myocardial infarction Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2019;31(1):93-105
DOI 10.5935/0103-507X.20190001
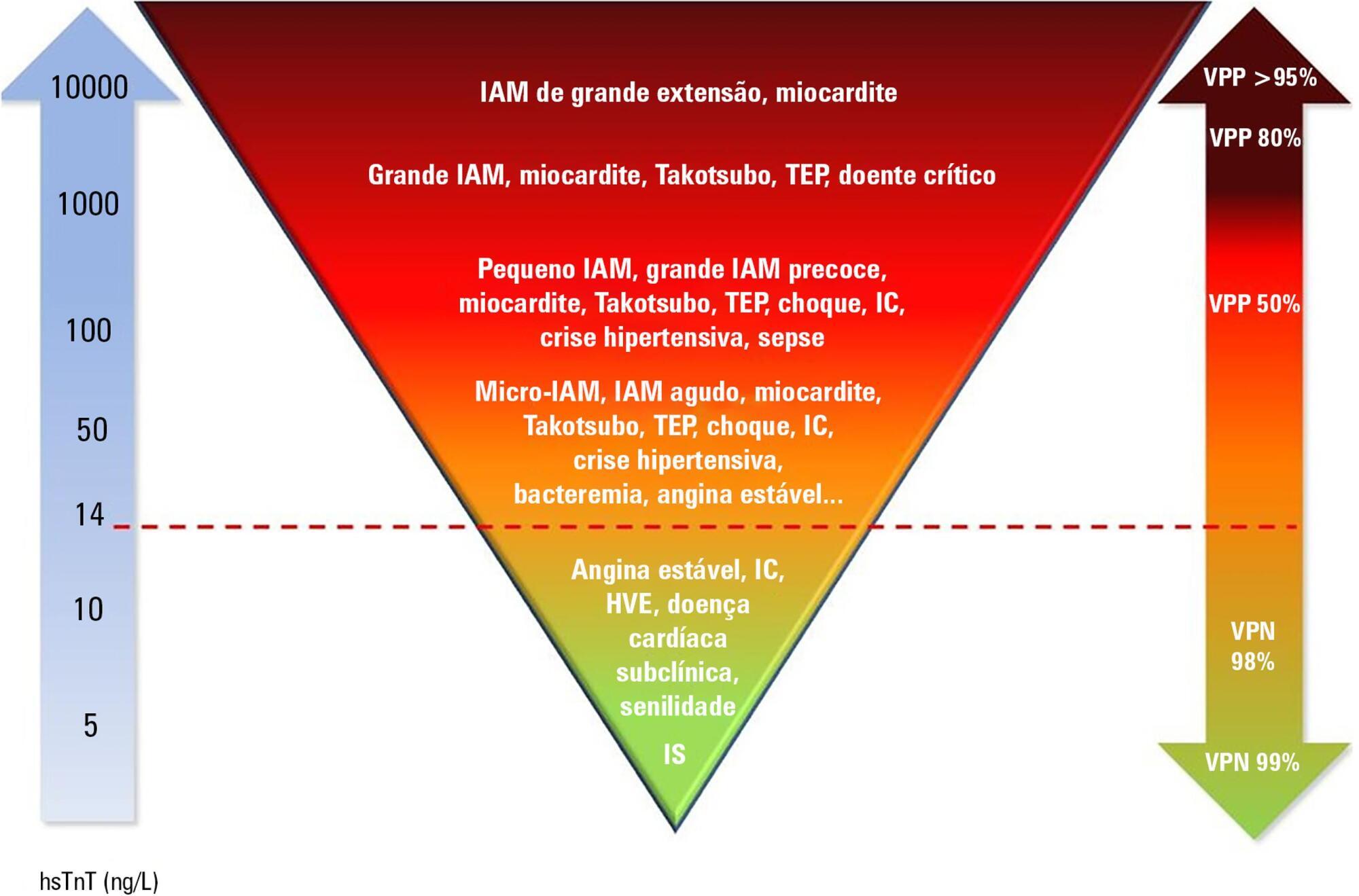
Cardiac troponins T and I are considered highly sensitive and specific markers for the diagnosis of acute myocardial infarction. Currently, a series of nonprimary cardiac abnormalities may manifest as an elevation in high-sensitive assays. The reduction in their detection limits has allowed earlier diagnosis and the use of evidence-based therapeutic measures; however, this characteristic has increased the spectrum of detectable noncoronary heart diseases, which poses challenges for characterizing acute coronary syndromes and creates a new role for these tests in known disorders in intensive care units, especially sepsis. Management of patients through a greater understanding of how these markers behave should be re-evaluated to ensure their correct interpretation.
