-
Commentaries
What every intensivist should know about using high-flow nasal oxygen for critically ill patients
Rev Bras Ter Intensiva. 2017;29(4):399-403
Abstract
CommentariesWhat every intensivist should know about using high-flow nasal oxygen for critically ill patients
Rev Bras Ter Intensiva. 2017;29(4):399-403
DOI 10.5935/0103-507X.20170060
Views0Introduction The most conventional forms of oxygen delivery rely on facemasks, a nasal cannula or nasal prongs. However, the use of these methods is limited by certain drawbacks, including the need for a flow of oxygen higher than 15L/min in case of severe hypoxemia or the dilution of administered oxygen by entrained room air in […]See moreViews0

Abstract
CommentariesWhat every intensivist should know about using high-flow nasal oxygen for critically ill patients
Rev Bras Ter Intensiva. 2017;29(4):399-403
DOI 10.5935/0103-507X.20170060
Views0IntroductionThe most conventional forms of oxygen delivery rely on facemasks, a nasal cannula or nasal prongs. However, the use of these methods is limited by certain drawbacks, including the need for a flow of oxygen higher than 15L/min in case of severe hypoxemia or the dilution of administered oxygen by entrained room air in cases […]See more -
Commentaries
Intraoperative protective mechanical ventilation: what is new?
Rev Bras Ter Intensiva. 2017;29(4):404-407
Abstract
CommentariesIntraoperative protective mechanical ventilation: what is new?
Rev Bras Ter Intensiva. 2017;29(4):404-407
DOI 10.5935/0103-507X.20170065
Views0IntroductionPostoperative pulmonary complications are an important cause of hospital morbidity and mortality and are known to be associated with longer hospital stays and higher long-term mortality rates.() Thus, it is imperative to recognize early risk factors for the development of postoperative pulmonary complications (PPC) and to focus on the adoption of measures to prevent them […]See moreViews0Abstract
CommentariesIntraoperative protective mechanical ventilation: what is new?
Rev Bras Ter Intensiva. 2017;29(4):404-407
DOI 10.5935/0103-507X.20170065
Views0IntroductionPostoperative pulmonary complications are an important cause of hospital morbidity and mortality and are known to be associated with longer hospital stays and higher long-term mortality rates.() Thus, it is imperative to recognize early risk factors for the development of postoperative pulmonary complications (PPC) and to focus on the adoption of measures to prevent them […]See more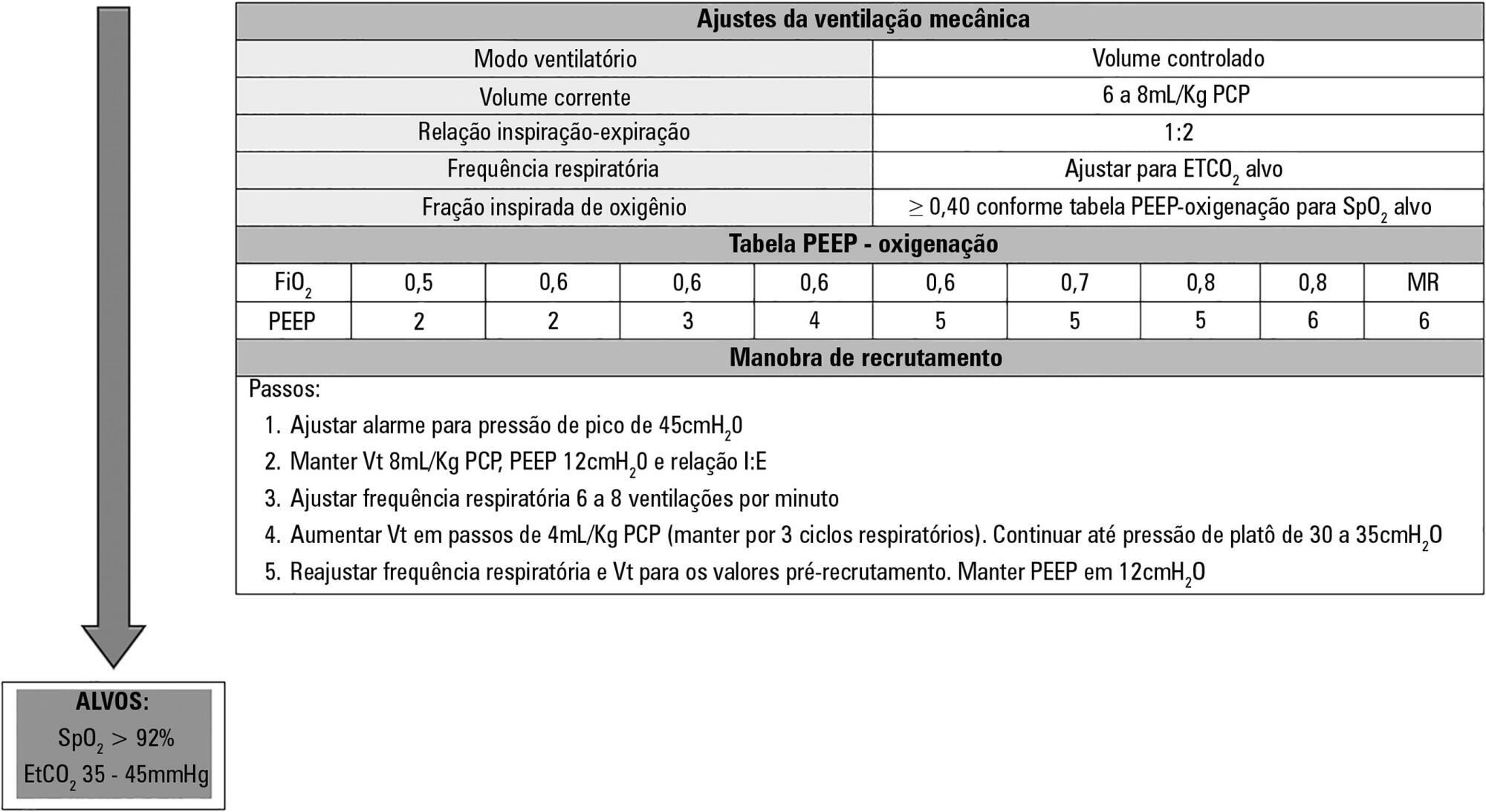
-
Commentaries
Neurally adjusted ventilatory assist in pediatrics: why, when, and how?
Rev Bras Ter Intensiva. 2017;29(4):408-413
Abstract
CommentariesNeurally adjusted ventilatory assist in pediatrics: why, when, and how?
Rev Bras Ter Intensiva. 2017;29(4):408-413
DOI 10.5935/0103-507X.20170064
Views0IntroductionIn pediatrics, good synchrony in controlled assisted ventilation is not always possible and may delay recovery, prolong mechanical ventilation (MV), and contribute to loss of muscle strength and increased calorie expenditure.()In controlled assisted ventilation, the trigger (drive) is a decisive factor in the release of the assisted cycle, as it is regulated by the pressure […]See moreViews0Abstract
CommentariesNeurally adjusted ventilatory assist in pediatrics: why, when, and how?
Rev Bras Ter Intensiva. 2017;29(4):408-413
DOI 10.5935/0103-507X.20170064
Views0IntroductionIn pediatrics, good synchrony in controlled assisted ventilation is not always possible and may delay recovery, prolong mechanical ventilation (MV), and contribute to loss of muscle strength and increased calorie expenditure.()In controlled assisted ventilation, the trigger (drive) is a decisive factor in the release of the assisted cycle, as it is regulated by the pressure […]See more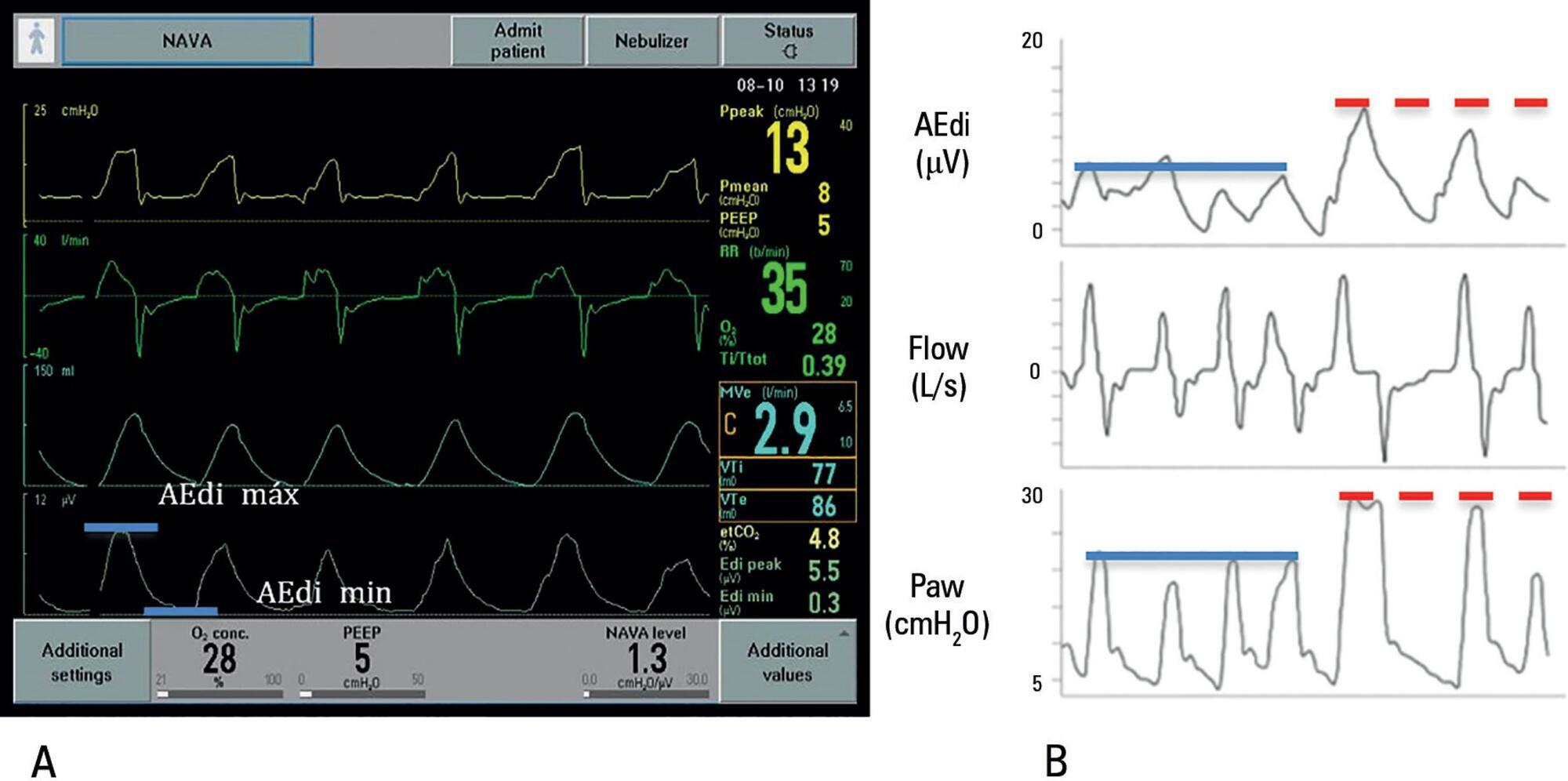
-
Commentaries
What every intensivist should know about intensive care unit admission criteria
Rev Bras Ter Intensiva. 2017;29(4):414-417
Abstract
CommentariesWhat every intensivist should know about intensive care unit admission criteria
Rev Bras Ter Intensiva. 2017;29(4):414-417
DOI 10.5935/0103-507X.20170073
Views0IntroductionThe Institute of Medicine (IOM) published a landmark report in 2001() recommending a thoughtful new health care delivery framework to improve the quality of care for the American population in the 21st century. The IOM defined six quality domains that should be at the foundation of how we deliver critical care services: safety, timeliness, efficacy, […]See moreViews0Abstract
CommentariesWhat every intensivist should know about intensive care unit admission criteria
Rev Bras Ter Intensiva. 2017;29(4):414-417
DOI 10.5935/0103-507X.20170073
Views0IntroductionThe Institute of Medicine (IOM) published a landmark report in 2001() recommending a thoughtful new health care delivery framework to improve the quality of care for the American population in the 21st century. The IOM defined six quality domains that should be at the foundation of how we deliver critical care services: safety, timeliness, efficacy, […]See more -
Original Articles
The Epimed Monitor ICU Database®: a cloud-based national registry for adult intensive care unit patients in Brazil
Rev Bras Ter Intensiva. 2017;29(4):418-426
Abstract
Original ArticlesThe Epimed Monitor ICU Database®: a cloud-based national registry for adult intensive care unit patients in Brazil
Rev Bras Ter Intensiva. 2017;29(4):418-426
DOI 10.5935/0103-507X.20170062
Views10See moreABSTRACT
Objective:
To describe the Epimed Monitor Database®, a Brazilian intensive care unit quality improvement database.
