-
Commentaries
From the International Pediatric Sepsis Conference 2005 to the Sepsis-3 Consensus
Rev Bras Ter Intensiva. 2018;30(1):1-5
Abstract
CommentariesFrom the International Pediatric Sepsis Conference 2005 to the Sepsis-3 Consensus
Rev Bras Ter Intensiva. 2018;30(1):1-5
DOI 10.5935/0103-507X.20180005
Views1INTRODUCTION In the last decades, sepsis, due to an immune response, has been defined as a potentially fatal organ dysfunction resulting from a dysregulated organism response to an infectious insult, in which pro- and anti-inflammatory responses can coexist in the early phase of the disease and which, together with non-immunological mechanisms, decisively influence prognosis and […]See moreViews1

Abstract
CommentariesFrom the International Pediatric Sepsis Conference 2005 to the Sepsis-3 Consensus
Rev Bras Ter Intensiva. 2018;30(1):1-5
DOI 10.5935/0103-507X.20180005
Views1INTRODUCTIONIn the last decades, sepsis, due to an immune response, has been defined as a potentially fatal organ dysfunction resulting from a dysregulated organism response to an infectious insult, in which pro- and anti-inflammatory responses can coexist in the early phase of the disease and which, together with non-immunological mechanisms, decisively influence prognosis and evolution.(–) […]See more -
Commentaries
First Brazilian datathon in critical care
Rev Bras Ter Intensiva. 2018;30(1):6-8
Abstract
CommentariesFirst Brazilian datathon in critical care
Rev Bras Ter Intensiva. 2018;30(1):6-8
DOI 10.5935/0103-507X.20180006
Views1“Health is a right of all and an obligation of the State, guaranteed by socioeconomic policies that seek reduction of the risk of disease and of other grievances and universal and equal access to the actions and services in its promotion, protection and recuperation.” Constitution of the Federative Republic of Brazil, 1988[…]See moreViews1Abstract
CommentariesFirst Brazilian datathon in critical care
Rev Bras Ter Intensiva. 2018;30(1):6-8
DOI 10.5935/0103-507X.20180006
Views1“Health is a right of all and an obligation of the State, guaranteed by socioeconomic policies that seek reduction of the risk of disease and of other grievances and universal and equal access to the actions and services in its promotion, protection and recuperation.” Constitution of the Federative Republic of Brazil, 1988[…]See more -
Commentaries
What every intensivist should know about the management of peritonitis in the intensive care unit
Rev Bras Ter Intensiva. 2018;30(1):9-14
Abstract
CommentariesWhat every intensivist should know about the management of peritonitis in the intensive care unit
Rev Bras Ter Intensiva. 2018;30(1):9-14
DOI 10.5935/0103-507X.20180007
Views1IntroductionComplicated intra-abdominal infections (cIAI) are among the more challenging infections in the intensive care unit, not only because they are typically associated with more severe organ dysfunction() but also because the need for an intervention is more important than in other infections.() In recent years, a number of new challenges have been added, further complicating […]See moreViews1Abstract
CommentariesWhat every intensivist should know about the management of peritonitis in the intensive care unit
Rev Bras Ter Intensiva. 2018;30(1):9-14
DOI 10.5935/0103-507X.20180007
Views1IntroductionComplicated intra-abdominal infections (cIAI) are among the more challenging infections in the intensive care unit, not only because they are typically associated with more severe organ dysfunction() but also because the need for an intervention is more important than in other infections.() In recent years, a number of new challenges have been added, further complicating […]See more -
Original Article
Acute kidney injury and intra-abdominal hypertension in burn patients in intensive care
Rev Bras Ter Intensiva. 2018;30(1):15-20
Abstract
Original ArticleAcute kidney injury and intra-abdominal hypertension in burn patients in intensive care
Rev Bras Ter Intensiva. 2018;30(1):15-20
DOI 10.5935/0103-507X.20180001
Views0ABSTRACT
Objective:
To evaluate the frequency of intra-abdominal hypertension in major burn patients and its association with the occurrence of acute kidney injury.
Methods:
This was a prospective cohort study of a population of burn patients hospitalized in a specialized intensive care unit. A convenience sample was taken of adult patients hospitalized in the period from 1 August 2015 to 31 October 2016. Clinical and burn data were collected, and serial intra-abdominal pressure measurements taken. The significance level used was 5%.
Results:
A total of 46 patients were analyzed. Of these, 38 patients developed intra-abdominal hypertension (82.6%). The median increase in intra-abdominal pressure was 15.0mmHg (interquartile range: 12.0 to 19.0). Thirty-two patients (69.9%) developed acute kidney injury. The median time to development of acute kidney injury was 3 days (interquartile range: 1 – 7). The individual analysis of risk factors for acute kidney injury indicated an association with intra-abdominal hypertension (p = 0.041), use of glycopeptides (p = 0.001), use of vasopressors (p = 0.001) and use of mechanical ventilation (p = 0.006). Acute kidney injury was demonstrated to have an association with increased 30-day mortality (log-rank, p = 0.009).
Conclusion:
Intra-abdominal hypertension occurred in most patients, predominantly in grades I and II. The identified risk factors for the occurrence of acute kidney injury were intra-abdominal hypertension and use of glycopeptides, vasopressors and mechanical ventilation. Acute kidney injury was associated with increased 30-day mortality.
Keywords:Burn unitsburnsIntensive care unitsIntra-abdominal hypertensionMultiple organ failureRenal insufficiencySee moreViews0Abstract
Original ArticleAcute kidney injury and intra-abdominal hypertension in burn patients in intensive care
Rev Bras Ter Intensiva. 2018;30(1):15-20
DOI 10.5935/0103-507X.20180001
Views0ABSTRACT
Objective:
To evaluate the frequency of intra-abdominal hypertension in major burn patients and its association with the occurrence of acute kidney injury.
Methods:
This was a prospective cohort study of a population of burn patients hospitalized in a specialized intensive care unit. A convenience sample was taken of adult patients hospitalized in the period from 1 August 2015 to 31 October 2016. Clinical and burn data were collected, and serial intra-abdominal pressure measurements taken. The significance level used was 5%.
Results:
A total of 46 patients were analyzed. Of these, 38 patients developed intra-abdominal hypertension (82.6%). The median increase in intra-abdominal pressure was 15.0mmHg (interquartile range: 12.0 to 19.0). Thirty-two patients (69.9%) developed acute kidney injury. The median time to development of acute kidney injury was 3 days (interquartile range: 1 – 7). The individual analysis of risk factors for acute kidney injury indicated an association with intra-abdominal hypertension (p = 0.041), use of glycopeptides (p = 0.001), use of vasopressors (p = 0.001) and use of mechanical ventilation (p = 0.006). Acute kidney injury was demonstrated to have an association with increased 30-day mortality (log-rank, p = 0.009).
Conclusion:
Intra-abdominal hypertension occurred in most patients, predominantly in grades I and II. The identified risk factors for the occurrence of acute kidney injury were intra-abdominal hypertension and use of glycopeptides, vasopressors and mechanical ventilation. Acute kidney injury was associated with increased 30-day mortality.
Keywords:Burn unitsburnsIntensive care unitsIntra-abdominal hypertensionMultiple organ failureRenal insufficiencySee more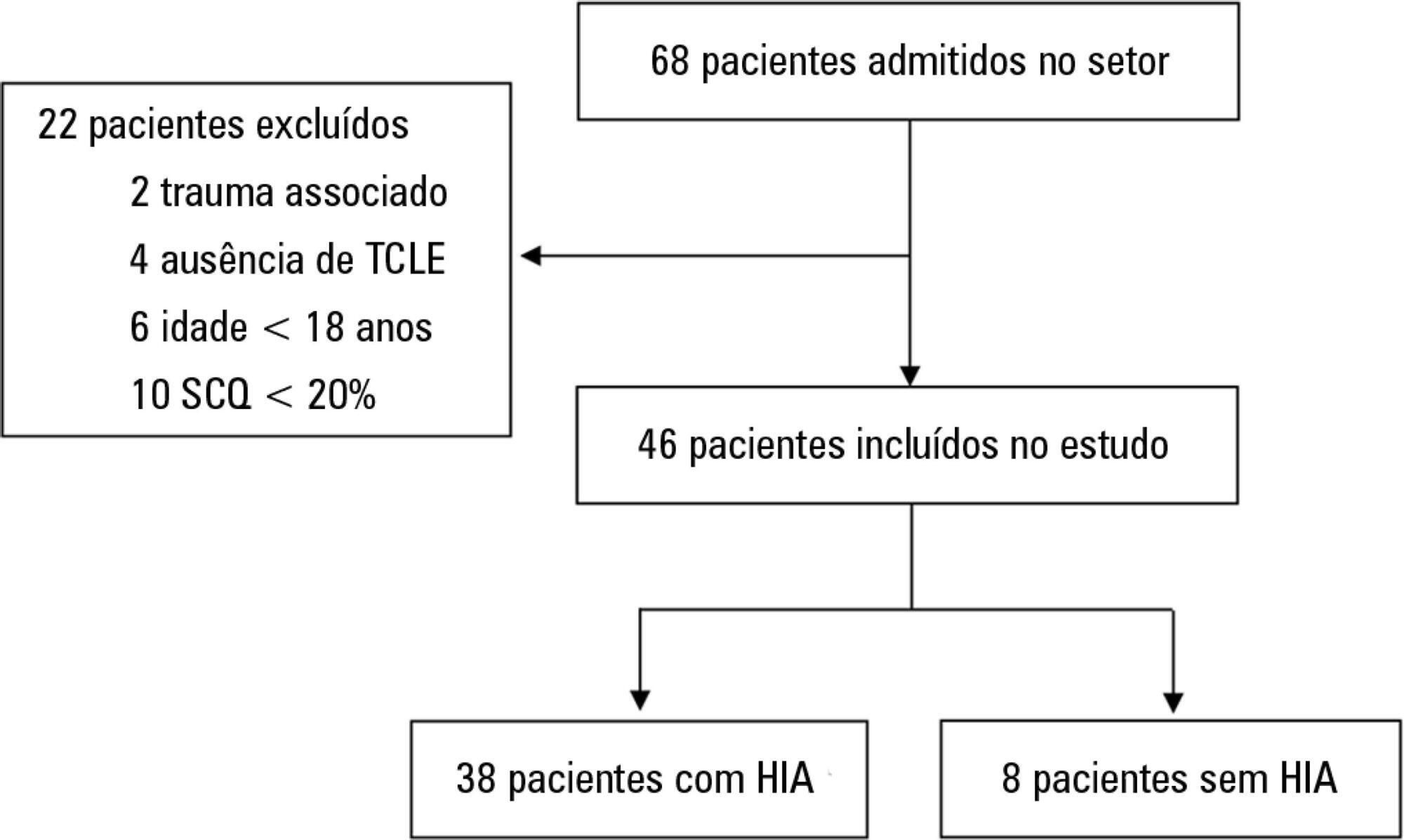
-
Original Article
Hemoglobin metabolism by-products are associated with an inflammatory response in patients with hemorrhagic stroke
Rev Bras Ter Intensiva. 2018;30(1):21-27
Abstract
Original ArticleHemoglobin metabolism by-products are associated with an inflammatory response in patients with hemorrhagic stroke
Rev Bras Ter Intensiva. 2018;30(1):21-27
DOI 10.5935/0103-507X.20180003
Views0ABSTRACT
Objective:
To evaluate the relationships of brain iron and heme with the inflammatory response of the systemic and central nervous systems and to investigate the role of defensive systems against the toxicity of iron and heme in the central nervous system.
Methods:
We assessed a prospective cohort of patients presenting with intracerebral and subarachnoid hemorrhage. We assayed plasma and cerebrospinal fluid samples for the presence of iron, heme, hemopexin, haptoglobin, enolase, S100-β and cytokines for the first three days following hemorrhagic stroke. We also analyzed the dynamic changes in these components within both fluids and their relationship with early mortality rates.
