under the curve of 0.816 (p < 0.001), with a sensitivity of 65.2% and a specificity of 82% for proBNP > 5,666pg/mL. There were no differences in mortality (p = 0.370), but the lengths of hospital stay (p = 0.002) and stay in the intensive care unit (p = 0.031) were higher in patients with de novo atrial fibrillation.
Conclusions:
A history of previous stroke and elevated proBNP during hospitalization were independent predictors of de novo atrial fibrillation in the polyvalent intensive care unit. The proBNP is a useful and easy- and quick-access tool in the stratification of atrial fibrillation risk.
Views1Abstract
Original ArticlesPredictors of de novo atrial fibrillation in a non-cardiac intensive care unit
Rev Bras Ter Intensiva. 2018;30(2):166-173
DOI 10.5935/0103-507X.20180022
Views1See moreABSTRACT
Objective:
To assess the predictors of de novo atrial fibrillation in patients in a non-cardiac intensive care unit.
Methods:
A total of 418 hospitalized patients were analyzed between January and September 2016 in a non-cardiac intensive care unit. Clinical characteristics, interventions, and biochemical markers were recorded during hospitalization. In-hospital mortality and length of hospital stay in the intensive care unit were also evaluated.
Results:
A total of 310 patients were included. The mean age of the patients was 61.0 ± 18.3 years, 49.4% were male, and 23.5% presented de novo atrial fibrillation. The multivariate model identified previous stroke (OR = 10.09; p = 0.016) and elevated levels of pro-B type natriuretic peptide (proBNP, OR = 1.28 for each 1,000pg/mL increment; p = 0.004) as independent predictors of de novo atrial fibrillation. Analysis of the proBNP receiver operating characteristic curve for prediction of de novo atrial fibrillation revealed an area under the curve of 0.816 (p < 0.001), with a sensitivity of 65.2% and a specificity of 82% for proBNP > 5,666pg/mL. There were no differences in mortality (p = 0.370), but the lengths of hospital stay (p = 0.002) and stay in the intensive care unit (p = 0.031) were higher in patients with de novo atrial fibrillation.
Conclusions:
A history of previous stroke and elevated proBNP during hospitalization were independent predictors of de novo atrial fibrillation in the polyvalent intensive care unit. The proBNP is a useful and easy- and quick-access tool in the stratification of atrial fibrillation risk.
-
Original Articles
Assessment of the neuropsychomotor development in the first year of life of premature infants with and without bronchopulmonary dysplasia
Rev Bras Ter Intensiva. 2018;30(2):174-180
Abstract
Original ArticlesAssessment of the neuropsychomotor development in the first year of life of premature infants with and without bronchopulmonary dysplasia
Rev Bras Ter Intensiva. 2018;30(2):174-180
DOI 10.5935/0103-507X.20180023
Views0ABSTRACT
Objective:
To compare the neuropsychomotor development in the first year of life of premature infants with and without bronchopulmonary dysplasia.
Methods:
A cross-sectional retrospective study was conducted between January 1, 2014, and December 30, 2015, with premature infants weighing < 1,500g at birth and diagnosed with bronchopulmonary dysplasia at the corrected ages of 6 and 9 months, assessed using the DENVER II Developmental Screening Test. Quantitative variables were described as the means, medians and standard deviations. Variables with normal distribution were tested using Student's t test; otherwise, the Mann-Whitney test was used, considering significance at p-value < 0.05. Qualitative variables were expressed as frequencies and percentages. Logistic regression was used with odds ratio analysis to evaluate the effects of other variables as risk factors for changes in neuropsychomotor development.
Results:
Infants with bronchopulmonary dysplasia showed greater developmental delay compared with those without bronchopulmonary dysplasia (p-value = 0.001). The factors associated with a higher incidence of changes in neuropsychomotor development, in addition to bronchopulmonary dysplasia, were antenatal steroid, gender, birth weight, 5-minute Apgar score, Score for Neonatal Acute Physiology-Perinatal Extension, duration of oxygen therapy, duration of mechanical ventilation and length of hospital stay. Other variables may also have influenced the result, such as drug use by mothers of infants with bronchopulmonary dysplasia.
Conclusion:
Bronchopulmonary dysplasia associated with other pre- and postnatal factors may be considered a risk factor for delayed neuropsychomotor development in the first year of life in premature infants born weighing less than 1,500g.
Keywords:Bronchopulmonary dysplasiaDevelopmental disabilitiesInfant, low birth weightInfant, prematurerisk factorsSee moreViews0Abstract
Original ArticlesAssessment of the neuropsychomotor development in the first year of life of premature infants with and without bronchopulmonary dysplasia
Rev Bras Ter Intensiva. 2018;30(2):174-180
DOI 10.5935/0103-507X.20180023
Views0ABSTRACT
Objective:
To compare the neuropsychomotor development in the first year of life of premature infants with and without bronchopulmonary dysplasia.
Methods:
A cross-sectional retrospective study was conducted between January 1, 2014, and December 30, 2015, with premature infants weighing < 1,500g at birth and diagnosed with bronchopulmonary dysplasia at the corrected ages of 6 and 9 months, assessed using the DENVER II Developmental Screening Test. Quantitative variables were described as the means, medians and standard deviations. Variables with normal distribution were tested using Student's t test; otherwise, the Mann-Whitney test was used, considering significance at p-value < 0.05. Qualitative variables were expressed as frequencies and percentages. Logistic regression was used with odds ratio analysis to evaluate the effects of other variables as risk factors for changes in neuropsychomotor development.
Results:
Infants with bronchopulmonary dysplasia showed greater developmental delay compared with those without bronchopulmonary dysplasia (p-value = 0.001). The factors associated with a higher incidence of changes in neuropsychomotor development, in addition to bronchopulmonary dysplasia, were antenatal steroid, gender, birth weight, 5-minute Apgar score, Score for Neonatal Acute Physiology-Perinatal Extension, duration of oxygen therapy, duration of mechanical ventilation and length of hospital stay. Other variables may also have influenced the result, such as drug use by mothers of infants with bronchopulmonary dysplasia.
Conclusion:
Bronchopulmonary dysplasia associated with other pre- and postnatal factors may be considered a risk factor for delayed neuropsychomotor development in the first year of life in premature infants born weighing less than 1,500g.
Keywords:Bronchopulmonary dysplasiaDevelopmental disabilitiesInfant, low birth weightInfant, prematurerisk factorsSee more -
Original Articles
APACHE IV score in postoperative kidney transplantation
Rev Bras Ter Intensiva. 2018;30(2):181-186
Abstract
Original ArticlesAPACHE IV score in postoperative kidney transplantation
Rev Bras Ter Intensiva. 2018;30(2):181-186
DOI 10.5935/0103-507X.20180032
Views0See moreABSTRACT
Objectives:
To evaluate the calibration and discrimination of APACHE IV in the postoperative period after kidney transplantation.
Methods:
This clinical cohort study included 986 hospitalized adult patients in the immediate postoperative period after kidney transplantation, in a single center in southern Brazil.