Methods:
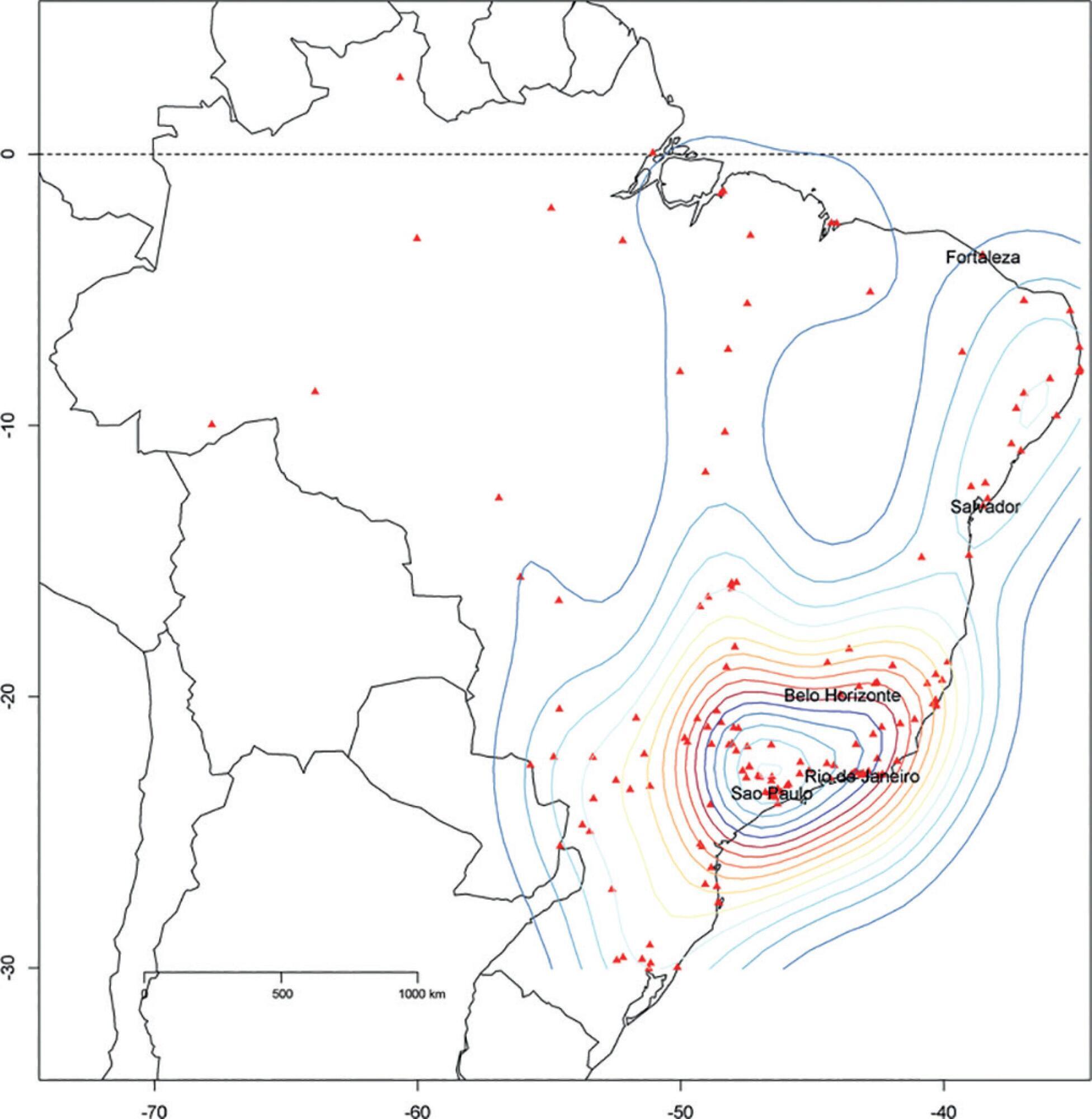
We described the Epimed Monitor® Database, including its structure and core data. We presented aggregated informative data from intensive care unit admissions from 2010 to 2016 using descriptive statistics. We also described the expansion and growth of the database along with the geographical distribution of participating units in Brazil.
Results:
The core data from the database includes demographic, administrative and physiological parameters, as well as specific report forms used to gather detailed data regarding the use of intensive care unit resources, infectious episodes, adverse events and checklists for adherence to best clinical practices. As of the end of 2016, 598 adult intensive care units in 318 hospitals totaling 8,160 intensive care unit beds were participating in the database. Most units were located at private hospitals in the southeastern region of the country. The number of yearly admissions rose during this period and included a predominance of medical admissions. The proportion of admissions due to cardiovascular disease declined, while admissions due to sepsis or infections became more common. Illness severity (Simplified Acute Physiology Score – SAPS 3 – 62 points), patient age (mean = 62 years) and hospital mortality (approximately 17%) remained reasonably stable during this time period.
Conclusion:
A large private database of critically ill patients is feasible and may provide relevant nationwide epidemiological data for quality improvement and benchmarking purposes among the participating intensive care units. This database is useful not only for administrative reasons but also for the improvement of daily care by facilitating the adoption of best practices and use for clinical research.
Views10Abstract
Original ArticlesThe Epimed Monitor ICU Database®: a cloud-based national registry for adult intensive care unit patients in Brazil
Rev Bras Ter Intensiva. 2017;29(4):418-426
DOI 10.5935/0103-507X.20170062
Views10See moreABSTRACT
Objective:
To describe the Epimed Monitor Database®, a Brazilian intensive care unit quality improvement database.
Methods:
We described the Epimed Monitor® Database, including its structure and core data. We presented aggregated informative data from intensive care unit admissions from 2010 to 2016 using descriptive statistics. We also described the expansion and growth of the database along with the geographical distribution of participating units in Brazil.
Results:
The core data from the database includes demographic, administrative and physiological parameters, as well as specific report forms used to gather detailed data regarding the use of intensive care unit resources, infectious episodes, adverse events and checklists for adherence to best clinical practices. As of the end of 2016, 598 adult intensive care units in 318 hospitals totaling 8,160 intensive care unit beds were participating in the database. Most units were located at private hospitals in the southeastern region of the country. The number of yearly admissions rose during this period and included a predominance of medical admissions. The proportion of admissions due to cardiovascular disease declined, while admissions due to sepsis or infections became more common. Illness severity (Simplified Acute Physiology Score – SAPS 3 – 62 points), patient age (mean = 62 years) and hospital mortality (approximately 17%) remained reasonably stable during this time period.
Conclusion:
A large private database of critically ill patients is feasible and may provide relevant nationwide epidemiological data for quality improvement and benchmarking purposes among the participating intensive care units. This database is useful not only for administrative reasons but also for the improvement of daily care by facilitating the adoption of best practices and use for clinical research.
-
Original Articles
Comparison between conventional protective mechanical ventilation and high-frequency oscillatory ventilation associated with the prone position
Rev Bras Ter Intensiva. 2017;29(4):427-435
Abstract
Original ArticlesComparison between conventional protective mechanical ventilation and high-frequency oscillatory ventilation associated with the prone position
Rev Bras Ter Intensiva. 2017;29(4):427-435
DOI 10.5935/0103-507X.20170067
Views0ABSTRACT
Objective:
To compare the effects of high-frequency oscillatory ventilation and conventional protective mechanical ventilation associated with the prone position on oxygenation, histology and pulmonary oxidative damage in an experimental model of acute lung injury.
Methods:
Forty-five rabbits with tracheostomy and vascular access were underwent mechanical ventilation. Acute lung injury was induced by tracheal infusion of warm saline. Three experimental groups were formed: healthy animals + conventional protective mechanical ventilation, supine position (Control Group; n = 15); animals with acute lung injury + conventional protective mechanical ventilation, prone position (CMVG; n = 15); and animals with acute lung injury + high-frequency oscillatory ventilation, prone position (HFOG; n = 15). Ten minutes after the beginning of the specific ventilation of each group, arterial gasometry was collected, with this timepoint being called time zero, after which the animal was placed in prone position and remained in this position for 4 hours. Oxidative stress was evaluated by the total antioxidant performance assay. Pulmonary tissue injury was determined by histopathological score. The level of significance was 5%.
Results:
Both groups with acute lung injury showed worsening of oxygenation after induction of injury compared with the Control Group. After 4 hours, there was a significant improvement in oxygenation in the HFOG group compared with CMVG. Analysis of total antioxidant performance in plasma showed greater protection in HFOG. HFOG had a lower histopathological lesion score in lung tissue than CMVG.
Conclusion:
High-frequency oscillatory ventilation, associated with prone position, improves oxygenation and attenuates oxidative damage and histopathological lung injury compared with conventional protective mechanical ventilation.
