Influenza A virus, H1N1 subtype Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2017;29(3):271-278
DOI 10.5935/0103-507X.20170048
This report aimed to describe the outcomes of the patients with severe H1N1 associated acute respiratory distress syndrome who were treated with extracorporeal membrane oxygenation therapy.
This retrospective review analyzed a single-center cohort of adult patients with H1N1-related acute respiratory distress syndrome who were managed with veno-venous extracorporeal membrane oxygenation during the winter of 2013/2014.
A total of 10 patients received veno-venous extracorporeal membrane oxygenation for H1N1 influenza between January 2013 and March 2014. Seven patients were transferred to our center for extracorporeal membrane oxygenation consideration (all within 72 hours of initiating mechanical ventilation). The median patient age was forty years, and 30% were female. The median arterial oxygen partial pressure to fraction of inspired oxygen ratio was 62.5, and the median RESP score was 6. Three patients received inhaled nitric oxide, and four patients were proned as rescue therapy before extracorporeal membrane oxygenation was initiated. The median duration of mechanical ventilation was twenty-two days (range, 14 - 32). The median length of stay in the intensive care unit was twenty-seven days (range, 14 - 39). The median hospital length of stay was 29.1 days (range, 16.0 - 46.9). Minor bleeding complications occurred in 6 of 10 patients. Eight of the ten patients survived to hospital discharge.
The survivors were relatively young and discharged with good functional status (i.e., enhancing quality-adjusted life-years-saved). Our experience shows that even a relatively new extracorporeal membrane oxygenation program can play an important role in that capacity and provide excellent outcomes for the sickest patients.
Abstract
Rev Bras Ter Intensiva. 2017;29(3):271-278
DOI 10.5935/0103-507X.20170048
This report aimed to describe the outcomes of the patients with severe H1N1 associated acute respiratory distress syndrome who were treated with extracorporeal membrane oxygenation therapy.
This retrospective review analyzed a single-center cohort of adult patients with H1N1-related acute respiratory distress syndrome who were managed with veno-venous extracorporeal membrane oxygenation during the winter of 2013/2014.
A total of 10 patients received veno-venous extracorporeal membrane oxygenation for H1N1 influenza between January 2013 and March 2014. Seven patients were transferred to our center for extracorporeal membrane oxygenation consideration (all within 72 hours of initiating mechanical ventilation). The median patient age was forty years, and 30% were female. The median arterial oxygen partial pressure to fraction of inspired oxygen ratio was 62.5, and the median RESP score was 6. Three patients received inhaled nitric oxide, and four patients were proned as rescue therapy before extracorporeal membrane oxygenation was initiated. The median duration of mechanical ventilation was twenty-two days (range, 14 - 32). The median length of stay in the intensive care unit was twenty-seven days (range, 14 - 39). The median hospital length of stay was 29.1 days (range, 16.0 - 46.9). Minor bleeding complications occurred in 6 of 10 patients. Eight of the ten patients survived to hospital discharge.
The survivors were relatively young and discharged with good functional status (i.e., enhancing quality-adjusted life-years-saved). Our experience shows that even a relatively new extracorporeal membrane oxygenation program can play an important role in that capacity and provide excellent outcomes for the sickest patients.
Abstract
Rev Bras Ter Intensiva. 2013;25(2):123-129
DOI 10.5935/0103-507X.20130023
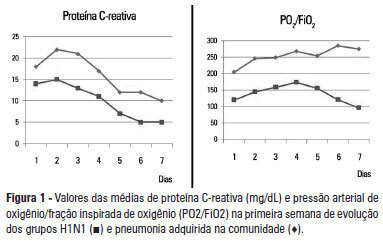
OBJECTIVE: To analyze the clinical, laboratory and evolution data of patients with severe influenza A H1N1 pneumonia and compare the data with that of patients with severe community-acquired bacterial pneumonia. METHODS: Cohort and retrospective study. All patients admitted to the intensive care unit between May 2009 and December 2010 with a diagnosis of severe pneumonia caused by the influenza A H1N1 virus were included in the study. Thirty patients with severe community-acquired pneumonia admitted within the same period were used as a control group. Severe community-acquired pneumonia was defined as the presence of at least one major severity criteria (ventilator or vasopressor use) or two minor criteria. RESULTS: The data of 45 patients were evaluated. Of these patients, 15 were infected with H1N1. When compared to the group with community-acquired pneumonia, patients from the H1N1 group had significantly lower leukocyte counts on admission (6,728±4,070 versus 16,038±7,863; p<0.05) and lower C-reactive protein levels (Day 2: 15.1±8.1 versus 22.1±10.9 mg/dL; p<0.05). The PaO2/FiO2 ratio values were lower in the first week in patients with H1N1. Patients who did not survive the H1N1 severe pneumonia had significantly higher levels of C-reactive protein and higher serum creatinine levels compared with patients who survived. The mortality rate was significantly higher in the H1N1 group than in the control group (53% versus 20%; p=0.056, respectivelly). CONCLUSION: Differences in the leukocyte count, C-reactive protein concentrations and oxygenation profiles may contribute to the diagnosis and prognosis of patients with severe influenza A H1N1 virus-related pneumonia and community-acquired pneumonia.