Results:
Hemopexin and haptoglobin concentrations were nearly negligible in the brain after intracerebral and subarachnoid hemorrhage. Cerebrospinal fluid iron and heme concentrations correlated with a pro-inflammatory response in the central nervous system, and plasmatic and cerebrospinal fluid inflammatory profiles on the third day after hemorrhagic stroke were related to early mortality rates. Interleukin 4 levels within the cerebrospinal fluid during the first 24 hours after hemorrhagic stroke were found to be higher in survivors than in non-survivors.
Conclusion:
Iron and heme are associated with a pro-inflammatory response in the central nervous system following hemorrhagic stroke, and protections against hemoglobin and heme are lacking within the human brain. Patient inflammatory profiles were associated with a poorer prognosis, and local anti-inflammatory responses appeared to have a protective role.
Keywords:Central nervous systemCytokinesHaptoglobinHemeHemopexinInflammatory responseIronSubarachnoid hemorrhageSee moreViews0Abstract
Original ArticleHemoglobin metabolism by-products are associated with an inflammatory response in patients with hemorrhagic stroke
Rev Bras Ter Intensiva. 2018;30(1):21-27
DOI 10.5935/0103-507X.20180003
Views0ABSTRACT
Objective:
To evaluate the relationships of brain iron and heme with the inflammatory response of the systemic and central nervous systems and to investigate the role of defensive systems against the toxicity of iron and heme in the central nervous system.
Methods:
We assessed a prospective cohort of patients presenting with intracerebral and subarachnoid hemorrhage. We assayed plasma and cerebrospinal fluid samples for the presence of iron, heme, hemopexin, haptoglobin, enolase, S100-β and cytokines for the first three days following hemorrhagic stroke. We also analyzed the dynamic changes in these components within both fluids and their relationship with early mortality rates.
Results:
Hemopexin and haptoglobin concentrations were nearly negligible in the brain after intracerebral and subarachnoid hemorrhage. Cerebrospinal fluid iron and heme concentrations correlated with a pro-inflammatory response in the central nervous system, and plasmatic and cerebrospinal fluid inflammatory profiles on the third day after hemorrhagic stroke were related to early mortality rates. Interleukin 4 levels within the cerebrospinal fluid during the first 24 hours after hemorrhagic stroke were found to be higher in survivors than in non-survivors.
Conclusion:
Iron and heme are associated with a pro-inflammatory response in the central nervous system following hemorrhagic stroke, and protections against hemoglobin and heme are lacking within the human brain. Patient inflammatory profiles were associated with a poorer prognosis, and local anti-inflammatory responses appeared to have a protective role.
Keywords:Central nervous systemCytokinesHaptoglobinHemeHemopexinInflammatory responseIronSubarachnoid hemorrhageSee more -
Original Articles
Long-term psychological outcome after discharge from intensive care
Rev Bras Ter Intensiva. 2018;30(1):28-34
Abstract
Original ArticlesLong-term psychological outcome after discharge from intensive care
Rev Bras Ter Intensiva. 2018;30(1):28-34
DOI 10.5935/0103-507X.20180008
Views0ABSTRACT
Objective:
To investigate the longterm psychological outcome in survivors of critical illness after intensive care unit discharge.
Methods:
A prospective cohort of survivors admitted to a mixed intensive care unit between January and September 2010 was evaluated six months and five years after hospital discharge. The Dementia Rating Scale-2, the Hospital Anxiety and Depression Scale, the Posttraumatic stress syndrome 14-questions inventory, the Euro Quality of Life 5 Dimensions (EQ-5-D), and the Visual Analogue Scale (EQ VAS) were assessed at both follow-up periods.
Results:
Of 267 patients, 25 patients were evaluated at 6 months after discharge (62 ± 16 years); 12 (48%) presented cognitive impairment, 6 (24%) anxiety, 4 (16%) depression, and 4 (16%) post-traumatic stress disorder. Among those re-evaluated five years after discharge (n = 17; 65 ± 15 years), the frequency of cognitive impairment dropped from 8 (47%) to 3 (18%) (p = 0.063), due to improvement in these patients over time, and other patients did not acquire any dysfunction after discharge. At five years after discharge, only two patients (12%) reported anxiety, and none had depression or post-traumatic stress disorder. No differences were found between the six-month and five-year follow-ups regarding EQ-5-D and EQ VAS.
Conclusion:
Survivors do not show a progressive decline in cognitive function or quality of life within five years after intensive care unit discharge. Psychopathological symptoms tend to decrease with time.
Keywords:AnxietyCognitive dysfunctionDepressionIntensive care unitsPatient dischargeQuality of lifeStress disorders, post-traumaticSee moreViews0Abstract
Original ArticlesLong-term psychological outcome after discharge from intensive care
Rev Bras Ter Intensiva. 2018;30(1):28-34
DOI 10.5935/0103-507X.20180008
Views0ABSTRACT
Objective:
To investigate the longterm psychological outcome in survivors of critical illness after intensive care unit discharge.
Methods:
A prospective cohort of survivors admitted to a mixed intensive care unit between January and September 2010 was evaluated six months and five years after hospital discharge. The Dementia Rating Scale-2, the Hospital Anxiety and Depression Scale, the Posttraumatic stress syndrome 14-questions inventory, the Euro Quality of Life 5 Dimensions (EQ-5-D), and the Visual Analogue Scale (EQ VAS) were assessed at both follow-up periods.
Results:
Of 267 patients, 25 patients were evaluated at 6 months after discharge (62 ± 16 years); 12 (48%) presented cognitive impairment, 6 (24%) anxiety, 4 (16%) depression, and 4 (16%) post-traumatic stress disorder. Among those re-evaluated five years after discharge (n = 17; 65 ± 15 years), the frequency of cognitive impairment dropped from 8 (47%) to 3 (18%) (p = 0.063), due to improvement in these patients over time, and other patients did not acquire any dysfunction after discharge. At five years after discharge, only two patients (12%) reported anxiety, and none had depression or post-traumatic stress disorder. No differences were found between the six-month and five-year follow-ups regarding EQ-5-D and EQ VAS.
Conclusion:
Survivors do not show a progressive decline in cognitive function or quality of life within five years after intensive care unit discharge. Psychopathological symptoms tend to decrease with time.
Keywords:AnxietyCognitive dysfunctionDepressionIntensive care unitsPatient dischargeQuality of lifeStress disorders, post-traumaticSee more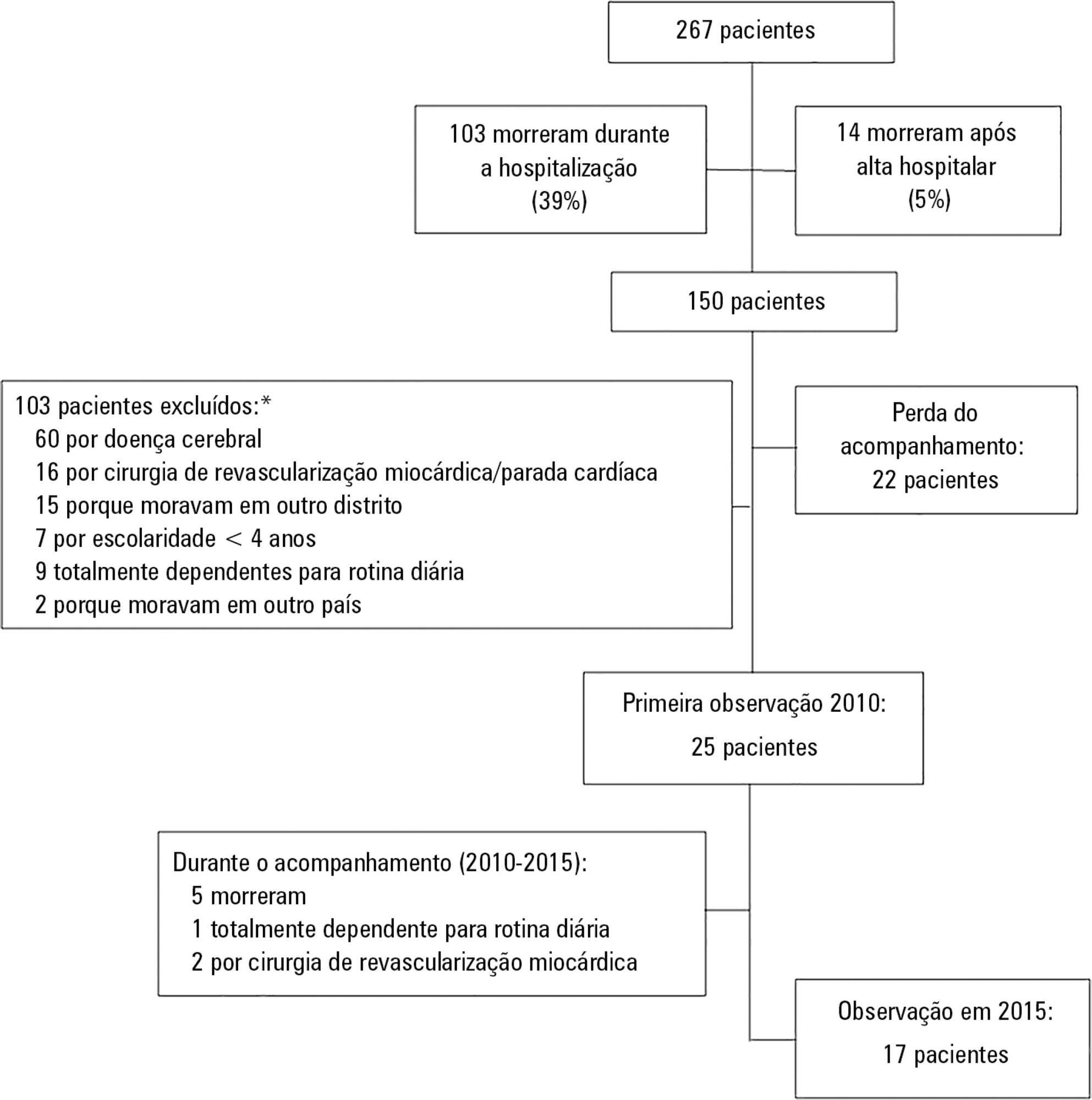
-
Original Article
Sex and spouse conditions influence symptoms of anxiety, depression, and posttraumatic stress disorder in both patients admitted to intensive care units and their spouses
Rev Bras Ter Intensiva. 2018;30(1):35-41
Abstract
Original ArticleSex and spouse conditions influence symptoms of anxiety, depression, and posttraumatic stress disorder in both patients admitted to intensive care units and their spouses
Rev Bras Ter Intensiva. 2018;30(1):35-41
DOI 10.5935/0103-507X.20180004
Views1See moreABSTRACT
Objectives:
To assess the effect of sex and spouse condition on symptoms of anxiety, depression and posttraumatic stress symptoms in patients and their spouses.