Results:
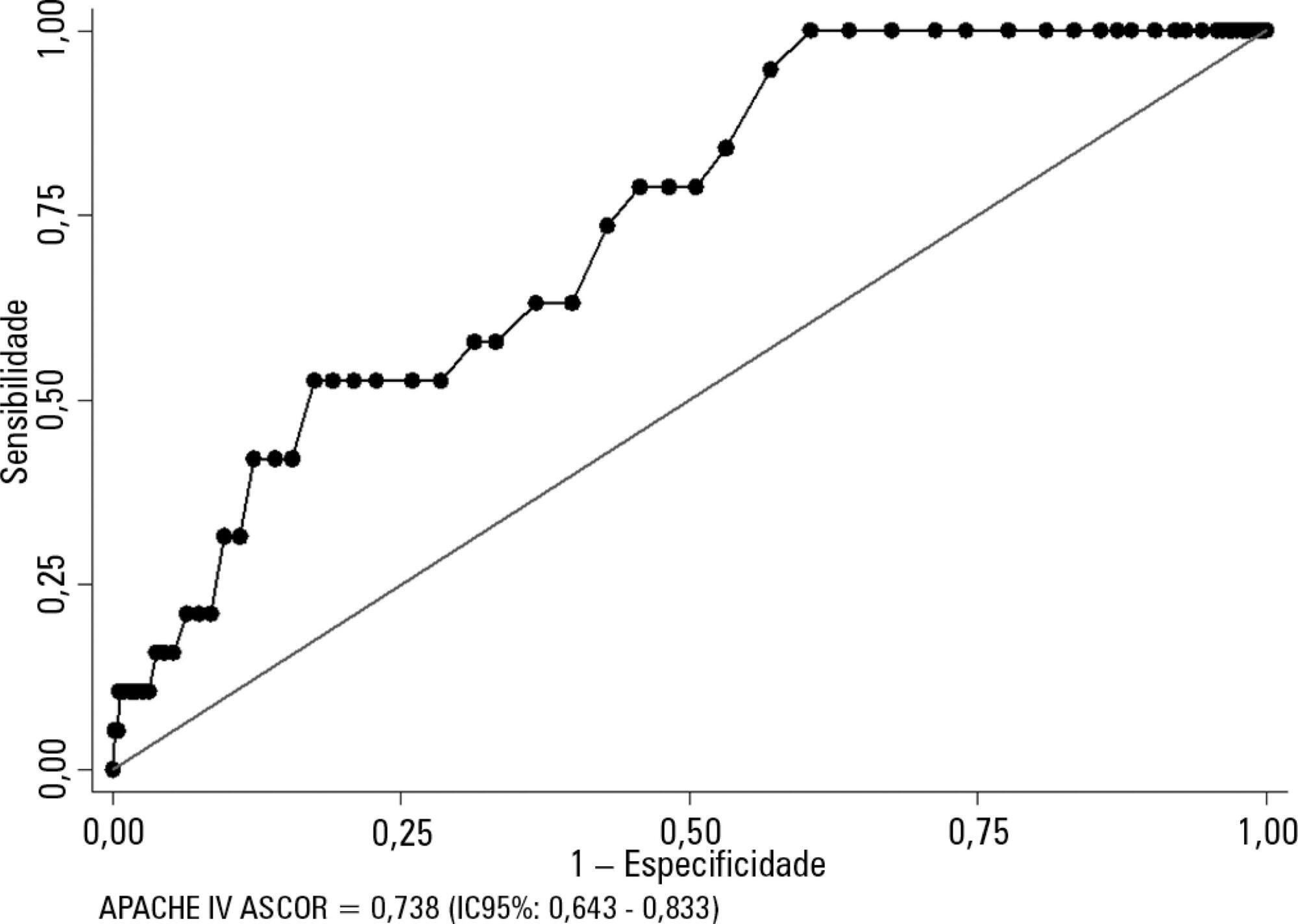
Kidney transplant patients who died in hospital had significantly higher APACHE IV values and higher predicted mortality. The APACHE IV score showed adequate calibration (H-L 11.24 p = 0.188) and a good discrimination ROC curve of 0.738 (95%CI 0.643 – 0.833, p < 0.001), although SMR overestimated mortality (SMR = 0.73; 95%CI: 0.24 - 1.42, p = 0.664).
Conclusions:
The APACHE IV score showed adequate performance for predicting hospital outcomes in the postoperative period for kidney transplant recipients.
Views0Abstract
Original ArticlesAPACHE IV score in postoperative kidney transplantation
Rev Bras Ter Intensiva. 2018;30(2):181-186
DOI 10.5935/0103-507X.20180032
Views0See moreABSTRACT
Objectives:
To evaluate the calibration and discrimination of APACHE IV in the postoperative period after kidney transplantation.
Methods:
This clinical cohort study included 986 hospitalized adult patients in the immediate postoperative period after kidney transplantation, in a single center in southern Brazil.
Results:
Kidney transplant patients who died in hospital had significantly higher APACHE IV values and higher predicted mortality. The APACHE IV score showed adequate calibration (H-L 11.24 p = 0.188) and a good discrimination ROC curve of 0.738 (95%CI 0.643 – 0.833, p < 0.001), although SMR overestimated mortality (SMR = 0.73; 95%CI: 0.24 - 1.42, p = 0.664).
Conclusions:
The APACHE IV score showed adequate performance for predicting hospital outcomes in the postoperative period for kidney transplant recipients.
-
Original Articles
Clinical attitudes and perceived barriers to early mobilization of critically ill patients in adult intensive care units
Rev Bras Ter Intensiva. 2018;30(2):187-194
Abstract
Original ArticlesClinical attitudes and perceived barriers to early mobilization of critically ill patients in adult intensive care units
Rev Bras Ter Intensiva. 2018;30(2):187-194
DOI 10.5935/0103-507X.20180037
Views0ABSTRACT
Objective:
To investigate the knowledge of multi-professional staff members about the early mobilization of critically ill adult patients and identify attitudes and perceived barriers to its application.
Methods:
A cross-sectional study was conducted during the second semester of 2016 with physicians, nursing professionals and physical therapists from six intensive care units at two teaching hospitals. Questions were answered on a 5-point Likert scale and analyzed as proportions of professionals who agreed or disagreed with statements. The chi-square and Fisher’s exact tests were used to investigate differences in the responses according to educational/training level, previous experience with early mobilization and years of experience in intensive care units.
Results:
The questionnaire was answered by 98 out of 514 professionals (response rate: 19%). The acknowledged benefits of early mobilization were maintenance of muscle strength (53%) and shortened length of mechanical ventilation (83%). Favorable attitudes toward early mobilization included recognition that its benefits for patients under mechanical ventilation exceed the risks for both patients and staff, that early mobilization should be routinely performed via nursing and physical therapy protocols, and readiness to change the parameters of mechanical ventilation and reduce sedation to facilitate the early mobilization of patients. The main barriers mentioned were the unavailability of professionals and time to mobilize patients, excessive sedation, delirium, risk of musculoskeletal self-injury and excessive stress at work.
Conclusion:
The participants were aware of the benefits of early mobilization and manifested attitudes favorable to its application. However, the actual performance of early mobilization was perceived as a challenge, mainly due to the lack of professionals and time, excessive sedation, delirium, risk of musculoskeletal self-injury and excessive stress at work.
Keywords:Early ambulationMuscle weaknessPatient care teamPhysical therapy modalitiesRespiration, artificialSee moreViews0Abstract
Original ArticlesClinical attitudes and perceived barriers to early mobilization of critically ill patients in adult intensive care units
Rev Bras Ter Intensiva. 2018;30(2):187-194
DOI 10.5935/0103-507X.20180037
Views0ABSTRACT
Objective:
To investigate the knowledge of multi-professional staff members about the early mobilization of critically ill adult patients and identify attitudes and perceived barriers to its application.
Methods:
A cross-sectional study was conducted during the second semester of 2016 with physicians, nursing professionals and physical therapists from six intensive care units at two teaching hospitals. Questions were answered on a 5-point Likert scale and analyzed as proportions of professionals who agreed or disagreed with statements. The chi-square and Fisher’s exact tests were used to investigate differences in the responses according to educational/training level, previous experience with early mobilization and years of experience in intensive care units.
Results:
The questionnaire was answered by 98 out of 514 professionals (response rate: 19%). The acknowledged benefits of early mobilization were maintenance of muscle strength (53%) and shortened length of mechanical ventilation (83%). Favorable attitudes toward early mobilization included recognition that its benefits for patients under mechanical ventilation exceed the risks for both patients and staff, that early mobilization should be routinely performed via nursing and physical therapy protocols, and readiness to change the parameters of mechanical ventilation and reduce sedation to facilitate the early mobilization of patients. The main barriers mentioned were the unavailability of professionals and time to mobilize patients, excessive sedation, delirium, risk of musculoskeletal self-injury and excessive stress at work.
Conclusion:
The participants were aware of the benefits of early mobilization and manifested attitudes favorable to its application. However, the actual performance of early mobilization was perceived as a challenge, mainly due to the lack of professionals and time, excessive sedation, delirium, risk of musculoskeletal self-injury and excessive stress at work.