Abstract
Rev Bras Ter Intensiva. 2013;25(2):123-129
DOI 10.5935/0103-507X.20130023
OBJECTIVE: To analyze the clinical, laboratory and evolution data of patients with severe influenza A H1N1 pneumonia and compare the data with that of patients with severe community-acquired bacterial pneumonia. METHODS: Cohort and retrospective study. All patients admitted to the intensive care unit between May 2009 and December 2010 with a diagnosis of severe pneumonia caused by the influenza A H1N1 virus were included in the study. Thirty patients with severe community-acquired pneumonia admitted within the same period were used as a control group. Severe community-acquired pneumonia was defined as the presence of at least one major severity criteria (ventilator or vasopressor use) or two minor criteria. RESULTS: The data of 45 patients were evaluated. Of these patients, 15 were infected with H1N1. When compared to the group with community-acquired pneumonia, patients from the H1N1 group had significantly lower leukocyte counts on admission (6,728±4,070 versus 16,038±7,863; p<0.05) and lower C-reactive protein levels (Day 2: 15.1±8.1 versus 22.1±10.9 mg/dL; p<0.05). The PaO2/FiO2 ratio values were lower in the first week in patients with H1N1. Patients who did not survive the H1N1 severe pneumonia had significantly higher levels of C-reactive protein and higher serum creatinine levels compared with patients who survived. The mortality rate was significantly higher in the H1N1 group than in the control group (53% versus 20%; p=0.056, respectivelly). CONCLUSION: Differences in the leukocyte count, C-reactive protein concentrations and oxygenation profiles may contribute to the diagnosis and prognosis of patients with severe influenza A H1N1 virus-related pneumonia and community-acquired pneumonia.
Abstract
Rev Bras Ter Intensiva. 2010;22(4):333-338
DOI 10.1590/S0103-507X2010000400004
OBJECTIVES: To describe the clinical features and outcomes of patients admitted with influenza A (H1N1) infection in two private hospitals' intensive care units in São Paulo, Brazil, during the 2009 pandemics. METHODS: A retrospective cohort study was conducted to evaluate demographic data, initial clinical presentation, prognostic scores [Simplified Acute Physiology Score (SAPS) 3 and Sequential Organ Failure Assessment (SOFA)], comorbidities, outcomes and treatment of patients with confirmed pandemic influenza diagnosis from July to September 2009. RESULTS: 22 patients were admitted. Median age was 30 (25-43.5) years. Median SAPS 3 and SOFA were 42 (37-49) and 2 (1-3.5), respectively. Comorbidities were common (45.4%), especially obesity (22.7%). Two (9.1%) patients were pregnant. Five (22.7%) patients required invasive mechanical ventilation, with high positive end expiratory pressures (median of 16 cmH2O, interquartile range 10-25cmH2O). There was a 50% incidence of non-invasive ventilation failure. Most (77.2%) of patients were treated with oseltamivir. Hospital mortality was 4.5%. Initial SAPS 3, SOFA and PaO2/FiO2 ratio were associated with mechanical ventilation requirement (p<0.01). CONCLUSIONS: Pandemic influenza infection mainly affected young and obese patients. In this study, patients were less severe than those previously described, what explains our low mortality and mechanical ventilation needs. However, high positive end expiratory pressures were required for mechanically ventilated patients.
Abstract
Rev Bras Ter Intensiva. 2010;22(4):333-338
DOI 10.1590/S0103-507X2010000400004
OBJECTIVES: To describe the clinical features and outcomes of patients admitted with influenza A (H1N1) infection in two private hospitals' intensive care units in São Paulo, Brazil, during the 2009 pandemics. METHODS: A retrospective cohort study was conducted to evaluate demographic data, initial clinical presentation, prognostic scores [Simplified Acute Physiology Score (SAPS) 3 and Sequential Organ Failure Assessment (SOFA)], comorbidities, outcomes and treatment of patients with confirmed pandemic influenza diagnosis from July to September 2009. RESULTS: 22 patients were admitted. Median age was 30 (25-43.5) years. Median SAPS 3 and SOFA were 42 (37-49) and 2 (1-3.5), respectively. Comorbidities were common (45.4%), especially obesity (22.7%). Two (9.1%) patients were pregnant. Five (22.7%) patients required invasive mechanical ventilation, with high positive end expiratory pressures (median of 16 cmH2O, interquartile range 10-25cmH2O). There was a 50% incidence of non-invasive ventilation failure. Most (77.2%) of patients were treated with oseltamivir. Hospital mortality was 4.5%. Initial SAPS 3, SOFA and PaO2/FiO2 ratio were associated with mechanical ventilation requirement (p<0.01). CONCLUSIONS: Pandemic influenza infection mainly affected young and obese patients. In this study, patients were less severe than those previously described, what explains our low mortality and mechanical ventilation needs. However, high positive end expiratory pressures were required for mechanically ventilated patients.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (116) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)