-
Commentaries
Is APACHE II a useful tool for clinical research?
Rev Bras Ter Intensiva. 2017;29(3):264-267
Abstract
CommentariesIs APACHE II a useful tool for clinical research?
Rev Bras Ter Intensiva. 2017;29(3):264-267
DOI 10.5935/0103-507X.20170046
Views0The population of patients admitted to the intensive care unit (ICU) is quite heterogeneous. Overall, the outcome of ICU treatment depends on the site, cause of admission, age, prior comorbidities, and acute physiological changes at admission and during the first several hours of treatment. Predictions of the in-hospital mortality of ICU patients play important roles […]See moreViews0

Abstract
CommentariesIs APACHE II a useful tool for clinical research?
Rev Bras Ter Intensiva. 2017;29(3):264-267
DOI 10.5935/0103-507X.20170046
Views0The population of patients admitted to the intensive care unit (ICU) is quite heterogeneous. Overall, the outcome of ICU treatment depends on the site, cause of admission, age, prior comorbidities, and acute physiological changes at admission and during the first several hours of treatment. Predictions of the in-hospital mortality of ICU patients play important roles […]See more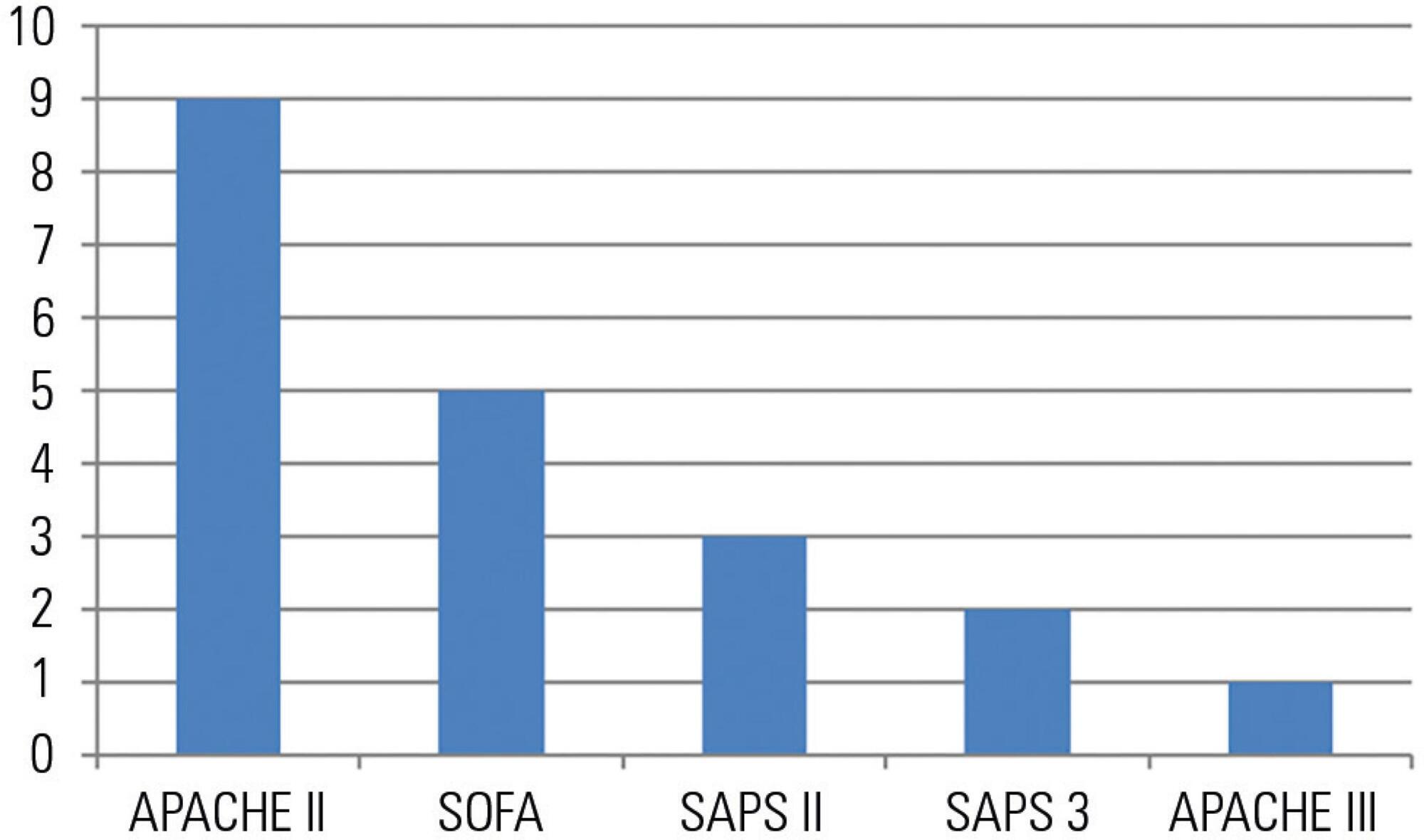
-
Commentaries
Why should we not use APACHE II for performance measurement and benchmarking?
Rev Bras Ter Intensiva. 2017;29(3):268-270
Abstract
CommentariesWhy should we not use APACHE II for performance measurement and benchmarking?
Rev Bras Ter Intensiva. 2017;29(3):268-270
DOI 10.5935/0103-507X.20170043
Views0The Acute Physiology and Chronic Health Evaluation (APACHE) is the most frequently used general severity-of-illness score in adult intensive care units (ICUs). APACHE scores use clinical, physiological and laboratory data observed at admission and during the first 24 hours after ICU admission. This is in order to estimate a given patient’s severity of illness by […]See moreViews0Abstract
CommentariesWhy should we not use APACHE II for performance measurement and benchmarking?
Rev Bras Ter Intensiva. 2017;29(3):268-270
DOI 10.5935/0103-507X.20170043
Views0The Acute Physiology and Chronic Health Evaluation (APACHE) is the most frequently used general severity-of-illness score in adult intensive care units (ICUs). APACHE scores use clinical, physiological and laboratory data observed at admission and during the first 24 hours after ICU admission. This is in order to estimate a given patient’s severity of illness by […]See more -
Articles
Extracorporeal membrane oxygenation in acute respiratory distress syndrome due to influenza A (H1N1)pdm09 pneumonia. A single-center experience during the 2013-2014 season
Rev Bras Ter Intensiva. 2017;29(3):271-278
Abstract
ArticlesExtracorporeal membrane oxygenation in acute respiratory distress syndrome due to influenza A (H1N1)pdm09 pneumonia. A single-center experience during the 2013-2014 season
Rev Bras Ter Intensiva. 2017;29(3):271-278
DOI 10.5935/0103-507X.20170048
Views3ABSTRACT
Objective:
This report aimed to describe the outcomes of the patients with severe H1N1 associated acute respiratory distress syndrome who were treated with extracorporeal membrane oxygenation therapy.
Methods:
This retrospective review analyzed a single-center cohort of adult patients with H1N1-related acute respiratory distress syndrome who were managed with veno-venous extracorporeal membrane oxygenation during the winter of 2013/2014.
Results:
A total of 10 patients received veno-venous extracorporeal membrane oxygenation for H1N1 influenza between January 2013 and March 2014. Seven patients were transferred to our center for extracorporeal membrane oxygenation consideration (all within 72 hours of initiating mechanical ventilation). The median patient age was forty years, and 30% were female. The median arterial oxygen partial pressure to fraction of inspired oxygen ratio was 62.5, and the median RESP score was 6. Three patients received inhaled nitric oxide, and four patients were proned as rescue therapy before extracorporeal membrane oxygenation was initiated. The median duration of mechanical ventilation was twenty-two days (range, 14 – 32). The median length of stay in the intensive care unit was twenty-seven days (range, 14 – 39). The median hospital length of stay was 29.1 days (range, 16.0 – 46.9). Minor bleeding complications occurred in 6 of 10 patients. Eight of the ten patients survived to hospital discharge.
Conclusion:
The survivors were relatively young and discharged with good functional status (i.e., enhancing quality-adjusted life-years-saved). Our experience shows that even a relatively new extracorporeal membrane oxygenation program can play an important role in that capacity and provide excellent outcomes for the sickest patients.
Keywords:Extracorporeal membrane oxygenationInfluenza A virus, H1N1 subtypeRespiratory distress syndrome, acuteSee moreViews3Abstract
ArticlesExtracorporeal membrane oxygenation in acute respiratory distress syndrome due to influenza A (H1N1)pdm09 pneumonia. A single-center experience during the 2013-2014 season
Rev Bras Ter Intensiva. 2017;29(3):271-278
DOI 10.5935/0103-507X.20170048
Views3ABSTRACT
Objective:
This report aimed to describe the outcomes of the patients with severe H1N1 associated acute respiratory distress syndrome who were treated with extracorporeal membrane oxygenation therapy.
Methods:
This retrospective review analyzed a single-center cohort of adult patients with H1N1-related acute respiratory distress syndrome who were managed with veno-venous extracorporeal membrane oxygenation during the winter of 2013/2014.
Results:
A total of 10 patients received veno-venous extracorporeal membrane oxygenation for H1N1 influenza between January 2013 and March 2014. Seven patients were transferred to our center for extracorporeal membrane oxygenation consideration (all within 72 hours of initiating mechanical ventilation). The median patient age was forty years, and 30% were female. The median arterial oxygen partial pressure to fraction of inspired oxygen ratio was 62.5, and the median RESP score was 6. Three patients received inhaled nitric oxide, and four patients were proned as rescue therapy before extracorporeal membrane oxygenation was initiated. The median duration of mechanical ventilation was twenty-two days (range, 14 – 32). The median length of stay in the intensive care unit was twenty-seven days (range, 14 – 39). The median hospital length of stay was 29.1 days (range, 16.0 – 46.9). Minor bleeding complications occurred in 6 of 10 patients. Eight of the ten patients survived to hospital discharge.
Conclusion:
The survivors were relatively young and discharged with good functional status (i.e., enhancing quality-adjusted life-years-saved). Our experience shows that even a relatively new extracorporeal membrane oxygenation program can play an important role in that capacity and provide excellent outcomes for the sickest patients.
Keywords:Extracorporeal membrane oxygenationInfluenza A virus, H1N1 subtypeRespiratory distress syndrome, acuteSee more -
Articles
Behavior of lung ultrasound findings during spontaneous breathing trial
Rev Bras Ter Intensiva. 2017;29(3):279-286
Abstract
ArticlesBehavior of lung ultrasound findings during spontaneous breathing trial
Rev Bras Ter Intensiva. 2017;29(3):279-286
DOI 10.5935/0103-507X.20170038
Views0See moreABSTRACT
Objective:
We aimed to investigate a potential association between B-lines and weaning failure.
Methods:
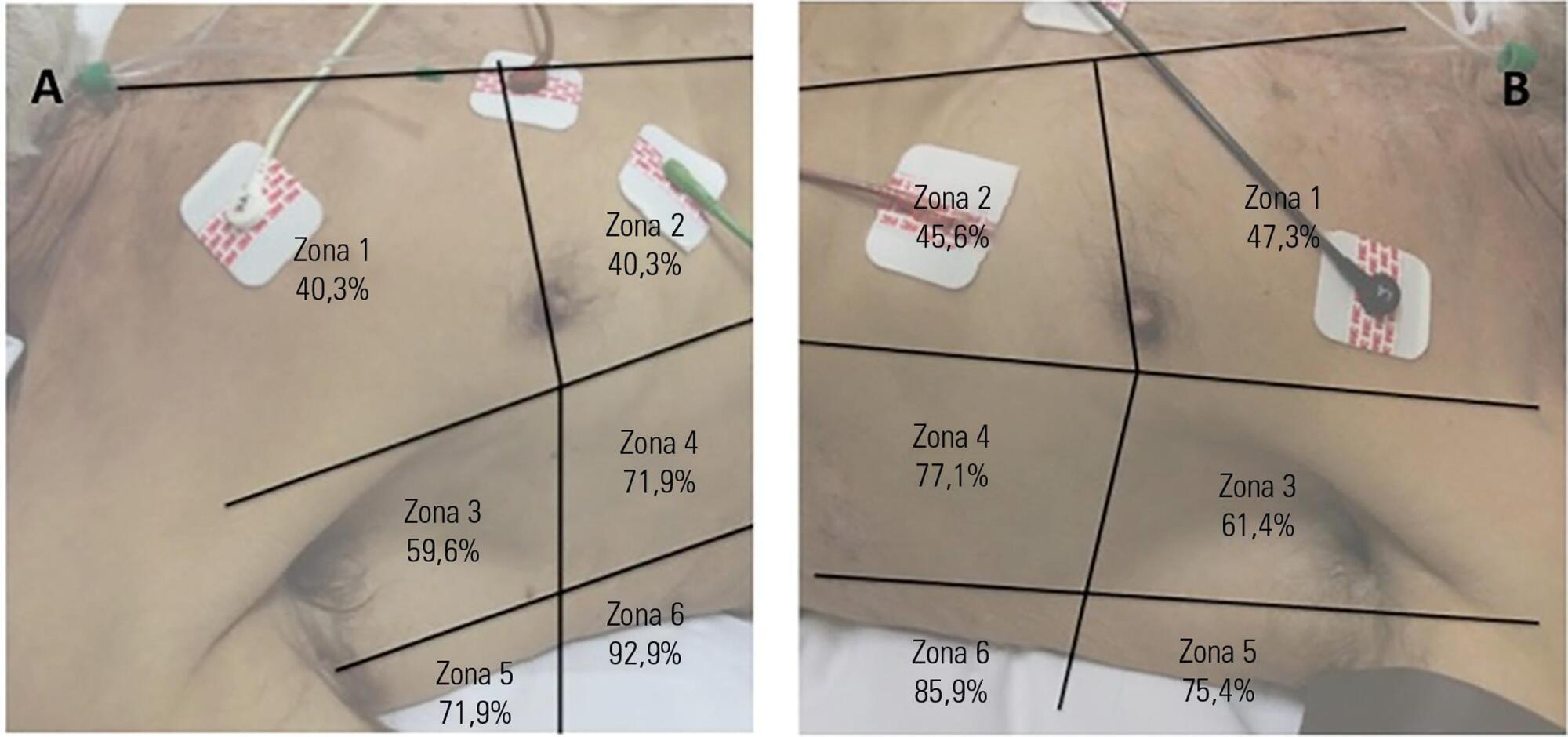
Fifty-seven subjects eligible for ventilation liberation were enrolled. Patients with tracheostomy were excluded. Lung ultrasound assessments of six thoracic zones were performed immediately before and at the exnd of the spontaneous breathing trial. B-predominance was defined as any profile with anterior bilateral B-pattern. Patients were followed up to 48 hours after extubation.