Keywords:Early ambulationMuscle weaknessPatient care teamPhysical therapy modalitiesRespiration, artificialSee more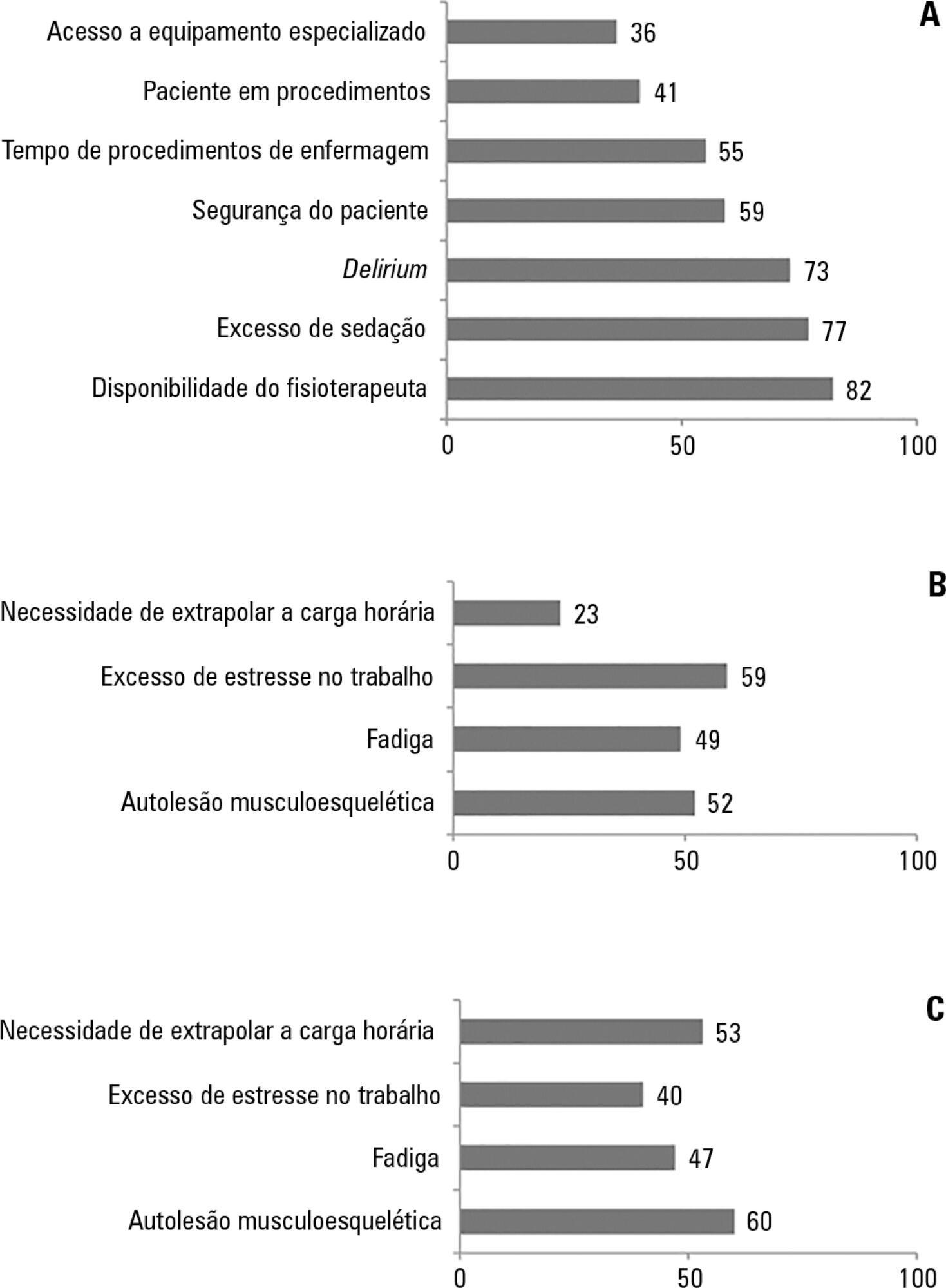
-
Original Articles
Translation and cross-cultural adaptation of the Cornell Assessment of Pediatric Delirium scale for the Portuguese language
Rev Bras Ter Intensiva. 2018;30(2):195-200
Abstract
Original ArticlesTranslation and cross-cultural adaptation of the Cornell Assessment of Pediatric Delirium scale for the Portuguese language
Rev Bras Ter Intensiva. 2018;30(2):195-200
DOI 10.5935/0103-507X.20180033
Views0See moreABSTRACT
Objective:
This study sought to translate the Cornell Assessment of Pediatric Delirium from English into Brazilian Portuguese and cross-culturally adapt it for use in Brazil.
Methods:
Following the authorization granted by its main author, the processes of translation and cross-cultural adaptation were performed with regard to the Cornell Assessment of Pediatric Delirium in accordance with the following internationally recommended steps: translation of the original into Portuguese by two native speakers of the target language; synthesis of the translated versions; back-translation by two native speakers of the original language; review and harmonization of the back-translation; a review of the Portuguese version of the Cornell Assessment of Pediatric Delirium by an expert panel composed of specialists; pretesting including assessments of clarity, comprehensibility, and acceptability of the translated version using a sample of the target population; and finishing modifications to achieve the final version.
Results:
The translation and cross-cultural adaptation of the Cornell Assessment of Pediatric Delirium followed international recommendations. The linguistic and semantic issues that emerged during the process were discussed by the expert panel, which unanimously agreed to slight modifications. During pretesting, the Cornell Assessment of Pediatric Delirium was administered to 30 eligible children, twice per day; the final version was easy to understand, could be completed quickly, and showed a high inter-rater correlation coefficient (0.955).
Conclusions:
The translation of the Cornell Assessment of Pediatric Delirium into Brazilian Portuguese and its cross-cultural adaptation were successful and preserved the linguistic and semantic properties of the original instrument. The Cornell Assessment of Pediatric Delirium proved to be easy to understand and could be completed quickly. Additional studies are needed to test the validity and psychometric properties of this version in Brazil.
Views0Abstract
Original ArticlesTranslation and cross-cultural adaptation of the Cornell Assessment of Pediatric Delirium scale for the Portuguese language
Rev Bras Ter Intensiva. 2018;30(2):195-200
DOI 10.5935/0103-507X.20180033
Views0See moreABSTRACT
Objective:
This study sought to translate the Cornell Assessment of Pediatric Delirium from English into Brazilian Portuguese and cross-culturally adapt it for use in Brazil.
Methods:
Following the authorization granted by its main author, the processes of translation and cross-cultural adaptation were performed with regard to the Cornell Assessment of Pediatric Delirium in accordance with the following internationally recommended steps: translation of the original into Portuguese by two native speakers of the target language; synthesis of the translated versions; back-translation by two native speakers of the original language; review and harmonization of the back-translation; a review of the Portuguese version of the Cornell Assessment of Pediatric Delirium by an expert panel composed of specialists; pretesting including assessments of clarity, comprehensibility, and acceptability of the translated version using a sample of the target population; and finishing modifications to achieve the final version.
Results:
The translation and cross-cultural adaptation of the Cornell Assessment of Pediatric Delirium followed international recommendations. The linguistic and semantic issues that emerged during the process were discussed by the expert panel, which unanimously agreed to slight modifications. During pretesting, the Cornell Assessment of Pediatric Delirium was administered to 30 eligible children, twice per day; the final version was easy to understand, could be completed quickly, and showed a high inter-rater correlation coefficient (0.955).
Conclusions:
The translation of the Cornell Assessment of Pediatric Delirium into Brazilian Portuguese and its cross-cultural adaptation were successful and preserved the linguistic and semantic properties of the original instrument. The Cornell Assessment of Pediatric Delirium proved to be easy to understand and could be completed quickly. Additional studies are needed to test the validity and psychometric properties of this version in Brazil.
-
Original Articles
Organ donation: the reality of an intensive care unit in Portugal
Rev Bras Ter Intensiva. 2018;30(2):201-207
Abstract
Original ArticlesOrgan donation: the reality of an intensive care unit in Portugal
Rev Bras Ter Intensiva. 2018;30(2):201-207
DOI 10.5935/0103-507X.20180040
Views0See moreABSTRACT
Objective:
To clinically and demographically characterize potential organ donors admitted to a general intensive care unit and analyze data on donated organs.
Methods:
This retrospective study was conducted from 2010 to 2015 and analyzed demographic and clinical variables and the number of harvested organs and tissues.