Methods:
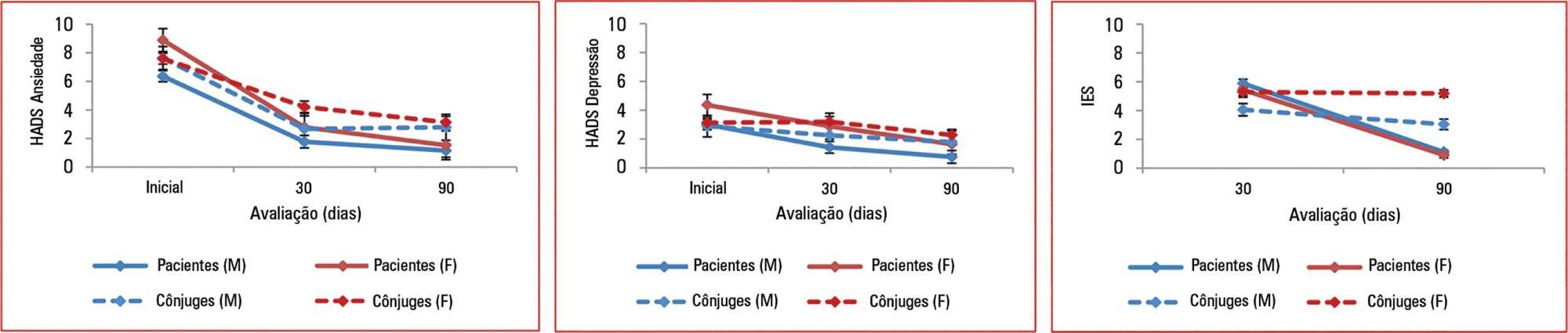
A prospective study conducted in a 22-bed adult mixed intensive care unit in a tertiary hospital in São Paulo, Brazil. Patients and their spouses were enrolled 2 days after intensive care unit admission. They were interviewed while in the intensive care unit using the Hospital Anxiety and Depression Scale. At 30 and 90 days after intensive care unit discharge, they completed the Impact of Event Scale and Hospital Anxiety and Depression Scale by phone.
Results:
From March 2011 to March 2013, we analyzed 118 patients and their spouses. We observed that female sex was associated with higher scores than male sex was in terms of the anxiety Hospital Anxiety and Depression Scale – subscale (p = 0.032) and depression (p = 0.034). There was no association between sex and posttraumatic stress disorder symptoms. However, spouses had higher Impact of Event Scale points compared with patients (p = 0.001).
Conclusions:
Female sex was associated with anxiety and depression, and spouses were more vulnerable to post-traumatic stress symptoms than the patients were. Increasing age and a later time of assessment were also associated with lower scores on the Impact of Event Scale.
Views1Abstract
Original ArticleSex and spouse conditions influence symptoms of anxiety, depression, and posttraumatic stress disorder in both patients admitted to intensive care units and their spouses
Rev Bras Ter Intensiva. 2018;30(1):35-41
DOI 10.5935/0103-507X.20180004
Views1See moreABSTRACT
Objectives:
To assess the effect of sex and spouse condition on symptoms of anxiety, depression and posttraumatic stress symptoms in patients and their spouses.
Methods:
A prospective study conducted in a 22-bed adult mixed intensive care unit in a tertiary hospital in São Paulo, Brazil. Patients and their spouses were enrolled 2 days after intensive care unit admission. They were interviewed while in the intensive care unit using the Hospital Anxiety and Depression Scale. At 30 and 90 days after intensive care unit discharge, they completed the Impact of Event Scale and Hospital Anxiety and Depression Scale by phone.
Results:
From March 2011 to March 2013, we analyzed 118 patients and their spouses. We observed that female sex was associated with higher scores than male sex was in terms of the anxiety Hospital Anxiety and Depression Scale – subscale (p = 0.032) and depression (p = 0.034). There was no association between sex and posttraumatic stress disorder symptoms. However, spouses had higher Impact of Event Scale points compared with patients (p = 0.001).
Conclusions:
Female sex was associated with anxiety and depression, and spouses were more vulnerable to post-traumatic stress symptoms than the patients were. Increasing age and a later time of assessment were also associated with lower scores on the Impact of Event Scale.
-
Original Articles
Pain assessment of traumatic brain injury victims using the Brazilian version of the Behavioral Pain Scale
Rev Bras Ter Intensiva. 2018;30(1):42-49
Abstract
Original ArticlesPain assessment of traumatic brain injury victims using the Brazilian version of the Behavioral Pain Scale
Rev Bras Ter Intensiva. 2018;30(1):42-49
DOI 10.5935/0103-507X.20180009
Views0See moreABSTRACT
Objective:
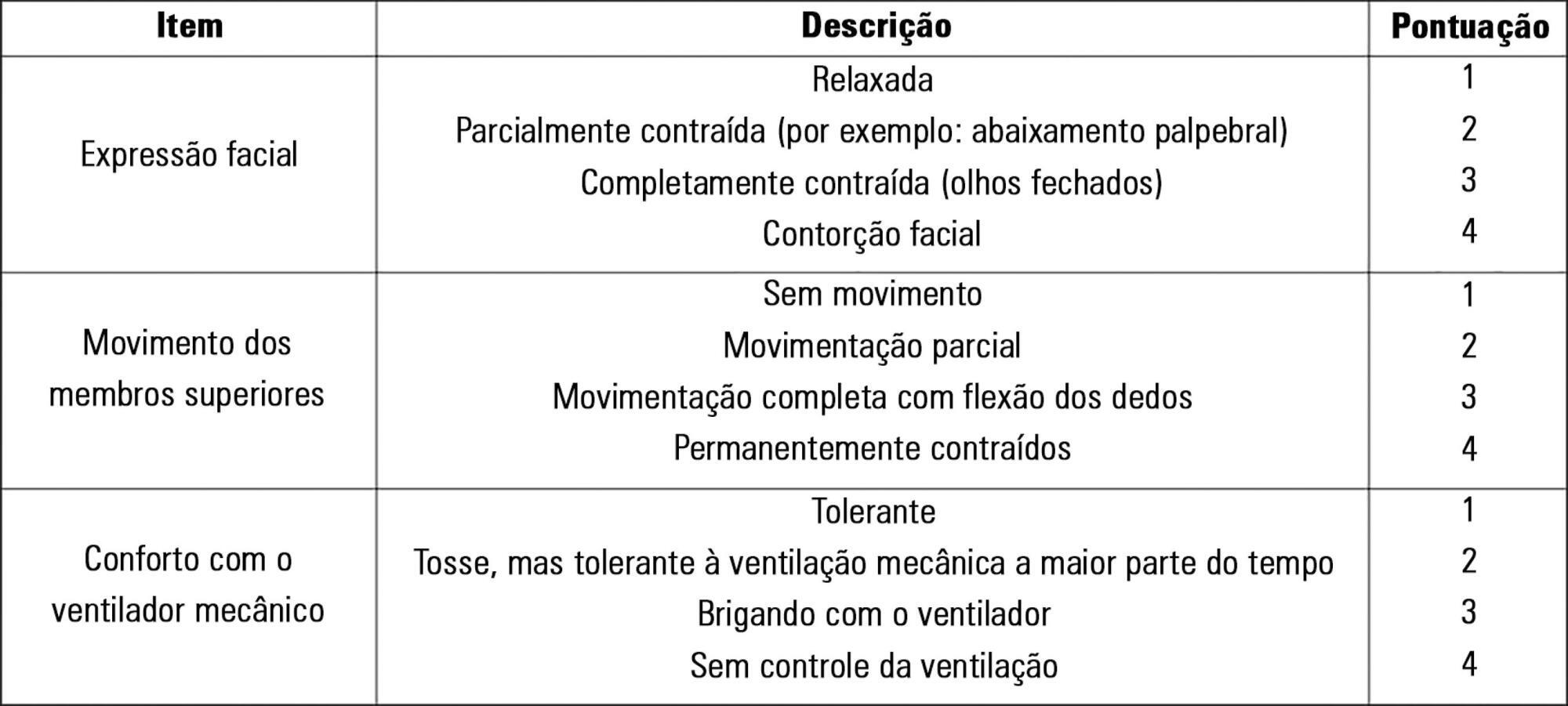
To evaluate the validity and reliability of the Brazilian version of the Behavioral Pain Scale (BPS-Br) in victims of traumatic brain injury.
Methods:
Observational prospective study with paired and repeated measures conducted at two intensive care units (clinical and surgical) of a large general hospital. The convenience sample consisted of adult victims of moderate or severe penetrating or blunt craniocerebral trauma who were sedated and mechanically ventilated. A total of 432 paired observations were performed by independent evaluators simultaneously, prior to eye cleaning, during eye cleaning, during tracheal aspiration and after tracheal aspiration. Sociodemographic, clinical, trauma-related, sedoanalgesia and physiological parameter data (heart rate, systolic and diastolic blood pressure) were collected. The discriminant validity was tested using the Friedman and Wilcoxon paired tests. The intraclass correlation coefficient and Cohen’s Kappa coefficient were used to evaluate the reliability. The Spearman correlation test was used to test the association between clinical variables and BPS-Br scores during tracheal aspiration.
Results:
There was a significant increase in the physiological parameters during tracheal aspiration, but without correlation with the BPS-Br scores. Pain was significantly more intense during tracheal aspiration (p < 0.005). Satisfactory interobserver agreement was found, with an intraclass correlation coefficient of 0.95 (0.90 - 0.98) and Kappa coefficient of 0.70.
Conclusion:
Brazilian version of the Behavioral Pain Scale scores increased during tracheal aspiration. The Brazilian version of the scale was valid and reliable for pain assessment of traumatic brain injury victims undergoing tracheal aspiration.
Views0Abstract
Original ArticlesPain assessment of traumatic brain injury victims using the Brazilian version of the Behavioral Pain Scale
Rev Bras Ter Intensiva. 2018;30(1):42-49
DOI 10.5935/0103-507X.20180009
Views0See moreABSTRACT
Objective:
To evaluate the validity and reliability of the Brazilian version of the Behavioral Pain Scale (BPS-Br) in victims of traumatic brain injury.
Methods:
Observational prospective study with paired and repeated measures conducted at two intensive care units (clinical and surgical) of a large general hospital. The convenience sample consisted of adult victims of moderate or severe penetrating or blunt craniocerebral trauma who were sedated and mechanically ventilated. A total of 432 paired observations were performed by independent evaluators simultaneously, prior to eye cleaning, during eye cleaning, during tracheal aspiration and after tracheal aspiration. Sociodemographic, clinical, trauma-related, sedoanalgesia and physiological parameter data (heart rate, systolic and diastolic blood pressure) were collected. The discriminant validity was tested using the Friedman and Wilcoxon paired tests. The intraclass correlation coefficient and Cohen’s Kappa coefficient were used to evaluate the reliability. The Spearman correlation test was used to test the association between clinical variables and BPS-Br scores during tracheal aspiration.
Results:
There was a significant increase in the physiological parameters during tracheal aspiration, but without correlation with the BPS-Br scores. Pain was significantly more intense during tracheal aspiration (p < 0.005). Satisfactory interobserver agreement was found, with an intraclass correlation coefficient of 0.95 (0.90 - 0.98) and Kappa coefficient of 0.70.
Conclusion:
Brazilian version of the Behavioral Pain Scale scores increased during tracheal aspiration. The Brazilian version of the scale was valid and reliable for pain assessment of traumatic brain injury victims undergoing tracheal aspiration.
-
Original Articles
Assessment of delirium using the PRE-DELIRIC model in an intensive care unit in Argentina
Rev Bras Ter Intensiva. 2018;30(1):50-56
Abstract
Original ArticlesAssessment of delirium using the PRE-DELIRIC model in an intensive care unit in Argentina
Rev Bras Ter Intensiva. 2018;30(1):50-56
DOI 10.5935/0103-507X.20180010
Views0ABSTRACT
Objective:
To describe the incidence of and risk factors for delirium in the intensive care unit of a tertiary care teaching hospital in Argentina and to conduct the first non-European study exploring the performance of the PREdiction of DELIRium in ICu patients (PRE-DELIRIC) model.
Methods:
Prospective observational study in a 20-bed intensive care unit of a tertiary care teaching hospital in Buenos Aires, Argentina. The PRE-DELIRIC model was applied to 178 consecutive patients within 24 hours of admission to the intensive care unit; delirium was assessed with the Confusion Assessment Method for the Intensive Care Unit (CAM-ICU).