Results:
Thirty-eight individuals were successfully extubated; 11 failed the spontaneous breathing trial and 8 needed reintubation within 48 hours of extubation. At the beginning of the T-piece trial, B-pattern or consolidation was already found at the lower and posterior lung regions in more than half of the individuals and remained non-aerated at the end of the trial. A trend toward loss of lung aeration during spontaneous breathing trials was observed only in the spontaneous breathing trial-failure group (p = 0.07), and there was higher B-predominance at the end of the trial (p = 0.01).
Conclusion:
A loss of lung aeration during the spontaneous breathing trial in non-dependent lung zones was demonstrated in subjects who failed to wean.
Views0Abstract
ArticlesBehavior of lung ultrasound findings during spontaneous breathing trial
Rev Bras Ter Intensiva. 2017;29(3):279-286
DOI 10.5935/0103-507X.20170038
Views0See moreABSTRACT
Objective:
We aimed to investigate a potential association between B-lines and weaning failure.
Methods:
Fifty-seven subjects eligible for ventilation liberation were enrolled. Patients with tracheostomy were excluded. Lung ultrasound assessments of six thoracic zones were performed immediately before and at the exnd of the spontaneous breathing trial. B-predominance was defined as any profile with anterior bilateral B-pattern. Patients were followed up to 48 hours after extubation.
Results:
Thirty-eight individuals were successfully extubated; 11 failed the spontaneous breathing trial and 8 needed reintubation within 48 hours of extubation. At the beginning of the T-piece trial, B-pattern or consolidation was already found at the lower and posterior lung regions in more than half of the individuals and remained non-aerated at the end of the trial. A trend toward loss of lung aeration during spontaneous breathing trials was observed only in the spontaneous breathing trial-failure group (p = 0.07), and there was higher B-predominance at the end of the trial (p = 0.01).
Conclusion:
A loss of lung aeration during the spontaneous breathing trial in non-dependent lung zones was demonstrated in subjects who failed to wean.
-
Articles
Oxygen saturation and lactate concentration gradient from the right atrium to the pulmonary artery in the immediate postoperative following cardiac surgery with extracorporeal circulation
Rev Bras Ter Intensiva. 2017;29(3):287-292
Abstract
ArticlesOxygen saturation and lactate concentration gradient from the right atrium to the pulmonary artery in the immediate postoperative following cardiac surgery with extracorporeal circulation
Rev Bras Ter Intensiva. 2017;29(3):287-292
DOI 10.5935/0103-507X.20170042
Views1ABSTRACT
Objective:
This prospective study aimed to characterize the changes in blood lactate concentration and blood oxygen saturation in patients during the immediate postoperative period of cardiac surgery with extracorporeal circulation.
Methods:
Blood samples were collected from 35 patients in a rapid and random order from the arterial line and from the proximal and distal port of a pulmonary artery catheter.
Results:
The results showed no statistically significant differences between the blood oxygen saturation in the right atrium (72% ± 0.11%) and the blood oxygen saturation in the pulmonary artery (71% ± 0.08%). The blood lactate concentration in the right atrium was 1.7mmol/L ± 0.5mmol/L, and the blood lactate concentration in the pulmonary artery was 1.6mmol/L ± 0.5mmol/L (p < 0.0005).
Conclusion:
The difference between the blood lactate concentration in the right atrium and the blood lactate concentration in the pulmonary artery might be a consequence of the low blood lactate concentration in the blood from the coronary sinus, as it constitutes an important substrate for the myocardium during this period. The lack of differences between the blood oxygen saturation in the right atrium and the percentage of blood oxygen saturation in the pulmonary artery suggests a lower oxygen extraction by the myocardium given a lower oxygen consumption.
Keywords:Extracorporeal circulationLactateOxygen consumption/physiologyOxygen/metabolismPostoperative periodThoracic surgerySee moreViews1Abstract
ArticlesOxygen saturation and lactate concentration gradient from the right atrium to the pulmonary artery in the immediate postoperative following cardiac surgery with extracorporeal circulation
Rev Bras Ter Intensiva. 2017;29(3):287-292
DOI 10.5935/0103-507X.20170042
Views1ABSTRACT
Objective:
This prospective study aimed to characterize the changes in blood lactate concentration and blood oxygen saturation in patients during the immediate postoperative period of cardiac surgery with extracorporeal circulation.
Methods:
Blood samples were collected from 35 patients in a rapid and random order from the arterial line and from the proximal and distal port of a pulmonary artery catheter.
Results:
The results showed no statistically significant differences between the blood oxygen saturation in the right atrium (72% ± 0.11%) and the blood oxygen saturation in the pulmonary artery (71% ± 0.08%). The blood lactate concentration in the right atrium was 1.7mmol/L ± 0.5mmol/L, and the blood lactate concentration in the pulmonary artery was 1.6mmol/L ± 0.5mmol/L (p < 0.0005).
Conclusion:
The difference between the blood lactate concentration in the right atrium and the blood lactate concentration in the pulmonary artery might be a consequence of the low blood lactate concentration in the blood from the coronary sinus, as it constitutes an important substrate for the myocardium during this period. The lack of differences between the blood oxygen saturation in the right atrium and the percentage of blood oxygen saturation in the pulmonary artery suggests a lower oxygen extraction by the myocardium given a lower oxygen consumption.
Keywords:Extracorporeal circulationLactateOxygen consumption/physiologyOxygen/metabolismPostoperative periodThoracic surgerySee more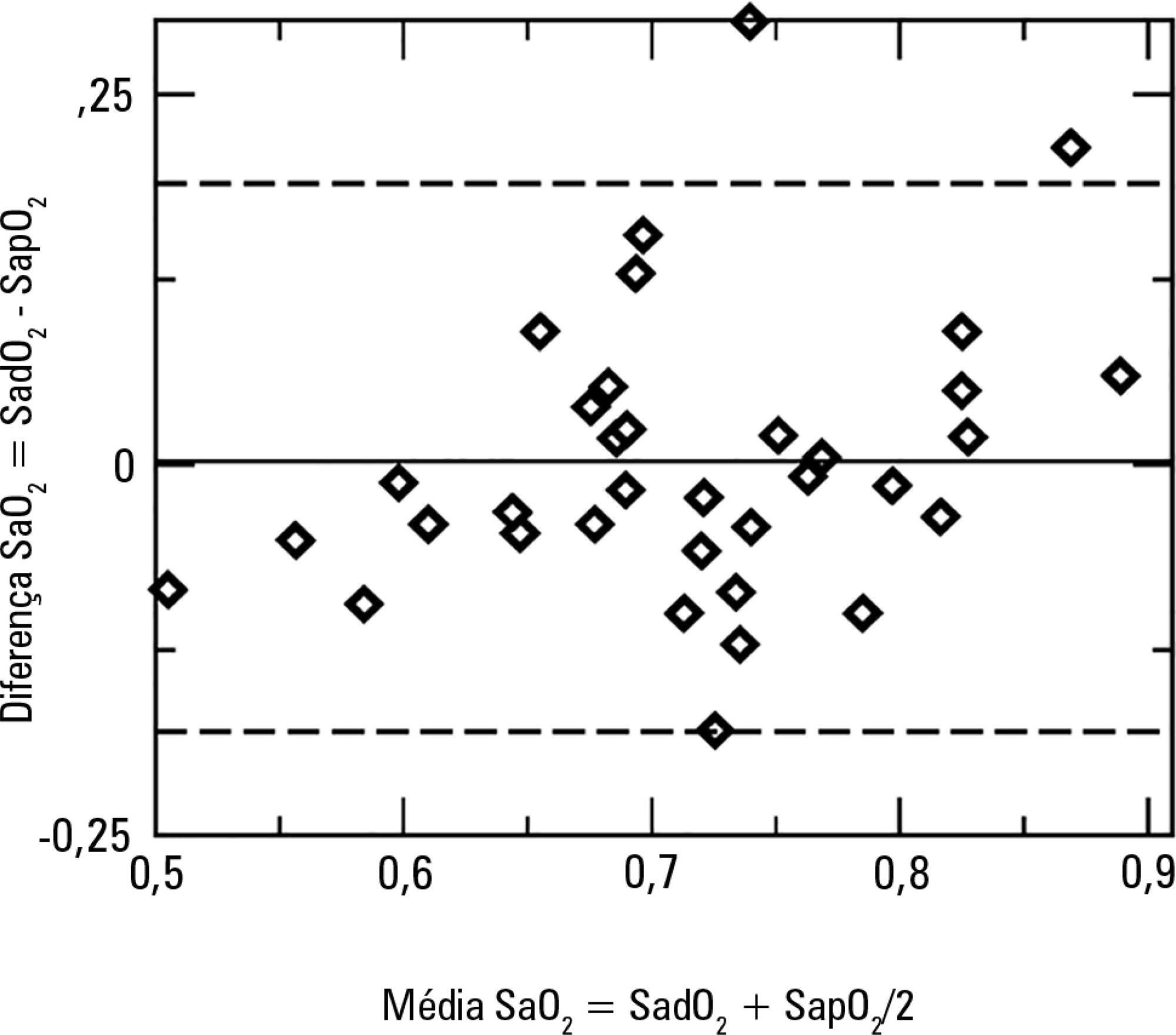
-
Original Articles
Functional ability in younger and older elderlies after discharge from the intensive care unit. A prospective cohort
Rev Bras Ter Intensiva. 2017;29(3):293-302
Abstract
Original ArticlesFunctional ability in younger and older elderlies after discharge from the intensive care unit. A prospective cohort
Rev Bras Ter Intensiva. 2017;29(3):293-302
DOI 10.5935/0103-507X.20170055
Views0See moreABSTRACT
Objective:
To compare the functional capacity of younger elderly individuals (60 to 79 years old) with that of older elderly individuals (≥ 80 years old) during the first 6 months after discharge from the intensive care unit.
Methods:
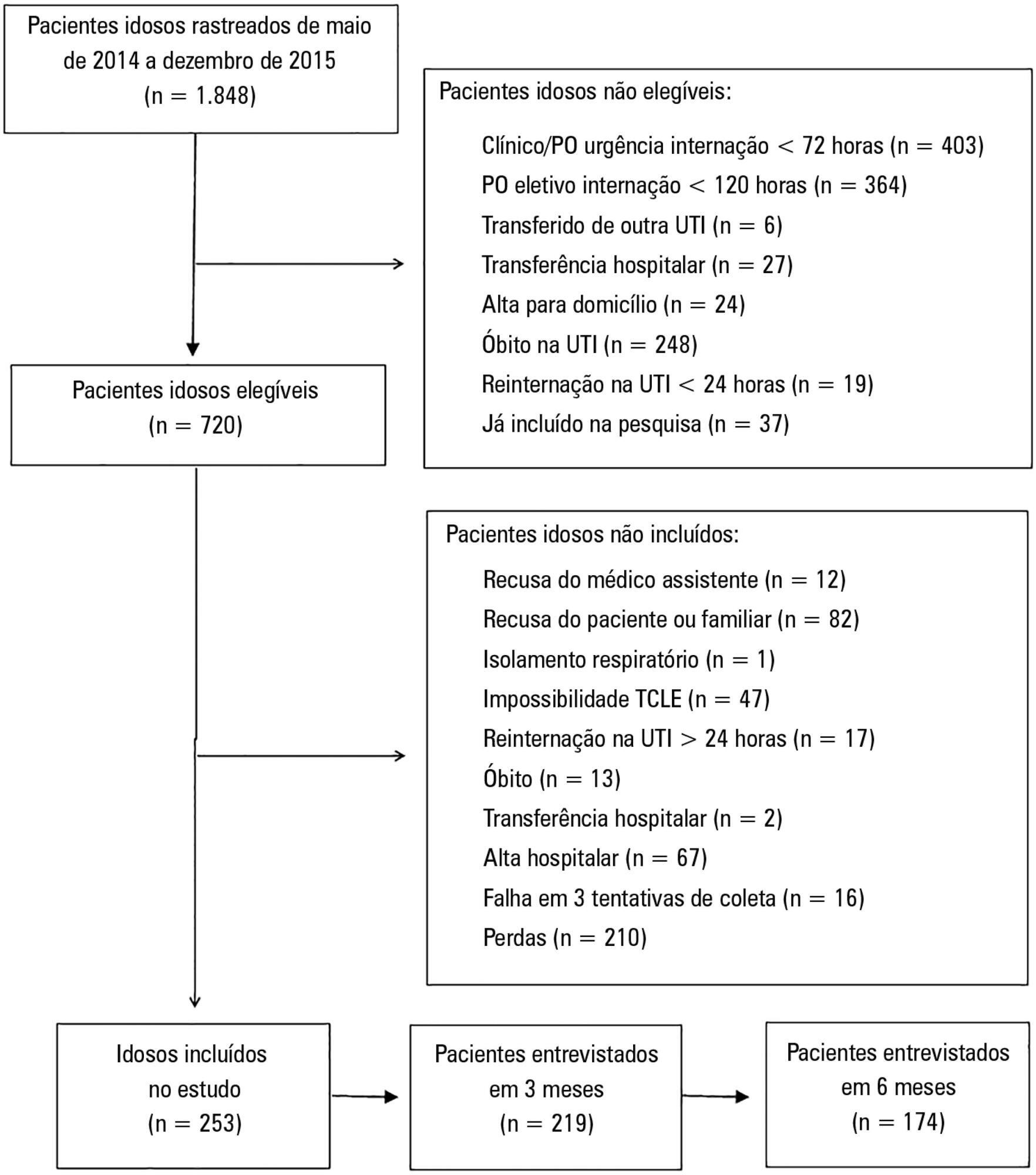
A multicenter prospective cohort study was conducted, in which data on intensive care unit admission and outcomes after hospital discharge (immediate post-discharge, after 3 months and after 6 months) were collected. Muscle strength was evaluated through the protocol of the Medical Research Council and dynamometry (handgrip); the ability to perform activities of daily life and functional independence were assessed by the Barthel index and the usual level of physical activity (International Physical Activity Questionnaire); and quality of life was assessed by the 12-Item Short-Form Health Survey Version 2.
