pregnancy Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2018;30(4):508-511
DOI 10.5935/0103-507X.20180072
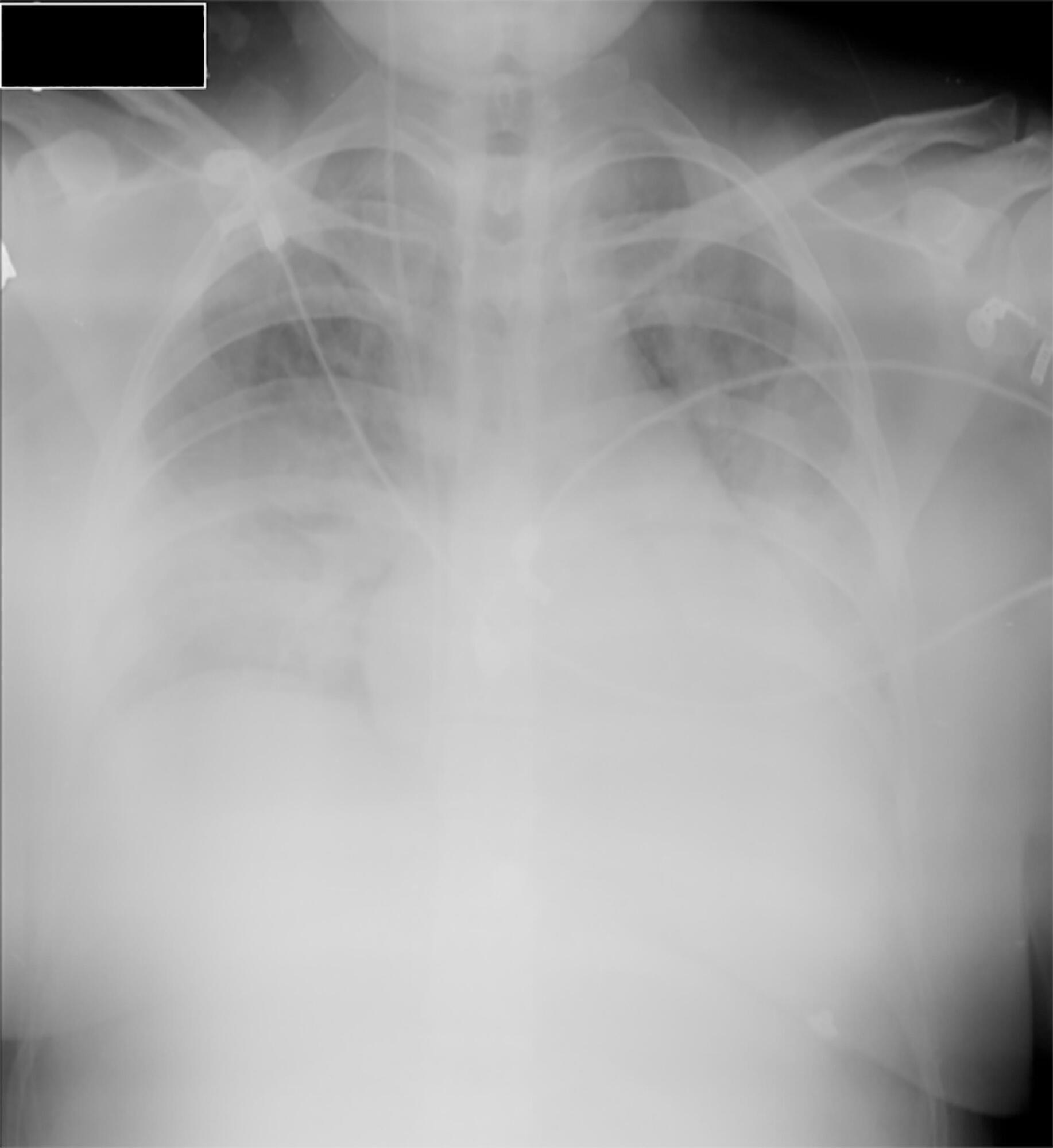
Little evidence exists to support the use of noninvasive mechanical ventilation for acute hypoxemic respiratory failure. However, considering the complications associated with endotracheal intubation, we attempted to implement noninvasive mechanical ventilation in a 24-year-old patient who was 32 weeks pregnant and was admitted to the intensive care unit with acute hypoxemic respiratory failure and sepsis secondary to a urinary tract infection. Lack of tolerance to noninvasive mechanical ventilation led us to use an alternative method to avoid endotracheal intubation. The use of high-flow nasal cannula allowed to overcome this situation, wich supports this technique as a treatment option for critical obstetric patients that is safe for both the mother and fetus.