Results:
The mean age was 64.3 ± 17.9 years. The median time of stay in the intensive care unit was 6 (range, 2 – 56) days. Of the total number of patients, 49/178 (27.5%) developed delirium, defined as a positive CAM-ICU assessment, during their stay in the intensive care unit. Patients in the delirium group were significantly older and had a significantly higher Acute Physiological and Chronic Health Evaluation II (APACHE II) score. The mortality rate in the intensive care unit was 14.6%; no significant difference was observed between the two groups. Predictive factors for the development of delirium were increased age, prolonged intensive care unit stay, and opioid use. The area under the curve for the PRE-DELIRIC model was 0.83 (95%CI; 0.77 – 0.90).
Conclusions:
The observed incidence of delirium highlights the importance of this problem in the intensive care unit setting. In this first study conducted outside Europe, PRE-DELIRIC accurately predicted the development of delirium.
Keywords:CAM-ICUDelirium/epidemiologyIntensive care unitsPRE-DELIRICPsychiatric status rating scalesrisk factorsSee moreViews0Abstract
Original ArticlesAssessment of delirium using the PRE-DELIRIC model in an intensive care unit in Argentina
Rev Bras Ter Intensiva. 2018;30(1):50-56
DOI 10.5935/0103-507X.20180010
Views0ABSTRACT
Objective:
To describe the incidence of and risk factors for delirium in the intensive care unit of a tertiary care teaching hospital in Argentina and to conduct the first non-European study exploring the performance of the PREdiction of DELIRium in ICu patients (PRE-DELIRIC) model.
Methods:
Prospective observational study in a 20-bed intensive care unit of a tertiary care teaching hospital in Buenos Aires, Argentina. The PRE-DELIRIC model was applied to 178 consecutive patients within 24 hours of admission to the intensive care unit; delirium was assessed with the Confusion Assessment Method for the Intensive Care Unit (CAM-ICU).
Results:
The mean age was 64.3 ± 17.9 years. The median time of stay in the intensive care unit was 6 (range, 2 – 56) days. Of the total number of patients, 49/178 (27.5%) developed delirium, defined as a positive CAM-ICU assessment, during their stay in the intensive care unit. Patients in the delirium group were significantly older and had a significantly higher Acute Physiological and Chronic Health Evaluation II (APACHE II) score. The mortality rate in the intensive care unit was 14.6%; no significant difference was observed between the two groups. Predictive factors for the development of delirium were increased age, prolonged intensive care unit stay, and opioid use. The area under the curve for the PRE-DELIRIC model was 0.83 (95%CI; 0.77 – 0.90).
Conclusions:
The observed incidence of delirium highlights the importance of this problem in the intensive care unit setting. In this first study conducted outside Europe, PRE-DELIRIC accurately predicted the development of delirium.
Keywords:CAM-ICUDelirium/epidemiologyIntensive care unitsPRE-DELIRICPsychiatric status rating scalesrisk factorsSee more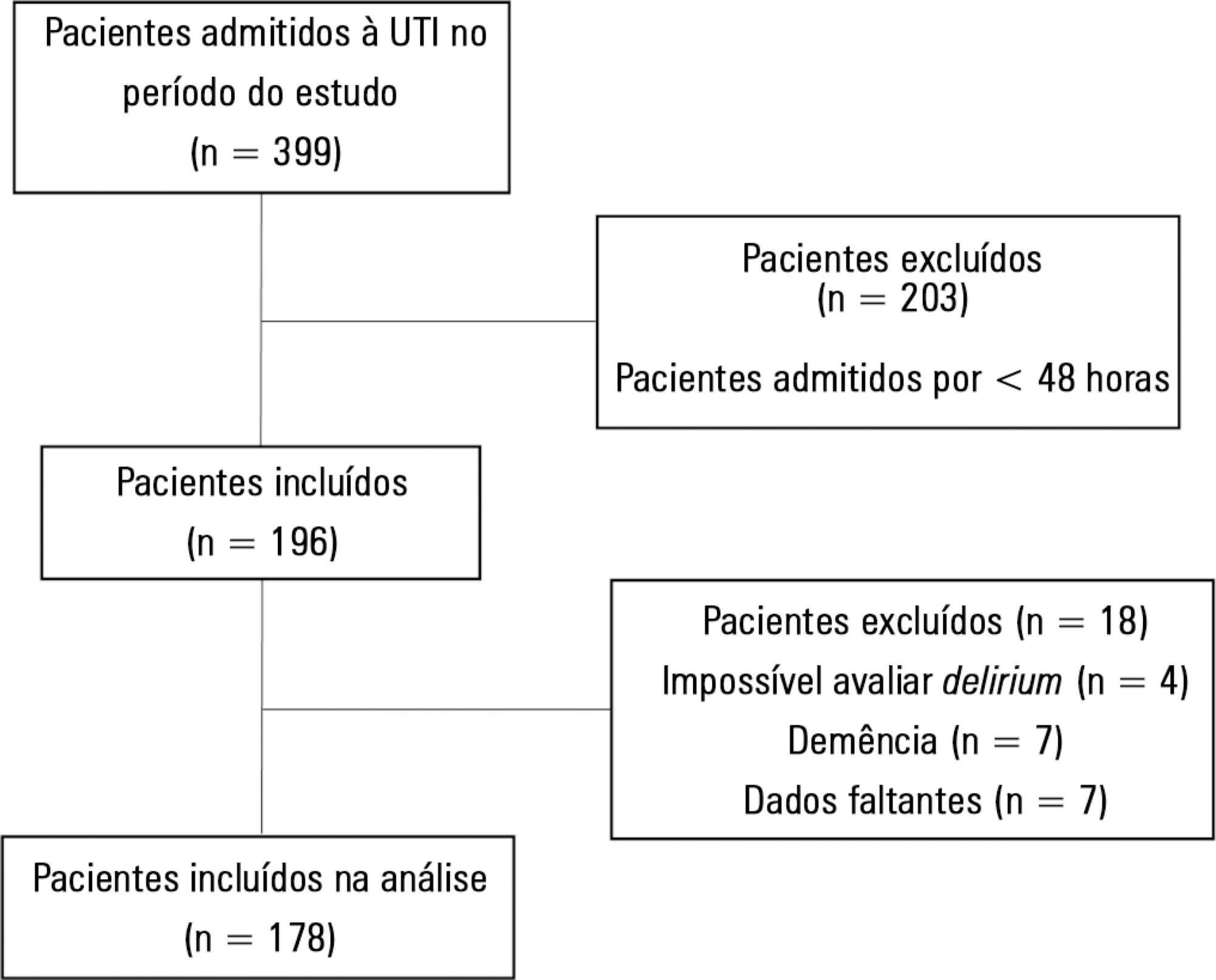
-
Original Articles
Organization of rehabilitation care in Portuguese intensive care units
Rev Bras Ter Intensiva. 2018;30(1):57-63
Abstract
Original ArticlesOrganization of rehabilitation care in Portuguese intensive care units
Rev Bras Ter Intensiva. 2018;30(1):57-63
DOI 10.5935/0103-507X.20180011
Views0ABSTRACT
Objective:
To describe the different rehabilitation care models in practice in Portuguese adult intensive care units.
Methods:
A simple observational (cross-sectional) study was conducted through an online survey sent to the head nurses or individuals responsible for the 58 adult intensive care units that are part of the database of the Sociedade Portuguesa de Cuidados Intensivos.
Results:
We identified three models of organization of rehabilitation care: care provided by the staff of the intensive care unit (22.9%), care provided by specialized external teams (25.0%), and a mixture of the previous models, combining the two situations (52.1%). In the first model, the care was provided mainly by nurses with specialization in rehabilitation and, in the second model, the care was provided by physiotherapists. No significant differences were found between the models regarding the availability of care, in hours/day or days/week (p = 0.268 and 0.994, respectively), or results such as length of hospital stay in intensive care, ventilation time, or mortality rate in the unit (p = 0.418, 0.923, and 0.240, respectively).
Conclusion:
The organization of rehabilitation care in Portuguese intensive care units is unique and heterogeneous. Despite different care organization models, the availability of hours of care is similar, as are the overall results observed in patients.
Keywords:Critical careHospital physical therapy service/organization & administrationPortugalRehabilitation nursingSee moreViews0Abstract
Original ArticlesOrganization of rehabilitation care in Portuguese intensive care units
Rev Bras Ter Intensiva. 2018;30(1):57-63
DOI 10.5935/0103-507X.20180011
Views0ABSTRACT
Objective:
To describe the different rehabilitation care models in practice in Portuguese adult intensive care units.
Methods:
A simple observational (cross-sectional) study was conducted through an online survey sent to the head nurses or individuals responsible for the 58 adult intensive care units that are part of the database of the Sociedade Portuguesa de Cuidados Intensivos.
Results:
We identified three models of organization of rehabilitation care: care provided by the staff of the intensive care unit (22.9%), care provided by specialized external teams (25.0%), and a mixture of the previous models, combining the two situations (52.1%). In the first model, the care was provided mainly by nurses with specialization in rehabilitation and, in the second model, the care was provided by physiotherapists. No significant differences were found between the models regarding the availability of care, in hours/day or days/week (p = 0.268 and 0.994, respectively), or results such as length of hospital stay in intensive care, ventilation time, or mortality rate in the unit (p = 0.418, 0.923, and 0.240, respectively).
Conclusion:
The organization of rehabilitation care in Portuguese intensive care units is unique and heterogeneous. Despite different care organization models, the availability of hours of care is similar, as are the overall results observed in patients.
Keywords:Critical careHospital physical therapy service/organization & administrationPortugalRehabilitation nursingSee more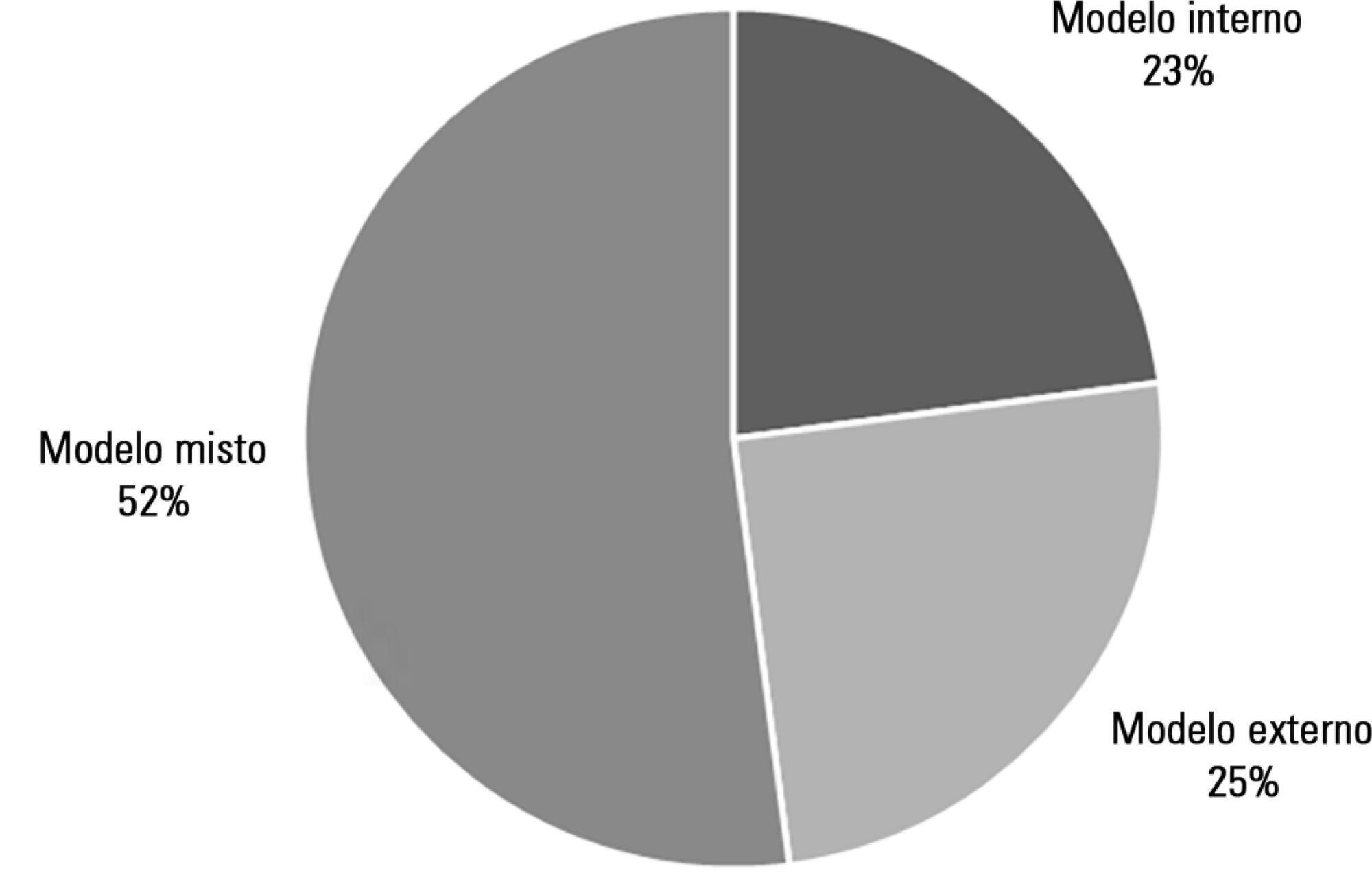
-
Original Articles
SOFA in the first 24 hours as an outcome predictor of acute liver failure
Rev Bras Ter Intensiva. 2018;30(1):64-70
Abstract
Original ArticlesSOFA in the first 24 hours as an outcome predictor of acute liver failure
Rev Bras Ter Intensiva. 2018;30(1):64-70
DOI 10.5935/0103-507X.20180012
Views2See moreABSTRACT
Objective:
To describe a cohort of patients with acute liver failure and to analyze the demographic and clinical factors associated with mortality.