Results:
Among the 253 patients included, 167 were younger elderly (between 61 and 79 years old), and 86 were older elderly (≥ 80 years old). During the sixth month of evaluation, the older elderlies presented a higher need for a caregiver (69.0% versus 49, 5%, p = 0.002). Functional capacity prior to intensive care unit admission and in the third month after discharge was lower in older elderlies than in younger ones (Barthel prior to the intensive care unit: 73.0 ± 30.0 versus 86.5 ± 22.6; p <0.001, Barthel in the third month: 63.5 ± 34.0 versus 71.5 ± 35.5, p = 0.03), as was the usual level of physical activity (International Physical Activity Questionnaire in the third month: active/very active 3.4% versus 18.3%, no physical activity 64.4% versus 39.7%, p < 0.001, and International Physical Activity Questionnaire in the sixth month: active/very active 5.8% versus 20.8%, no physical activity 69.2% versus 43.4%, p = 0.005). Older elderlies had lower muscle strength when assessed according to handgrip in both the dominant (14.5 ± 7.7 versus 19.9 ± 9.6, p = 0.008) and non-dominant limb (13.1 ± 6.7 versus 17.5 ± 9.1, p = 0.02). There were no differences in functional capacity loss or reported quality of life between the age groups.
Conclusion:
Although there were great functional capacity losses after discharge from the intensive care unit in both age groups, there was no difference in the magnitude of functional capacity loss between younger (60 to 79 years) and older elderly individuals (≥ 80 years old) during the first 6 months after discharge from the intensive care unit.
Views0Abstract
Original ArticlesFunctional ability in younger and older elderlies after discharge from the intensive care unit. A prospective cohort
Rev Bras Ter Intensiva. 2017;29(3):293-302
DOI 10.5935/0103-507X.20170055
Views0See moreABSTRACT
Objective:
To compare the functional capacity of younger elderly individuals (60 to 79 years old) with that of older elderly individuals (≥ 80 years old) during the first 6 months after discharge from the intensive care unit.
Methods:
A multicenter prospective cohort study was conducted, in which data on intensive care unit admission and outcomes after hospital discharge (immediate post-discharge, after 3 months and after 6 months) were collected. Muscle strength was evaluated through the protocol of the Medical Research Council and dynamometry (handgrip); the ability to perform activities of daily life and functional independence were assessed by the Barthel index and the usual level of physical activity (International Physical Activity Questionnaire); and quality of life was assessed by the 12-Item Short-Form Health Survey Version 2.
Results:
Among the 253 patients included, 167 were younger elderly (between 61 and 79 years old), and 86 were older elderly (≥ 80 years old). During the sixth month of evaluation, the older elderlies presented a higher need for a caregiver (69.0% versus 49, 5%, p = 0.002). Functional capacity prior to intensive care unit admission and in the third month after discharge was lower in older elderlies than in younger ones (Barthel prior to the intensive care unit: 73.0 ± 30.0 versus 86.5 ± 22.6; p <0.001, Barthel in the third month: 63.5 ± 34.0 versus 71.5 ± 35.5, p = 0.03), as was the usual level of physical activity (International Physical Activity Questionnaire in the third month: active/very active 3.4% versus 18.3%, no physical activity 64.4% versus 39.7%, p < 0.001, and International Physical Activity Questionnaire in the sixth month: active/very active 5.8% versus 20.8%, no physical activity 69.2% versus 43.4%, p = 0.005). Older elderlies had lower muscle strength when assessed according to handgrip in both the dominant (14.5 ± 7.7 versus 19.9 ± 9.6, p = 0.008) and non-dominant limb (13.1 ± 6.7 versus 17.5 ± 9.1, p = 0.02). There were no differences in functional capacity loss or reported quality of life between the age groups.
Conclusion:
Although there were great functional capacity losses after discharge from the intensive care unit in both age groups, there was no difference in the magnitude of functional capacity loss between younger (60 to 79 years) and older elderly individuals (≥ 80 years old) during the first 6 months after discharge from the intensive care unit.
-
Articles
Contrast-induced acute kidney injury: the importance of diagnostic criteria for establishing prevalence and prognosis in the intensive care unit
Rev Bras Ter Intensiva. 2017;29(3):303-309
Abstract
ArticlesContrast-induced acute kidney injury: the importance of diagnostic criteria for establishing prevalence and prognosis in the intensive care unit
Rev Bras Ter Intensiva. 2017;29(3):303-309
DOI 10.5935/0103-507X.20170041
Views0ABSTRACT
Objective:
To establish whether there is superiority between contrast-induced acute kidney injury and contrast-induced nephropathy criteria as predictors of unfavorable clinical outcomes.
Methods:
Retrospective study carried out in a tertiary hospital with 157 patients undergoing radiocontrast infusion for propaedeutic purposes.
Results:
One hundred forty patients fulfilled the inclusion criteria: patients who met the criteria for contrast-induced acute kidney injury (59) also met the criteria for contrast-induced nephropathy (76), 44.3% met the criteria for KDIGO staging, 6.4% of the patients required renal replacement therapy, and 10.7% died.
Conclusion:
The diagnosis of contrast-induced nephropathy was the most sensitive criterion for renal replacement therapy and death, whereas KDIGO showed the highest specificity; there was no correlation between contrast volume and progression to contrast-induced acute kidney injury, contrast-induced nephropathy, support dialysis or death in the assessed population.
Keywords:Acute kidney injury/chemically inducedContrast media/adverse effectsPrognosisRenal dialysisRisk assessmentSeverity of illness indexSee moreViews0Abstract
ArticlesContrast-induced acute kidney injury: the importance of diagnostic criteria for establishing prevalence and prognosis in the intensive care unit
Rev Bras Ter Intensiva. 2017;29(3):303-309
DOI 10.5935/0103-507X.20170041
Views0ABSTRACT
Objective:
To establish whether there is superiority between contrast-induced acute kidney injury and contrast-induced nephropathy criteria as predictors of unfavorable clinical outcomes.
Methods:
Retrospective study carried out in a tertiary hospital with 157 patients undergoing radiocontrast infusion for propaedeutic purposes.
Results:
One hundred forty patients fulfilled the inclusion criteria: patients who met the criteria for contrast-induced acute kidney injury (59) also met the criteria for contrast-induced nephropathy (76), 44.3% met the criteria for KDIGO staging, 6.4% of the patients required renal replacement therapy, and 10.7% died.
Conclusion:
The diagnosis of contrast-induced nephropathy was the most sensitive criterion for renal replacement therapy and death, whereas KDIGO showed the highest specificity; there was no correlation between contrast volume and progression to contrast-induced acute kidney injury, contrast-induced nephropathy, support dialysis or death in the assessed population.
Keywords:Acute kidney injury/chemically inducedContrast media/adverse effectsPrognosisRenal dialysisRisk assessmentSeverity of illness indexSee more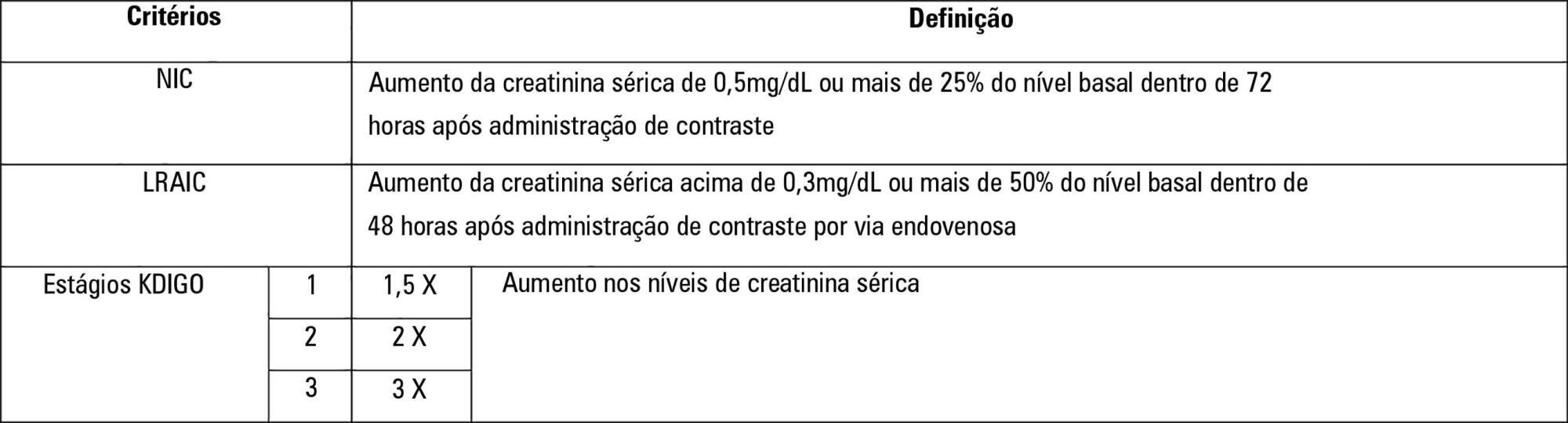
-
Articles
Analysis of biofilm production by clinical isolates of Pseudomonas aeruginosa from patients with ventilator-associated pneumonia
Rev Bras Ter Intensiva. 2017;29(3):310-316
Abstract
ArticlesAnalysis of biofilm production by clinical isolates of Pseudomonas aeruginosa from patients with ventilator-associated pneumonia
Rev Bras Ter Intensiva. 2017;29(3):310-316
DOI 10.5935/0103-507X.20170039
Views0ABSTRACT
Objective:
To phenotypically evaluate biofilm production by Pseudomonas aeruginosa clinically isolated from patients with ventilator-associated pneumonia.
Methods:
Twenty clinical isolates of P. aeruginosa were analyzed, 19 of which were from clinical samples of tracheal aspirate, and one was from a bronchoalveolar lavage sample. The evaluation of the capacity of P. aeruginosa to produce biofilm was verified using two techniques, one qualitative and the other quantitative.
Results:
The qualitative technique showed that only 15% of the isolates were considered biofilm producers, while the quantitative technique showed that 75% of the isolates were biofilm producers. The biofilm isolates presented the following susceptibility profile: 53.3% were multidrug-resistant, and 46.7% were multidrug-sensitive.
Conclusion:
The quantitative technique was more effective than the qualitative technique for the detection of biofilm production. For the bacterial population analyzed, biofilm production was independent of the susceptibility profile of the bacteria, demonstrating that the therapeutic failure could be related to biofilm production, as it prevented the destruction of the bacteria present in this structure, causing complications of pneumonia associated with mechanical ventilation, including extrapulmonary infections, and making it difficult to treat the infection.
Keywords:BiofilmsPneumonia, ventilator-associatedPseudomonas aeruginosaRespiration, artificial/adverse effectsSee moreViews0Abstract
ArticlesAnalysis of biofilm production by clinical isolates of Pseudomonas aeruginosa from patients with ventilator-associated pneumonia
Rev Bras Ter Intensiva. 2017;29(3):310-316
DOI 10.5935/0103-507X.20170039
Views0ABSTRACT
Objective:
To phenotypically evaluate biofilm production by Pseudomonas aeruginosa clinically isolated from patients with ventilator-associated pneumonia.
Methods:
Twenty clinical isolates of P. aeruginosa were analyzed, 19 of which were from clinical samples of tracheal aspirate, and one was from a bronchoalveolar lavage sample. The evaluation of the capacity of P. aeruginosa to produce biofilm was verified using two techniques, one qualitative and the other quantitative.
Results:
The qualitative technique showed that only 15% of the isolates were considered biofilm producers, while the quantitative technique showed that 75% of the isolates were biofilm producers. The biofilm isolates presented the following susceptibility profile: 53.3% were multidrug-resistant, and 46.7% were multidrug-sensitive.
Conclusion:
The quantitative technique was more effective than the qualitative technique for the detection of biofilm production. For the bacterial population analyzed, biofilm production was independent of the susceptibility profile of the bacteria, demonstrating that the therapeutic failure could be related to biofilm production, as it prevented the destruction of the bacteria present in this structure, causing complications of pneumonia associated with mechanical ventilation, including extrapulmonary infections, and making it difficult to treat the infection.