Results:
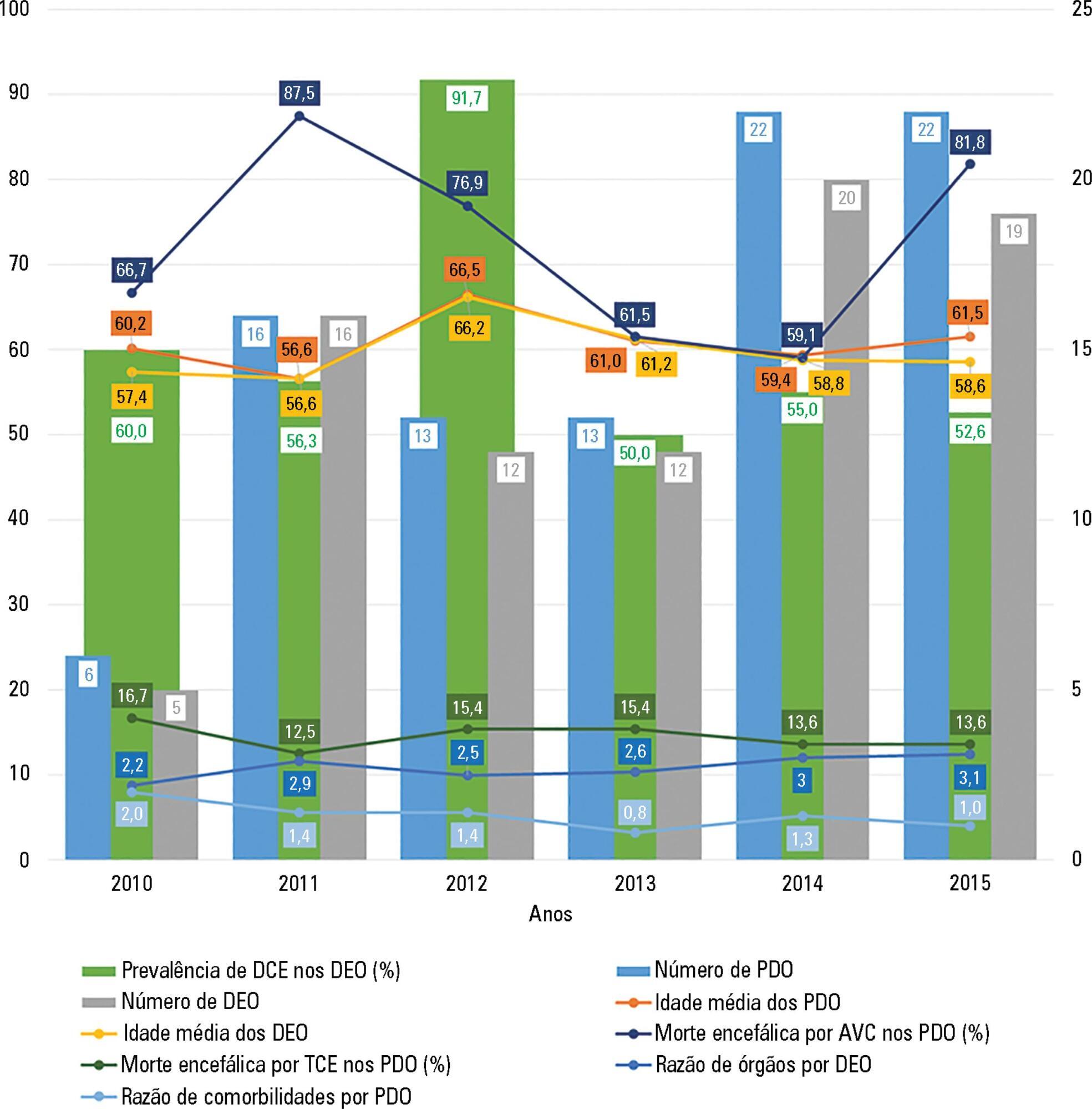
A total of 92 potential organ donors were identified, of whom eight were non-effective donors and 84 were effective donors (59.5% were expanded criteria donors). The mean age of the potential donors was 60.7 years, and the majority were men. Hemorrhagic stroke accounted for 55.4% of brain deaths. The most common blood type among the donors was A Rh+ (43.5%), and the most common comorbidity was arterial hypertension (43.3%). The most frequently collected organs were the kidneys (84.5%) and liver (66.7%). The average number of organs harvested per donor was 2.8, and this ratio was smaller for donors with expanded criteria compared to other donors.
Conclusion:
In most cases, potential organ donors died of brain death, were older than middle age, were male and were victims of a hemorrhagic stroke. The majority of the donors were expanded criteria donors and donated an average of two to three organs. The organs donated most frequently were the kidneys and liver.
Views0Abstract
Original ArticlesOrgan donation: the reality of an intensive care unit in Portugal
Rev Bras Ter Intensiva. 2018;30(2):201-207
DOI 10.5935/0103-507X.20180040
Views0See moreABSTRACT
Objective:
To clinically and demographically characterize potential organ donors admitted to a general intensive care unit and analyze data on donated organs.
Methods:
This retrospective study was conducted from 2010 to 2015 and analyzed demographic and clinical variables and the number of harvested organs and tissues.
Results:
A total of 92 potential organ donors were identified, of whom eight were non-effective donors and 84 were effective donors (59.5% were expanded criteria donors). The mean age of the potential donors was 60.7 years, and the majority were men. Hemorrhagic stroke accounted for 55.4% of brain deaths. The most common blood type among the donors was A Rh+ (43.5%), and the most common comorbidity was arterial hypertension (43.3%). The most frequently collected organs were the kidneys (84.5%) and liver (66.7%). The average number of organs harvested per donor was 2.8, and this ratio was smaller for donors with expanded criteria compared to other donors.
Conclusion:
In most cases, potential organ donors died of brain death, were older than middle age, were male and were victims of a hemorrhagic stroke. The majority of the donors were expanded criteria donors and donated an average of two to three organs. The organs donated most frequently were the kidneys and liver.
-
Review Articles
Chest wall effect on the monitoring of respiratory mechanics in acute respiratory distress syndrome
Rev Bras Ter Intensiva. 2018;30(2):208-218
Abstract
Review ArticlesChest wall effect on the monitoring of respiratory mechanics in acute respiratory distress syndrome
Rev Bras Ter Intensiva. 2018;30(2):208-218
DOI 10.5935/0103-507X.20180038
Views0ABSTRACT
The respiratory system mechanics depend on the characteristics of the lung and chest wall and their interaction. In patients with acute respiratory distress syndrome under mechanical ventilation, the monitoring of airway plateau pressure is fundamental given its prognostic value and its capacity to assess pulmonary stress. However, its validity can be affected by changes in mechanical characteristics of the chest wall, and it provides no data to correctly titrate positive end-expiratory pressure by restoring lung volume. The chest wall effect on respiratory mechanics in acute respiratory distress syndrome has not been completely described, and it has likely been overestimated, which may lead to erroneous decision making. The load imposed by the chest wall is negligible when the respiratory system is insufflated with positive end-expiratory pressure. Under dynamic conditions, moving this structure demands a pressure change whose magnitude is related to its mechanical characteristics, and this load remains constant regardless of the volume from which it is insufflated. Thus, changes in airway pressure reflect changes in the lung mechanical conditions. Advanced monitoring could be reserved for patients with increased intra-abdominal pressure in whom a protective mechanical ventilation strategy cannot be implemented. The estimates of alveolar recruitment based on respiratory system mechanics could reflect differences in chest wall response to insufflation and not actual alveolar recruitment.
Keywords:Respiration, artificialRespiratory distress syndrome, adultRespiratory mechanicsThoracic wallVentilator-induced lung injurySee moreViews0Abstract
Review ArticlesChest wall effect on the monitoring of respiratory mechanics in acute respiratory distress syndrome
Rev Bras Ter Intensiva. 2018;30(2):208-218
DOI 10.5935/0103-507X.20180038
Views0ABSTRACT
The respiratory system mechanics depend on the characteristics of the lung and chest wall and their interaction. In patients with acute respiratory distress syndrome under mechanical ventilation, the monitoring of airway plateau pressure is fundamental given its prognostic value and its capacity to assess pulmonary stress. However, its validity can be affected by changes in mechanical characteristics of the chest wall, and it provides no data to correctly titrate positive end-expiratory pressure by restoring lung volume. The chest wall effect on respiratory mechanics in acute respiratory distress syndrome has not been completely described, and it has likely been overestimated, which may lead to erroneous decision making. The load imposed by the chest wall is negligible when the respiratory system is insufflated with positive end-expiratory pressure. Under dynamic conditions, moving this structure demands a pressure change whose magnitude is related to its mechanical characteristics, and this load remains constant regardless of the volume from which it is insufflated. Thus, changes in airway pressure reflect changes in the lung mechanical conditions. Advanced monitoring could be reserved for patients with increased intra-abdominal pressure in whom a protective mechanical ventilation strategy cannot be implemented. The estimates of alveolar recruitment based on respiratory system mechanics could reflect differences in chest wall response to insufflation and not actual alveolar recruitment.