Keywords:Acute Lung Injuryacute respiratory distress syndromeHigh-frequency ventilationOxidative stressRabbitsRespiration, artificialSee moreViews0Abstract
Original ArticlesComparison between conventional protective mechanical ventilation and high-frequency oscillatory ventilation associated with the prone position
Rev Bras Ter Intensiva. 2017;29(4):427-435
DOI 10.5935/0103-507X.20170067
Views0ABSTRACT
Objective:
To compare the effects of high-frequency oscillatory ventilation and conventional protective mechanical ventilation associated with the prone position on oxygenation, histology and pulmonary oxidative damage in an experimental model of acute lung injury.
Methods:
Forty-five rabbits with tracheostomy and vascular access were underwent mechanical ventilation. Acute lung injury was induced by tracheal infusion of warm saline. Three experimental groups were formed: healthy animals + conventional protective mechanical ventilation, supine position (Control Group; n = 15); animals with acute lung injury + conventional protective mechanical ventilation, prone position (CMVG; n = 15); and animals with acute lung injury + high-frequency oscillatory ventilation, prone position (HFOG; n = 15). Ten minutes after the beginning of the specific ventilation of each group, arterial gasometry was collected, with this timepoint being called time zero, after which the animal was placed in prone position and remained in this position for 4 hours. Oxidative stress was evaluated by the total antioxidant performance assay. Pulmonary tissue injury was determined by histopathological score. The level of significance was 5%.
Results:
Both groups with acute lung injury showed worsening of oxygenation after induction of injury compared with the Control Group. After 4 hours, there was a significant improvement in oxygenation in the HFOG group compared with CMVG. Analysis of total antioxidant performance in plasma showed greater protection in HFOG. HFOG had a lower histopathological lesion score in lung tissue than CMVG.
Conclusion:
High-frequency oscillatory ventilation, associated with prone position, improves oxygenation and attenuates oxidative damage and histopathological lung injury compared with conventional protective mechanical ventilation.
Keywords:Acute Lung Injuryacute respiratory distress syndromeHigh-frequency ventilationOxidative stressRabbitsRespiration, artificialSee more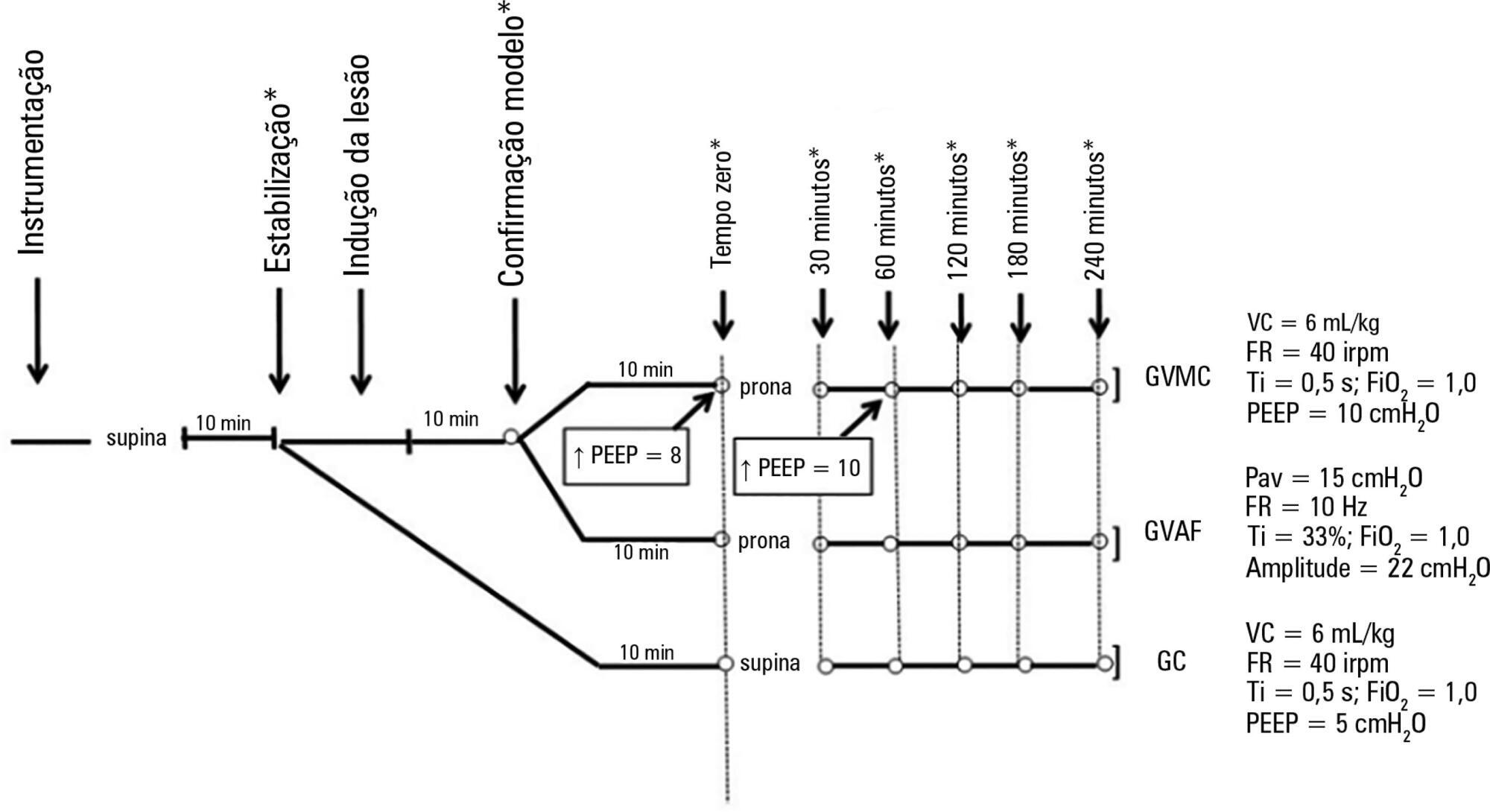
-
Original Articles
Prevalence of cytomegalovirus disease in kidney transplant patients in an intensive care unit
Rev Bras Ter Intensiva. 2017;29(4):436-443
Abstract
Original ArticlesPrevalence of cytomegalovirus disease in kidney transplant patients in an intensive care unit
Rev Bras Ter Intensiva. 2017;29(4):436-443
DOI 10.5935/0103-507X.20170070
Views0See moreABSTRACT
Objectives:
To define the frequency of cytomegalovirus disease among kidney transplant patients in an intensive care unit in which this complication was suspected and to identify predisposing factors and their possible impact on clinical outcome.
Methods:
Retrospective observational study in which kidney transplant patients over the age of 18 years were hospitalized for any reason in an intensive care unit with at least one collection of samples to test for the presence of antigenemia or cytomegalovirus via polymerase chain reaction during hospitalization. Cytomegalovirus disease was defined as positive antigenemia or polymerase chain reaction above 500 copies/mL in the presence of symptoms and in the appropriate clinical setting, as judged by the attending physician.
Results:
A total of 99 patients were included (age: 53.4 ± 12.8 years, 71.6% male). Cytomegalovirus disease was diagnosed in 39 patients (39.4%). Respiratory symptoms (51%), non-specific clinical worsening (20%) or gastrointestinal symptoms (14%) were the main reasons for exam collection. Transplant time was lower in those with cytomegalovirus disease than in those without this diagnosis (6.5 months and 31.2 months, p = 0.001), along with pulse therapy in the last 6 months (41% and 16.9%, p = 0.008) and previous use of thymoglobulin in the last year (35.9% and 6.8%, p < 0.001). In the logistic regression model, only the transplant time and the use of thymoglobulin were associated with a higher frequency of cytomegalovirus. There was no difference in clinical evolution between patients with and without cytomegalovirus disease.
Conclusion:
In kidney transplant patients suspected of cytomegalovirus disease, the prevalence was high. Transplant time less than 6 months, and the use of thymoglobulin in the last year should increase the intensivist’s suspicion for this complication.
Views0Abstract
Original ArticlesPrevalence of cytomegalovirus disease in kidney transplant patients in an intensive care unit
Rev Bras Ter Intensiva. 2017;29(4):436-443
DOI 10.5935/0103-507X.20170070
Views0See moreABSTRACT
Objectives:
To define the frequency of cytomegalovirus disease among kidney transplant patients in an intensive care unit in which this complication was suspected and to identify predisposing factors and their possible impact on clinical outcome.
Methods:
Retrospective observational study in which kidney transplant patients over the age of 18 years were hospitalized for any reason in an intensive care unit with at least one collection of samples to test for the presence of antigenemia or cytomegalovirus via polymerase chain reaction during hospitalization. Cytomegalovirus disease was defined as positive antigenemia or polymerase chain reaction above 500 copies/mL in the presence of symptoms and in the appropriate clinical setting, as judged by the attending physician.
Results:
A total of 99 patients were included (age: 53.4 ± 12.8 years, 71.6% male). Cytomegalovirus disease was diagnosed in 39 patients (39.4%). Respiratory symptoms (51%), non-specific clinical worsening (20%) or gastrointestinal symptoms (14%) were the main reasons for exam collection. Transplant time was lower in those with cytomegalovirus disease than in those without this diagnosis (6.5 months and 31.2 months, p = 0.001), along with pulse therapy in the last 6 months (41% and 16.9%, p = 0.008) and previous use of thymoglobulin in the last year (35.9% and 6.8%, p < 0.001). In the logistic regression model, only the transplant time and the use of thymoglobulin were associated with a higher frequency of cytomegalovirus. There was no difference in clinical evolution between patients with and without cytomegalovirus disease.
Conclusion:
In kidney transplant patients suspected of cytomegalovirus disease, the prevalence was high. Transplant time less than 6 months, and the use of thymoglobulin in the last year should increase the intensivist’s suspicion for this complication.
-
Original Articles
Epidemiology of acute kidney injury and chronic kidney disease in the intensive care unit
Rev Bras Ter Intensiva. 2017;29(4):444-452
Abstract
Original ArticlesEpidemiology of acute kidney injury and chronic kidney disease in the intensive care unit
Rev Bras Ter Intensiva. 2017;29(4):444-452
DOI 10.5935/0103-507X.20170061
Views0See moreABSTRACT
Objective:
To describe the epidemiology of acute kidney injury, its relationship to chronic kidney disease, and the factors associated with its incidence.
Methods:
A cohort study and follow-up were conducted in an intensive care unit in Montevideo, Uruguay. We included patients admitted between November 2014 and October 2015 who were older than 15 years of age and who had at least two measurements of serum creatinine. We excluded patients who were hospitalized for less than 48 hours, patients who died at the time of hospitalization, and patients with chronic renal disease who were on hemodialysis or peritoneal dialysis. There were no interventions. Acute kidney injury was defined according to the criteria set forth in Acute Kidney Injury Disease: Improving Global Outcomes, and chronic kidney disease was defined according to the Chronic Kidney Disease Work Group.