Keywords:BiofilmsPneumonia, ventilator-associatedPseudomonas aeruginosaRespiration, artificial/adverse effectsSee more -
Articles
Systemic inflammatory response syndrome criteria and the prediction of hospital mortality in critically ill patients: a retrospective cohort study
Rev Bras Ter Intensiva. 2017;29(3):317-324
Abstract
ArticlesSystemic inflammatory response syndrome criteria and the prediction of hospital mortality in critically ill patients: a retrospective cohort study
Rev Bras Ter Intensiva. 2017;29(3):317-324
DOI 10.5935/0103-507X.20170047
Views1See moreABSTRACT
Objective:
This study intended to determine whether the systemic inflammatory response syndrome criteria can predict hospital mortality in a Brazilian cohort of critically ill patients.
Methods:
We performed a retrospective cohort study at a private tertiary hospital in São Paulo (SP), Brazil. We extracted information from the adult intensive care unit database (Sistema EpimedTM). We compared the SAPS 3 and the systemic inflammatory response syndrome model as dichotomous (≥ 2 criteria: systemic inflammatory response syndrome -positive versus 0 – 1 criterion: systemic inflammatory response syndrome -negative) and ordinal variables from 0 to 4 (according to the number of systemic inflammatory response syndrome criteria met) in the prediction of hospital mortality at intensive care unit admission. Model discrimination was compared using the area under the receiver operating characteristics (AUROC) curve.
Results:
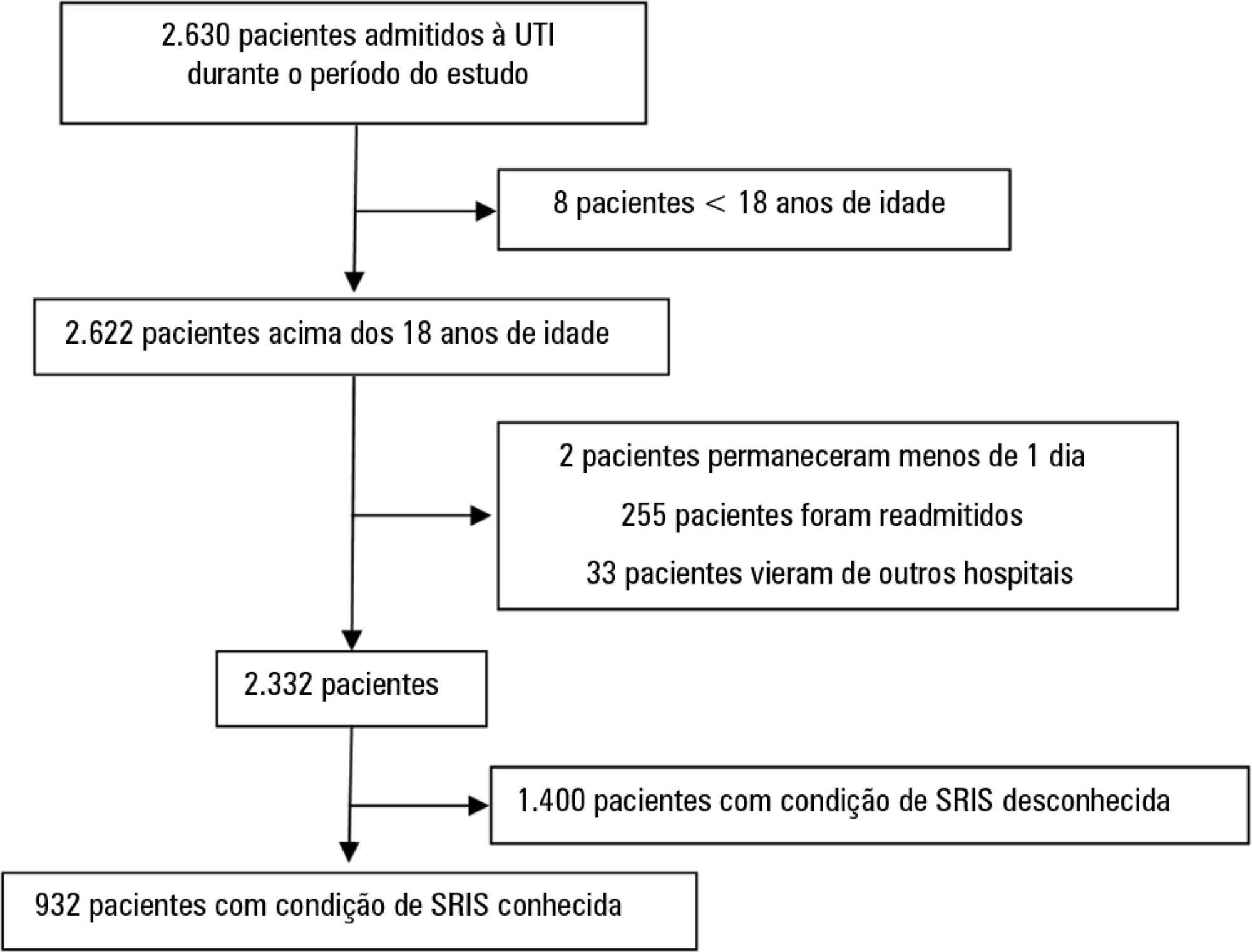
From January to December 2012, we studied 932 patients (60.4% were systemic inflammatory response syndrome -positive). systemic inflammatory response syndrome -positive patients were more critically ill than systemic inflammatory response syndrome -negative patients and had higher hospital mortality (16.9% versus 8.1%, p < 0.001). In the adjusted analysis, being systemic inflammatory response syndrome -positive independently increased the risk of death by 82% (odds ratio 1.82; 95% confidence interval [CI] 1.12 - 2.96, p = 0.016). However, the AUROC curve for the SAPS 3 model was higher (0.81, 95%CI 0.78 - 0.85) compared to the systemic inflammatory response syndrome model with the systemic inflammatory response syndrome criteria as a dichotomous variable (0.60, 95%CI 0.55 - 0.65) and as an ordinal variable (0.62, 95%CI 0.57 - 0.68; p < 0.001) for hospital mortality.
Conclusion:
Although systemic inflammatory response syndrome is associated with hospital mortality, the systemic inflammatory response syndrome criteria show low accuracy in the prediction of mortality compared with the SAPS 3.
Views1Abstract
ArticlesSystemic inflammatory response syndrome criteria and the prediction of hospital mortality in critically ill patients: a retrospective cohort study
Rev Bras Ter Intensiva. 2017;29(3):317-324
DOI 10.5935/0103-507X.20170047
Views1See moreABSTRACT
Objective:
This study intended to determine whether the systemic inflammatory response syndrome criteria can predict hospital mortality in a Brazilian cohort of critically ill patients.
Methods:
We performed a retrospective cohort study at a private tertiary hospital in São Paulo (SP), Brazil. We extracted information from the adult intensive care unit database (Sistema EpimedTM). We compared the SAPS 3 and the systemic inflammatory response syndrome model as dichotomous (≥ 2 criteria: systemic inflammatory response syndrome -positive versus 0 – 1 criterion: systemic inflammatory response syndrome -negative) and ordinal variables from 0 to 4 (according to the number of systemic inflammatory response syndrome criteria met) in the prediction of hospital mortality at intensive care unit admission. Model discrimination was compared using the area under the receiver operating characteristics (AUROC) curve.
Results:
From January to December 2012, we studied 932 patients (60.4% were systemic inflammatory response syndrome -positive). systemic inflammatory response syndrome -positive patients were more critically ill than systemic inflammatory response syndrome -negative patients and had higher hospital mortality (16.9% versus 8.1%, p < 0.001). In the adjusted analysis, being systemic inflammatory response syndrome -positive independently increased the risk of death by 82% (odds ratio 1.82; 95% confidence interval [CI] 1.12 - 2.96, p = 0.016). However, the AUROC curve for the SAPS 3 model was higher (0.81, 95%CI 0.78 - 0.85) compared to the systemic inflammatory response syndrome model with the systemic inflammatory response syndrome criteria as a dichotomous variable (0.60, 95%CI 0.55 - 0.65) and as an ordinal variable (0.62, 95%CI 0.57 - 0.68; p < 0.001) for hospital mortality.
Conclusion:
Although systemic inflammatory response syndrome is associated with hospital mortality, the systemic inflammatory response syndrome criteria show low accuracy in the prediction of mortality compared with the SAPS 3.
-
Original Articles
Immediate postoperative of bariatric surgery in the intensive care unit versus an inpatient unit. A retrospective study with 828 patients
Rev Bras Ter Intensiva. 2017;29(3):325-330
Abstract
Original ArticlesImmediate postoperative of bariatric surgery in the intensive care unit versus an inpatient unit. A retrospective study with 828 patients
Rev Bras Ter Intensiva. 2017;29(3):325-330
DOI 10.5935/0103-507X.20170050
Views0ABSTRACT
Objective:
To compare the incidence of complications and the duration of hospitalization of patients undergoing bariatric surgery admitted to the intensive care unit or a post-surgical hospitalization unit.
Methods:
This retrospective observational study included 828 patients admitted between January 2010 and February 2015 during the immediate postoperative period of bariatric surgery in a hospital. Data were collected via electronic medical records. The Mann-Whitney test was used to compare continuous variables, and the chi-square was used to compare categorical variables.
Results:
Patients in both groups had similar demographic characteristics, with no significant differences in anthropometric data and comorbidities. There was no significant difference in the comparison of complications between the two groups. However, the group admitted to the intensive care unit had longer hospitalization times (median of 3 days versus 2 days, p < 0.05), and hospital costs were 8% higher.
Conclusion:
The present study found no benefit in the routine admittance of patients to the intensive care unit after undergoing bariatric surgery. This practice increased hospitalization time and hospital costs, which wasted resources. It is necessary to create objective criteria to identify patients requiring intensive care unit admission after bariatric surgery.
Keywords:Bariatric surgery/complicationsInpatient care unitsIntensive care unitsObesity/surgeryPerioperative careQuality of health careSee moreViews0Abstract
Original ArticlesImmediate postoperative of bariatric surgery in the intensive care unit versus an inpatient unit. A retrospective study with 828 patients
Rev Bras Ter Intensiva. 2017;29(3):325-330
DOI 10.5935/0103-507X.20170050
Views0ABSTRACT
Objective:
To compare the incidence of complications and the duration of hospitalization of patients undergoing bariatric surgery admitted to the intensive care unit or a post-surgical hospitalization unit.
Methods:
This retrospective observational study included 828 patients admitted between January 2010 and February 2015 during the immediate postoperative period of bariatric surgery in a hospital. Data were collected via electronic medical records. The Mann-Whitney test was used to compare continuous variables, and the chi-square was used to compare categorical variables.
Results:
Patients in both groups had similar demographic characteristics, with no significant differences in anthropometric data and comorbidities. There was no significant difference in the comparison of complications between the two groups. However, the group admitted to the intensive care unit had longer hospitalization times (median of 3 days versus 2 days, p < 0.05), and hospital costs were 8% higher.
Conclusion:
The present study found no benefit in the routine admittance of patients to the intensive care unit after undergoing bariatric surgery. This practice increased hospitalization time and hospital costs, which wasted resources. It is necessary to create objective criteria to identify patients requiring intensive care unit admission after bariatric surgery.
Keywords:Bariatric surgery/complicationsInpatient care unitsIntensive care unitsObesity/surgeryPerioperative careQuality of health careSee more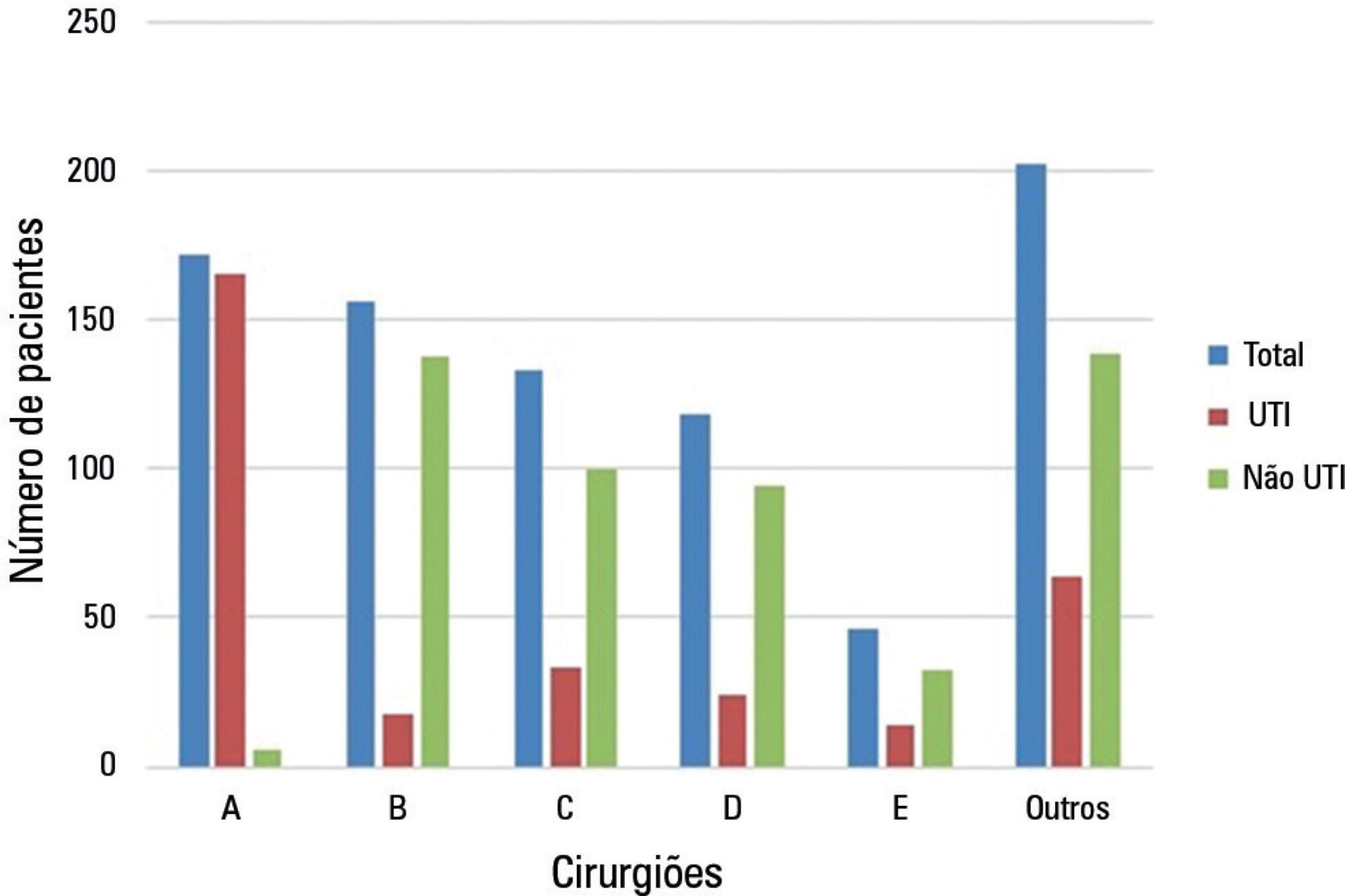
-
Articles
Antimicrobial drug-related problems in a neonatal intensive care unit
Rev Bras Ter Intensiva. 2017;29(3):331-336
Abstract
ArticlesAntimicrobial drug-related problems in a neonatal intensive care unit
Rev Bras Ter Intensiva. 2017;29(3):331-336
DOI 10.5935/0103-507X.20170040
Views0ABSTRACT
Objective:
The goal was to determine the main drug-related problems in neonates who were using antimicrobials.