Abstract
Rev Bras Ter Intensiva. 2019;31(1):93-105
DOI 10.5935/0103-507X.20190001
Cardiac troponins T and I are considered highly sensitive and specific markers for the diagnosis of acute myocardial infarction. Currently, a series of nonprimary cardiac abnormalities may manifest as an elevation in high-sensitive assays. The reduction in their detection limits has allowed earlier diagnosis and the use of evidence-based therapeutic measures; however, this characteristic has increased the spectrum of detectable noncoronary heart diseases, which poses challenges for characterizing acute coronary syndromes and creates a new role for these tests in known disorders in intensive care units, especially sepsis. Management of patients through a greater understanding of how these markers behave should be re-evaluated to ensure their correct interpretation.
Abstract
Rev Bras Ter Intensiva. 2014;26(1):71-76
DOI 10.5935/0103-507X.20140011
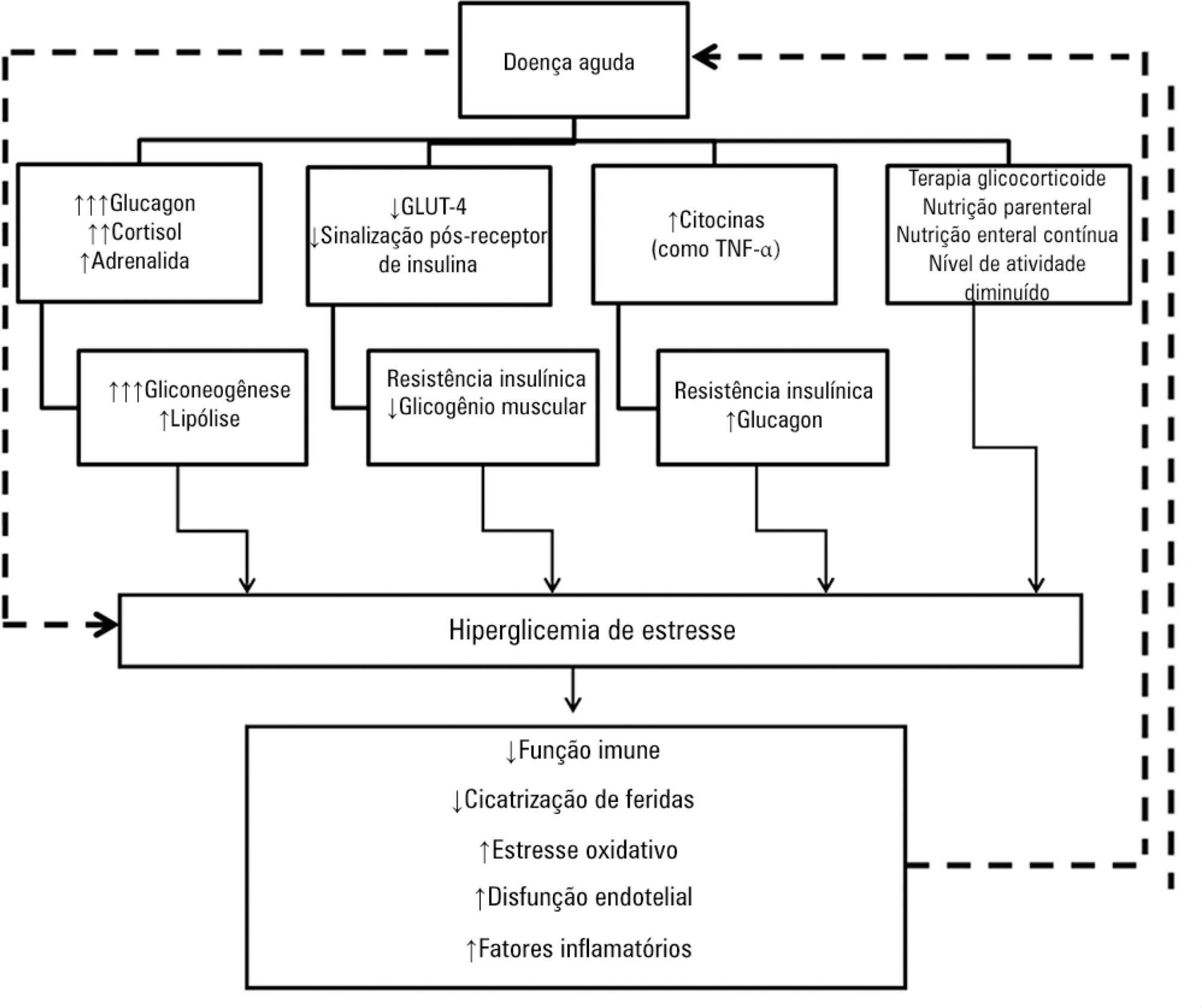
Hyperglycemia is a commonly encountered issue in critically ill patients in the intensive care setting. The presence of hyperglycemia is associated with increased morbidity and mortality, regardless of the reason for admission (e.g., acute myocardial infarction, status post-cardiovascular surgery, stroke, sepsis). However, the pathophysiology and, in particular, the treatment of hyperglycemia in the critically ill patient remain controversial. In clinical practice, several aspects must be taken into account in the management of these patients, including blood glucose targets, history of diabetes mellitus, the route of nutrition (enteral or parenteral), and available monitoring equipment, which substantially increases the workload of providers involved in the patients' care. This review describes the epidemiology, pathophysiology, management, and monitoring of hyperglycemia in the critically ill adult patient.