Keywords:Respiration, artificialRespiratory distress syndrome, adultRespiratory mechanicsThoracic wallVentilator-induced lung injurySee more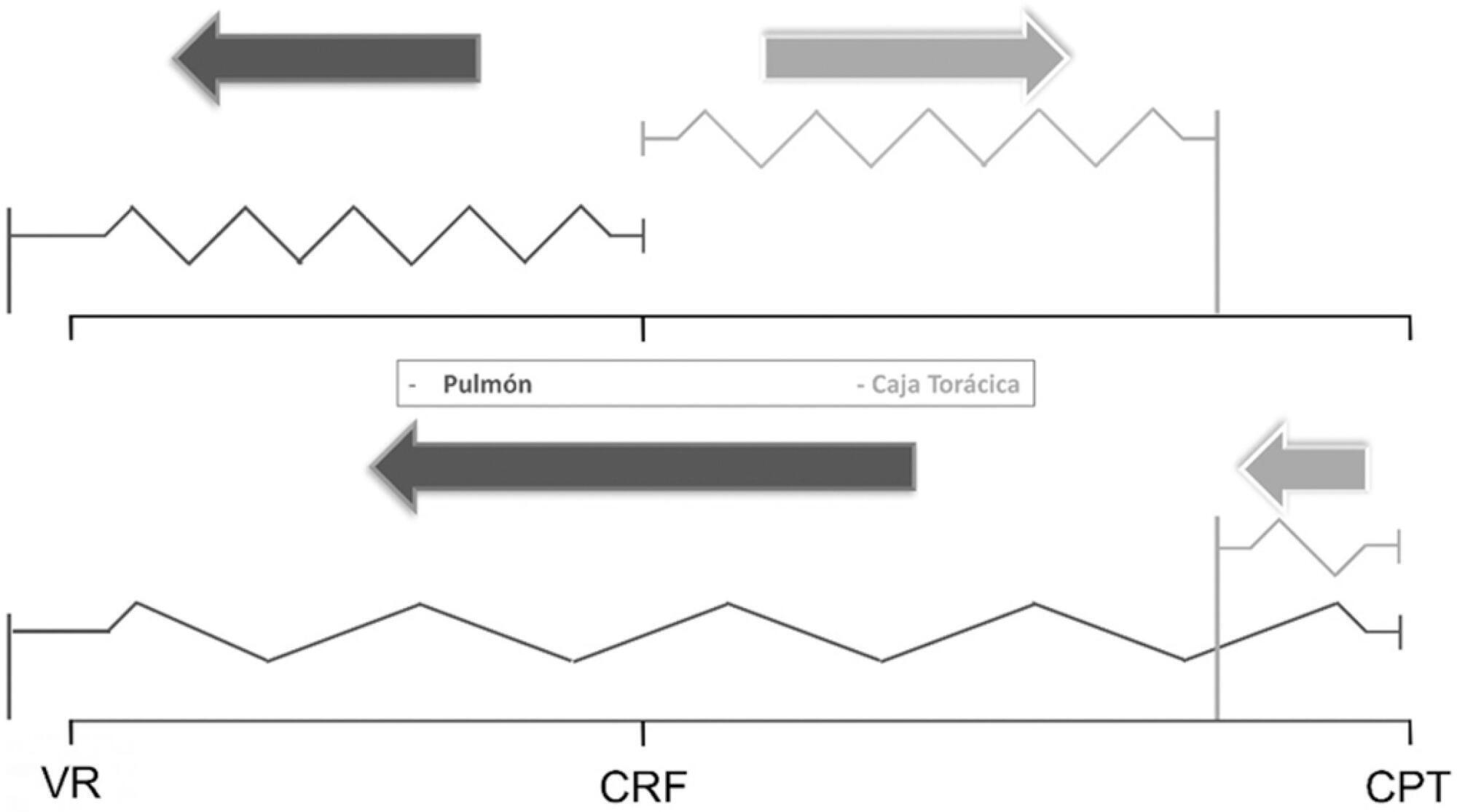
-
Review Articles
Safety of neuromuscular electrical stimulation among critically ill patients: systematic review
Rev Bras Ter Intensiva. 2018;30(2):219-225
Abstract
Review ArticlesSafety of neuromuscular electrical stimulation among critically ill patients: systematic review
Rev Bras Ter Intensiva. 2018;30(2):219-225
DOI 10.5935/0103-507X.20180036
Views0ABSTRACT
Objective:
To review the evidence on the safety of neuromuscular electrical stimulation when used in the intensive care unit.
Methods:
A systematic review was conducted; a literature search was performed of the MEDLINE (via PubMed), PEDro, Cochrane CENTRAL and EMBASE databases, and a further manual search was performed among the references cited in randomized studies. Randomized clinical trials that compared neuromuscular electrical stimulation to a control or placebo group in the intensive care unit and reporting on the technique safety in the outcomes were included. Hemodynamic variables and information on adverse effects were considered safety parameters. Articles were independently analyzed by two reviewers, and the data analysis was descriptive.
Results:
The initial search located 1,533 articles, from which only four randomized clinical trials were included. Two studies assessed safety based on hemodynamic variables, and only one study reported an increase in heart rate, respiratory rate and blood lactate, without clinical relevance. The other two studies assessed safety based on reported adverse effects. In one, 15% of patients described a prickling sensation, without any clinically relevant abnormalities. In the other, one patient suffered a superficial burn due to improper parameter configuration.
Conclusion:
Neuromuscular electrical stimulation is safe for critically ill patients; however, it should be applied by duly trained professionals and with proper evidence-based parameters.
Keywords:Drug-related side effects and adverse reactionsElectric stimulation therapyIntensive care unitsPhysical stimulationRespiration, artificialSafetySee moreViews0Abstract
Review ArticlesSafety of neuromuscular electrical stimulation among critically ill patients: systematic review
Rev Bras Ter Intensiva. 2018;30(2):219-225
DOI 10.5935/0103-507X.20180036
Views0ABSTRACT
Objective:
To review the evidence on the safety of neuromuscular electrical stimulation when used in the intensive care unit.
Methods:
A systematic review was conducted; a literature search was performed of the MEDLINE (via PubMed), PEDro, Cochrane CENTRAL and EMBASE databases, and a further manual search was performed among the references cited in randomized studies. Randomized clinical trials that compared neuromuscular electrical stimulation to a control or placebo group in the intensive care unit and reporting on the technique safety in the outcomes were included. Hemodynamic variables and information on adverse effects were considered safety parameters. Articles were independently analyzed by two reviewers, and the data analysis was descriptive.
Results:
The initial search located 1,533 articles, from which only four randomized clinical trials were included. Two studies assessed safety based on hemodynamic variables, and only one study reported an increase in heart rate, respiratory rate and blood lactate, without clinical relevance. The other two studies assessed safety based on reported adverse effects. In one, 15% of patients described a prickling sensation, without any clinically relevant abnormalities. In the other, one patient suffered a superficial burn due to improper parameter configuration.
Conclusion:
Neuromuscular electrical stimulation is safe for critically ill patients; however, it should be applied by duly trained professionals and with proper evidence-based parameters.