Method:
This was an observational, prospective and longitudinal study. Drug-related problems were classified according to version 6.2 of the Pharmaceutical Care Network Europe Foundation classification. A descriptive analysis was performed, in which the clinical and therapeutic variables were presented as absolute and relative frequencies or as the mean and standard deviation, as appropriate.
Results:
In total, 152 neonates with a predominance of males (58.5%), gestational age of 32.7 ± 4.2 weeks and weight of 1,903.1 ± 846.9g were included. The main diagnostic hypothesis of infection was early sepsis (66.5%), and 71.7% of the neonates had some risk factor for infection. Among the neonates, 33.6% had at least one drug-related problem. Of these, 84.8% were related to treatment effectiveness and 15.2% to adverse reactions. The main cause of drug-related problems was the selected dose, particularly for aminoglycosides and cephalosporins.
Conclusion:
The use of antimicrobials in the neonatal intensive care is mainly associated with problems related to medication effectiveness, predominantly the prescription of subdoses of antimicrobials, especially aminoglycosides.
Keywords:AminoglycosidesAnti-infective agentsInfant, newbornIntensive care units, neonatalMedication errorsSee moreViews0Abstract
ArticlesAntimicrobial drug-related problems in a neonatal intensive care unit
Rev Bras Ter Intensiva. 2017;29(3):331-336
DOI 10.5935/0103-507X.20170040
Views0ABSTRACT
Objective:
The goal was to determine the main drug-related problems in neonates who were using antimicrobials.
Method:
This was an observational, prospective and longitudinal study. Drug-related problems were classified according to version 6.2 of the Pharmaceutical Care Network Europe Foundation classification. A descriptive analysis was performed, in which the clinical and therapeutic variables were presented as absolute and relative frequencies or as the mean and standard deviation, as appropriate.
Results:
In total, 152 neonates with a predominance of males (58.5%), gestational age of 32.7 ± 4.2 weeks and weight of 1,903.1 ± 846.9g were included. The main diagnostic hypothesis of infection was early sepsis (66.5%), and 71.7% of the neonates had some risk factor for infection. Among the neonates, 33.6% had at least one drug-related problem. Of these, 84.8% were related to treatment effectiveness and 15.2% to adverse reactions. The main cause of drug-related problems was the selected dose, particularly for aminoglycosides and cephalosporins.
Conclusion:
The use of antimicrobials in the neonatal intensive care is mainly associated with problems related to medication effectiveness, predominantly the prescription of subdoses of antimicrobials, especially aminoglycosides.
Keywords:AminoglycosidesAnti-infective agentsInfant, newbornIntensive care units, neonatalMedication errorsSee more -
Original Articles
Delirium in a Latin American intensive care unit. A prospective cohort study of mechanically ventilated patients
Rev Bras Ter Intensiva. 2017;29(3):337-345
Abstract
Original ArticlesDelirium in a Latin American intensive care unit. A prospective cohort study of mechanically ventilated patients
Rev Bras Ter Intensiva. 2017;29(3):337-345
DOI 10.5935/0103-507X.20170058
Views0ABSTRACT
Objective:
To establish the prevalence of delirium in a general intensive care unit and to identify associated factors, clinical expression and the influence on outcomes.
Methods:
This was a prospective cohort study in a medical surgical intensive care unit. The Richmond Agitation-Sedation Scale and Confusion Assessment Method for the Intensive Care Unit were used daily to identify delirium in mechanically ventilated patients.
Results:
In this series, delirium prevalence was 80% (N = 184 delirious patients out of 230 patients). The number of patients according to delirium psychomotor subtypes was as follows: 11 hyperactive patients (6%), 9 hypoactive patients (5%) and 160 mixed patients (89%). Multiple logistic regression modeling using delirium as the dependent outcome variable (to study the risk factors for delirium) revealed that age > 65 years, history of alcohol consumption, and number of mechanical ventilation days were independent variables associated with the development of delirium. The multiple logistic regression model using hospital mortality as the dependent outcome variable (to study the risk factors for death) showed that severity of illness, according to the Acute Physiology and Chronic Health Evaluation II, mechanical ventilation for more than 7 days, and sedation days were all independent predictors for excess hospital mortality.
Conclusion:
This Latin American prospective cohort investigation confirmed specific factors important for the development of delirium and the outcome of death among general intensive care unit patients. In both analyses, we found that the duration of mechanical ventilation was a predictor of untoward outcomes.
Keywords:analgesiaBrain organ dysfunctionConcencious sedationDeliriumMortalityRespiration, artificialSee moreViews0Abstract
Original ArticlesDelirium in a Latin American intensive care unit. A prospective cohort study of mechanically ventilated patients
Rev Bras Ter Intensiva. 2017;29(3):337-345
DOI 10.5935/0103-507X.20170058
Views0ABSTRACT
Objective:
To establish the prevalence of delirium in a general intensive care unit and to identify associated factors, clinical expression and the influence on outcomes.
Methods:
This was a prospective cohort study in a medical surgical intensive care unit. The Richmond Agitation-Sedation Scale and Confusion Assessment Method for the Intensive Care Unit were used daily to identify delirium in mechanically ventilated patients.
Results:
In this series, delirium prevalence was 80% (N = 184 delirious patients out of 230 patients). The number of patients according to delirium psychomotor subtypes was as follows: 11 hyperactive patients (6%), 9 hypoactive patients (5%) and 160 mixed patients (89%). Multiple logistic regression modeling using delirium as the dependent outcome variable (to study the risk factors for delirium) revealed that age > 65 years, history of alcohol consumption, and number of mechanical ventilation days were independent variables associated with the development of delirium. The multiple logistic regression model using hospital mortality as the dependent outcome variable (to study the risk factors for death) showed that severity of illness, according to the Acute Physiology and Chronic Health Evaluation II, mechanical ventilation for more than 7 days, and sedation days were all independent predictors for excess hospital mortality.
Conclusion:
This Latin American prospective cohort investigation confirmed specific factors important for the development of delirium and the outcome of death among general intensive care unit patients. In both analyses, we found that the duration of mechanical ventilation was a predictor of untoward outcomes.
Keywords:analgesiaBrain organ dysfunctionConcencious sedationDeliriumMortalityRespiration, artificialSee more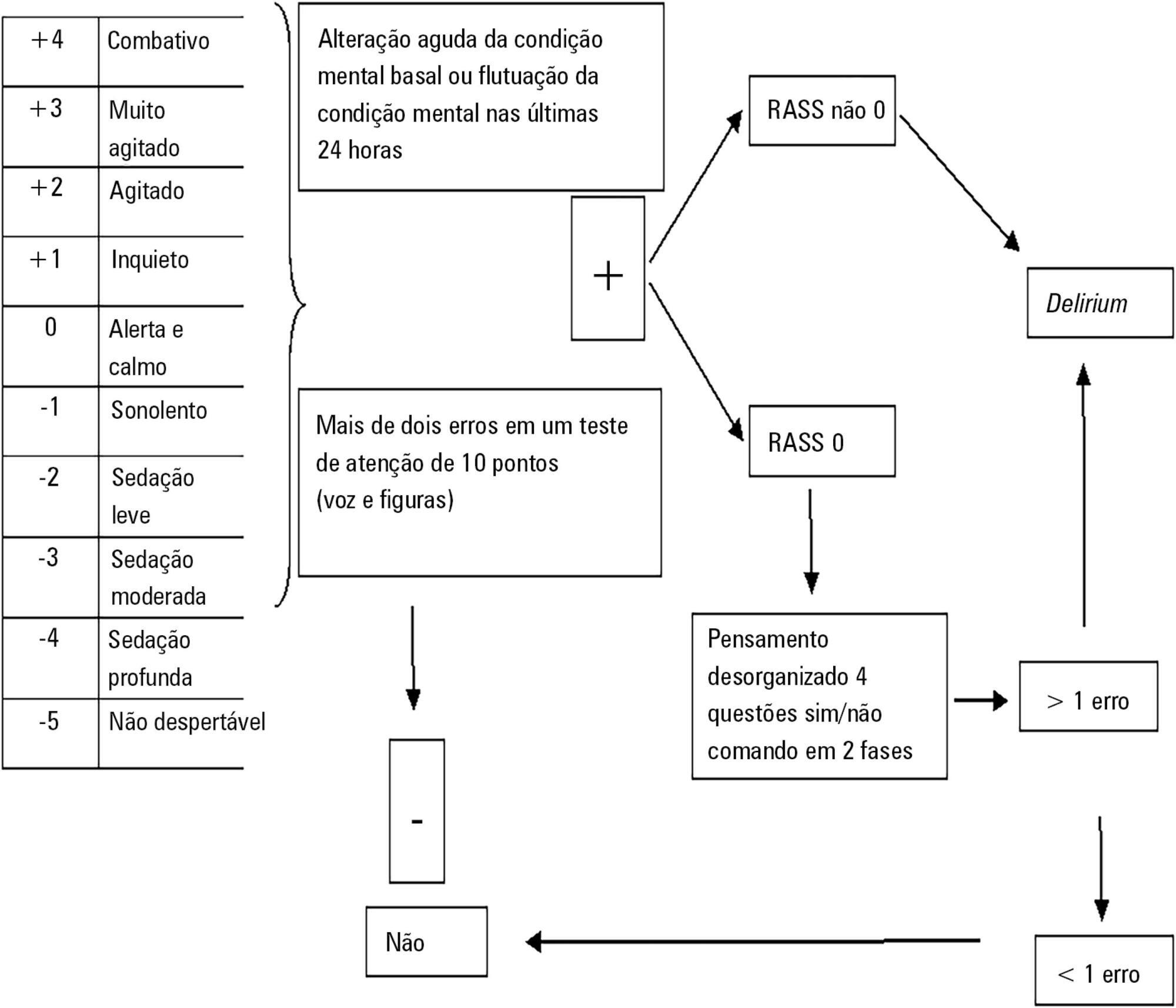
-
Review Articles
Fluid overload in children undergoing mechanical ventilation
Rev Bras Ter Intensiva. 2017;29(3):346-353
Abstract
Review ArticlesFluid overload in children undergoing mechanical ventilation
Rev Bras Ter Intensiva. 2017;29(3):346-353
DOI 10.5935/0103-507X.20170045
Views0ABSTRACT
Patients admitted to an intensive care unit are prone to cumulated fluid overload and receive intravenous volumes through the aggressive resuscitation recommended for septic shock treatment, as well as other fluid sources related to medications and nutritional support. The liberal liquid supply strategy has been associated with higher morbidity and mortality. Although there are few prospective pediatric studies, new strategies are being proposed. This non-systematic review discusses the pathophysiology of fluid overload, its consequences, and the available therapeutic strategies. During systemic inflammatory response syndrome, the endothelial glycocalyx is damaged, favoring fluid extravasation and resulting in interstitial edema. Extravasation to the third space results in longer mechanical ventilation, a greater need for renal replacement therapy, and longer intensive care unit and hospital stays, among other changes. Proper hemodynamic monitoring, as well as cautious infusion of fluids, can minimize these damages. Once cumulative fluid overload is established, treatment with long-term use of loop diuretics may lead to resistance to these medications. Strategies that can reduce intensive care unit morbidity and mortality include the early use of vasopressors (norepinephrine) to improve cardiac output and renal perfusion, the use of a combination of diuretics and aminophylline to induce diuresis, and the use of sedation and early mobilization protocols.
Keywords:Fluid therapyHemodynamicsRenal insufficiencyRespiration, artificialWater-electrolyte imbalanceSee moreViews0Abstract
Review ArticlesFluid overload in children undergoing mechanical ventilation
Rev Bras Ter Intensiva. 2017;29(3):346-353
DOI 10.5935/0103-507X.20170045
Views0ABSTRACT
Patients admitted to an intensive care unit are prone to cumulated fluid overload and receive intravenous volumes through the aggressive resuscitation recommended for septic shock treatment, as well as other fluid sources related to medications and nutritional support. The liberal liquid supply strategy has been associated with higher morbidity and mortality. Although there are few prospective pediatric studies, new strategies are being proposed. This non-systematic review discusses the pathophysiology of fluid overload, its consequences, and the available therapeutic strategies. During systemic inflammatory response syndrome, the endothelial glycocalyx is damaged, favoring fluid extravasation and resulting in interstitial edema. Extravasation to the third space results in longer mechanical ventilation, a greater need for renal replacement therapy, and longer intensive care unit and hospital stays, among other changes. Proper hemodynamic monitoring, as well as cautious infusion of fluids, can minimize these damages. Once cumulative fluid overload is established, treatment with long-term use of loop diuretics may lead to resistance to these medications. Strategies that can reduce intensive care unit morbidity and mortality include the early use of vasopressors (norepinephrine) to improve cardiac output and renal perfusion, the use of a combination of diuretics and aminophylline to induce diuresis, and the use of sedation and early mobilization protocols.