Results:
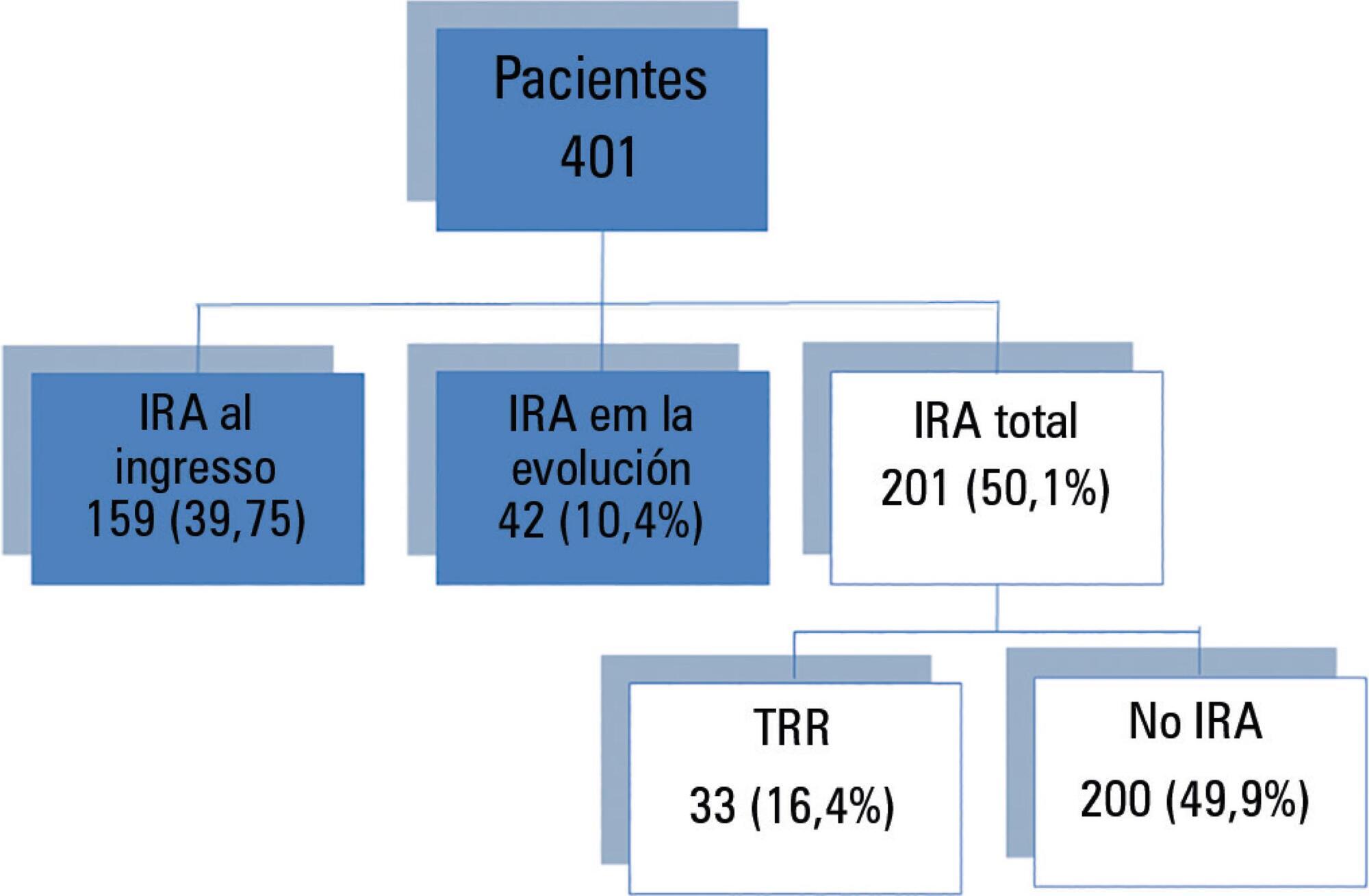
We included 401 patients, 56.6% male, median age of 68 years (interquartile range (IQR) 51-79 years). The diagnosis at admission was severe sepsis 36.3%, neurocritical 16.3%, polytrauma 15.2%, and other 32.2%. The incidence of acute kidney injury was 50.1%, and 14.1% of the patients suffered from chronic kidney disease. The incidence of acute septic kidney injury was 75.3%. Mortality in patients with or without acute kidney injury was 41.8% and 14%, respectively (p < 0.001). In the multivariate analysis, the most significant variables for acute kidney injury were chronic kidney disease (odds ratio (OR) 5.39, 95%CI 2.04 - 14.29, p = 0.001), shock (OR 3.94, 95%CI 1.72 - 9.07, p = 0.001), and severe sepsis (OR 7.79, 95%CI 2.02 - 29.97, p = 0.003).
Conclusion:
The incidence of acute kidney injury is high mainly in septic patients. Chronic kidney disease was independently associated with the development of acute kidney injury.
Views0Abstract
Original ArticlesEpidemiology of acute kidney injury and chronic kidney disease in the intensive care unit
Rev Bras Ter Intensiva. 2017;29(4):444-452
DOI 10.5935/0103-507X.20170061
Views0See moreABSTRACT
Objective:
To describe the epidemiology of acute kidney injury, its relationship to chronic kidney disease, and the factors associated with its incidence.
Methods:
A cohort study and follow-up were conducted in an intensive care unit in Montevideo, Uruguay. We included patients admitted between November 2014 and October 2015 who were older than 15 years of age and who had at least two measurements of serum creatinine. We excluded patients who were hospitalized for less than 48 hours, patients who died at the time of hospitalization, and patients with chronic renal disease who were on hemodialysis or peritoneal dialysis. There were no interventions. Acute kidney injury was defined according to the criteria set forth in Acute Kidney Injury Disease: Improving Global Outcomes, and chronic kidney disease was defined according to the Chronic Kidney Disease Work Group.
Results:
We included 401 patients, 56.6% male, median age of 68 years (interquartile range (IQR) 51-79 years). The diagnosis at admission was severe sepsis 36.3%, neurocritical 16.3%, polytrauma 15.2%, and other 32.2%. The incidence of acute kidney injury was 50.1%, and 14.1% of the patients suffered from chronic kidney disease. The incidence of acute septic kidney injury was 75.3%. Mortality in patients with or without acute kidney injury was 41.8% and 14%, respectively (p < 0.001). In the multivariate analysis, the most significant variables for acute kidney injury were chronic kidney disease (odds ratio (OR) 5.39, 95%CI 2.04 - 14.29, p = 0.001), shock (OR 3.94, 95%CI 1.72 - 9.07, p = 0.001), and severe sepsis (OR 7.79, 95%CI 2.02 - 29.97, p = 0.003).
Conclusion:
The incidence of acute kidney injury is high mainly in septic patients. Chronic kidney disease was independently associated with the development of acute kidney injury.
-
Original Articles
Assessment of PIM-2 performance among surgical patients with heart disease and correlation of results with RACHS-1
Rev Bras Ter Intensiva. 2017;29(4):453-459
Abstract
Original ArticlesAssessment of PIM-2 performance among surgical patients with heart disease and correlation of results with RACHS-1
Rev Bras Ter Intensiva. 2017;29(4):453-459
DOI 10.5935/0103-507X.20170069
Views0ABSTRACT
Objective:
To assess the performance of the Pediatric Index of Mortality (PIM) 2 and the Risk Adjustment for Congenital Heart Surgery (RACHS) in the postoperative period of congenital heart disease patients.
Methods:
Retrospective cross-sectional study. Data were collected from patient records to generate the scores and predictions using recommended techniques, demographic data and outcomes. The Mann-Whitney test, Hosmer-Lemeshow test, standardized mortality rate, area under the receiver operating characteristic (ROC) curve, chi square test, Poisson regression with robust variance and Spearman’s test were used for statistical analysis.
Results:
A total of 263 patients were evaluated, and 72 died (27.4%). These patients presented significantly higher PIM-2 values than survivors (p < 0.001). In the RACHS-1 classification, mortality was progressively higher according to the complexity of the procedure, with a 3.24-fold increase in the comparison between groups 6 and 2. The area under the ROC curve for PIM-2 was 0.81 (95%CI 0.75 - 0.87), while for RACHS-1, it was 0.70 (95%CI 0.63 - 0.77). The RACHS presented better calibration power in the sample analyzed. A significantly positive correlation was found between the results of both scores (rs = 0.532; p < 0.001).
Conclusion:
RACHS presented good calibration power, and RACHS-1 and PIM-2 demonstrated good performance with regard to their discriminating capacities between survivors and non-survivors. Moreover, a positive correlation was found between the results of the two risk scores.
Keywords:Heart defects, congenital/mortalityHeart defects, congenital/surgeryPostoperative periodRisk adjustmentRisk assessmentSee moreViews0Abstract
Original ArticlesAssessment of PIM-2 performance among surgical patients with heart disease and correlation of results with RACHS-1
Rev Bras Ter Intensiva. 2017;29(4):453-459
DOI 10.5935/0103-507X.20170069
Views0ABSTRACT
Objective:
To assess the performance of the Pediatric Index of Mortality (PIM) 2 and the Risk Adjustment for Congenital Heart Surgery (RACHS) in the postoperative period of congenital heart disease patients.
Methods:
Retrospective cross-sectional study. Data were collected from patient records to generate the scores and predictions using recommended techniques, demographic data and outcomes. The Mann-Whitney test, Hosmer-Lemeshow test, standardized mortality rate, area under the receiver operating characteristic (ROC) curve, chi square test, Poisson regression with robust variance and Spearman’s test were used for statistical analysis.
Results:
A total of 263 patients were evaluated, and 72 died (27.4%). These patients presented significantly higher PIM-2 values than survivors (p < 0.001). In the RACHS-1 classification, mortality was progressively higher according to the complexity of the procedure, with a 3.24-fold increase in the comparison between groups 6 and 2. The area under the ROC curve for PIM-2 was 0.81 (95%CI 0.75 - 0.87), while for RACHS-1, it was 0.70 (95%CI 0.63 - 0.77). The RACHS presented better calibration power in the sample analyzed. A significantly positive correlation was found between the results of both scores (rs = 0.532; p < 0.001).
Conclusion:
RACHS presented good calibration power, and RACHS-1 and PIM-2 demonstrated good performance with regard to their discriminating capacities between survivors and non-survivors. Moreover, a positive correlation was found between the results of the two risk scores.