Methods:
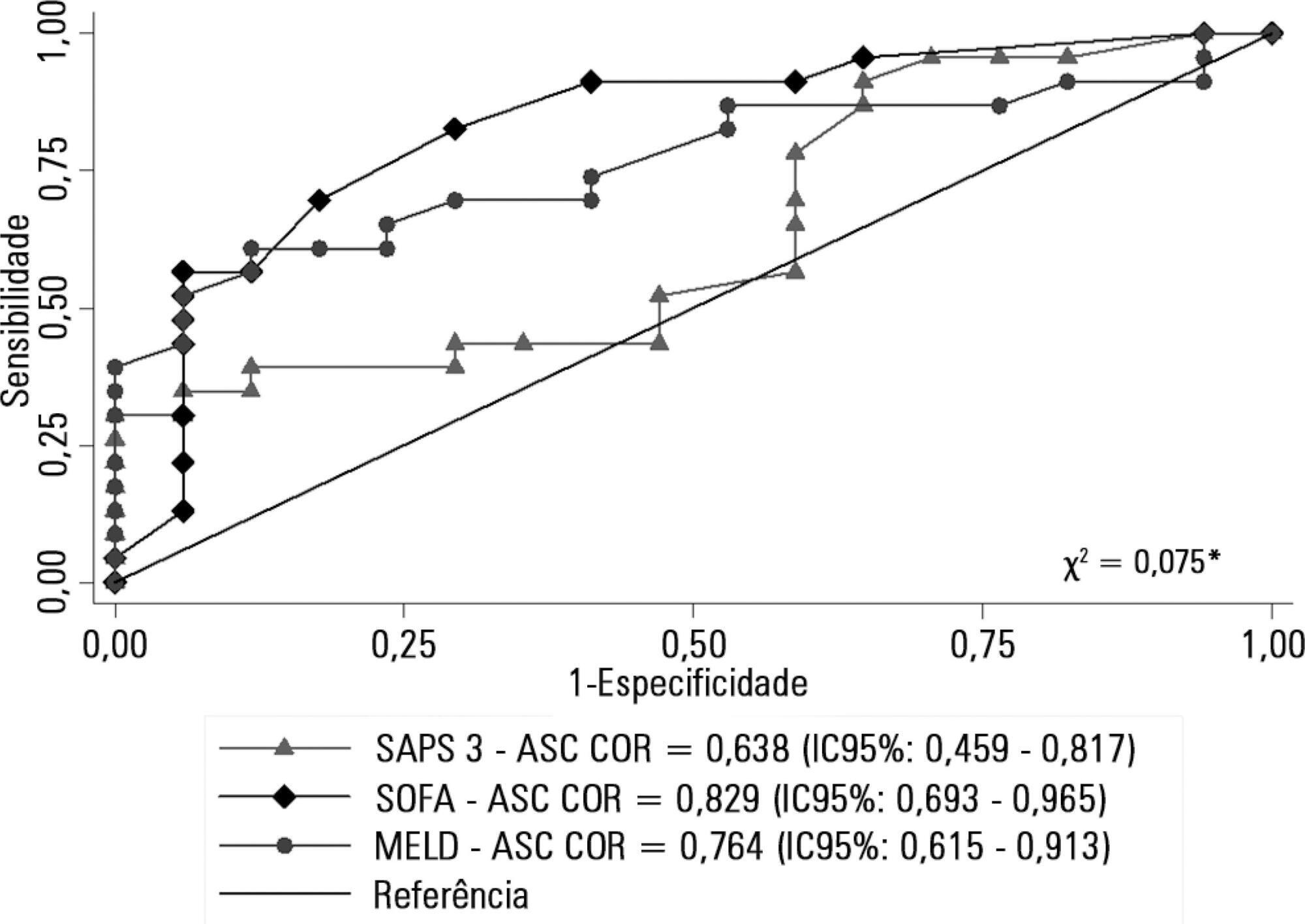
Retrospective cohort study in which all patients admitted for acute liver failure from July 28, 2012, to August 31, 2017, were included. Clinical and demographic data were collected using the Epimed System. The SAPS 3, SOFA, and MELD scores were measured. The odds ratios and 95% confidence intervals were estimated. Receiver operating characteristics curves were obtained for the prognostic scores, along with the Kaplan-Meier survival curve for the score best predicting mortality.
Results:
The majority of the 40 patients were female (77.5%), and the most frequent etiology was hepatitis B (n = 13). Only 35% of the patients underwent liver transplantation. The in-hospital mortality rate was 57.5% (95%CI: 41.5 – 73.5). Among the scores investigated, only SOFA remained associated with risk of death (OR = 1.37; 95%CI 1.11 – 1.69; p < 0.001). After SOFA stratification into < 12 and ≥ 12 points, survival was higher in patients with SOFA <12 (log-rank p < 0.001).
Conclusion:
SOFA score in the first 24 hours was the best predictor of fatal outcome.
Views2Abstract
Original ArticlesSOFA in the first 24 hours as an outcome predictor of acute liver failure
Rev Bras Ter Intensiva. 2018;30(1):64-70
DOI 10.5935/0103-507X.20180012
Views2See moreABSTRACT
Objective:
To describe a cohort of patients with acute liver failure and to analyze the demographic and clinical factors associated with mortality.
Methods:
Retrospective cohort study in which all patients admitted for acute liver failure from July 28, 2012, to August 31, 2017, were included. Clinical and demographic data were collected using the Epimed System. The SAPS 3, SOFA, and MELD scores were measured. The odds ratios and 95% confidence intervals were estimated. Receiver operating characteristics curves were obtained for the prognostic scores, along with the Kaplan-Meier survival curve for the score best predicting mortality.
Results:
The majority of the 40 patients were female (77.5%), and the most frequent etiology was hepatitis B (n = 13). Only 35% of the patients underwent liver transplantation. The in-hospital mortality rate was 57.5% (95%CI: 41.5 – 73.5). Among the scores investigated, only SOFA remained associated with risk of death (OR = 1.37; 95%CI 1.11 – 1.69; p < 0.001). After SOFA stratification into < 12 and ≥ 12 points, survival was higher in patients with SOFA <12 (log-rank p < 0.001).
Conclusion:
SOFA score in the first 24 hours was the best predictor of fatal outcome.
-
Original Articles
Translation and cross-cultural adaptation of the Pediatric Confusion Assessment Method for the Intensive Care Unit into Brazilian Portuguese for the detection of delirium in pediatric intensive care units
Rev Bras Ter Intensiva. 2018;30(1):71-79
Abstract
Original ArticlesTranslation and cross-cultural adaptation of the Pediatric Confusion Assessment Method for the Intensive Care Unit into Brazilian Portuguese for the detection of delirium in pediatric intensive care units
Rev Bras Ter Intensiva. 2018;30(1):71-79
DOI 10.5935/0103-507X.20180013
Views0ABSTRACT
Objective:
To undertake the translation and cross-cultural adaption into Brazilian Portuguese of the Pediatric Confusion Assessment Method for the Intensive Care Unit for the detection of delirium in pediatric intensive care units, including the algorithm and instructions.
Methods:
A universalist approach for the translation and cross-cultural adaptation of health measurement instruments was used. A group of pediatric critical care specialists assessed conceptual and item equivalences. Semantic equivalence was evaluated by means of a translation from English to Portuguese by two independent translators; reconciliation into a single version; back-translation by a native English speaker; and consensus among six experts with respect to language and content understanding by means of Likert scale responses and the Content Validity Index. Finally, operational equivalence was assessed by applying a pre-test to 30 patients.
Results:
The back-translation was approved by the original authors. The medians of the expert consensus responses varied between good and excellent, except for the feature “acute onset” of the instructions. Items with a low Content Validity Index for the features “acute onset” and “disorganized thinking” were adapted. In the pre-test, the expression “signal with your head” was modified into “nod your head” for better understanding. No further adjustments were necessary, resulting in the final version for Brazilian Portuguese.
Conclusion:
The Brazilian version of the Pediatric Confusion Assessment Method for the Intensive Care Unit was generated in agreement with the international recommendations and can be used in Brazil for the diagnosis of delirium in critically ill children 5 years of age or above and with no developmental cognitive disabilities.
Keywords:Confusion/diagnosisDelirium/diagnosisIntensive care units, pediatricpCAM-ICUSurveys and Questionnaires/standardsTranslationSee moreViews0Abstract
Original ArticlesTranslation and cross-cultural adaptation of the Pediatric Confusion Assessment Method for the Intensive Care Unit into Brazilian Portuguese for the detection of delirium in pediatric intensive care units
Rev Bras Ter Intensiva. 2018;30(1):71-79
DOI 10.5935/0103-507X.20180013
Views0ABSTRACT
Objective:
To undertake the translation and cross-cultural adaption into Brazilian Portuguese of the Pediatric Confusion Assessment Method for the Intensive Care Unit for the detection of delirium in pediatric intensive care units, including the algorithm and instructions.
Methods:
A universalist approach for the translation and cross-cultural adaptation of health measurement instruments was used. A group of pediatric critical care specialists assessed conceptual and item equivalences. Semantic equivalence was evaluated by means of a translation from English to Portuguese by two independent translators; reconciliation into a single version; back-translation by a native English speaker; and consensus among six experts with respect to language and content understanding by means of Likert scale responses and the Content Validity Index. Finally, operational equivalence was assessed by applying a pre-test to 30 patients.
Results:
The back-translation was approved by the original authors. The medians of the expert consensus responses varied between good and excellent, except for the feature “acute onset” of the instructions. Items with a low Content Validity Index for the features “acute onset” and “disorganized thinking” were adapted. In the pre-test, the expression “signal with your head” was modified into “nod your head” for better understanding. No further adjustments were necessary, resulting in the final version for Brazilian Portuguese.
Conclusion:
The Brazilian version of the Pediatric Confusion Assessment Method for the Intensive Care Unit was generated in agreement with the international recommendations and can be used in Brazil for the diagnosis of delirium in critically ill children 5 years of age or above and with no developmental cognitive disabilities.