Abstract
Rev Bras Ter Intensiva. 2018;30(4):508-511
DOI 10.5935/0103-507X.20180072
Little evidence exists to support the use of noninvasive mechanical ventilation for acute hypoxemic respiratory failure. However, considering the complications associated with endotracheal intubation, we attempted to implement noninvasive mechanical ventilation in a 24-year-old patient who was 32 weeks pregnant and was admitted to the intensive care unit with acute hypoxemic respiratory failure and sepsis secondary to a urinary tract infection. Lack of tolerance to noninvasive mechanical ventilation led us to use an alternative method to avoid endotracheal intubation. The use of high-flow nasal cannula allowed to overcome this situation, wich supports this technique as a treatment option for critical obstetric patients that is safe for both the mother and fetus.
Abstract
Rev Bras Ter Intensiva. 2013;25(2):175-180
DOI 10.5935/0103-507X.20130030
Preeclampsia, HELLP syndrome (hemolysis, elevated liver enzymes, and low-platelet count), and acute fatty liver of pregnancy are the main causes of thrombotic microangiopathy and evere liver dysfunction during pregnancy and represent different manifestations of the same pathological continuum. The case of a 35-week pregnant woman who was admitted to an intensive care unit immediately after a Cesarean section due to fetal death and the presence of nausea, vomiting, and jaundice is reported. Postpartum preeclampsia and acute fatty liver of pregnancy were diagnosed. The patient developed an acute subdural hematoma and an intracerebral hemorrhage, which were subjected to neurosurgical treatment. The patient died from refractory hemolytic anemia and spontaneous bleeding of multiple organs. Preeclampsia HELLP syndrome, and acute fatty liver of pregnancy might overlap and be associated with potentially fatal complications, including intracranial hemorrhage, as in the present case. Early detection and diagnosis are crucial to ensure management and treatment success.
Abstract
Rev Bras Ter Intensiva. 2013;25(2):175-180
DOI 10.5935/0103-507X.20130030
Preeclampsia, HELLP syndrome (hemolysis, elevated liver enzymes, and low-platelet count), and acute fatty liver of pregnancy are the main causes of thrombotic microangiopathy and evere liver dysfunction during pregnancy and represent different manifestations of the same pathological continuum. The case of a 35-week pregnant woman who was admitted to an intensive care unit immediately after a Cesarean section due to fetal death and the presence of nausea, vomiting, and jaundice is reported. Postpartum preeclampsia and acute fatty liver of pregnancy were diagnosed. The patient developed an acute subdural hematoma and an intracerebral hemorrhage, which were subjected to neurosurgical treatment. The patient died from refractory hemolytic anemia and spontaneous bleeding of multiple organs. Preeclampsia HELLP syndrome, and acute fatty liver of pregnancy might overlap and be associated with potentially fatal complications, including intracranial hemorrhage, as in the present case. Early detection and diagnosis are crucial to ensure management and treatment success.
Abstract
Rev Bras Ter Intensiva. 2013;25(4):334-344
DOI 10.5935/0103-507X.20130056
Sepsis is defined as an acute inflammatory response syndrome secondary to an infectious focus. It has a high incidence, morbidity and mortality, causing substantial financial costs, especially due to complications such as septic shock and multiple organ dysfunction. The pathogen toxins associated with individual susceptibility culminate with cytokine release, which promotes a systemic inflammatory response that can progress to multiple organ dysfunction and eventual patient death.
Specifically, sepsis incidence, morbidity and mortality are lower in pregnant women, as this group is typically younger with fewer comorbidities having a polymicrobial etiology resulting in sepsis.
Pregnant women exhibit physiological characteristics that may confer specific clinical presentation and laboratory patterns during the sepsis course. Thus, a better understanding of these changes is critical for better identification and management of these patients. The presence of a fetus also requires unique approaches in a pregnant woman with sepsis.