Keywords:Heart defects, congenital/mortalityHeart defects, congenital/surgeryPostoperative periodRisk adjustmentRisk assessmentSee more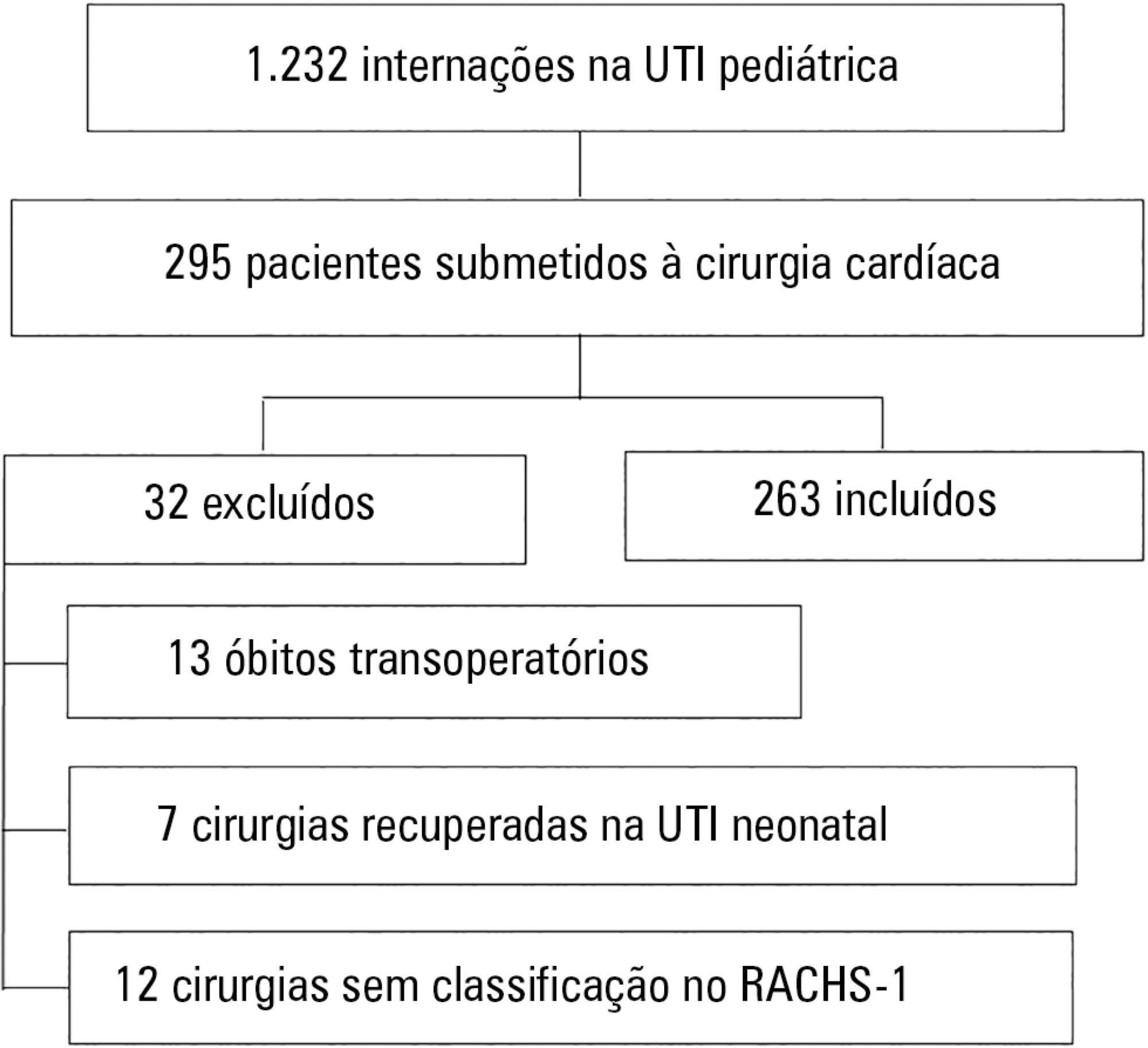
-
Original Articles
Functional evaluation of pediatric patients after discharge from the intensive care unit using the Functional Status Scale
Rev Bras Ter Intensiva. 2017;29(4):460-465
Abstract
Original ArticlesFunctional evaluation of pediatric patients after discharge from the intensive care unit using the Functional Status Scale
Rev Bras Ter Intensiva. 2017;29(4):460-465
DOI 10.5935/0103-507X.20170066
Views0See moreABSTRACT
Objective:
To evaluate the functional status of pediatric patients after discharge from the pediatric intensive care unit using the Functional Status Scale and to compare the time of invasive mechanical ventilation, length of stay in the pediatric intensive care unit, and Pediatric Index of Mortality 2 results among individuals with different degrees of functional impairment.
Methods:
A cross-sectional study was conducted on patients who were discharged from a pediatric intensive care unit. The functional evaluation by the Functional Status Scale was performed on the first day after discharge from the unit, and the Pediatric Index of Mortality 2 was used to predict the mortality rate at the time of admission to the pediatric intensive care unit.
Results:
The sample consisted of 50 individuals, 60% of which were male, with a median age of 19 [6 – 61] months. The overall score of the Functional Status Scale was 11.5 [7 – 15], and the highest scores were observed in the “motor function” 3 [1 – 4] and “feeding” 4 [1 – 4] domains. Compared to patients who were not readmitted to the pediatric intensive care unit, patients who were readmitted presented a worse overall score (p = 0.01), worse scores in the “motor function” (p = 0.01), “feeding” (p = 0.02), and “respiratory” (p = 0.036) domains, and a higher mortality rate according to the Pediatric Index of Mortality 2 (p = 0.025).
Conclusion:
Evaluation of the functional status using the Functional Status Scale indicated moderate impairment in patients after discharge from the pediatric intensive care unit, mainly in the “motor function” and “feeding” domains; patients who were readmitted to the pediatric intensive care unit demonstrated worse overall functional, motor function, feeding and respiratory scores. Individuals with greater functional impairment had longer times of invasive mechanical ventilation and hospitalization in the pediatric intensive care unit.
Views0Abstract
Original ArticlesFunctional evaluation of pediatric patients after discharge from the intensive care unit using the Functional Status Scale
Rev Bras Ter Intensiva. 2017;29(4):460-465
DOI 10.5935/0103-507X.20170066
Views0See moreABSTRACT
Objective:
To evaluate the functional status of pediatric patients after discharge from the pediatric intensive care unit using the Functional Status Scale and to compare the time of invasive mechanical ventilation, length of stay in the pediatric intensive care unit, and Pediatric Index of Mortality 2 results among individuals with different degrees of functional impairment.
Methods:
A cross-sectional study was conducted on patients who were discharged from a pediatric intensive care unit. The functional evaluation by the Functional Status Scale was performed on the first day after discharge from the unit, and the Pediatric Index of Mortality 2 was used to predict the mortality rate at the time of admission to the pediatric intensive care unit.
Results:
The sample consisted of 50 individuals, 60% of which were male, with a median age of 19 [6 – 61] months. The overall score of the Functional Status Scale was 11.5 [7 – 15], and the highest scores were observed in the “motor function” 3 [1 – 4] and “feeding” 4 [1 – 4] domains. Compared to patients who were not readmitted to the pediatric intensive care unit, patients who were readmitted presented a worse overall score (p = 0.01), worse scores in the “motor function” (p = 0.01), “feeding” (p = 0.02), and “respiratory” (p = 0.036) domains, and a higher mortality rate according to the Pediatric Index of Mortality 2 (p = 0.025).
Conclusion:
Evaluation of the functional status using the Functional Status Scale indicated moderate impairment in patients after discharge from the pediatric intensive care unit, mainly in the “motor function” and “feeding” domains; patients who were readmitted to the pediatric intensive care unit demonstrated worse overall functional, motor function, feeding and respiratory scores. Individuals with greater functional impairment had longer times of invasive mechanical ventilation and hospitalization in the pediatric intensive care unit.
-
Original Articles
Weakness acquired in the intensive care unit. Incidence, risk factors and their association with inspiratory weakness. Observational cohort study
Rev Bras Ter Intensiva. 2017;29(4):466-475
Abstract
Original ArticlesWeakness acquired in the intensive care unit. Incidence, risk factors and their association with inspiratory weakness. Observational cohort study
Rev Bras Ter Intensiva. 2017;29(4):466-475
DOI 10.5935/0103-507X.20170063
Views0See moreABSTRACT
Objective:
This paper sought to determine the accumulated incidence and analyze the risk factors associated with the development of weakness acquired in the intensive care unit and its relationship to inspiratory weakness.
Methods:
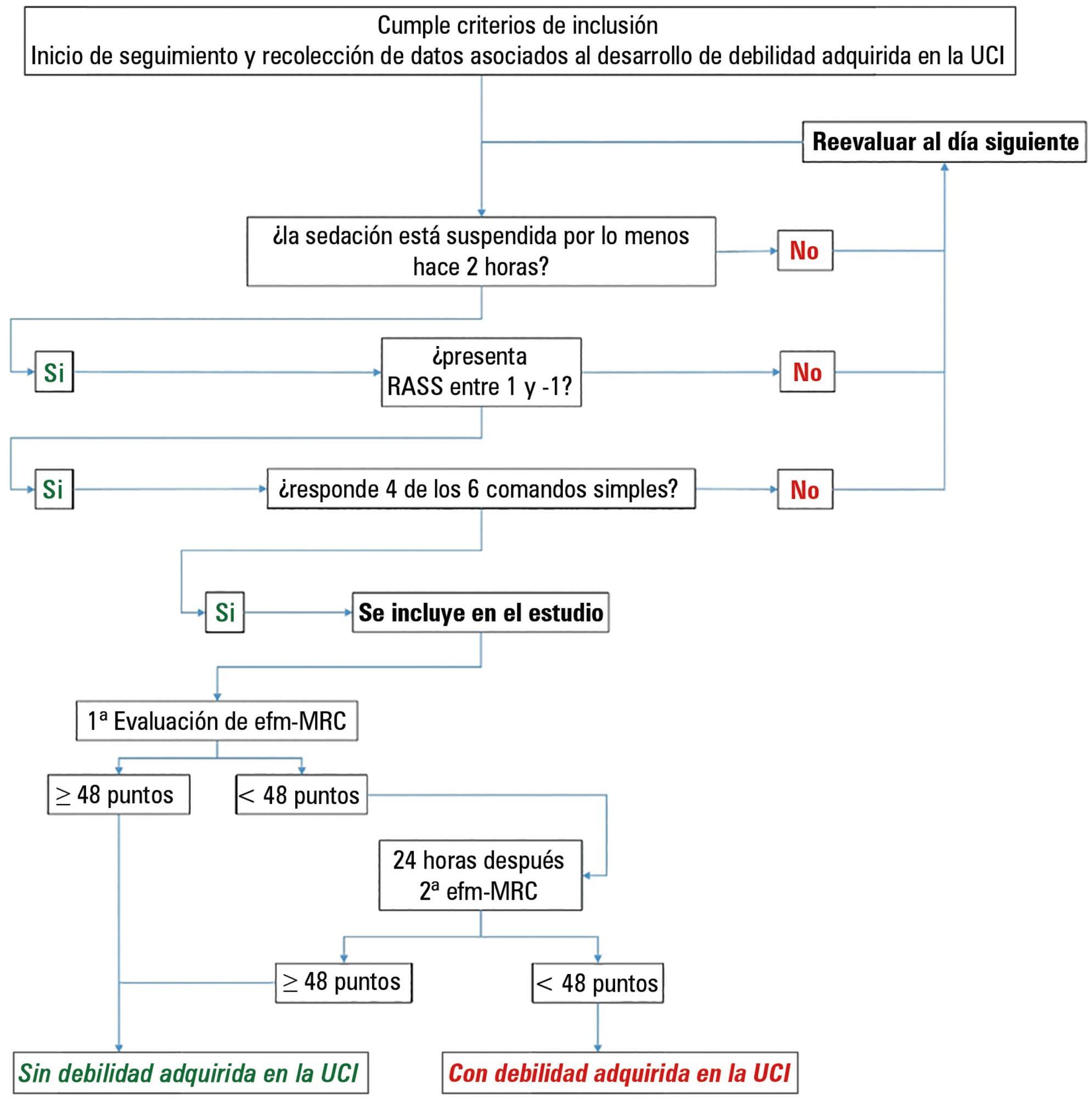
We conducted a prospective cohort study at a single center, multipurpose medical-surgical intensive care unit. We included adult patients who required mechanical ventilation ≥ 24 hours between July 2014 and January 2016. No interventions were performed. Demographic data, clinical diagnoses, the factors related to the development of intensive care unit -acquired weakness, and maximal inspiratory pressure were recorded.
