Respiratory therapy/methods Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2019;31(3):289-295
DOI 10.5935/0103-507X.20190052
To evaluate the effects of ventilator hyperinflation on respiratory mechanics.
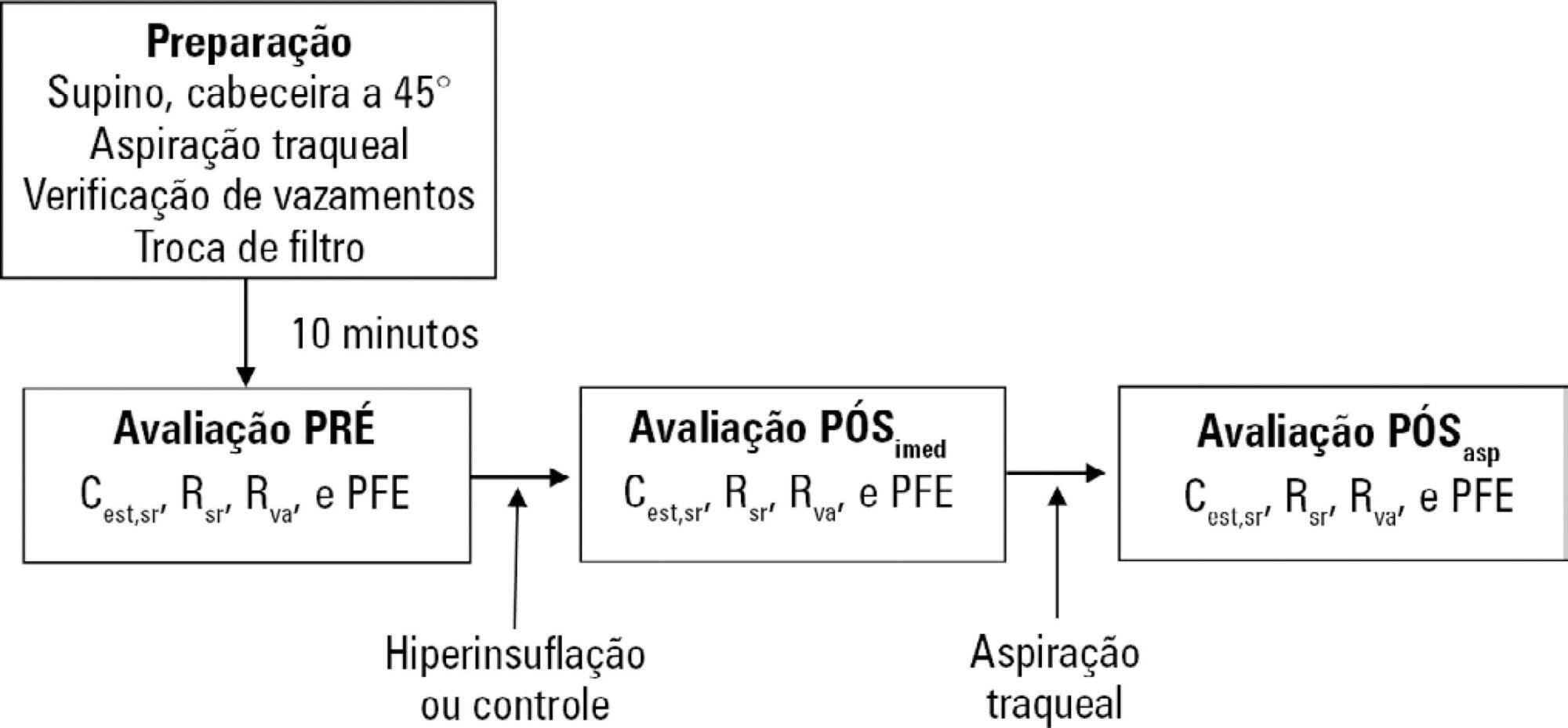
A randomized crossover clinical trial was conducted with 38 mechanically ventilated patients with pulmonary infection. The order of the hyperinflation and control (without changes in the parameters) conditions was randomized. Hyperinflation was performed for 5 minutes in pressure-controlled ventilation mode, with progressive increases of 5cmH2O until a maximum pressure of 35cmH2O was reached, maintaining positive end expiratory pressure. After 35cmH2O was reached, the inspiratory time and respiratory rate were adjusted so that the inspiratory and expiratory flows reached baseline levels. Measurements of static compliance, total resistance and airway resistance, and peak expiratory flow were evaluated before the technique, immediately after the technique and after aspiration. Two-way analysis of variance for repeated measures was used with Tukey's post hoc test, and p < 0.05 was considered significant.
Ventilator hyperinflation increased static compliance, which remained at the same level after aspiration (46.2 ± 14.8 versus 52.0 ± 14.9 versus 52.3 ± 16.0mL/cmH2O; p < 0.001). There was a transient increase in airway resistance (6.6 ± 3.6 versus 8.0 ± 5.5 versus 6.6 ± 3.5cmH2O/Ls-1; p < 0.001) and a transient reduction in peak expiratory flow (32.0 ± 16.0 versus 29.8 ± 14.8 versus 32.1 ± 15.3Lpm; p <0.05) immediately after the technique; these values returned to pretechnique levels after tracheal aspiration. There were no changes in the control condition, nor were hemodynamic alterations observed.
Ventilator hyperinflation promoted increased compliance associated with a transient increase in airway resistance and peak expiratory flow, with reduction after aspiration.