Keywords:Fluid therapyHemodynamicsRenal insufficiencyRespiration, artificialWater-electrolyte imbalanceSee more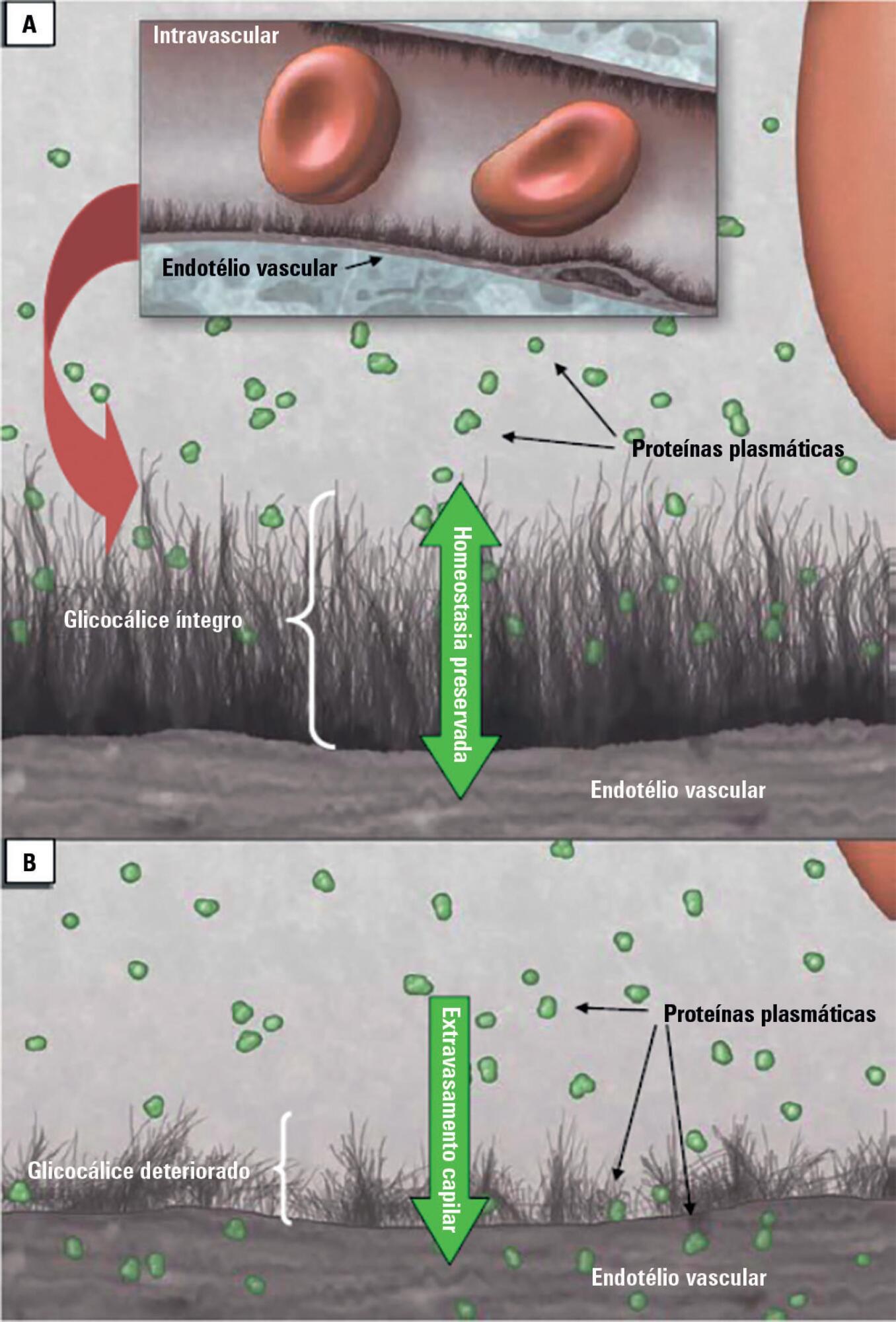
-
Review Articles
What every intensivist should know about acute respiratory distress syndrome and diffuse alveolar damage
Rev Bras Ter Intensiva. 2017;29(3):354-363
Abstract
Review ArticlesWhat every intensivist should know about acute respiratory distress syndrome and diffuse alveolar damage
Rev Bras Ter Intensiva. 2017;29(3):354-363
DOI 10.5935/0103-507X.20170044
Views0ABSTRACT
Acute respiratory distress syndrome is a challenging entity for the intensivist. The pathological hallmark of the acute phase is diffuse alveolar damage, which is present in approximately half of living patients with acute respiratory distress syndrome. It is clear that respiratory support for acute respiratory distress syndrome has gradually been improving over recent decades. However, it is also evident that these procedures are beneficial, as they reduce lung injury and keep the patient alive. This could be interpreted as a time-gaining strategy until the trigger or causal or risk factor improves, the inflammatory storm decreases and the lung heals. However, all except two pharmacological treatments (neuromuscular blockers and steroids) were unable to improve the acute respiratory distress syndrome outcome. The hypothesis that pharmacological negative results may be explained by the histological heterogeneity of acute respiratory distress syndrome has been supported by the recent demonstration that acute respiratory distress syndrome with diffuse alveolar damage constitutes a specific clinical-pathological entity. Given that diffuse alveolar damage is a pathological diagnosis and that open lung biopsy (the most common technique to obtain lung tissue) has several side effects, it is necessary to develop surrogate biomarkers for diffuse alveolar damage. The aim of this narrative review is to address the following three topics related to acute respiratory distress syndrome: (a) the relationship between acute respiratory distress syndrome and diffuse alveolar damage, (b) how diffuse alveolar damage could be surrogated in the clinical setting and (c) how enrichment in diffuse alveolar damage may improve the results of pharmacological clinical trials tried out on patients with acute respiratory distress syndrome.
Keywords:acute respiratory distress syndromeDiffuse alveolar damagePharmacological treatmentSurrogate biomarkersSee moreViews0Abstract
Review ArticlesWhat every intensivist should know about acute respiratory distress syndrome and diffuse alveolar damage
Rev Bras Ter Intensiva. 2017;29(3):354-363
DOI 10.5935/0103-507X.20170044
Views0ABSTRACT
Acute respiratory distress syndrome is a challenging entity for the intensivist. The pathological hallmark of the acute phase is diffuse alveolar damage, which is present in approximately half of living patients with acute respiratory distress syndrome. It is clear that respiratory support for acute respiratory distress syndrome has gradually been improving over recent decades. However, it is also evident that these procedures are beneficial, as they reduce lung injury and keep the patient alive. This could be interpreted as a time-gaining strategy until the trigger or causal or risk factor improves, the inflammatory storm decreases and the lung heals. However, all except two pharmacological treatments (neuromuscular blockers and steroids) were unable to improve the acute respiratory distress syndrome outcome. The hypothesis that pharmacological negative results may be explained by the histological heterogeneity of acute respiratory distress syndrome has been supported by the recent demonstration that acute respiratory distress syndrome with diffuse alveolar damage constitutes a specific clinical-pathological entity. Given that diffuse alveolar damage is a pathological diagnosis and that open lung biopsy (the most common technique to obtain lung tissue) has several side effects, it is necessary to develop surrogate biomarkers for diffuse alveolar damage. The aim of this narrative review is to address the following three topics related to acute respiratory distress syndrome: (a) the relationship between acute respiratory distress syndrome and diffuse alveolar damage, (b) how diffuse alveolar damage could be surrogated in the clinical setting and (c) how enrichment in diffuse alveolar damage may improve the results of pharmacological clinical trials tried out on patients with acute respiratory distress syndrome.
Keywords:acute respiratory distress syndromeDiffuse alveolar damagePharmacological treatmentSurrogate biomarkersSee more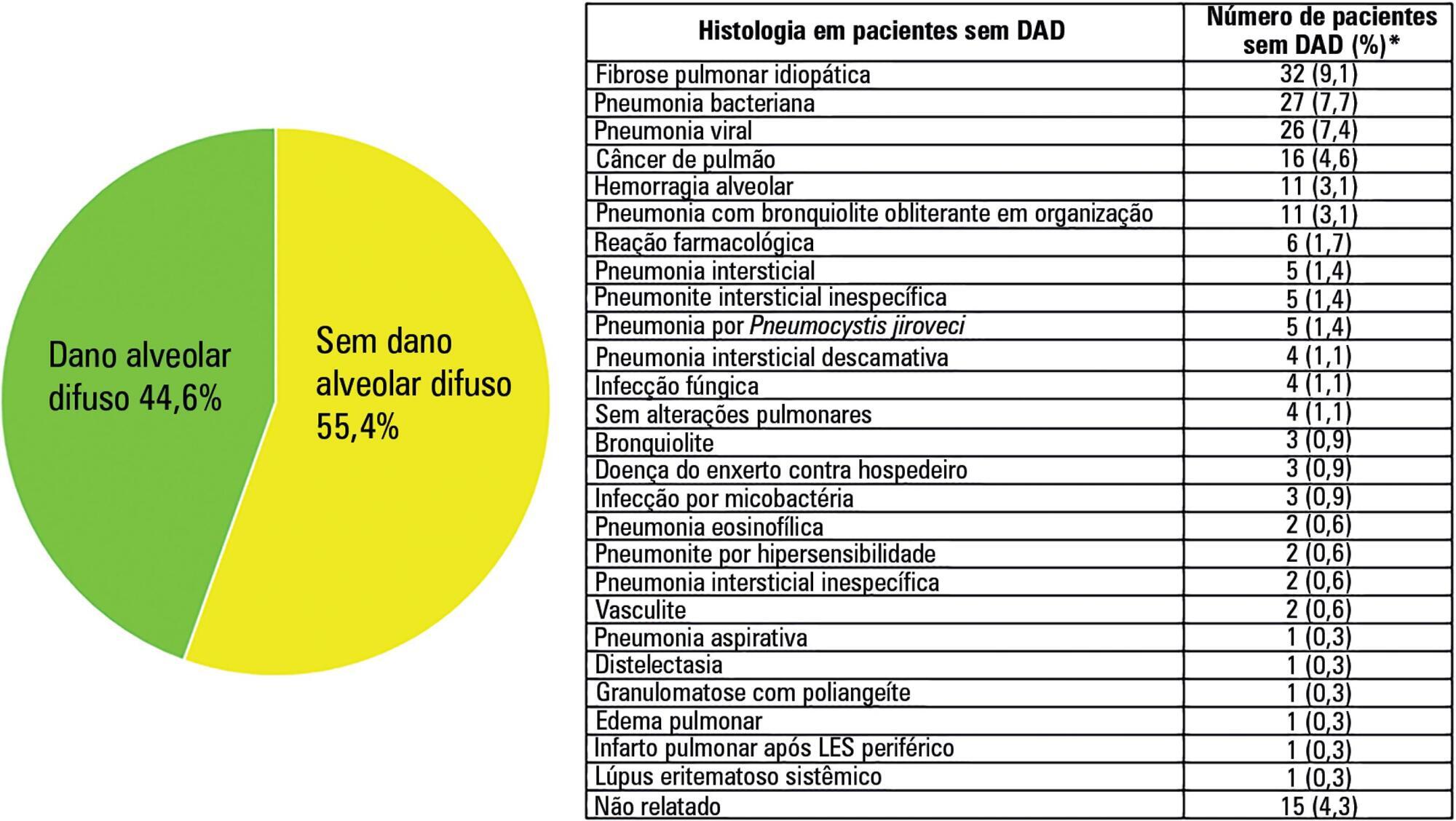
-
Review Articles
Dysglycemia in the critically ill patient: current evidence and future perspectives
Rev Bras Ter Intensiva. 2017;29(3):364-372
Abstract
Review ArticlesDysglycemia in the critically ill patient: current evidence and future perspectives
Rev Bras Ter Intensiva. 2017;29(3):364-372
DOI 10.5935/0103-507X.20170054
Views0ABSTRACT
Dysglycemia in critically ill patients (hyperglycemia, hypoglycemia, glycemic variability and time in range) is a biomarker of disease severity and is associated with higher mortality. However, this impact appears to be weakened in patients with previous diabetes mellitus, particularly in those with poor premorbid glycemic control; this phenomenon has been called “diabetes paradox”. This phenomenon determines that glycated hemoglobin (HbA1c) values should be considered in choosing glycemic control protocols on admission to an intensive care unit and that patients’ target blood glucose ranges should be adjusted according to their HbA1c values. Therefore, HbA1c emerges as a simple tool that allows information that has therapeutic utility and prognostic value to be obtained in the intensive care unit.