Results:
Of the 111 patients included, 66 developed intensive care unit -acquired weakness, with a cumulative incidence of 40.5% over 18 months. The group with intensive care unit-acquired weakness were older (55.9 ± 17.6 versus 45.8 ± 16.7), required more mechanical ventilation (7 [4 – 10] days versus 4 [2 – 7.3] days), and spent more time in the intensive care unit (15.5 [9.2 – 22.8] days versus 9 [6 – 14] days). More patients presented with delirium (68% versus 39%), hyperglycemia > 3 days (84% versus 59%), and positive balance > 3 days (73.3% versus 37%). All comparisons were significant at p < 0.05. A multiple logistic regression identified age, hyperglycemia ≥ 3 days, delirium, and mechanical ventilation > 5 days as independent predictors of intensive care unit-acquired weakness. Low maximal inspiratory pressure was associated with intensive care unit-acquired weakness (p < 0.001), and the maximum inspiratory pressure cut-off value of < 36cmH2O had sensitivity and specificity values of 31.8% and 95.5%, respectively, when classifying patients with intensive care unit-acquired weakness.
Conclusion:
The intensive care unit acquired weakness is a condition with a high incidence in our environment. The development of intensive care unit-acquired weakness was associated with age, delirium, hyperglycemia, and mechanical ventilation > 5 days. The maximum inspiratory pressure value of ≥ 36cmH2O was associated with a high diagnostic value to exclude the presence of intensive care unit -acquired weakness.
Views0Abstract
Original ArticlesWeakness acquired in the intensive care unit. Incidence, risk factors and their association with inspiratory weakness. Observational cohort study
Rev Bras Ter Intensiva. 2017;29(4):466-475
DOI 10.5935/0103-507X.20170063
Views0See moreABSTRACT
Objective:
This paper sought to determine the accumulated incidence and analyze the risk factors associated with the development of weakness acquired in the intensive care unit and its relationship to inspiratory weakness.
Methods:
We conducted a prospective cohort study at a single center, multipurpose medical-surgical intensive care unit. We included adult patients who required mechanical ventilation ≥ 24 hours between July 2014 and January 2016. No interventions were performed. Demographic data, clinical diagnoses, the factors related to the development of intensive care unit -acquired weakness, and maximal inspiratory pressure were recorded.
Results:
Of the 111 patients included, 66 developed intensive care unit -acquired weakness, with a cumulative incidence of 40.5% over 18 months. The group with intensive care unit-acquired weakness were older (55.9 ± 17.6 versus 45.8 ± 16.7), required more mechanical ventilation (7 [4 – 10] days versus 4 [2 – 7.3] days), and spent more time in the intensive care unit (15.5 [9.2 – 22.8] days versus 9 [6 – 14] days). More patients presented with delirium (68% versus 39%), hyperglycemia > 3 days (84% versus 59%), and positive balance > 3 days (73.3% versus 37%). All comparisons were significant at p < 0.05. A multiple logistic regression identified age, hyperglycemia ≥ 3 days, delirium, and mechanical ventilation > 5 days as independent predictors of intensive care unit-acquired weakness. Low maximal inspiratory pressure was associated with intensive care unit-acquired weakness (p < 0.001), and the maximum inspiratory pressure cut-off value of < 36cmH2O had sensitivity and specificity values of 31.8% and 95.5%, respectively, when classifying patients with intensive care unit-acquired weakness.
Conclusion:
The intensive care unit acquired weakness is a condition with a high incidence in our environment. The development of intensive care unit-acquired weakness was associated with age, delirium, hyperglycemia, and mechanical ventilation > 5 days. The maximum inspiratory pressure value of ≥ 36cmH2O was associated with a high diagnostic value to exclude the presence of intensive care unit -acquired weakness.
-
Original Articles
Bedside ultrasound is a practical measurement tool for assessing muscle mass
Rev Bras Ter Intensiva. 2017;29(4):476-480
Abstract
Original ArticlesBedside ultrasound is a practical measurement tool for assessing muscle mass
Rev Bras Ter Intensiva. 2017;29(4):476-480
DOI 10.5935/0103-507X.20170071
Views1ABSTRACT
Objective:
To evaluate the intra- and inter-reliability and the ease of measuring the quadriceps muscle thickness using bedside ultrasound.
Methods:
This is a prospective, observational study. The assessment of quadriceps muscle thickness was performed at two reference points and was quantified using portable B-mode ultrasound in two healthy volunteers. For standardization of measurements and validation of image collections, the team was trained through theoretical and practical classes, with a 6-hour workload.
Results:
A total of 112 images were examined by the coach and compared with the trainees. Pearson’s correlation analysis found an excellent relationship between the coach and all trainees (R2 > 0.90). The best association was between the coach and the dietitians (R2: 0.99; p < 0.001), and the worst association was between the coach and the medical trainees (R2: 0.92; p < 0.001). In the Bland-Altman comparison, the highest error rate found between coach and trainees was 5.12% (95% confidence interval [CI] 3.64-12.37), and the lowest was 1.01% (95%CI 0.72 - 2.58); the highest bias of the values described was -0.12 ± 0.19, and the lowest was -0.01 ± 0.04.
Conclusion:
The data analyzed showed a good correlation between the measurements made by the coach and trainees, indicating that ultrasound of the quadriceps muscle is a viable and easily applicable tool.
Keywords:Body compositionEvaluationIntensive care unitsPoint-of-care testingQuadriceps muscle/diagnostic imagingUltrasonographySee moreViews1Abstract
Original ArticlesBedside ultrasound is a practical measurement tool for assessing muscle mass
Rev Bras Ter Intensiva. 2017;29(4):476-480
DOI 10.5935/0103-507X.20170071
Views1ABSTRACT
Objective:
To evaluate the intra- and inter-reliability and the ease of measuring the quadriceps muscle thickness using bedside ultrasound.
Methods:
This is a prospective, observational study. The assessment of quadriceps muscle thickness was performed at two reference points and was quantified using portable B-mode ultrasound in two healthy volunteers. For standardization of measurements and validation of image collections, the team was trained through theoretical and practical classes, with a 6-hour workload.
Results:
A total of 112 images were examined by the coach and compared with the trainees. Pearson’s correlation analysis found an excellent relationship between the coach and all trainees (R2 > 0.90). The best association was between the coach and the dietitians (R2: 0.99; p < 0.001), and the worst association was between the coach and the medical trainees (R2: 0.92; p < 0.001). In the Bland-Altman comparison, the highest error rate found between coach and trainees was 5.12% (95% confidence interval [CI] 3.64-12.37), and the lowest was 1.01% (95%CI 0.72 - 2.58); the highest bias of the values described was -0.12 ± 0.19, and the lowest was -0.01 ± 0.04.
Conclusion:
The data analyzed showed a good correlation between the measurements made by the coach and trainees, indicating that ultrasound of the quadriceps muscle is a viable and easily applicable tool.
Keywords:Body compositionEvaluationIntensive care unitsPoint-of-care testingQuadriceps muscle/diagnostic imagingUltrasonographySee more
-
Review Articles
Autonomic nervous system monitoring in intensive care as a prognostic tool. Systematic review
Rev Bras Ter Intensiva. 2017;29(4):481-489
Abstract
Review ArticlesAutonomic nervous system monitoring in intensive care as a prognostic tool. Systematic review
Rev Bras Ter Intensiva. 2017;29(4):481-489
DOI 10.5935/0103-507X.20170072
Views0See moreABSTRACT
Objective:
To present a systematic review of the use of autonomic nervous system monitoring as a prognostic tool in intensive care units by assessing heart rate variability.
Methods:
Literature review of studies published until July 2016 listed in PubMed/Medline and conducted in intensive care units, on autonomic nervous system monitoring, via analysis of heart rate variability as a prognostic tool (mortality study). The following English terms were entered in the search field: (“autonomic nervous system” OR “heart rate variability”) AND (“intensive care” OR “critical care” OR “emergency care” OR “ICU”) AND (“prognosis” OR “prognoses” OR “mortality”).
Results:
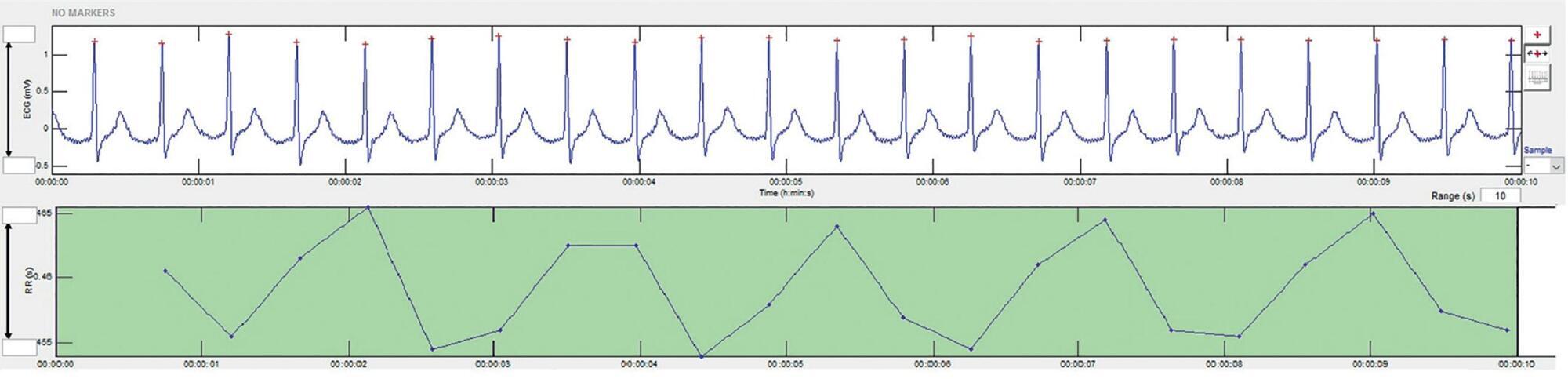
There was an increased likelihood of death in patients who had a decrease in heart rate variability as analyzed via heart rate variance, cardiac uncoupling, heart rate volatility, integer heart rate variability, standard deviation of NN intervals, root mean square of successive differences, total power, low frequency, very low frequency, low frequency/high frequency ratio, ratio of short-term to long-term fractal exponents, Shannon entropy, multiscale entropy and approximate entropy.
