Stevens Johnson Syndrome Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2017;29(4):499-508
DOI 10.5935/0103-507X.20170075
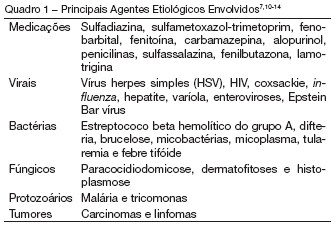
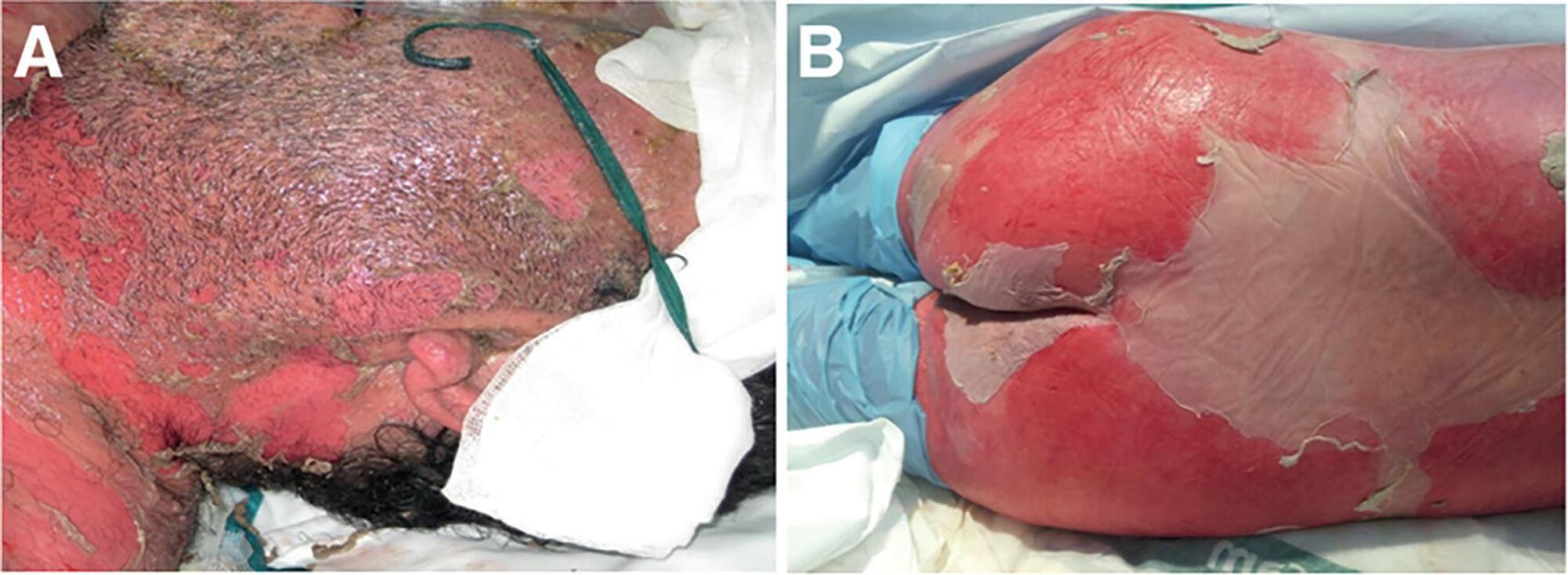
Toxic epidermal necrolysis is an adverse immunological skin reaction secondary in most cases to the administration of a drug. Toxic epidermal necrolysis, Stevens-Johnson syndrome, and multiform exudative erythema are part of the same disease spectrum. The mortality rate from toxic epidermal necrolysis is approximately 30%. The pathophysiology of toxic epidermal necrolysis is similar in many respects to that of superficial skin burns. Mucosal involvement of the ocular and genital epithelium is associated with serious sequelae if the condition is not treated early. It is generally accepted that patients with toxic epidermal necrolysis are better treated in burn units, which are experienced in the management of patients with extensive skin loss. Treatment includes support, elimination, and coverage with biosynthetic derivatives of the skin in affected areas, treatment of mucosal involvement, and specific immunosuppressive treatment. Of the treatments tested, only immunoglobulin G and cyclosporin A are currently used in most centers, even though there is no solid evidence to recommend any specific treatment. The particular aspects of the treatment of this disease include the prevention of sequelae related to the formation of synechiae, eye care to prevent serious sequelae that can lead to blindness, and specific immunosuppressive treatment. Better knowledge of the management principles of toxic epidermal necrolysis will lead to better disease management, higher survival rates, and lower prevalence of sequelae.
Abstract
Rev Bras Ter Intensiva. 2017;29(4):499-508
DOI 10.5935/0103-507X.20170075
Toxic epidermal necrolysis is an adverse immunological skin reaction secondary in most cases to the administration of a drug. Toxic epidermal necrolysis, Stevens-Johnson syndrome, and multiform exudative erythema are part of the same disease spectrum. The mortality rate from toxic epidermal necrolysis is approximately 30%. The pathophysiology of toxic epidermal necrolysis is similar in many respects to that of superficial skin burns. Mucosal involvement of the ocular and genital epithelium is associated with serious sequelae if the condition is not treated early. It is generally accepted that patients with toxic epidermal necrolysis are better treated in burn units, which are experienced in the management of patients with extensive skin loss. Treatment includes support, elimination, and coverage with biosynthetic derivatives of the skin in affected areas, treatment of mucosal involvement, and specific immunosuppressive treatment. Of the treatments tested, only immunoglobulin G and cyclosporin A are currently used in most centers, even though there is no solid evidence to recommend any specific treatment. The particular aspects of the treatment of this disease include the prevention of sequelae related to the formation of synechiae, eye care to prevent serious sequelae that can lead to blindness, and specific immunosuppressive treatment. Better knowledge of the management principles of toxic epidermal necrolysis will lead to better disease management, higher survival rates, and lower prevalence of sequelae.
Abstract
Rev Bras Ter Intensiva. 2006;18(3):292-297
DOI 10.1590/S0103-507X2006000300012
BACKGROUND AND OBJECTIVES: The Stevens Johnson Syndrome (SJS) and Toxical Epidermal Necrolisys (TEN) are important skin and mucosal lesions that need intensive care treatment. The aim of this article is to show a literature review about SJS and TEN. CONTENTS: This article reviews the concepts, diagnostic topics, clinical presentation and the principle of basic treatment in Intensive Care Unit for SJS and TEN. CONCLUSIONS: These illnesses are characterized as dermatological emergencies and its adequate management and cares must be part of the routine knowledge of the intensive care doctors.
Abstract
Rev Bras Ter Intensiva. 2006;18(3):292-297
DOI 10.1590/S0103-507X2006000300012
BACKGROUND AND OBJECTIVES: The Stevens Johnson Syndrome (SJS) and Toxical Epidermal Necrolisys (TEN) are important skin and mucosal lesions that need intensive care treatment. The aim of this article is to show a literature review about SJS and TEN. CONTENTS: This article reviews the concepts, diagnostic topics, clinical presentation and the principle of basic treatment in Intensive Care Unit for SJS and TEN. CONCLUSIONS: These illnesses are characterized as dermatological emergencies and its adequate management and cares must be part of the routine knowledge of the intensive care doctors.