Keywords:Blood glucoseHemoglobin A, glycosylatedhyperglycemiaHypoglycemiaIntensive care unitsMortalitySeverity of illness indexSee moreViews0Abstract
Review ArticlesDysglycemia in the critically ill patient: current evidence and future perspectives
Rev Bras Ter Intensiva. 2017;29(3):364-372
DOI 10.5935/0103-507X.20170054
Views0ABSTRACT
Dysglycemia in critically ill patients (hyperglycemia, hypoglycemia, glycemic variability and time in range) is a biomarker of disease severity and is associated with higher mortality. However, this impact appears to be weakened in patients with previous diabetes mellitus, particularly in those with poor premorbid glycemic control; this phenomenon has been called “diabetes paradox”. This phenomenon determines that glycated hemoglobin (HbA1c) values should be considered in choosing glycemic control protocols on admission to an intensive care unit and that patients’ target blood glucose ranges should be adjusted according to their HbA1c values. Therefore, HbA1c emerges as a simple tool that allows information that has therapeutic utility and prognostic value to be obtained in the intensive care unit.
Keywords:Blood glucoseHemoglobin A, glycosylatedhyperglycemiaHypoglycemiaIntensive care unitsMortalitySeverity of illness indexSee more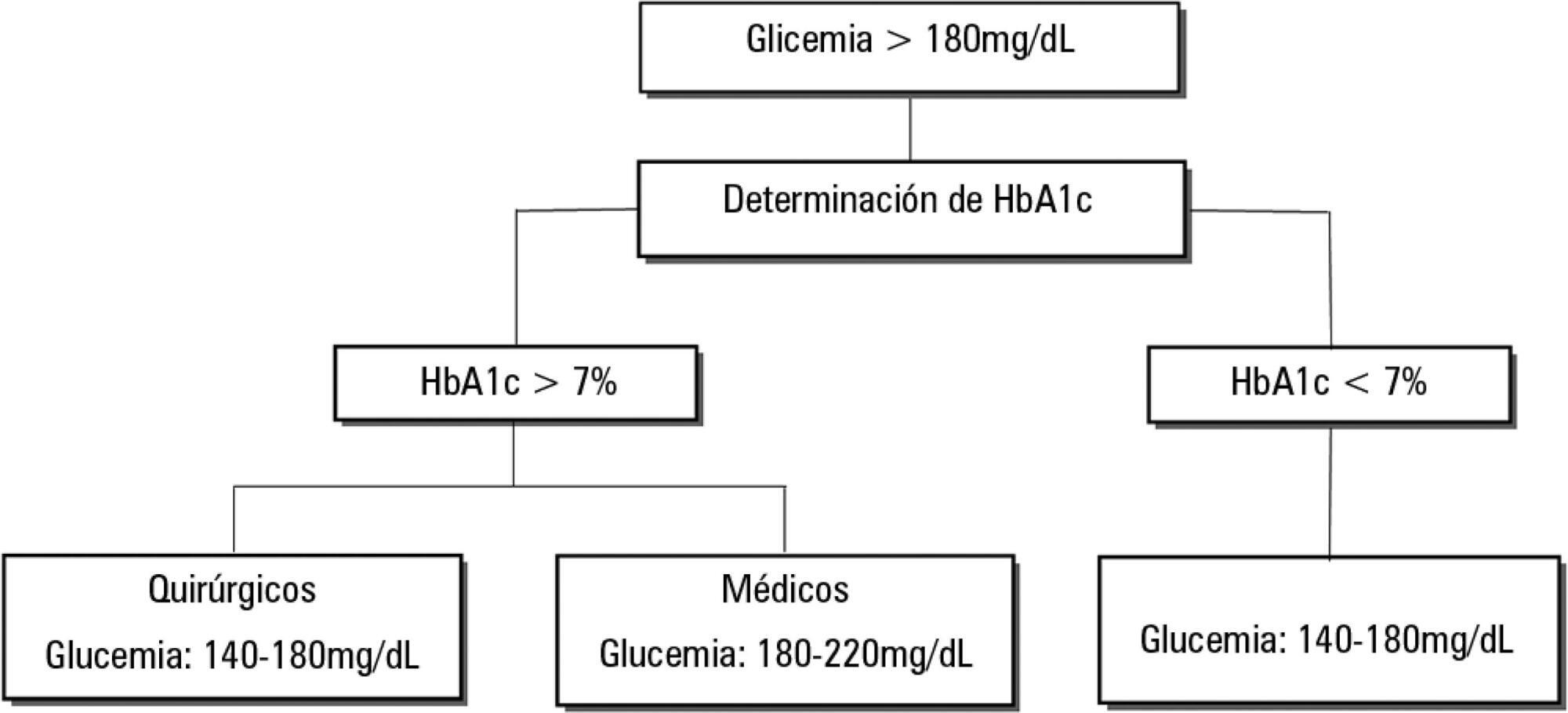
-
Review Articles
Biomarkers of renal recovery after acute kidney injury
Rev Bras Ter Intensiva. 2017;29(3):373-381
Abstract
Review ArticlesBiomarkers of renal recovery after acute kidney injury
Rev Bras Ter Intensiva. 2017;29(3):373-381
DOI 10.5935/0103-507X.20170051
Views0ABSTRACT
Novel biomarkers can be suitable for early acute kidney injury diagnosis and the prediction of the need for dialysis. It remains unclear whether such biomarkers may also play a role in the prediction of recovery after established acute kidney injury or in aiding the decision of when to stop renal support therapy. PubMed, Web of Science and Google Scholar were searched for studies that reported on the epidemiology of renal recovery after acute kidney injury, the risk factors of recovery versus non-recovery after acute kidney injury, and potential biomarkers of acute kidney injury recovery. The reference lists of these articles and relevant review articles were also reviewed. Final references were selected for inclusion in the review based on their relevance. New biomarkers exhibited a potential role in the early diagnosis of acute kidney injury recovery. Urine HGF, IGFBP-7, TIMP-2 and NGAL may improve our ability to predict the odds and timing of recovery and eventually renal support withdrawal. Acute kidney injury recovery requires more study, and its definition needs to be standardized to allow for better and more powerful research on biomarkers because some of them show potential for the prediction of acute kidney injury recovery.
Keywords:Acute kidney injuryBiomarkersCritical careIntensive careRenal insufficiencyRenal replacement therapySee moreViews0Abstract
Review ArticlesBiomarkers of renal recovery after acute kidney injury
Rev Bras Ter Intensiva. 2017;29(3):373-381
DOI 10.5935/0103-507X.20170051
Views0ABSTRACT
Novel biomarkers can be suitable for early acute kidney injury diagnosis and the prediction of the need for dialysis. It remains unclear whether such biomarkers may also play a role in the prediction of recovery after established acute kidney injury or in aiding the decision of when to stop renal support therapy. PubMed, Web of Science and Google Scholar were searched for studies that reported on the epidemiology of renal recovery after acute kidney injury, the risk factors of recovery versus non-recovery after acute kidney injury, and potential biomarkers of acute kidney injury recovery. The reference lists of these articles and relevant review articles were also reviewed. Final references were selected for inclusion in the review based on their relevance. New biomarkers exhibited a potential role in the early diagnosis of acute kidney injury recovery. Urine HGF, IGFBP-7, TIMP-2 and NGAL may improve our ability to predict the odds and timing of recovery and eventually renal support withdrawal. Acute kidney injury recovery requires more study, and its definition needs to be standardized to allow for better and more powerful research on biomarkers because some of them show potential for the prediction of acute kidney injury recovery.
Keywords:Acute kidney injuryBiomarkersCritical careIntensive careRenal insufficiencyRenal replacement therapySee more -
Case Reports
Immune reconstitution inflammatory syndrome as a cause of autoimmune hepatitis and acute liver failure
Rev Bras Ter Intensiva. 2017;29(3):382-385
Abstract
Case ReportsImmune reconstitution inflammatory syndrome as a cause of autoimmune hepatitis and acute liver failure
Rev Bras Ter Intensiva. 2017;29(3):382-385
DOI 10.5935/0103-507X.20170053
Views0ABSTRACT
Acute liver failure is a rare syndrome with high mortality and is often diagnosed late. Intensivist physicians play fundamental roles in the diagnostic suspicion and the management of the multiple-organic dysfunctions characteristic of this entity. Immune reconstitution inflammatory syndrome is an entity that is characterized by the paradoxical worsening of the patient’s previous condition, after the initiation of antiretrovirals, triggered against either pathogens present in the host or autoantigens. Autoimmune hepatitis has recently been described as one of these autoimmune manifestations. The authors report the first case with evolution to acute liver failure and death within a few days after the development of encephalopathy, review the cases of autoimmune hepatitis described and comment on the therapeutic possibilities in this context.
Keywords:Case reportsHepatitis, autoimmuneImmune reconstitution inflammatory syndromeLiver failure, acuteSee moreViews0Abstract
Case ReportsImmune reconstitution inflammatory syndrome as a cause of autoimmune hepatitis and acute liver failure
Rev Bras Ter Intensiva. 2017;29(3):382-385
DOI 10.5935/0103-507X.20170053
Views0ABSTRACT
Acute liver failure is a rare syndrome with high mortality and is often diagnosed late. Intensivist physicians play fundamental roles in the diagnostic suspicion and the management of the multiple-organic dysfunctions characteristic of this entity. Immune reconstitution inflammatory syndrome is an entity that is characterized by the paradoxical worsening of the patient’s previous condition, after the initiation of antiretrovirals, triggered against either pathogens present in the host or autoantigens. Autoimmune hepatitis has recently been described as one of these autoimmune manifestations. The authors report the first case with evolution to acute liver failure and death within a few days after the development of encephalopathy, review the cases of autoimmune hepatitis described and comment on the therapeutic possibilities in this context.
Keywords:Case reportsHepatitis, autoimmuneImmune reconstitution inflammatory syndromeLiver failure, acuteSee more -
Case Reports
Heart conduction system defects and sustained ventricular tachycardia complications in a patient with granulomatosis with polyangiitis. A case report and literature review
Rev Bras Ter Intensiva. 2017;29(3):386-390
Abstract
Case ReportsHeart conduction system defects and sustained ventricular tachycardia complications in a patient with granulomatosis with polyangiitis. A case report and literature review
Rev Bras Ter Intensiva. 2017;29(3):386-390
DOI 10.5935/0103-507X.20170052
Views0ABSTRACT
Granulomatosis with polyangiitis is a rare systemic inflammatory disorder characterized by vasculitis of the small arteries, the arterioles and the capillaries together with necrotizing granulomatous lesions. This case reports on a young female patient, previously diagnosed with granulomatosis with polyangiitis, who was admitted to the intensive care unit with seizures and hemodynamic instability due to a complete atrioventricular heart block. The event was associated with multiple episodes of sustained ventricular tachycardia without any structural heart changes or electrolyte disturbances. In the intensive care unit, the patient was fitted with a provisory pacemaker, followed by immunosuppression with corticosteroids and immunobiological therapy, resulting in a total hemodynamic improvement. Severe conduction disorders in patients presenting granulomatosis with polyangiitis are rare but can contribute to increased morbidity. Early detection and specific intervention can prevent unfavorable outcomes, specifically in the intensive care unit.
Keywords:Atrioventricular blockBradycardiaCase reportsGranulomatosis with polyangiitisHeart conduction systemPacemaker, artificialSee moreViews0Abstract
Case ReportsHeart conduction system defects and sustained ventricular tachycardia complications in a patient with granulomatosis with polyangiitis. A case report and literature review
Rev Bras Ter Intensiva. 2017;29(3):386-390
DOI 10.5935/0103-507X.20170052
Views0ABSTRACT
Granulomatosis with polyangiitis is a rare systemic inflammatory disorder characterized by vasculitis of the small arteries, the arterioles and the capillaries together with necrotizing granulomatous lesions. This case reports on a young female patient, previously diagnosed with granulomatosis with polyangiitis, who was admitted to the intensive care unit with seizures and hemodynamic instability due to a complete atrioventricular heart block. The event was associated with multiple episodes of sustained ventricular tachycardia without any structural heart changes or electrolyte disturbances. In the intensive care unit, the patient was fitted with a provisory pacemaker, followed by immunosuppression with corticosteroids and immunobiological therapy, resulting in a total hemodynamic improvement. Severe conduction disorders in patients presenting granulomatosis with polyangiitis are rare but can contribute to increased morbidity. Early detection and specific intervention can prevent unfavorable outcomes, specifically in the intensive care unit.