Conclusion:
In patients admitted to intensive care units, regardless of the pathology, heart rate variability varies inversely with clinical severity and prognosis.
Views0Abstract
Review ArticlesAutonomic nervous system monitoring in intensive care as a prognostic tool. Systematic review
Rev Bras Ter Intensiva. 2017;29(4):481-489
DOI 10.5935/0103-507X.20170072
Views0See moreABSTRACT
Objective:
To present a systematic review of the use of autonomic nervous system monitoring as a prognostic tool in intensive care units by assessing heart rate variability.
Methods:
Literature review of studies published until July 2016 listed in PubMed/Medline and conducted in intensive care units, on autonomic nervous system monitoring, via analysis of heart rate variability as a prognostic tool (mortality study). The following English terms were entered in the search field: (“autonomic nervous system” OR “heart rate variability”) AND (“intensive care” OR “critical care” OR “emergency care” OR “ICU”) AND (“prognosis” OR “prognoses” OR “mortality”).
Results:
There was an increased likelihood of death in patients who had a decrease in heart rate variability as analyzed via heart rate variance, cardiac uncoupling, heart rate volatility, integer heart rate variability, standard deviation of NN intervals, root mean square of successive differences, total power, low frequency, very low frequency, low frequency/high frequency ratio, ratio of short-term to long-term fractal exponents, Shannon entropy, multiscale entropy and approximate entropy.
Conclusion:
In patients admitted to intensive care units, regardless of the pathology, heart rate variability varies inversely with clinical severity and prognosis.
-
Review Articles
The spectrum of cardiovascular effects of dobutamine – from healthy subjects to septic shock patients
Rev Bras Ter Intensiva. 2017;29(4):490-498
Abstract
Review ArticlesThe spectrum of cardiovascular effects of dobutamine – from healthy subjects to septic shock patients
Rev Bras Ter Intensiva. 2017;29(4):490-498
DOI 10.5935/0103-507X.20170068
Views0See moreABSTRACT
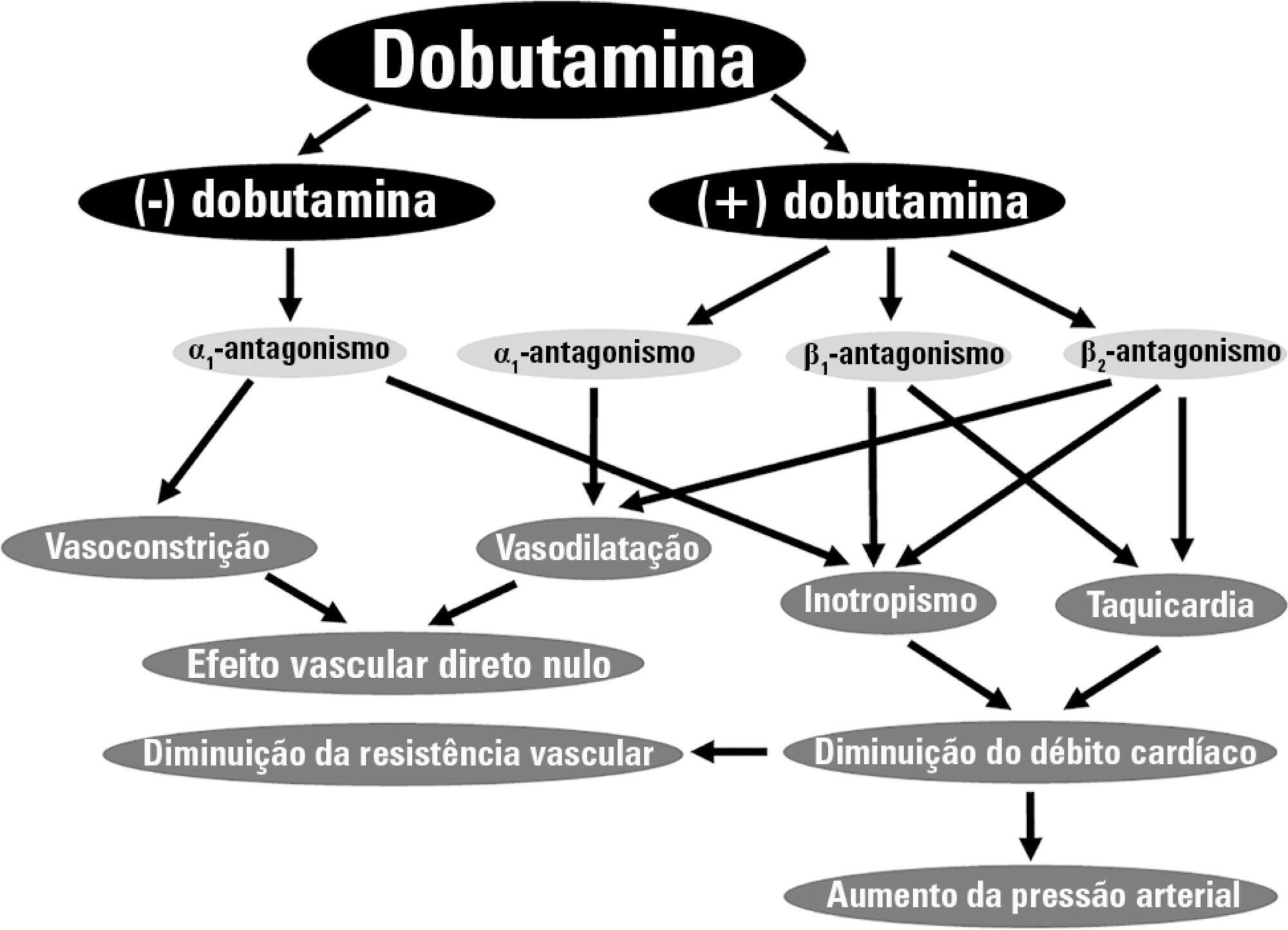
Dobutamine is the inotrope most commonly used in septic shock patients to increase cardiac output and correct hypoperfusion. Although some experimental and clinical studies have shown that dobutamine can improve systemic and regional hemodynamics, other research has found that its effects are heterogenous and unpredictable. In this review, we analyze the pharmacodynamic properties of dobutamine and its physiologic effects. Our goal is to show that the effects of dobutamine might differ between healthy subjects, in experimental and clinical cardiac failure, in animal models and in patients with septic shock. We discuss evidence supporting the claim that dobutamine, in septic shock, frequently behaves as a chronotropic and vasodilatory drug, without evidence of inotropic action. Since the side effects are very common, and the therapeutic benefits are unclear, we suggest that dobutamine should be used cautiously in septic shock. Before a definitive therapeutic decision, the efficacy and tolerance of dobutamine should be assessed during a brief time with close monitoring of its positive and negative side effects.
Views0Abstract
Review ArticlesThe spectrum of cardiovascular effects of dobutamine – from healthy subjects to septic shock patients
Rev Bras Ter Intensiva. 2017;29(4):490-498
DOI 10.5935/0103-507X.20170068
Views0See moreABSTRACT
Dobutamine is the inotrope most commonly used in septic shock patients to increase cardiac output and correct hypoperfusion. Although some experimental and clinical studies have shown that dobutamine can improve systemic and regional hemodynamics, other research has found that its effects are heterogenous and unpredictable. In this review, we analyze the pharmacodynamic properties of dobutamine and its physiologic effects. Our goal is to show that the effects of dobutamine might differ between healthy subjects, in experimental and clinical cardiac failure, in animal models and in patients with septic shock. We discuss evidence supporting the claim that dobutamine, in septic shock, frequently behaves as a chronotropic and vasodilatory drug, without evidence of inotropic action. Since the side effects are very common, and the therapeutic benefits are unclear, we suggest that dobutamine should be used cautiously in septic shock. Before a definitive therapeutic decision, the efficacy and tolerance of dobutamine should be assessed during a brief time with close monitoring of its positive and negative side effects.
-
Review Articles
Toxic epidermal necrolysis: a paradigm of critical illness
Rev Bras Ter Intensiva. 2017;29(4):499-508
Abstract
Review ArticlesToxic epidermal necrolysis: a paradigm of critical illness
Rev Bras Ter Intensiva. 2017;29(4):499-508
DOI 10.5935/0103-507X.20170075
Views0See moreABSTRACT
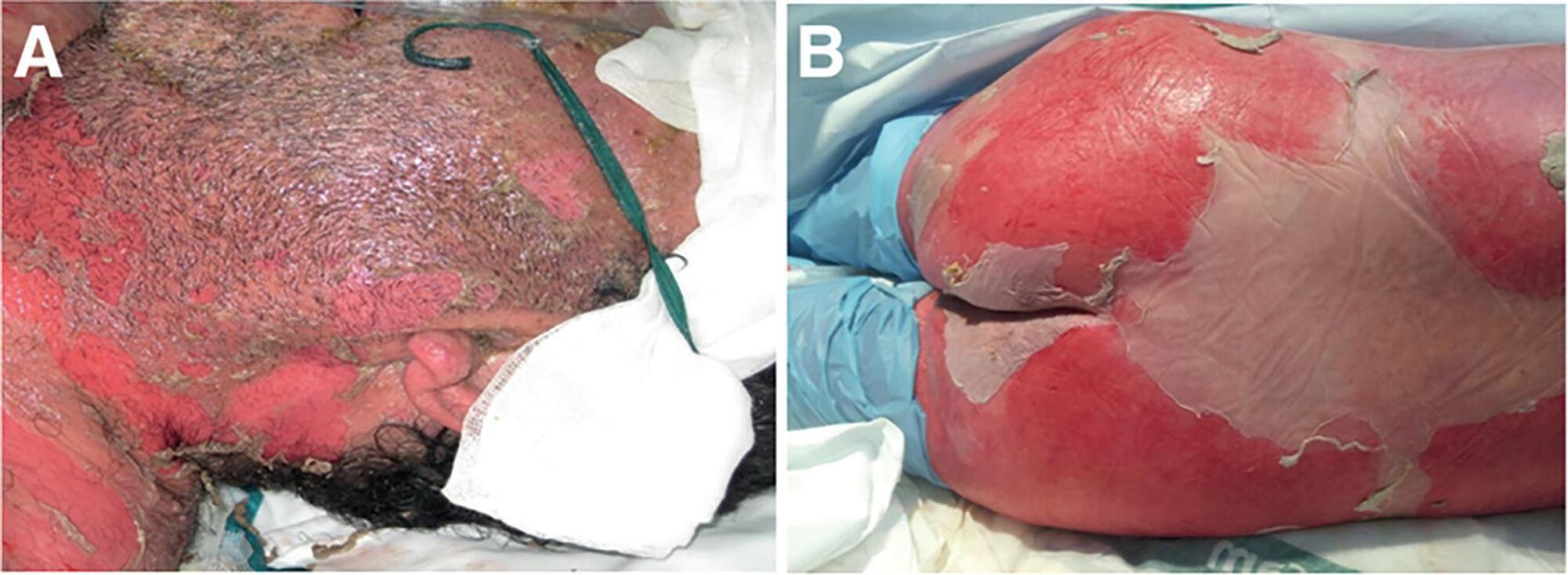
Toxic epidermal necrolysis is an adverse immunological skin reaction secondary in most cases to the administration of a drug. Toxic epidermal necrolysis, Stevens-Johnson syndrome, and multiform exudative erythema are part of the same disease spectrum. The mortality rate from toxic epidermal necrolysis is approximately 30%. The pathophysiology of toxic epidermal necrolysis is similar in many respects to that of superficial skin burns. Mucosal involvement of the ocular and genital epithelium is associated with serious sequelae if the condition is not treated early. It is generally accepted that patients with toxic epidermal necrolysis are better treated in burn units, which are experienced in the management of patients with extensive skin loss. Treatment includes support, elimination, and coverage with biosynthetic derivatives of the skin in affected areas, treatment of mucosal involvement, and specific immunosuppressive treatment. Of the treatments tested, only immunoglobulin G and cyclosporin A are currently used in most centers, even though there is no solid evidence to recommend any specific treatment. The particular aspects of the treatment of this disease include the prevention of sequelae related to the formation of synechiae, eye care to prevent serious sequelae that can lead to blindness, and specific immunosuppressive treatment. Better knowledge of the management principles of toxic epidermal necrolysis will lead to better disease management, higher survival rates, and lower prevalence of sequelae.