Sepsis treatment is based on certain guidelines that were established after major clinical trials, which, unfortunately, all classified pregnancy as a exclusion criteria.
Thus, the treatment of sepsis in the general population has been extrapolated to the pregnant population, with the following main goals: maintenance of tissue perfusion with fluid replacement and vasoactive drugs (initial resuscitation), adequate oxygenation, control of the infection source and an early start of antibiotic therapy, corticosteroid infusion and blood transfusion when properly indicated, prophylaxis, and specifically monitoring and maintenance of fetal heath.
Abstract
Rev Bras Ter Intensiva. 2013;25(4):334-344
DOI 10.5935/0103-507X.20130056
Sepsis is defined as an acute inflammatory response syndrome secondary to an infectious focus. It has a high incidence, morbidity and mortality, causing substantial financial costs, especially due to complications such as septic shock and multiple organ dysfunction. The pathogen toxins associated with individual susceptibility culminate with cytokine release, which promotes a systemic inflammatory response that can progress to multiple organ dysfunction and eventual patient death.
Specifically, sepsis incidence, morbidity and mortality are lower in pregnant women, as this group is typically younger with fewer comorbidities having a polymicrobial etiology resulting in sepsis.
Pregnant women exhibit physiological characteristics that may confer specific clinical presentation and laboratory patterns during the sepsis course. Thus, a better understanding of these changes is critical for better identification and management of these patients. The presence of a fetus also requires unique approaches in a pregnant woman with sepsis.
Sepsis treatment is based on certain guidelines that were established after major clinical trials, which, unfortunately, all classified pregnancy as a exclusion criteria.
Thus, the treatment of sepsis in the general population has been extrapolated to the pregnant population, with the following main goals: maintenance of tissue perfusion with fluid replacement and vasoactive drugs (initial resuscitation), adequate oxygenation, control of the infection source and an early start of antibiotic therapy, corticosteroid infusion and blood transfusion when properly indicated, prophylaxis, and specifically monitoring and maintenance of fetal heath.
Abstract
Rev Bras Ter Intensiva. 2007;19(2):237-241
DOI 10.1590/S0103-507X2007000200017
BACKGROUND AND OBJECTIVES: Amniotic fluid embolism is a rare complication of pregnancy whose physiopathology is not completely known and still not frequently remembered by intensive care physicians and obstetricians. The main aim of this case report was to emphasize the need of better knowledge of this disease by physicians. CASE REPORT: A 15 years old, primigravida, 35th week of gestation was admitted in our intensive care unit (ICU) with a sudden respiratory distress. Soon after admission she was intubated and put on mechanical ventilation. After stabilization she was transferred to the operating room and a cesarean section was undertaken. During the operation, instead of fluid reposition with crystalloids in large amounts, her hemodynamic status deteriorated and it was necessary to use vasoactive drugs. After three days on mechanical ventilation she was successfully weaned and discharged from the intensive care unit (ICU) after 6 days. She and her baby were discharged from hospital on13th day of hospitalization. CONCLUSIONS: Amniotic fluid embolism is a rare and catastrophic complication of pregnancy, at least in its classic presentation. It is characterized by acute respiratory distress, hemodynamic compromise and coagulopathy that occur during or within 30 min after labor. Diagnosis is by exclusion of other conditions of pregnancy or diseases that can be aggravated during pregnancy such as eclampsia, sepsis, pos-partum cardiomyopathy, anaphylaxis, pulmonary thromboembolism, transfusion reactions, anesthetic complications and mitral stenosis. There is growing evidence that we have a spectrum of manifestation which can be more common that in the classic ones. The treatment is supportive of vital functions, such as mechanical ventilation, fluid reposition, vasoactive drugs and fresh frozen plasma as necessary. The intensive care physicians and obstetricians should be aware of this disease in order to make early diagnosis and prompt treatment.