Keywords:Drug-related side effects and adverse reactionsElectric stimulation therapyIntensive care unitsPhysical stimulationRespiration, artificialSafetySee more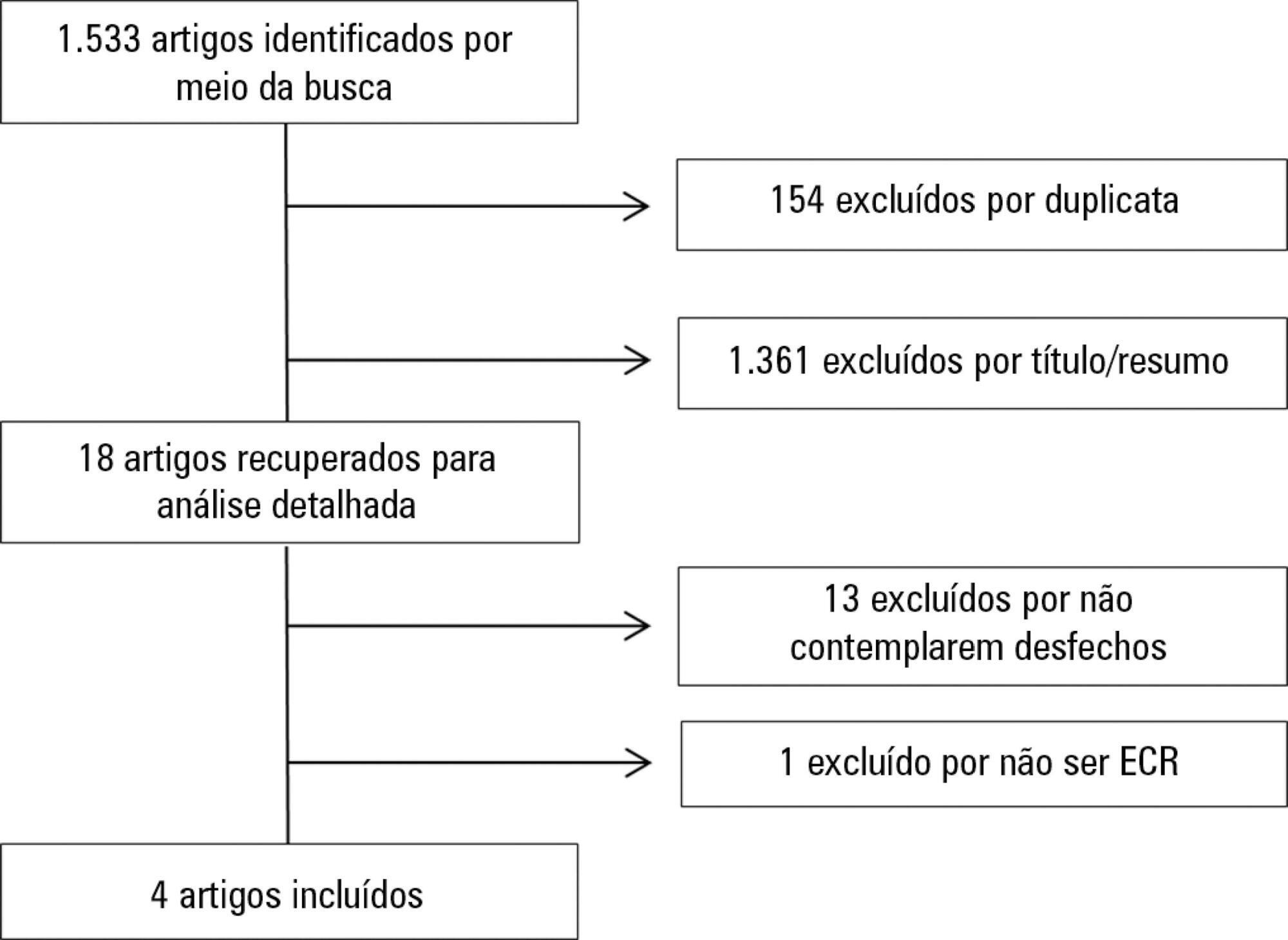
-
Review Articles
Difficult decisions in pediatric practice and moral distress in the intensive care unit
Rev Bras Ter Intensiva. 2018;30(2):226-232
Abstract
Review ArticlesDifficult decisions in pediatric practice and moral distress in the intensive care unit
Rev Bras Ter Intensiva. 2018;30(2):226-232
DOI 10.5935/0103-507X.20180039
Views0ABSTRACT
In an ethical dilemma, there is always an option that can be identified as the best one to be chosen. When it is impossible to adopt such option, the situation can lead professionals to experience moral distress. This review aims to define the issue of moral distress and propose coping strategies. Systematic searches in the MEDLINE/PubMed and SciELO databases were conducted using the keywords “moral distress” and “moral suffering” in articles published between 2000 and 2017. This review was non-exhaustive and contextual, with a focus on definitions, etiologies and methods of resolution for moral distress. In the daily practice of intensive care, moral distress was commonly related to the prolongation of patients’ suffering and feelings of helplessness, as well as difficulties in communication among team members. Coping strategies for moral distress included organizational, personal and administrative actions. Actions such as workload management, mutual support among professionals and the development of techniques to cultivate open communication, reflection and questioning within the multidisciplinary team were identified. In clinical practice, health professionals need to be recognized as moral agents, and the development of moral courage was considered helpful to overcome ethical dilemmas and interprofessional conflicts. Both in pediatric and adult intensive care, professionals are challenged by questions about their practice, and they may experience moral distress. This suffering can be minimized and solved by understanding that the focus is always on the patient and acting with moral courage and good communication in an environment of mutual respect.
Keywords:Attitudes of health personnelChildConflict (psychology)Decision making/ethicsEthics, clinicalInfantIntensive care units, pediatric/ethicsMoralsStress, psychologicalSee moreViews0Abstract
Review ArticlesDifficult decisions in pediatric practice and moral distress in the intensive care unit
Rev Bras Ter Intensiva. 2018;30(2):226-232
DOI 10.5935/0103-507X.20180039
Views0ABSTRACT
In an ethical dilemma, there is always an option that can be identified as the best one to be chosen. When it is impossible to adopt such option, the situation can lead professionals to experience moral distress. This review aims to define the issue of moral distress and propose coping strategies. Systematic searches in the MEDLINE/PubMed and SciELO databases were conducted using the keywords “moral distress” and “moral suffering” in articles published between 2000 and 2017. This review was non-exhaustive and contextual, with a focus on definitions, etiologies and methods of resolution for moral distress. In the daily practice of intensive care, moral distress was commonly related to the prolongation of patients’ suffering and feelings of helplessness, as well as difficulties in communication among team members. Coping strategies for moral distress included organizational, personal and administrative actions. Actions such as workload management, mutual support among professionals and the development of techniques to cultivate open communication, reflection and questioning within the multidisciplinary team were identified. In clinical practice, health professionals need to be recognized as moral agents, and the development of moral courage was considered helpful to overcome ethical dilemmas and interprofessional conflicts. Both in pediatric and adult intensive care, professionals are challenged by questions about their practice, and they may experience moral distress. This suffering can be minimized and solved by understanding that the focus is always on the patient and acting with moral courage and good communication in an environment of mutual respect.
Keywords:Attitudes of health personnelChildConflict (psychology)Decision making/ethicsEthics, clinicalInfantIntensive care units, pediatric/ethicsMoralsStress, psychologicalSee more -
Case Reports
Use of extracorporeal membrane oxygenation for treating acute cardiomyopathy after liver transplantation: a case report
Rev Bras Ter Intensiva. 2018;30(2):233-236
Abstract
Case ReportsUse of extracorporeal membrane oxygenation for treating acute cardiomyopathy after liver transplantation: a case report
Rev Bras Ter Intensiva. 2018;30(2):233-236
DOI 10.5935/0103-507X.20180029
Views0ABSTRACT
We report the case of a female patient, 58 years of age, without known heart disease, who underwent liver transplantation without complications. On the second postoperative day, the patient developed cardiogenic shock secondary to stress-induced cardiomyopathy (Takotsubo-like syndrome). The patient was successfully managed with veno-arterial peripheral extracorporeal membrane oxygenation for 6 days, with complete recovery of cardiac function and of the hepatic graft. Coronary syndrome and acute myocarditis were excluded as the causes of the shock. The use of extracorporeal membrane oxygenation in this scenario is possible and safe, considering its specialized protocols and treatment.
Keywords:CardiomyopathiesCase reportsCoagulation agentsExtracorporeal membrane oxygenationLiver transplantationShock, cardiogenicSee moreViews0Abstract
Case ReportsUse of extracorporeal membrane oxygenation for treating acute cardiomyopathy after liver transplantation: a case report
Rev Bras Ter Intensiva. 2018;30(2):233-236
DOI 10.5935/0103-507X.20180029
Views0ABSTRACT
We report the case of a female patient, 58 years of age, without known heart disease, who underwent liver transplantation without complications. On the second postoperative day, the patient developed cardiogenic shock secondary to stress-induced cardiomyopathy (Takotsubo-like syndrome). The patient was successfully managed with veno-arterial peripheral extracorporeal membrane oxygenation for 6 days, with complete recovery of cardiac function and of the hepatic graft. Coronary syndrome and acute myocarditis were excluded as the causes of the shock. The use of extracorporeal membrane oxygenation in this scenario is possible and safe, considering its specialized protocols and treatment.