Views0Abstract
Review ArticlesToxic epidermal necrolysis: a paradigm of critical illness
Rev Bras Ter Intensiva. 2017;29(4):499-508
DOI 10.5935/0103-507X.20170075
Views0See moreABSTRACT
Toxic epidermal necrolysis is an adverse immunological skin reaction secondary in most cases to the administration of a drug. Toxic epidermal necrolysis, Stevens-Johnson syndrome, and multiform exudative erythema are part of the same disease spectrum. The mortality rate from toxic epidermal necrolysis is approximately 30%. The pathophysiology of toxic epidermal necrolysis is similar in many respects to that of superficial skin burns. Mucosal involvement of the ocular and genital epithelium is associated with serious sequelae if the condition is not treated early. It is generally accepted that patients with toxic epidermal necrolysis are better treated in burn units, which are experienced in the management of patients with extensive skin loss. Treatment includes support, elimination, and coverage with biosynthetic derivatives of the skin in affected areas, treatment of mucosal involvement, and specific immunosuppressive treatment. Of the treatments tested, only immunoglobulin G and cyclosporin A are currently used in most centers, even though there is no solid evidence to recommend any specific treatment. The particular aspects of the treatment of this disease include the prevention of sequelae related to the formation of synechiae, eye care to prevent serious sequelae that can lead to blindness, and specific immunosuppressive treatment. Better knowledge of the management principles of toxic epidermal necrolysis will lead to better disease management, higher survival rates, and lower prevalence of sequelae.
-
Review Articles
Safety criteria to start early mobilization in intensive care units. Systematic review
Rev Bras Ter Intensiva. 2017;29(4):509-519
Abstract
Review ArticlesSafety criteria to start early mobilization in intensive care units. Systematic review
Rev Bras Ter Intensiva. 2017;29(4):509-519
DOI 10.5935/0103-507X.20170076
Views0ABSTRACT
Mobilization of critically ill patients admitted to intensive care units should be performed based on safety criteria. The aim of the present review was to establish which safety criteria are most often used to start early mobilization for patients under mechanical ventilation admitted to intensive care units. Articles were searched in the PubMed, PEDro, LILACS, Cochrane and CINAHL databases; randomized and quasi-randomized clinical trials, cohort studies, comparative studies with or without simultaneous controls, case series with 10 or more consecutive cases and descriptive studies were included. The same was performed regarding prospective, retrospective or cross-sectional studies where safety criteria to start early mobilization should be described in the Methods section. Two reviewers independently selected potentially eligible studies according to the established inclusion criteria, extracted data and assessed the studies’ methodological quality. Narrative description was employed in data analysis to summarize the characteristics and results of the included studies; safety criteria were categorized as follows: cardiovascular, respiratory, neurological, orthopedic and other. A total of 37 articles were considered eligible. Cardiovascular safety criteria exhibited the largest number of variables. However, respiratory safety criteria exhibited higher concordance among studies. There was greater divergence among the authors regarding neurological criteria. There is a need to reinforce the recognition of the safety criteria used to start early mobilization for critically ill patients; the parameters and variables found might contribute to inclusion into service routines so as to start, make progress and guide clinical practice.
Keywords:Critical careEarly ambulationHospitalizationPatient safetyRehabilitationRespiration, artificialSee moreViews0Abstract
Review ArticlesSafety criteria to start early mobilization in intensive care units. Systematic review
Rev Bras Ter Intensiva. 2017;29(4):509-519
DOI 10.5935/0103-507X.20170076
Views0ABSTRACT
Mobilization of critically ill patients admitted to intensive care units should be performed based on safety criteria. The aim of the present review was to establish which safety criteria are most often used to start early mobilization for patients under mechanical ventilation admitted to intensive care units. Articles were searched in the PubMed, PEDro, LILACS, Cochrane and CINAHL databases; randomized and quasi-randomized clinical trials, cohort studies, comparative studies with or without simultaneous controls, case series with 10 or more consecutive cases and descriptive studies were included. The same was performed regarding prospective, retrospective or cross-sectional studies where safety criteria to start early mobilization should be described in the Methods section. Two reviewers independently selected potentially eligible studies according to the established inclusion criteria, extracted data and assessed the studies’ methodological quality. Narrative description was employed in data analysis to summarize the characteristics and results of the included studies; safety criteria were categorized as follows: cardiovascular, respiratory, neurological, orthopedic and other. A total of 37 articles were considered eligible. Cardiovascular safety criteria exhibited the largest number of variables. However, respiratory safety criteria exhibited higher concordance among studies. There was greater divergence among the authors regarding neurological criteria. There is a need to reinforce the recognition of the safety criteria used to start early mobilization for critically ill patients; the parameters and variables found might contribute to inclusion into service routines so as to start, make progress and guide clinical practice.
Keywords:Critical careEarly ambulationHospitalizationPatient safetyRehabilitationRespiration, artificialSee more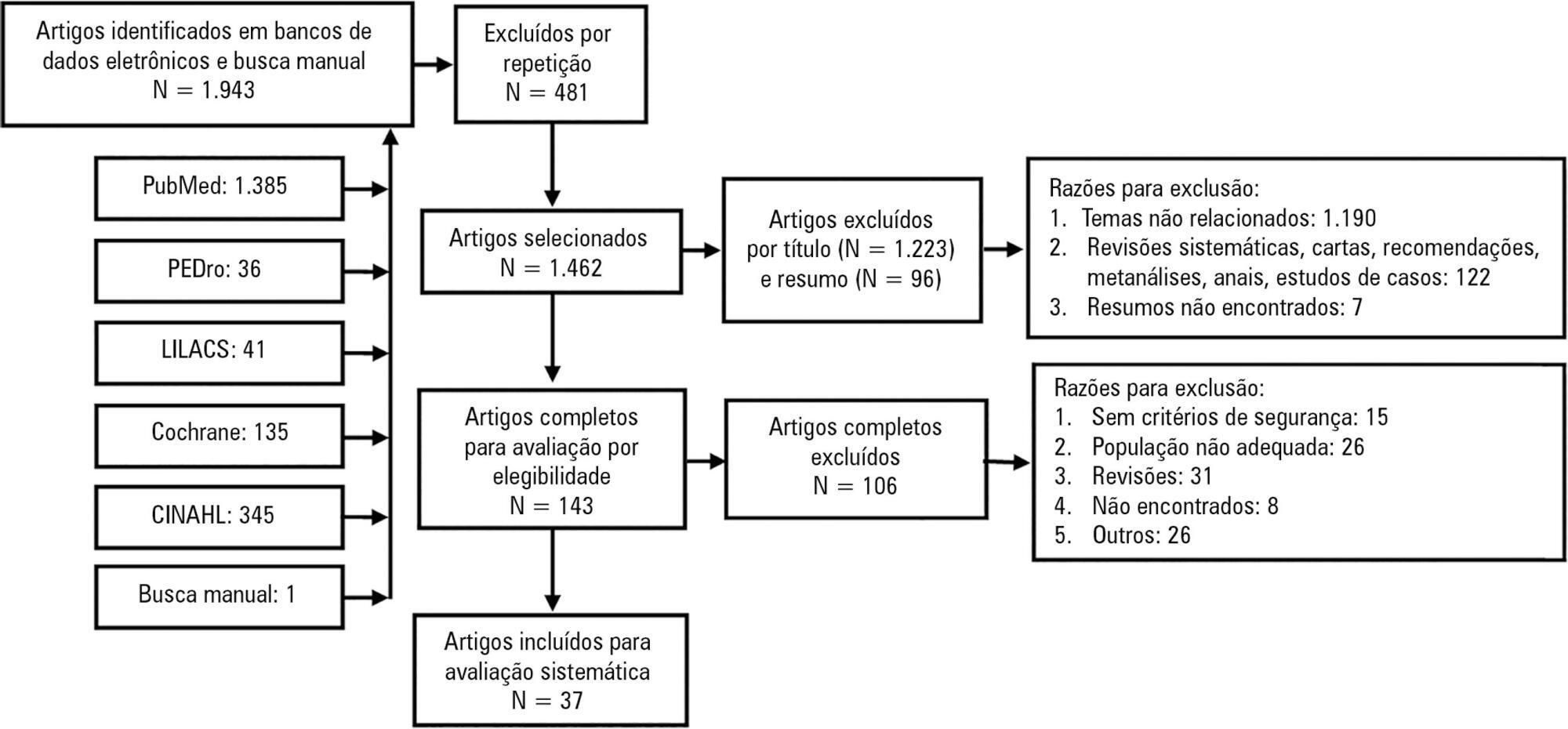
-
Letter to the Editor
Sepsis definitions
Rev Bras Ter Intensiva. 2017;29(4):520-521
Abstract
Letter to the EditorSepsis definitions
Rev Bras Ter Intensiva. 2017;29(4):520-521
DOI 10.5935/0103-507X.20170074
Views0To the EditorThe recent study in the Revista Brasileira de Terapia Intensiva (RBTI)() on the search for consensus on new definitions of sepsis in countries with limited resources represents another attempt to achieve uniformity of the phenotype of a syndrome that is polygenic in nature and thus has a wide variety of presentations. In addition […]See moreViews0Abstract
Letter to the EditorSepsis definitions
Rev Bras Ter Intensiva. 2017;29(4):520-521
DOI 10.5935/0103-507X.20170074
Views0To the EditorThe recent study in the Revista Brasileira de Terapia Intensiva (RBTI)() on the search for consensus on new definitions of sepsis in countries with limited resources represents another attempt to achieve uniformity of the phenotype of a syndrome that is polygenic in nature and thus has a wide variety of presentations. In addition […]See more -
Volume Articles - Critical Care Science (CCS)