Keywords:Confusion/diagnosisDelirium/diagnosisIntensive care units, pediatricpCAM-ICUSurveys and Questionnaires/standardsTranslationSee more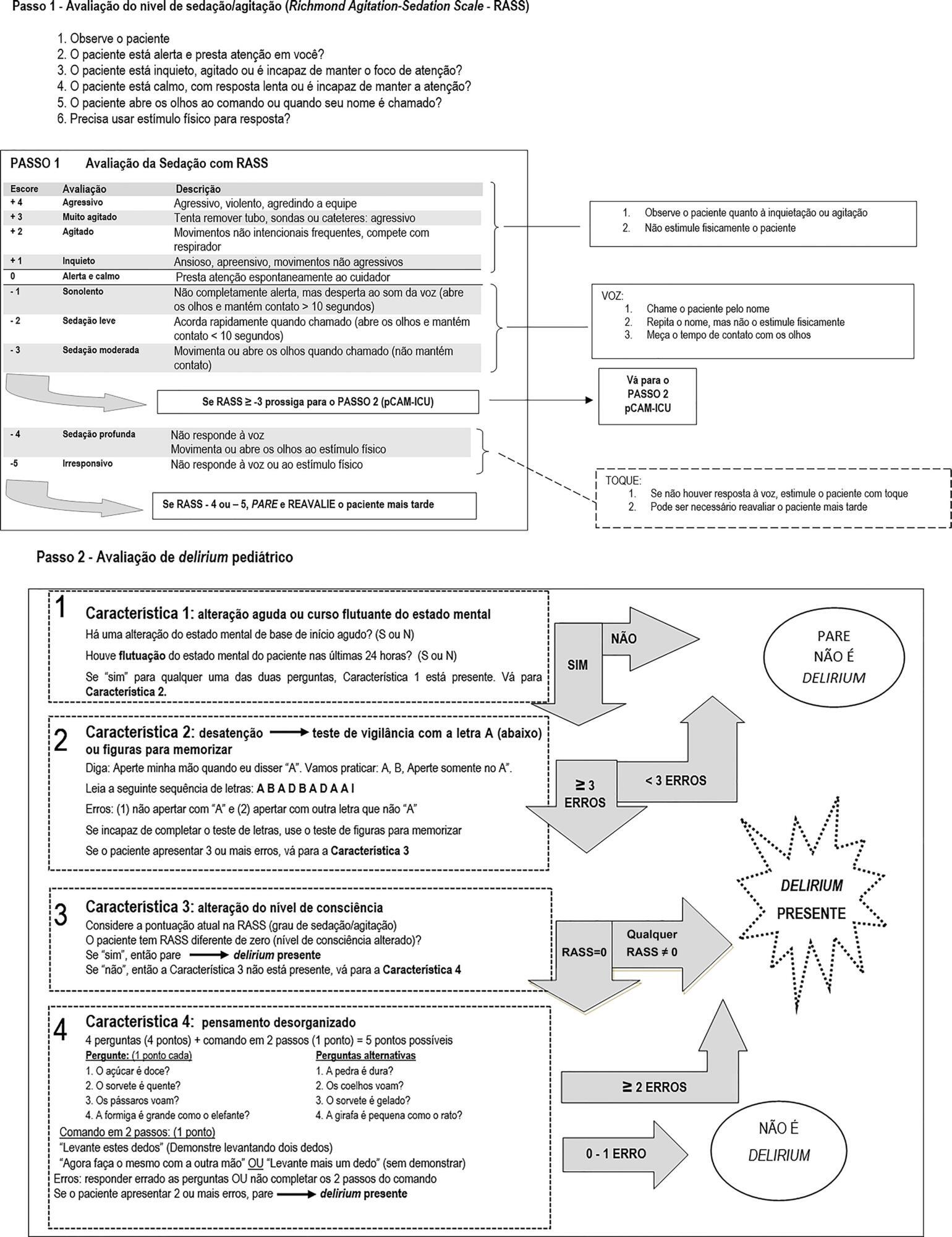
-
Review Articles
Antibiotic therapy in ventilator-associated tracheobronchitis: a literature review
Rev Bras Ter Intensiva. 2018;30(1):80-85
Abstract
Review ArticlesAntibiotic therapy in ventilator-associated tracheobronchitis: a literature review
Rev Bras Ter Intensiva. 2018;30(1):80-85
DOI 10.5935/0103-507X.20180014
Views0ABSTRACT
The concept of ventilator-associated tracheobronchitis is controversial; its definition is not unanimously accepted and often overlaps with ventilator-associated pneumonia. Ventilator-associated tracheobronchitis has an incidence similar to that of ventilator-associated pneumonia, with a high prevalence of isolated multiresistant agents, resulting in an increase in the time of mechanical ventilation and hospitalization but without an impact on mortality. The performance of quantitative cultures may allow better diagnostic definition of tracheobronchitis associated with mechanical ventilation, possibly avoiding the overdiagnosis of this condition. One of the major difficulties in differentiating between ventilator-associated tracheobronchitis and ventilator-associated pneumonia is the exclusion of a pulmonary infiltrate by chest radiography; thoracic computed tomography, thoracic ultrasonography, or invasive specimen collection may also be required. The institution of systemic antibiotic therapy does not improve the clinical impact of ventilator-associated tracheobronchitis, particularly in reducing time of mechanical ventilation, hospitalization or mortality, despite the possible reduced progression to ventilator-associated pneumonia. However, there are doubts regarding the methodology used. Thus, considering the high prevalence of tracheobronchitis associated with mechanical ventilation, routine treatment of this condition would result in high antibiotic usage without clear benefits. However, we suggest the institution of antibiotic therapy in patients with tracheobronchitis associated with mechanical ventilation and septic shock and/or worsening of oxygenation, and other auxiliary diagnostic tests should be simultaneously performed to exclude ventilator-associated pneumonia. This review provides a better understanding of the differentiation between tracheobronchitis associated with mechanical ventilation and pneumonia associated with mechanical ventilation, which can significantly decrease the use of antibiotics in critically ventilated patients.
Keywords:Bronchitis/diagnosisBronchitis/drug therapyBronchitis/epidemiologyBronchitis/microbiologyPneumonia ventilator-associated/drug therapyTracheitis/diagnosisTracheitis/drug therapyTracheitis/epidemiologyTracheitis/microbiologySee moreViews0Abstract
Review ArticlesAntibiotic therapy in ventilator-associated tracheobronchitis: a literature review
Rev Bras Ter Intensiva. 2018;30(1):80-85
DOI 10.5935/0103-507X.20180014
Views0ABSTRACT
The concept of ventilator-associated tracheobronchitis is controversial; its definition is not unanimously accepted and often overlaps with ventilator-associated pneumonia. Ventilator-associated tracheobronchitis has an incidence similar to that of ventilator-associated pneumonia, with a high prevalence of isolated multiresistant agents, resulting in an increase in the time of mechanical ventilation and hospitalization but without an impact on mortality. The performance of quantitative cultures may allow better diagnostic definition of tracheobronchitis associated with mechanical ventilation, possibly avoiding the overdiagnosis of this condition. One of the major difficulties in differentiating between ventilator-associated tracheobronchitis and ventilator-associated pneumonia is the exclusion of a pulmonary infiltrate by chest radiography; thoracic computed tomography, thoracic ultrasonography, or invasive specimen collection may also be required. The institution of systemic antibiotic therapy does not improve the clinical impact of ventilator-associated tracheobronchitis, particularly in reducing time of mechanical ventilation, hospitalization or mortality, despite the possible reduced progression to ventilator-associated pneumonia. However, there are doubts regarding the methodology used. Thus, considering the high prevalence of tracheobronchitis associated with mechanical ventilation, routine treatment of this condition would result in high antibiotic usage without clear benefits. However, we suggest the institution of antibiotic therapy in patients with tracheobronchitis associated with mechanical ventilation and septic shock and/or worsening of oxygenation, and other auxiliary diagnostic tests should be simultaneously performed to exclude ventilator-associated pneumonia. This review provides a better understanding of the differentiation between tracheobronchitis associated with mechanical ventilation and pneumonia associated with mechanical ventilation, which can significantly decrease the use of antibiotics in critically ventilated patients.
Keywords:Bronchitis/diagnosisBronchitis/drug therapyBronchitis/epidemiologyBronchitis/microbiologyPneumonia ventilator-associated/drug therapyTracheitis/diagnosisTracheitis/drug therapyTracheitis/epidemiologyTracheitis/microbiologySee more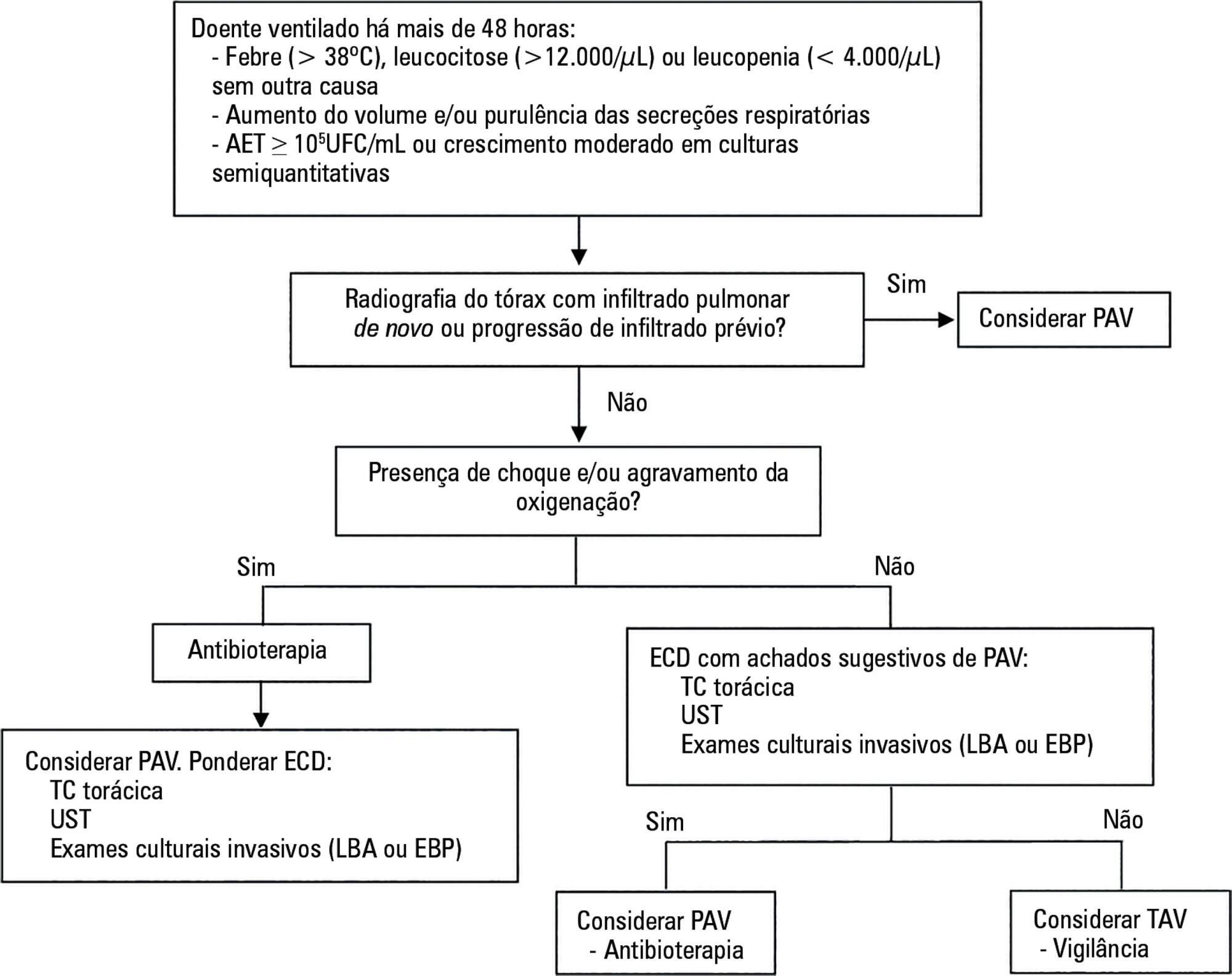
-
Review Articles
Humidification and heating of inhaled gas in patients with artificial airway. A narrative review
Rev Bras Ter Intensiva. 2018;30(1):86-97
Abstract
Review ArticlesHumidification and heating of inhaled gas in patients with artificial airway. A narrative review
Rev Bras Ter Intensiva. 2018;30(1):86-97
DOI 10.5935/0103-507X.20180015
Views2See moreABSTRACT
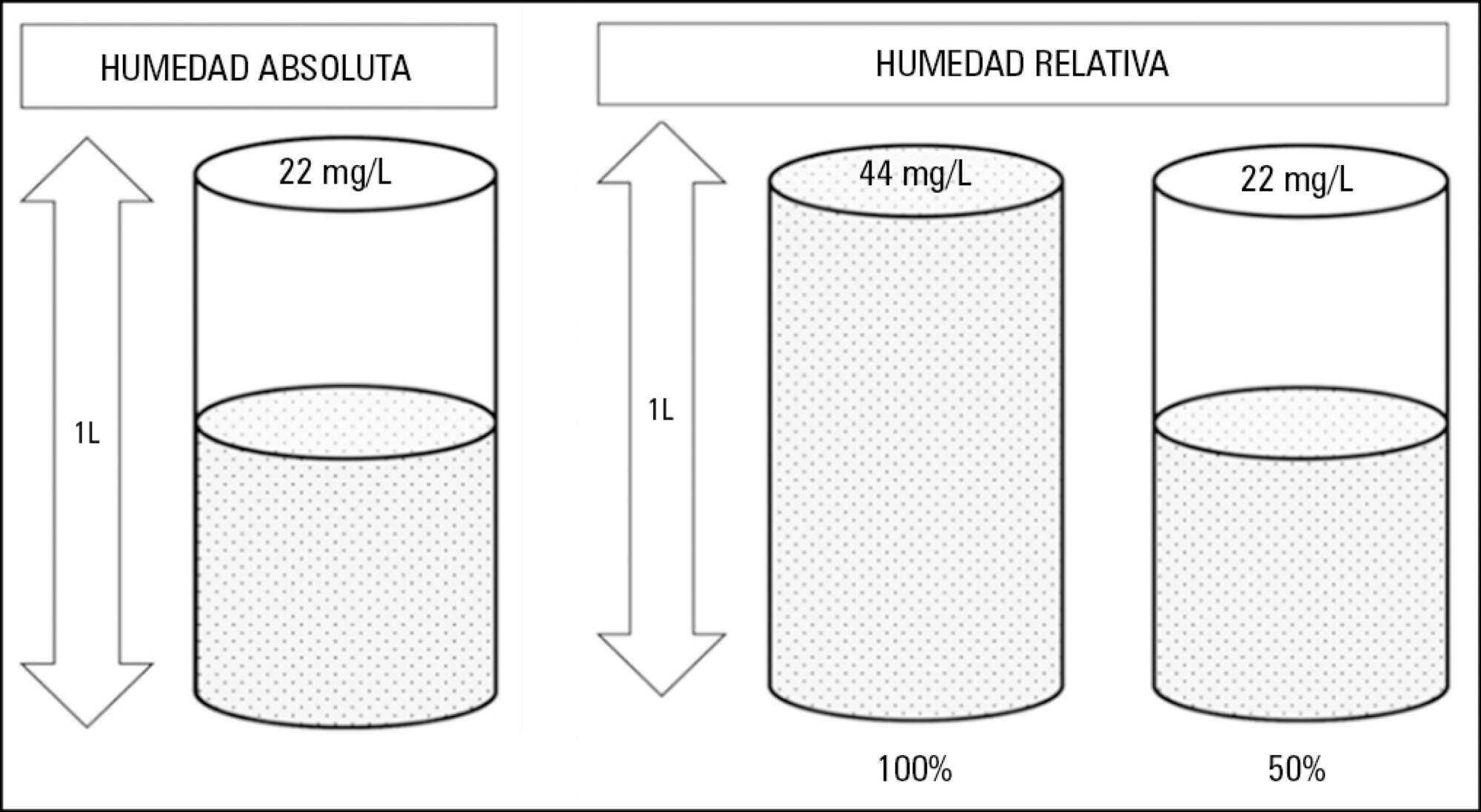
Instrumentation of the airways in critical patients (endotracheal tube or tracheostomy cannula) prevents them from performing their function of humidify and heating the inhaled gas. In addition, the administration of cold and dry medical gases and the high flows that patients experience during invasive and non-invasive mechanical ventilation generate an even worse condition. For this reason, a device for gas conditioning is needed, even in short-term treatments, to avoid potential damage to the structure and function of the respiratory epithelium. In the field of intensive therapy, the use of heat and moisture exchangers is common for this purpose, as is the use of active humidification systems. Acquiring knowledge about technical specifications and the advantages and disadvantages of each device is needed for proper use since the conditioning of inspired gases is a key intervention in patients with artificial airway and has become routine care. Incorrect selection or inappropriate configuration of a device can have a negative impact on clinical outcomes. The members of the Capítulo de Kinesiología Intensivista of the Sociedad Argentina de Terapia Intensiva conducted a narrative review aiming to show the available evidence regarding conditioning of inhaled gas in patients with artificial airways, going into detail on concepts related to the working principles of each one.
Views2Abstract
Review ArticlesHumidification and heating of inhaled gas in patients with artificial airway. A narrative review
Rev Bras Ter Intensiva. 2018;30(1):86-97
DOI 10.5935/0103-507X.20180015
Views2See moreABSTRACT