Abstract
Rev Bras Ter Intensiva. 2019;31(3):289-295
DOI 10.5935/0103-507X.20190052
To evaluate the effects of ventilator hyperinflation on respiratory mechanics.
A randomized crossover clinical trial was conducted with 38 mechanically ventilated patients with pulmonary infection. The order of the hyperinflation and control (without changes in the parameters) conditions was randomized. Hyperinflation was performed for 5 minutes in pressure-controlled ventilation mode, with progressive increases of 5cmH2O until a maximum pressure of 35cmH2O was reached, maintaining positive end expiratory pressure. After 35cmH2O was reached, the inspiratory time and respiratory rate were adjusted so that the inspiratory and expiratory flows reached baseline levels. Measurements of static compliance, total resistance and airway resistance, and peak expiratory flow were evaluated before the technique, immediately after the technique and after aspiration. Two-way analysis of variance for repeated measures was used with Tukey's post hoc test, and p < 0.05 was considered significant.
Ventilator hyperinflation increased static compliance, which remained at the same level after aspiration (46.2 ± 14.8 versus 52.0 ± 14.9 versus 52.3 ± 16.0mL/cmH2O; p < 0.001). There was a transient increase in airway resistance (6.6 ± 3.6 versus 8.0 ± 5.5 versus 6.6 ± 3.5cmH2O/Ls-1; p < 0.001) and a transient reduction in peak expiratory flow (32.0 ± 16.0 versus 29.8 ± 14.8 versus 32.1 ± 15.3Lpm; p <0.05) immediately after the technique; these values returned to pretechnique levels after tracheal aspiration. There were no changes in the control condition, nor were hemodynamic alterations observed.
Ventilator hyperinflation promoted increased compliance associated with a transient increase in airway resistance and peak expiratory flow, with reduction after aspiration.
Abstract
Rev Bras Ter Intensiva. 2011;23(2):190-198
DOI 10.1590/S0103-507X2011000200012
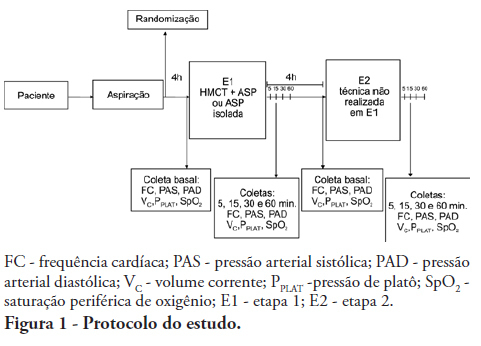
OBJECTIVES: To evaluate the effects of the manual hyperinflation with thoracic compression (MHTC) maneuver on the clearance of secretions, pulmonary mechanics, hemodynamics and oxygenation in mechanically ventilated patients. METHODS: This was a controlled, crossover study that included twenty patients who were under invasive ventilation for more than 48 hours. Four hours after the last airway suctioning procedure, the patients underwent the study interventions, Suction alone or MHTC plus Suction, in sequence at four hour intervals. The sequence order for the procedures was established by randomization. Data were collected before, during and 5, 15, 30 and 60 minutes after each intervention. The suctioned secretions were collected and weighed. RESULTS: No significant differences between the procedures were found regarding tidal volume, plateau pressure and pulmonary compliance (p>0.05). The hemodynamic variables showed increased pressures and heart rate during the procedures and returned to baseline values five minutes after the end of the procedure (p≤0.001). No significant hemodynamic differences were seen between the interventions (p>0.05). For the duration of the study, oxygen saturation was 99% with only two exceptions during the MHTC + Suction procedure, where saturation was 98% (p<0.05). No significant differences were observed between the techniques regarding the weight of the suctioned secretion. CONCLUSION: The results suggest that MHTC, as performed in this study, adds no benefit with respect to oxygenation optimization, pulmonary mechanics and clearance of secretions. However, the MHTC maneuver did not result in hemodynamic changes when compared to the suctioning procedure alone.
Abstract
Rev Bras Ter Intensiva. 2011;23(2):190-198
DOI 10.1590/S0103-507X2011000200012
OBJECTIVES: To evaluate the effects of the manual hyperinflation with thoracic compression (MHTC) maneuver on the clearance of secretions, pulmonary mechanics, hemodynamics and oxygenation in mechanically ventilated patients. METHODS: This was a controlled, crossover study that included twenty patients who were under invasive ventilation for more than 48 hours. Four hours after the last airway suctioning procedure, the patients underwent the study interventions, Suction alone or MHTC plus Suction, in sequence at four hour intervals. The sequence order for the procedures was established by randomization. Data were collected before, during and 5, 15, 30 and 60 minutes after each intervention. The suctioned secretions were collected and weighed. RESULTS: No significant differences between the procedures were found regarding tidal volume, plateau pressure and pulmonary compliance (p>0.05). The hemodynamic variables showed increased pressures and heart rate during the procedures and returned to baseline values five minutes after the end of the procedure (p≤0.001). No significant hemodynamic differences were seen between the interventions (p>0.05). For the duration of the study, oxygen saturation was 99% with only two exceptions during the MHTC + Suction procedure, where saturation was 98% (p<0.05). No significant differences were observed between the techniques regarding the weight of the suctioned secretion. CONCLUSION: The results suggest that MHTC, as performed in this study, adds no benefit with respect to oxygenation optimization, pulmonary mechanics and clearance of secretions. However, the MHTC maneuver did not result in hemodynamic changes when compared to the suctioning procedure alone.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (116) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)