Keywords:CardiomyopathiesCase reportsCoagulation agentsExtracorporeal membrane oxygenationLiver transplantationShock, cardiogenicSee more -
Case Reports
Paroxysmal sympathetic hyperactivity syndrome caused by fat embolism syndrome
Rev Bras Ter Intensiva. 2018;30(2):237-243
Abstract
Case ReportsParoxysmal sympathetic hyperactivity syndrome caused by fat embolism syndrome
Rev Bras Ter Intensiva. 2018;30(2):237-243
DOI 10.5935/0103-507X.20180035
Views0See moreABSTRACT
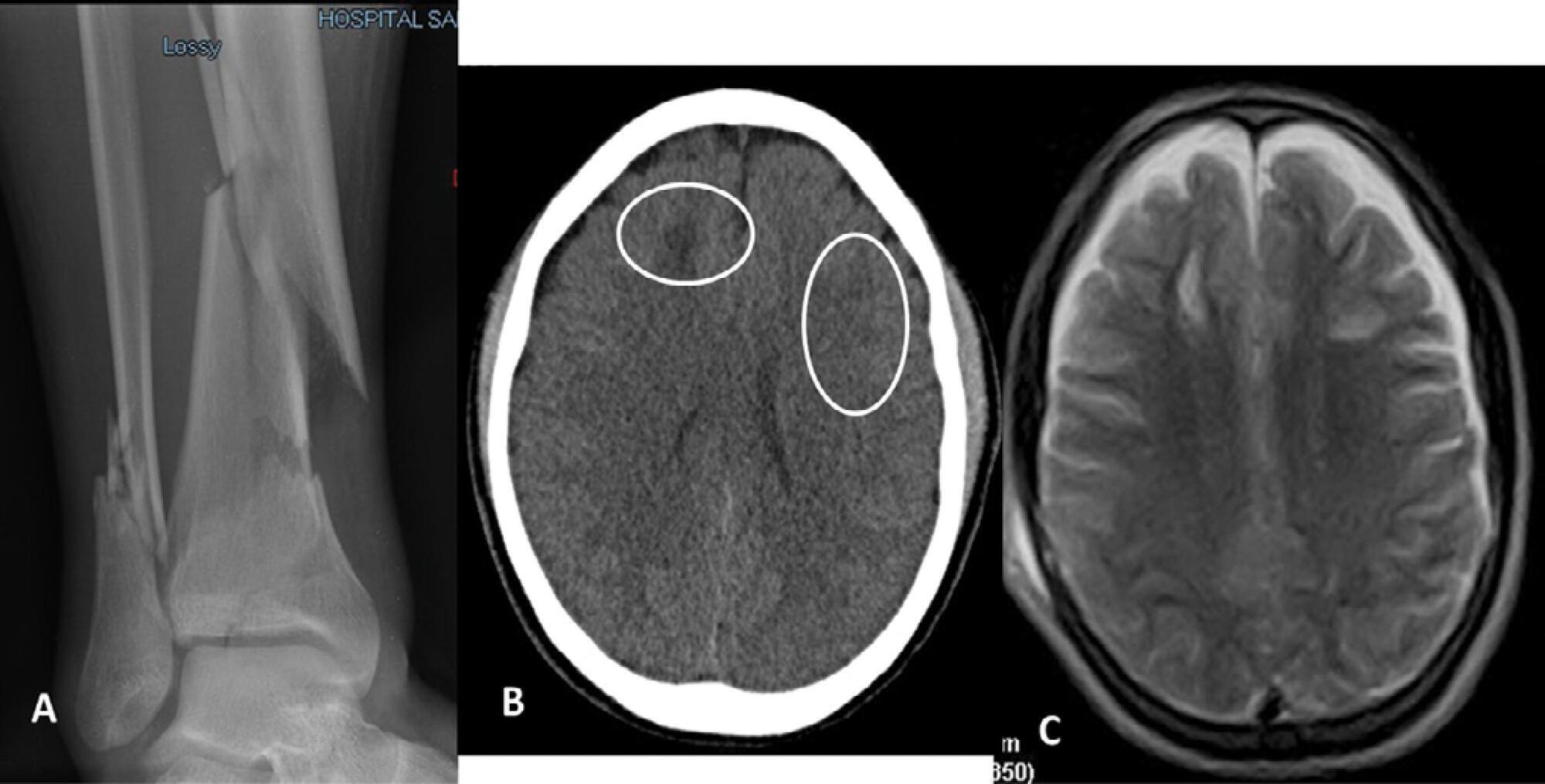
Paroxysmal sympathetic hyperactivity represents an uncommon and potentially life-threatening complication of severe brain injuries, which are most commonly traumatic. This syndrome is a clinical diagnosis based on the recurrent occurrence of tachycardia, hypertension, diaphoresis, tachypnea, and occasionally high fever and dystonic postures. The episodes may be induced by stimulation or may occur spontaneously. Underdiagnosis is common, and delayed recognition may increase morbidity and long-term disability. Trigger avoidance and pharmacological therapy can be very successful in controlling this complication. Fat embolism syndrome is a rare but serious complication of long bone fractures. Neurologic signs, petechial hemorrhages and acute respiratory failure constitute the characteristic presenting triad. The term cerebral fat embolism is used when the neurological involvement predominates. The diagnosis is clinical, but specific neuroimaging findings can be supportive. The neurologic manifestations include different degrees of alteration of consciousness, focal deficits or seizures. Management is supportive, but good outcomes are possible even in cases with very severe presentation. We report two cases of paroxysmal sympathetic hyperactivity after cerebral fat embolism, which is a very uncommon association.
Views0Abstract
Case ReportsParoxysmal sympathetic hyperactivity syndrome caused by fat embolism syndrome
Rev Bras Ter Intensiva. 2018;30(2):237-243
DOI 10.5935/0103-507X.20180035
Views0See moreABSTRACT
Paroxysmal sympathetic hyperactivity represents an uncommon and potentially life-threatening complication of severe brain injuries, which are most commonly traumatic. This syndrome is a clinical diagnosis based on the recurrent occurrence of tachycardia, hypertension, diaphoresis, tachypnea, and occasionally high fever and dystonic postures. The episodes may be induced by stimulation or may occur spontaneously. Underdiagnosis is common, and delayed recognition may increase morbidity and long-term disability. Trigger avoidance and pharmacological therapy can be very successful in controlling this complication. Fat embolism syndrome is a rare but serious complication of long bone fractures. Neurologic signs, petechial hemorrhages and acute respiratory failure constitute the characteristic presenting triad. The term cerebral fat embolism is used when the neurological involvement predominates. The diagnosis is clinical, but specific neuroimaging findings can be supportive. The neurologic manifestations include different degrees of alteration of consciousness, focal deficits or seizures. Management is supportive, but good outcomes are possible even in cases with very severe presentation. We report two cases of paroxysmal sympathetic hyperactivity after cerebral fat embolism, which is a very uncommon association.
-
Letters to the Editor
Periodontal disease and bronchoaspiration in a neurovegetative patient
Rev Bras Ter Intensiva. 2018;30(2):244-245
Abstract
Letters to the EditorPeriodontal disease and bronchoaspiration in a neurovegetative patient
Rev Bras Ter Intensiva. 2018;30(2):244-245
DOI 10.5935/0103-507X.20180024
Views0To the Editor, Teamwork within the hospital setting is fundamental to increase the quality of life of the patient. In this sense, the introduction of hospital dentistry contributes to multidisciplinary and comprehensive health.()[…]See moreViews0Abstract