Instrumentation of the airways in critical patients (endotracheal tube or tracheostomy cannula) prevents them from performing their function of humidify and heating the inhaled gas. In addition, the administration of cold and dry medical gases and the high flows that patients experience during invasive and non-invasive mechanical ventilation generate an even worse condition. For this reason, a device for gas conditioning is needed, even in short-term treatments, to avoid potential damage to the structure and function of the respiratory epithelium. In the field of intensive therapy, the use of heat and moisture exchangers is common for this purpose, as is the use of active humidification systems. Acquiring knowledge about technical specifications and the advantages and disadvantages of each device is needed for proper use since the conditioning of inspired gases is a key intervention in patients with artificial airway and has become routine care. Incorrect selection or inappropriate configuration of a device can have a negative impact on clinical outcomes. The members of the Capítulo de Kinesiología Intensivista of the Sociedad Argentina de Terapia Intensiva conducted a narrative review aiming to show the available evidence regarding conditioning of inhaled gas in patients with artificial airways, going into detail on concepts related to the working principles of each one.
-
Review Articles
Post-intensive care outpatient clinic: is it feasible and effective? A literature review
Rev Bras Ter Intensiva. 2018;30(1):98-111
Abstract
Review ArticlesPost-intensive care outpatient clinic: is it feasible and effective? A literature review
Rev Bras Ter Intensiva. 2018;30(1):98-111
DOI 10.5935/0103-507X.20180016
Views0See moreABSTRACT
The follow-up of patients who are discharged from intensive care units follows distinct flows in different parts of the world. Outpatient clinics or post-intensive care clinics represent one of the forms of follow-up, with more than 20 years of experience in some countries. Qualitative studies that followed up patients in these outpatient clinics suggest more encouraging results than quantitative studies, demonstrating improvements in intermediate outcomes, such as patient and family satisfaction. More important results, such as mortality and improvement in the quality of life of patients and their families, have not yet been demonstrated. In addition, which patients should be indicated for these outpatient clinics? How long should they be followed up? Can we expect an improvement of clinical outcomes in these followed-up patients? Are outpatient clinics cost-effective? These are only some of the questions that arise from this form of follow-up of the survivors of intensive care units. This article aims to review all aspects relating to the organization and performance of post-intensive care outpatient clinics and to provide an overview of studies that evaluated clinical outcomes related to this practice.
Views0Abstract
Review ArticlesPost-intensive care outpatient clinic: is it feasible and effective? A literature review
Rev Bras Ter Intensiva. 2018;30(1):98-111
DOI 10.5935/0103-507X.20180016
Views0See moreABSTRACT
The follow-up of patients who are discharged from intensive care units follows distinct flows in different parts of the world. Outpatient clinics or post-intensive care clinics represent one of the forms of follow-up, with more than 20 years of experience in some countries. Qualitative studies that followed up patients in these outpatient clinics suggest more encouraging results than quantitative studies, demonstrating improvements in intermediate outcomes, such as patient and family satisfaction. More important results, such as mortality and improvement in the quality of life of patients and their families, have not yet been demonstrated. In addition, which patients should be indicated for these outpatient clinics? How long should they be followed up? Can we expect an improvement of clinical outcomes in these followed-up patients? Are outpatient clinics cost-effective? These are only some of the questions that arise from this form of follow-up of the survivors of intensive care units. This article aims to review all aspects relating to the organization and performance of post-intensive care outpatient clinics and to provide an overview of studies that evaluated clinical outcomes related to this practice.
-
Case Reports
Accidental strangulation in children by the automatic closing of a car window
Rev Bras Ter Intensiva. 2018;30(1):112-115
Abstract
Case ReportsAccidental strangulation in children by the automatic closing of a car window
Rev Bras Ter Intensiva. 2018;30(1):112-115
DOI 10.5935/0103-507X.20180017
Views1See moreABSTRACT
Among the main causes of death in our country are car accidents, drowning and accidental burns. Strangulation is a potentially fatal injury and an important cause of homicide and suicide among adults and adolescents. In children, its occurrence is usually accidental. However, in recent years, several cases of accidental strangulation in children around the world have been reported. A 2-year-old male patient was strangled in a car window. The patient was admitted to the pediatric intensive care unit with a Glasgow Coma Scale score of 8 and presented with progressive worsening of respiratory dysfunction and torpor. The patient also presented acute respiratory distress syndrome, acute pulmonary edema and shock. He was managed with protective mechanical ventilation, vasoactive drugs and antibiotic therapy. He was discharged from the intensive care unit without neurological or pulmonary sequelae. After 12 days of hospitalization, he was discharged from the hospital, and his state was very good. The incidence of automobile window strangulation is rare but of high morbidity and mortality due to the resulting choking mechanism. Fortunately, newer cars have devices that stop the automatic closing of the windows if resistance is encountered. However, considering the severity of complications strangulated patients experience, the intensive neuro-ventilatory and hemodynamic management of the pathologies involved is important to reduce morbidity and mortality, as is the need to implement new campaigns for the education of parents and caregivers of children, aiming to avoid easily preventable accidents and to optimize safety mechanisms in cars with electric windows.
Views1Abstract
Case ReportsAccidental strangulation in children by the automatic closing of a car window
Rev Bras Ter Intensiva. 2018;30(1):112-115
DOI 10.5935/0103-507X.20180017
Views1See moreABSTRACT
Among the main causes of death in our country are car accidents, drowning and accidental burns. Strangulation is a potentially fatal injury and an important cause of homicide and suicide among adults and adolescents. In children, its occurrence is usually accidental. However, in recent years, several cases of accidental strangulation in children around the world have been reported. A 2-year-old male patient was strangled in a car window. The patient was admitted to the pediatric intensive care unit with a Glasgow Coma Scale score of 8 and presented with progressive worsening of respiratory dysfunction and torpor. The patient also presented acute respiratory distress syndrome, acute pulmonary edema and shock. He was managed with protective mechanical ventilation, vasoactive drugs and antibiotic therapy. He was discharged from the intensive care unit without neurological or pulmonary sequelae. After 12 days of hospitalization, he was discharged from the hospital, and his state was very good. The incidence of automobile window strangulation is rare but of high morbidity and mortality due to the resulting choking mechanism. Fortunately, newer cars have devices that stop the automatic closing of the windows if resistance is encountered. However, considering the severity of complications strangulated patients experience, the intensive neuro-ventilatory and hemodynamic management of the pathologies involved is important to reduce morbidity and mortality, as is the need to implement new campaigns for the education of parents and caregivers of children, aiming to avoid easily preventable accidents and to optimize safety mechanisms in cars with electric windows.