Abstract
Rev Bras Ter Intensiva. 2014;26(1):71-76
DOI 10.5935/0103-507X.20140011
Hyperglycemia is a commonly encountered issue in critically ill patients in the intensive care setting. The presence of hyperglycemia is associated with increased morbidity and mortality, regardless of the reason for admission (e.g., acute myocardial infarction, status post-cardiovascular surgery, stroke, sepsis). However, the pathophysiology and, in particular, the treatment of hyperglycemia in the critically ill patient remain controversial. In clinical practice, several aspects must be taken into account in the management of these patients, including blood glucose targets, history of diabetes mellitus, the route of nutrition (enteral or parenteral), and available monitoring equipment, which substantially increases the workload of providers involved in the patients' care. This review describes the epidemiology, pathophysiology, management, and monitoring of hyperglycemia in the critically ill adult patient.
Abstract
Rev Bras Ter Intensiva. 2008;20(2):197-204
DOI 10.1590/S0103-507X2008000200014
BACKGROUND AND OBJECTIVES: Acute coronary syndromes result from a disruption of a vulnerable coronary plaque complicated by intraluminal thrombus formation, embolisation, and variable degrees of coronary obstruction. Patients with total occlusion may present with acute ST Elevation Myocardial Infarction (STEMI). Partial vessel obstruction may result in Non-ST-Elevation Acute Myocardial Infarction (NSTEMI) or unstable angina (UA). Clinical symptoms and electrocardiographic changes are the main components of identification of ACS. The rapid and effective triage of such patients regarding presence or absence of ST-segment elevation is critical to dictate further therapeutic strategies. The objective of this chapter was to review current evidence and recommendations for the evaluation and early treatment of acute coronary syndromes. CONTENTS: We performed a clinical review using the electronic databases MedLine and LILACS from January 1990 to September 2007. CONCLUSIONS: Reperfusion of the infarct-related artery is the cornerstone of therapy for STEMI. Fibrinolysis and percutaneous coronary intervention are both well established as effective options. Management of UA/NSTEMI patients requires early risk stratification. High-risk patients should undergo an early invasive strategy that consists in performance of cardiac catheterization in the first 24 to 48 hours of presentation.
Abstract
Rev Bras Ter Intensiva. 2008;20(2):197-204
DOI 10.1590/S0103-507X2008000200014
BACKGROUND AND OBJECTIVES: Acute coronary syndromes result from a disruption of a vulnerable coronary plaque complicated by intraluminal thrombus formation, embolisation, and variable degrees of coronary obstruction. Patients with total occlusion may present with acute ST Elevation Myocardial Infarction (STEMI). Partial vessel obstruction may result in Non-ST-Elevation Acute Myocardial Infarction (NSTEMI) or unstable angina (UA). Clinical symptoms and electrocardiographic changes are the main components of identification of ACS. The rapid and effective triage of such patients regarding presence or absence of ST-segment elevation is critical to dictate further therapeutic strategies. The objective of this chapter was to review current evidence and recommendations for the evaluation and early treatment of acute coronary syndromes. CONTENTS: We performed a clinical review using the electronic databases MedLine and LILACS from January 1990 to September 2007. CONCLUSIONS: Reperfusion of the infarct-related artery is the cornerstone of therapy for STEMI. Fibrinolysis and percutaneous coronary intervention are both well established as effective options. Management of UA/NSTEMI patients requires early risk stratification. High-risk patients should undergo an early invasive strategy that consists in performance of cardiac catheterization in the first 24 to 48 hours of presentation.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (115) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)