Abstract
Rev Bras Ter Intensiva. 2007;19(2):237-241
DOI 10.1590/S0103-507X2007000200017
BACKGROUND AND OBJECTIVES: Amniotic fluid embolism is a rare complication of pregnancy whose physiopathology is not completely known and still not frequently remembered by intensive care physicians and obstetricians. The main aim of this case report was to emphasize the need of better knowledge of this disease by physicians. CASE REPORT: A 15 years old, primigravida, 35th week of gestation was admitted in our intensive care unit (ICU) with a sudden respiratory distress. Soon after admission she was intubated and put on mechanical ventilation. After stabilization she was transferred to the operating room and a cesarean section was undertaken. During the operation, instead of fluid reposition with crystalloids in large amounts, her hemodynamic status deteriorated and it was necessary to use vasoactive drugs. After three days on mechanical ventilation she was successfully weaned and discharged from the intensive care unit (ICU) after 6 days. She and her baby were discharged from hospital on13th day of hospitalization. CONCLUSIONS: Amniotic fluid embolism is a rare and catastrophic complication of pregnancy, at least in its classic presentation. It is characterized by acute respiratory distress, hemodynamic compromise and coagulopathy that occur during or within 30 min after labor. Diagnosis is by exclusion of other conditions of pregnancy or diseases that can be aggravated during pregnancy such as eclampsia, sepsis, pos-partum cardiomyopathy, anaphylaxis, pulmonary thromboembolism, transfusion reactions, anesthetic complications and mitral stenosis. There is growing evidence that we have a spectrum of manifestation which can be more common that in the classic ones. The treatment is supportive of vital functions, such as mechanical ventilation, fluid reposition, vasoactive drugs and fresh frozen plasma as necessary. The intensive care physicians and obstetricians should be aware of this disease in order to make early diagnosis and prompt treatment.
Abstract
Rev Bras Ter Intensiva. 2007;19(2):242-244
DOI 10.1590/S0103-507X2007000200018
BACKGROUND AND OBJECTIVES: Sepsis during pregnancy is a rare complication. This potentially fatal disease often occurs due to maternal infectious and can lead to fetal loss. Therefore, any attempted treatment must be aimed at the mother’s well being. As a matter of fact, there are few recent medical publications about sepsis in pregnancy. In spite of this, the treatment based on Surviving Sepsis Campaign seems suitable and practical. The aim of this article is making a case report highlighting a very well succeeded treatment of a pregnant woman with urinary sepsis. CASE REPORT: A 22 year old in her 27th week of pregnancy is hospitalized with pyelonefhritis. One day later, she begins presenting signs of sepsis and unresponsive hypoxemia, resulting in intubation. Afterwards, she evolved with persistent low blood pressure that was unresponsive to volume expansion and had to be put on vasopressor medication. She received intensive care support based on Surviving Sepsis Campaign. The patient evolved with an important improvement of her ventilatory stats and was extubated. After completing antibiotic treatment, she was discharged and delivered a healthy baby after 42 weeks pregnancy. CONCLUSIONS: Sepsis in pregnancy is a rare and potentially fatal complication. The main treatment is based on Surviving Sepsis Campaign. The patient had an outstanding improvement and overcame her condition after intensive care support.
Abstract
Rev Bras Ter Intensiva. 2007;19(2):242-244
DOI 10.1590/S0103-507X2007000200018
BACKGROUND AND OBJECTIVES: Sepsis during pregnancy is a rare complication. This potentially fatal disease often occurs due to maternal infectious and can lead to fetal loss. Therefore, any attempted treatment must be aimed at the mother’s well being. As a matter of fact, there are few recent medical publications about sepsis in pregnancy. In spite of this, the treatment based on Surviving Sepsis Campaign seems suitable and practical. The aim of this article is making a case report highlighting a very well succeeded treatment of a pregnant woman with urinary sepsis. CASE REPORT: A 22 year old in her 27th week of pregnancy is hospitalized with pyelonefhritis. One day later, she begins presenting signs of sepsis and unresponsive hypoxemia, resulting in intubation. Afterwards, she evolved with persistent low blood pressure that was unresponsive to volume expansion and had to be put on vasopressor medication. She received intensive care support based on Surviving Sepsis Campaign. The patient evolved with an important improvement of her ventilatory stats and was extubated. After completing antibiotic treatment, she was discharged and delivered a healthy baby after 42 weeks pregnancy. CONCLUSIONS: Sepsis in pregnancy is a rare and potentially fatal complication. The main treatment is based on Surviving Sepsis Campaign. The patient had an outstanding improvement and overcame her condition after intensive care support.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (116) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)