-
Case Report
Massive hemoptysis successfully treated with extracorporeal membrane oxygenation and endobronchial thrombolysis
Rev Bras Ter Intensiva. 2018;30(1):116-120
Abstract
Case ReportMassive hemoptysis successfully treated with extracorporeal membrane oxygenation and endobronchial thrombolysis
Rev Bras Ter Intensiva. 2018;30(1):116-120
DOI 10.5935/0103-507X.20180002
Views1See moreABSTRACT
Extracorporeal membrane oxygenation has been used to treat refractory hypoxemia in numerous clinical scenarios. The fundamental principles for the management of massive hemoptysis patients include protecting the airway and healthy lung, locating the source of bleeding and controlling the hemorrhage. We report the case of a patient with acute respiratory failure associated with massive hemoptysis secondary to lung laceration during cardiac surgery. The use of extracorporeal membrane oxygenation allowed patient survival. However, due to the great difficulty in managing pulmonary clots after hemoptysis, it was necessary to use an unusual therapy involving endobronchial infusion of a thrombolytic agent as described in rare cases in the literature.
Views1Abstract
Case ReportMassive hemoptysis successfully treated with extracorporeal membrane oxygenation and endobronchial thrombolysis
Rev Bras Ter Intensiva. 2018;30(1):116-120
DOI 10.5935/0103-507X.20180002
Views1See moreABSTRACT
Extracorporeal membrane oxygenation has been used to treat refractory hypoxemia in numerous clinical scenarios. The fundamental principles for the management of massive hemoptysis patients include protecting the airway and healthy lung, locating the source of bleeding and controlling the hemorrhage. We report the case of a patient with acute respiratory failure associated with massive hemoptysis secondary to lung laceration during cardiac surgery. The use of extracorporeal membrane oxygenation allowed patient survival. However, due to the great difficulty in managing pulmonary clots after hemoptysis, it was necessary to use an unusual therapy involving endobronchial infusion of a thrombolytic agent as described in rare cases in the literature.
-
Case Reports
Symptomatic bradycardia due to nicotine intoxication
Rev Bras Ter Intensiva. 2018;30(1):121-126
Abstract
Case ReportsSymptomatic bradycardia due to nicotine intoxication
Rev Bras Ter Intensiva. 2018;30(1):121-126
DOI 10.5935/0103-507X.20180018
Views0See moreABSTRACT
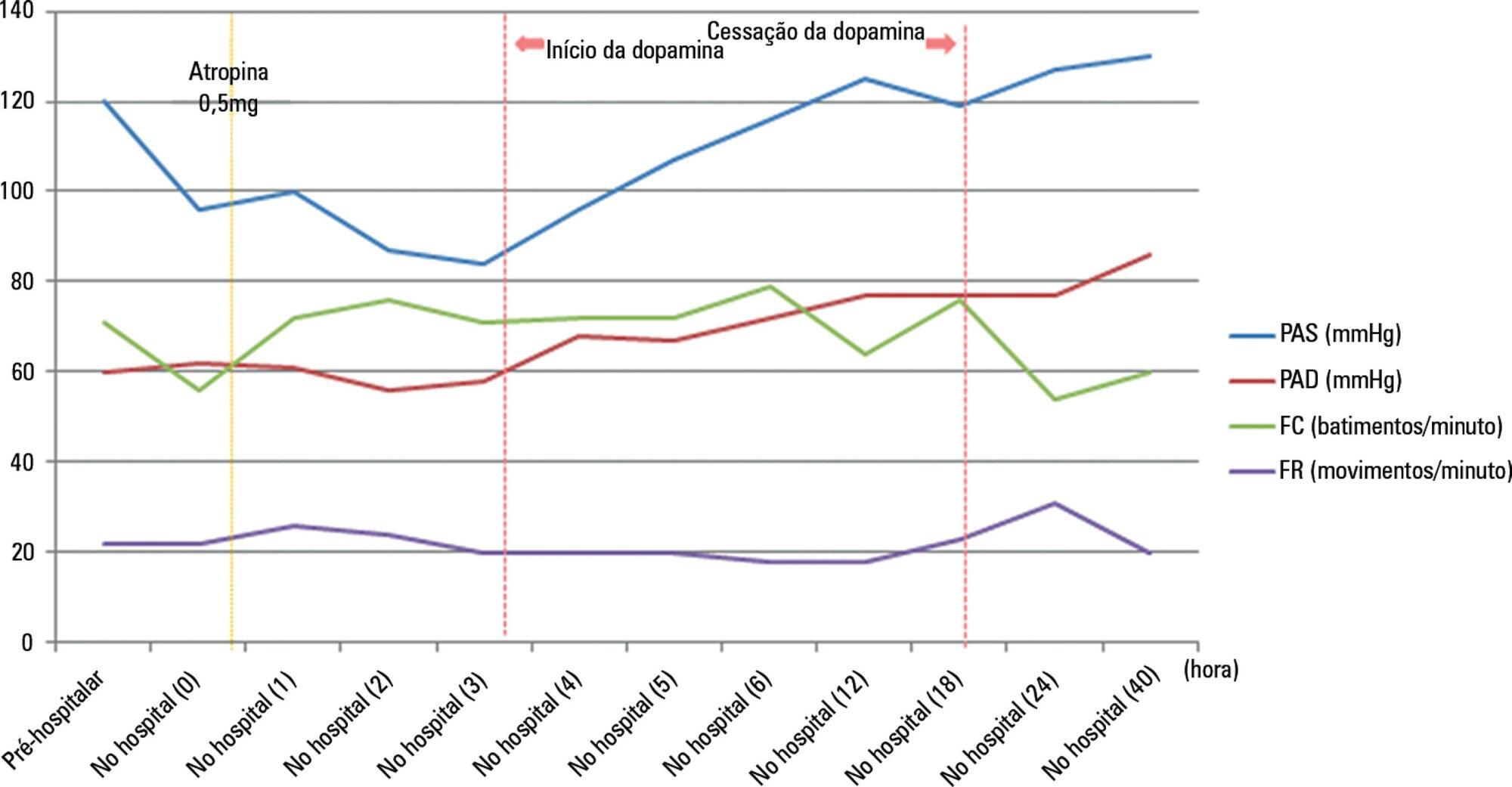
Nicotine is a dangerous substance extracted from tobacco leaves. When nicotine is absorbed in excessive amounts, it can lead to respiratory failure and cardiac arrest. The commercialization of electronic cigarettes (e-cigarettes) has allowed users to directly handle e-cigarette liquid. Consequently, the risk of liquid nicotine exposure has increased. We describe our experience of managing the case of a patient who orally ingested a high concentration of liquid nicotine from e-cigarette liquid. The patient presented with bradycardia and hypotension, which are symptoms of parasympathetic stimulation, together with impaired consciousness. He recovered following treatment with atropine and a vasopressor.
Views0Abstract
Case ReportsSymptomatic bradycardia due to nicotine intoxication
Rev Bras Ter Intensiva. 2018;30(1):121-126
DOI 10.5935/0103-507X.20180018
Views0See moreABSTRACT
Nicotine is a dangerous substance extracted from tobacco leaves. When nicotine is absorbed in excessive amounts, it can lead to respiratory failure and cardiac arrest. The commercialization of electronic cigarettes (e-cigarettes) has allowed users to directly handle e-cigarette liquid. Consequently, the risk of liquid nicotine exposure has increased. We describe our experience of managing the case of a patient who orally ingested a high concentration of liquid nicotine from e-cigarette liquid. The patient presented with bradycardia and hypotension, which are symptoms of parasympathetic stimulation, together with impaired consciousness. He recovered following treatment with atropine and a vasopressor.
-
Case Reports
Influenza A non-H1N1 associated with acute respiratory failure and acute renal failure in a previously vaccinated cystic fibrosis patient
Rev Bras Ter Intensiva. 2018;30(1):127-130
Abstract
Case ReportsInfluenza A non-H1N1 associated with acute respiratory failure and acute renal failure in a previously vaccinated cystic fibrosis patient
Rev Bras Ter Intensiva. 2018;30(1):127-130
DOI 10.5935/0103-507X.20180019
Views1See moreABSTRACT
In the 2014 – 2015 season, most influenza infections were due to A (H3N2) viruses. More than two-thirds of circulating A (H3N2) viruses are antigenically and genetically different (drifted) from the A (H3N2) vaccine component of 2014 – 2015 northern and southern Hemisphere seasonal influenza vaccines. The purpose of this paper is to report a case of seasonal influenza A non-H1N1 infection that occurred in June 2015 in an adult cystic fibrosis patient with severe lung disease previously vaccinated with the anti-flu trivalent vaccine. The patient evolved to respiratory and renal failure (without rhabdomyolysis) and was placed under mechanical ventilation and hemodialysis. The clinical outcome was positive after 39 days of hospital stay. In addition, the patient was clinically stable after 18 months of follow-up. With the recent advances in critical care medicine and in cystic fibrosis treatment, survival with advanced pulmonary disease in cystic fibrosis presents new questions and potential problems, which are still being formulated.
Views1Abstract
Case ReportsInfluenza A non-H1N1 associated with acute respiratory failure and acute renal failure in a previously vaccinated cystic fibrosis patient
Rev Bras Ter Intensiva. 2018;30(1):127-130
DOI 10.5935/0103-507X.20180019
Views1See moreABSTRACT
In the 2014 – 2015 season, most influenza infections were due to A (H3N2) viruses. More than two-thirds of circulating A (H3N2) viruses are antigenically and genetically different (drifted) from the A (H3N2) vaccine component of 2014 – 2015 northern and southern Hemisphere seasonal influenza vaccines. The purpose of this paper is to report a case of seasonal influenza A non-H1N1 infection that occurred in June 2015 in an adult cystic fibrosis patient with severe lung disease previously vaccinated with the anti-flu trivalent vaccine. The patient evolved to respiratory and renal failure (without rhabdomyolysis) and was placed under mechanical ventilation and hemodialysis. The clinical outcome was positive after 39 days of hospital stay. In addition, the patient was clinically stable after 18 months of follow-up. With the recent advances in critical care medicine and in cystic fibrosis treatment, survival with advanced pulmonary disease in cystic fibrosis presents new questions and potential problems, which are still being formulated.

-
Letter to the Editor
To: Behavior of lung ultrasound findings during spontaneous breathing trial
Rev Bras Ter Intensiva. 2018;30(1):131-132
Abstract
Letter to the EditorTo: Behavior of lung ultrasound findings during spontaneous breathing trial
Rev Bras Ter Intensiva. 2018;30(1):131-132
DOI 10.5935/0103-507X.20180020
Views0To the Editor The new century brought a “new” kid on the block to the field of intensive care. Ultrasound (US) came from the radiology departments, and it has renewed intensive care medicine. Focused on the critical care patient and with the intensivist as a performer, US has set a new paradigm for medicine. Due […]See moreViews0Abstract
Letter to the EditorTo: Behavior of lung ultrasound findings during spontaneous breathing trial
Rev Bras Ter Intensiva. 2018;30(1):131-132
DOI 10.5935/0103-507X.20180020
Views0To the Editor The new century brought a “new” kid on the block to the field of intensive care. Ultrasound (US) came from the radiology departments, and it has renewed intensive care medicine. Focused on the critical care patient and with the intensivist as a performer, US has set a new paradigm for medicine. Due […]See more
Volume Articles - Critical Care Science (CCS)