Keywords:Atrioventricular blockBradycardiaCase reportsGranulomatosis with polyangiitisHeart conduction systemPacemaker, artificialSee more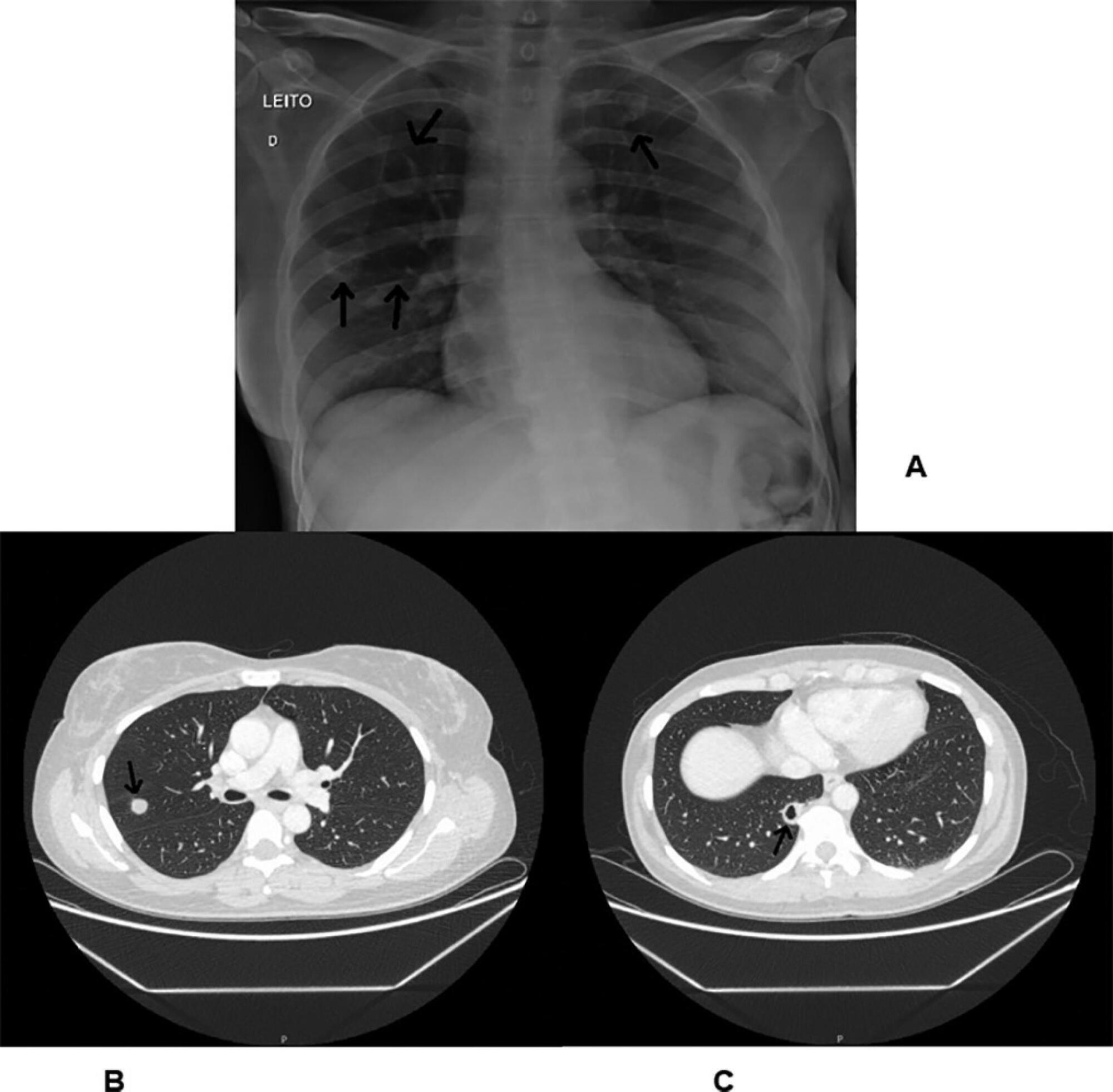
-
Brief Communication
Influence of dentistry professionals and oral health assistance protocols on intensive care unit nursing staff. A survey study
Rev Bras Ter Intensiva. 2017;29(3):391-393
Abstract
Brief CommunicationInfluence of dentistry professionals and oral health assistance protocols on intensive care unit nursing staff. A survey study
Rev Bras Ter Intensiva. 2017;29(3):391-393
DOI 10.5935/0103-507X.20170049
Views0INTRODUCTIONPatients admitted to intensive care units (ICU) often lack oral health assistance,(–) with a direct influence on oral health problems related to higher morbidity and mortality. Poor oral health can lead to clinical problems such as locally spreading infections, respiratory tract infections, higher costs of ICU admissions, and higher use of medications such as antibiotics, […]See moreViews0Abstract
Brief CommunicationInfluence of dentistry professionals and oral health assistance protocols on intensive care unit nursing staff. A survey study
Rev Bras Ter Intensiva. 2017;29(3):391-393
DOI 10.5935/0103-507X.20170049
Views0INTRODUCTIONPatients admitted to intensive care units (ICU) often lack oral health assistance,(–) with a direct influence on oral health problems related to higher morbidity and mortality. Poor oral health can lead to clinical problems such as locally spreading infections, respiratory tract infections, higher costs of ICU admissions, and higher use of medications such as antibiotics, […]See more -
Letters to the Editor
Oral histoplasmosis
Rev Bras Ter Intensiva. 2017;29(3):394-396
Abstract
Letters to the EditorOral histoplasmosis
Rev Bras Ter Intensiva. 2017;29(3):394-396
DOI 10.5935/0103-507X.20170057
Views0To the editor,Histoplasmosis is an opportunistic fungal infection, endemic to Latin America, that is caused by Histoplasma capsulatum. This infection mostly occurs in the lungs() and is frequently associated with AIDS.() Sometimes, histoplasmosis is misinterpreted with tuberculosis due to their clinical similarities.(,) Oral involvement is very rare in histoplasmosis, being associated only with its disseminated […]See moreViews0Abstract
Letters to the EditorOral histoplasmosis
Rev Bras Ter Intensiva. 2017;29(3):394-396
DOI 10.5935/0103-507X.20170057
Views0To the editor,Histoplasmosis is an opportunistic fungal infection, endemic to Latin America, that is caused by Histoplasma capsulatum. This infection mostly occurs in the lungs() and is frequently associated with AIDS.() Sometimes, histoplasmosis is misinterpreted with tuberculosis due to their clinical similarities.(,) Oral involvement is very rare in histoplasmosis, being associated only with its disseminated […]See more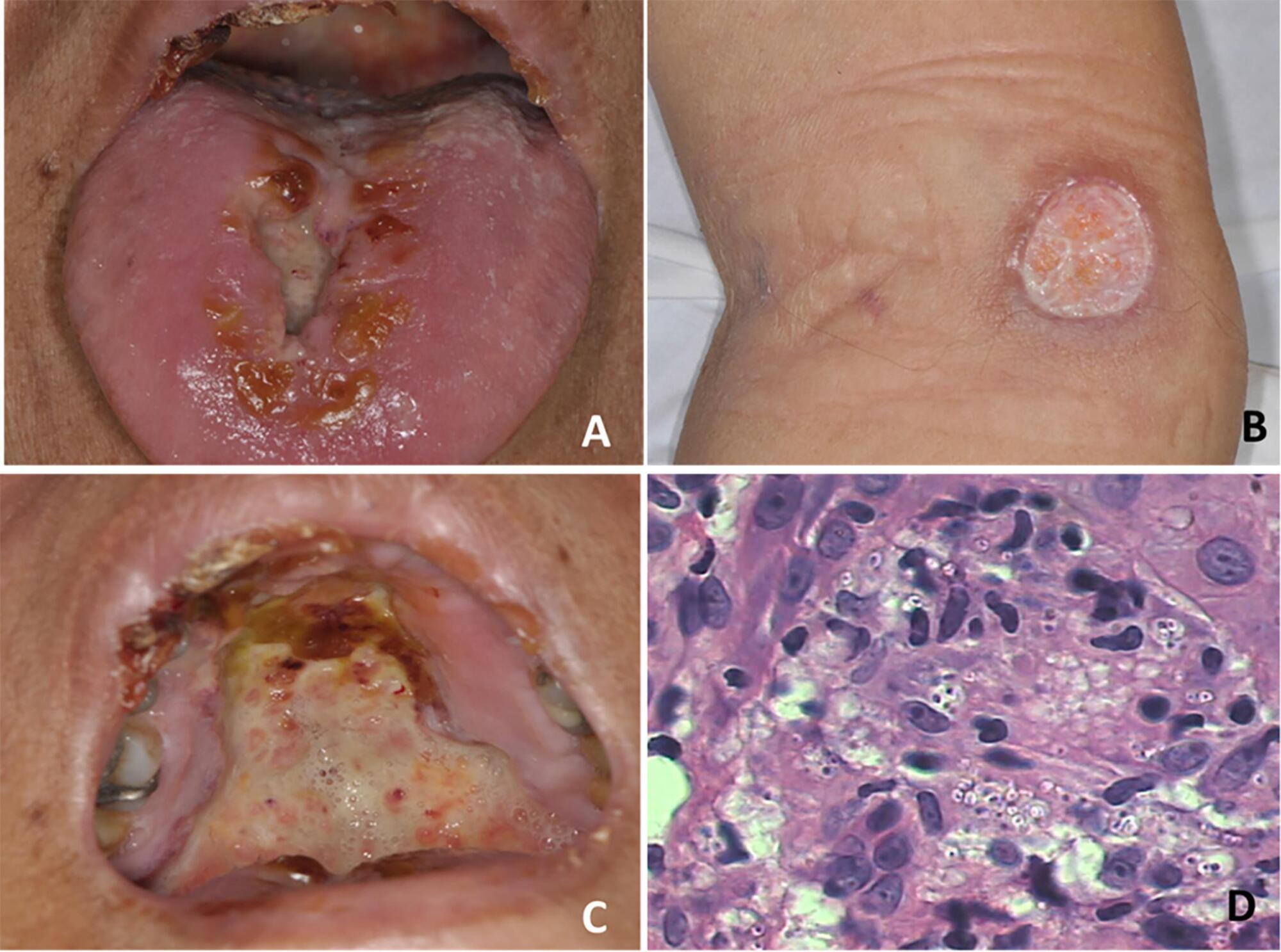
-
Letters to the Editor
Accidental breakage of needle during subclavian vein catheterization: an adversity uncalled for!
Rev Bras Ter Intensiva. 2017;29(3):397-398
Abstract
Letters to the EditorAccidental breakage of needle during subclavian vein catheterization: an adversity uncalled for!
Rev Bras Ter Intensiva. 2017;29(3):397-398
DOI 10.5935/0103-507X.20170056
Views0To the editor,Central venous catheter (CVC) placement is an essential component of modern-day critical care. Its use was first documented by Werner Forssman in 1929, and Seldinger perfected the technique in 1953.() Although CVC insertion is a routine practice, it is not devoid of complications. We report a rare event in which the introducer needle […]See moreViews0Abstract
Letters to the EditorAccidental breakage of needle during subclavian vein catheterization: an adversity uncalled for!
Rev Bras Ter Intensiva. 2017;29(3):397-398
DOI 10.5935/0103-507X.20170056
Views0To the editor,Central venous catheter (CVC) placement is an essential component of modern-day critical care. Its use was first documented by Werner Forssman in 1929, and Seldinger perfected the technique in 1953.() Although CVC insertion is a routine practice, it is not devoid of complications. We report a rare event in which the introducer needle […]See more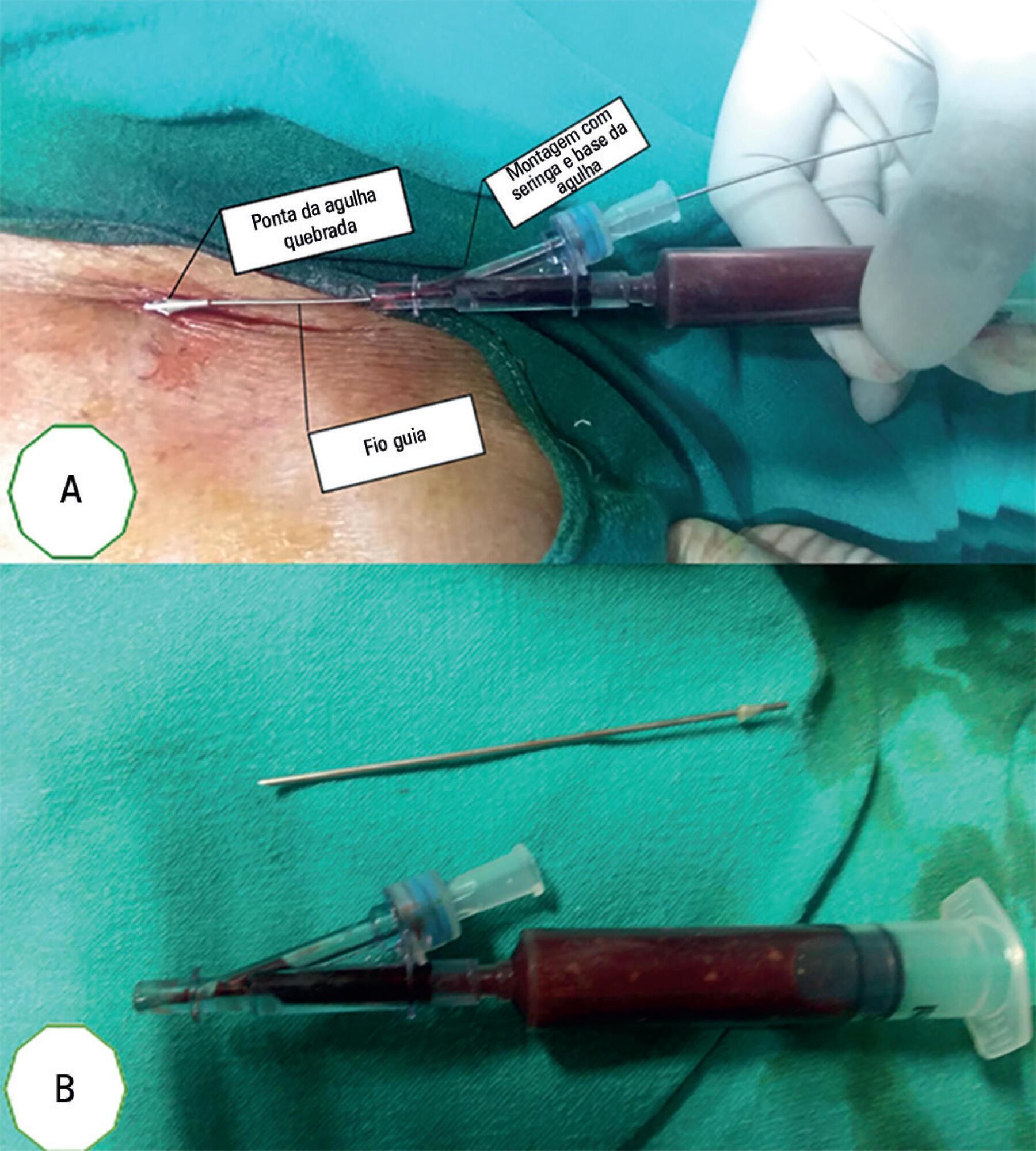
Volume Articles - Critical Care Science (CCS)