Letters to the EditorPeriodontal disease and bronchoaspiration in a neurovegetative patient
Rev Bras Ter Intensiva. 2018;30(2):244-245
DOI 10.5935/0103-507X.20180024
Views0To the Editor, Teamwork within the hospital setting is fundamental to increase the quality of life of the patient. In this sense, the introduction of hospital dentistry contributes to multidisciplinary and comprehensive health.()[…]See more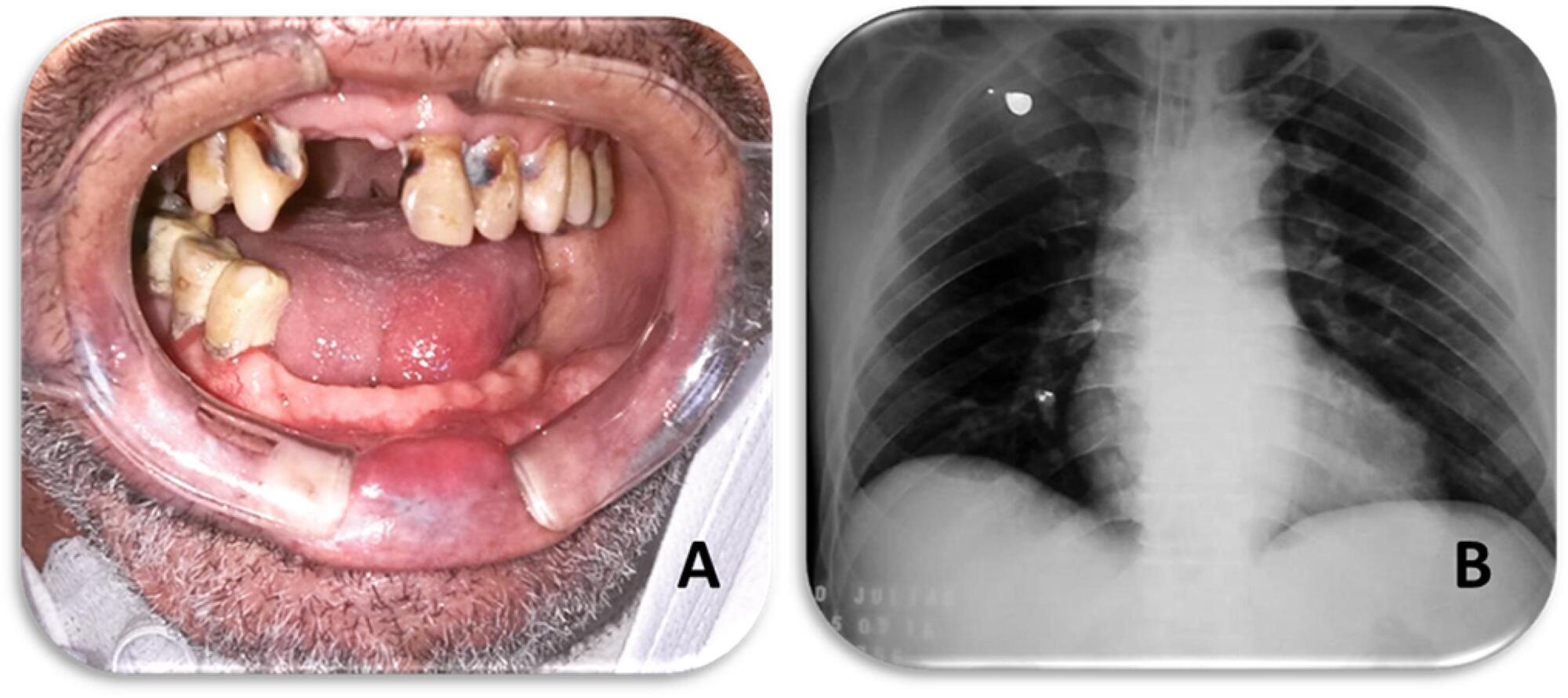
-
Letters to the Editor
Analgosedation and delirium in intensive care units in Brazil: current status. ASDUTI study
Rev Bras Ter Intensiva. 2018;30(2):246-248
Abstract
Letters to the EditorAnalgosedation and delirium in intensive care units in Brazil: current status. ASDUTI study
Rev Bras Ter Intensiva. 2018;30(2):246-248
DOI 10.5935/0103-507X.20180025
Views0To the Editor, The adequate management of analgosedation and delirium is related to better outcomes in intensive care units.(–) The objective of this study is to evaluate the current status of the management of analgosedation and delirium in Brazil.[…]See moreViews0Abstract
Letters to the EditorAnalgosedation and delirium in intensive care units in Brazil: current status. ASDUTI study
Rev Bras Ter Intensiva. 2018;30(2):246-248
DOI 10.5935/0103-507X.20180025
Views0To the Editor, The adequate management of analgosedation and delirium is related to better outcomes in intensive care units.(–) The objective of this study is to evaluate the current status of the management of analgosedation and delirium in Brazil.[…]See more -
Letters to the Editor
Infective endocarditis of the tricuspid valve
Rev Bras Ter Intensiva. 2018;30(2):249-250
Abstract
Letters to the EditorInfective endocarditis of the tricuspid valve
Rev Bras Ter Intensiva. 2018;30(2):249-250
DOI 10.5935/0103-507X.20180026
Views0To the Editor Infectious endocarditis of the tricuspid valve is rare(,) and is usually associated with the use of injectable drugs and the manipulation of intravenous devices.(–)[…]See moreViews0Abstract
Letters to the EditorInfective endocarditis of the tricuspid valve
Rev Bras Ter Intensiva. 2018;30(2):249-250
DOI 10.5935/0103-507X.20180026
Views0To the Editor Infectious endocarditis of the tricuspid valve is rare(,) and is usually associated with the use of injectable drugs and the manipulation of intravenous devices.(–)[…]See more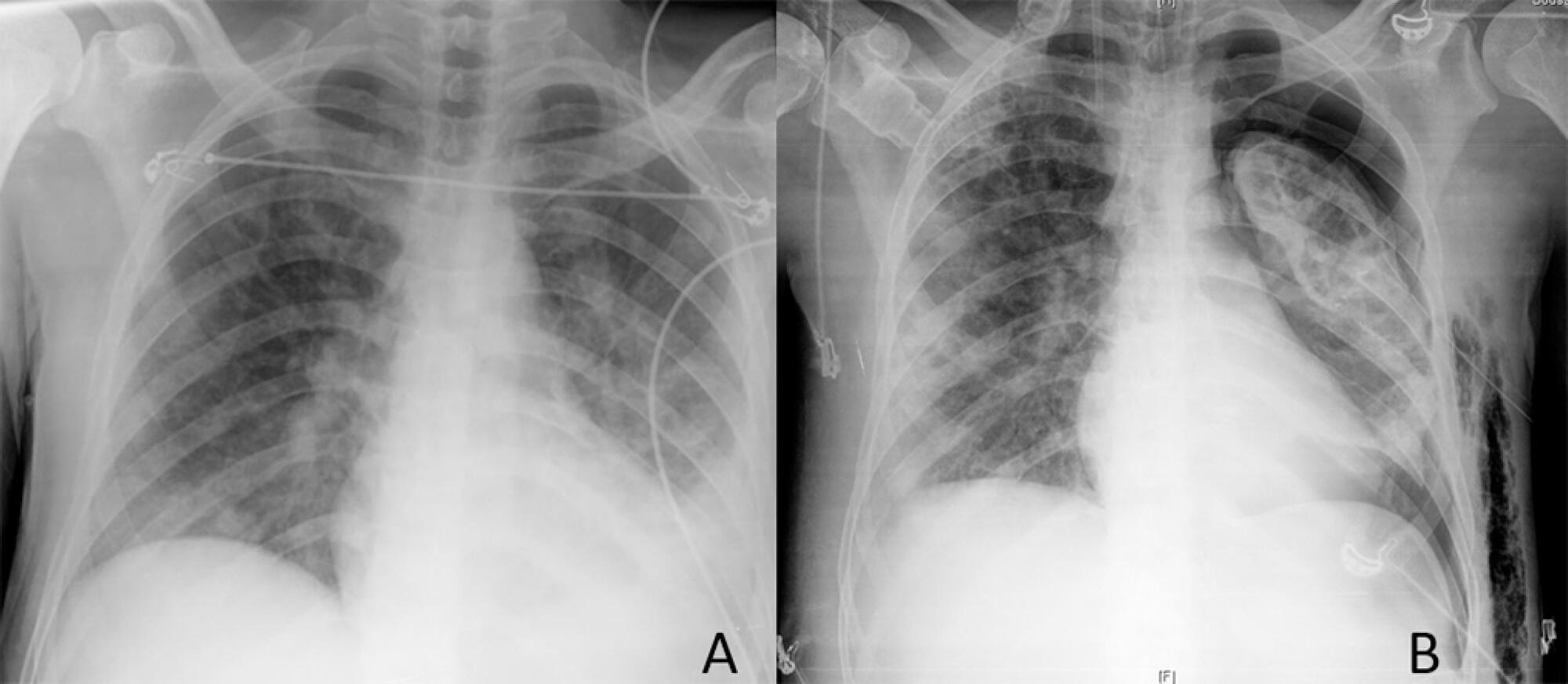
-
Letters to the Editor
To: The Epimed Monitor ICU Database®: a cloud-based national registry for adult intensive care unit patients in Brazil
Rev Bras Ter Intensiva. 2018;30(2):251-252
Abstract
Letters to the EditorTo: The Epimed Monitor ICU Database®: a cloud-based national registry for adult intensive care unit patients in Brazil
Rev Bras Ter Intensiva. 2018;30(2):251-252
DOI 10.5935/0103-507X.20180031
Views1To the Editor We congratulate the Epimed collaborators() on their impressive results from a privately owned registry in Brazil, an upper-middle income country. In addition to the examples from high income countries cited by the authors, Sri Lanka – a lower-middle-income country in South Asia – has implemented a national cloud-based intensive care unit (ICU) […]See moreViews1Abstract
Letters to the EditorTo: The Epimed Monitor ICU Database®: a cloud-based national registry for adult intensive care unit patients in Brazil
Rev Bras Ter Intensiva. 2018;30(2):251-252
DOI 10.5935/0103-507X.20180031
Views1To the Editor We congratulate the Epimed collaborators() on their impressive results from a privately owned registry in Brazil, an upper-middle income country. In addition to the examples from high income countries cited by the authors, Sri Lanka – a lower-middle-income country in South Asia – has implemented a national cloud-based intensive care unit (ICU) […]See more
Volume Articles - Critical Care Science (CCS)
