-
Special Article
Brazilian Guidelines for Early Mobilization in Intensive Care Unit
- Esperidião Elias Aquim
 ,
, - Wanderley Marques Bernardo,
- Renata Ferreira Buzzini,
- Nara Selaimen Gaertner de Azeredo,
- Laura Severo da Cunha, [ … ],
- Cleber Verona
Abstract
Special ArticleBrazilian Guidelines for Early Mobilization in Intensive Care Unit
Rev Bras Ter Intensiva. 2019;31(4):434-443
DOI 10.5935/0103-507X.20190084
- Esperidião Elias Aquim ,
- Wanderley Marques Bernardo,
- Renata Ferreira Buzzini,
- Nara Selaimen Gaertner de Azeredo,
- Laura Severo da Cunha,
- Marta Cristina Pauleti Damasceno,
- Rafael Alexandre de Oliveira Deucher,
- Antonio Carlos Magalhães Duarte,
- Juliana Thiemy Librelato,
- Cesar Augusto Melo-Silva,
- Sergio Nogueira Nemer,
- Sabrina Donatti Ferreira da Silva,
- Cleber Verona
Views0ABSTRACT
Immobility can cause several complications, including skeletal muscle atrophy and weakness, that influence the recovery of critically ill patients. This effect can be mitigated by early mobilization. Six key questions guided this research: Is early mobilization safe? Which patients are candidates for early mobilization? What are the contraindications? What is the appropriate dose, and how should it be defined? What results are obtained? What are the prognostic indicators for the use of early mobilization? The objective of this guideline was to produce a document that would provide evidence-based recommendations and suggestions regarding the early mobilization of critically ill adult patients, with the aim of improving understanding of the topic and making a positive impact on patient care. This guideline was based on a systematic review of articles conducted using the PICO search strategy, as recommended by the Guidelines Project of the Associação Médica Brasileira. Randomized clinical trials, prognostic cohort studies, and systematic reviews with or without meta-analysis were selected, and the evidence was classified according to the Oxford Center for Evidence-based Medicine Levels of Evidence. For all the questions addressed, enough evidence was found to support safe and well-defined early mobilization, with prognostic indicators that support and recommend the technique. Early mobilization is associated with better functional outcomes and should be performed whenever indicated. Early mobilization is safe and should be the goal of the entire multidisciplinary team.
Keywords:Critical careEarly ambulationExerciseIntensive care unitsMobilityPatient safetyRespiration, artificialSee moreViews0

Abstract
Special ArticleBrazilian Guidelines for Early Mobilization in Intensive Care Unit
Rev Bras Ter Intensiva. 2019;31(4):434-443
DOI 10.5935/0103-507X.20190084
- Esperidião Elias Aquim ,
- Wanderley Marques Bernardo,
- Renata Ferreira Buzzini,
- Nara Selaimen Gaertner de Azeredo,
- Laura Severo da Cunha,
- Marta Cristina Pauleti Damasceno,
- Rafael Alexandre de Oliveira Deucher,
- Antonio Carlos Magalhães Duarte,
- Juliana Thiemy Librelato,
- Cesar Augusto Melo-Silva,
- Sergio Nogueira Nemer,
- Sabrina Donatti Ferreira da Silva,
- Cleber Verona
Views0ABSTRACT
Immobility can cause several complications, including skeletal muscle atrophy and weakness, that influence the recovery of critically ill patients. This effect can be mitigated by early mobilization. Six key questions guided this research: Is early mobilization safe? Which patients are candidates for early mobilization? What are the contraindications? What is the appropriate dose, and how should it be defined? What results are obtained? What are the prognostic indicators for the use of early mobilization? The objective of this guideline was to produce a document that would provide evidence-based recommendations and suggestions regarding the early mobilization of critically ill adult patients, with the aim of improving understanding of the topic and making a positive impact on patient care. This guideline was based on a systematic review of articles conducted using the PICO search strategy, as recommended by the Guidelines Project of the Associação Médica Brasileira. Randomized clinical trials, prognostic cohort studies, and systematic reviews with or without meta-analysis were selected, and the evidence was classified according to the Oxford Center for Evidence-based Medicine Levels of Evidence. For all the questions addressed, enough evidence was found to support safe and well-defined early mobilization, with prognostic indicators that support and recommend the technique. Early mobilization is associated with better functional outcomes and should be performed whenever indicated. Early mobilization is safe and should be the goal of the entire multidisciplinary team.
Keywords:Critical careEarly ambulationExerciseIntensive care unitsMobilityPatient safetyRespiration, artificialSee more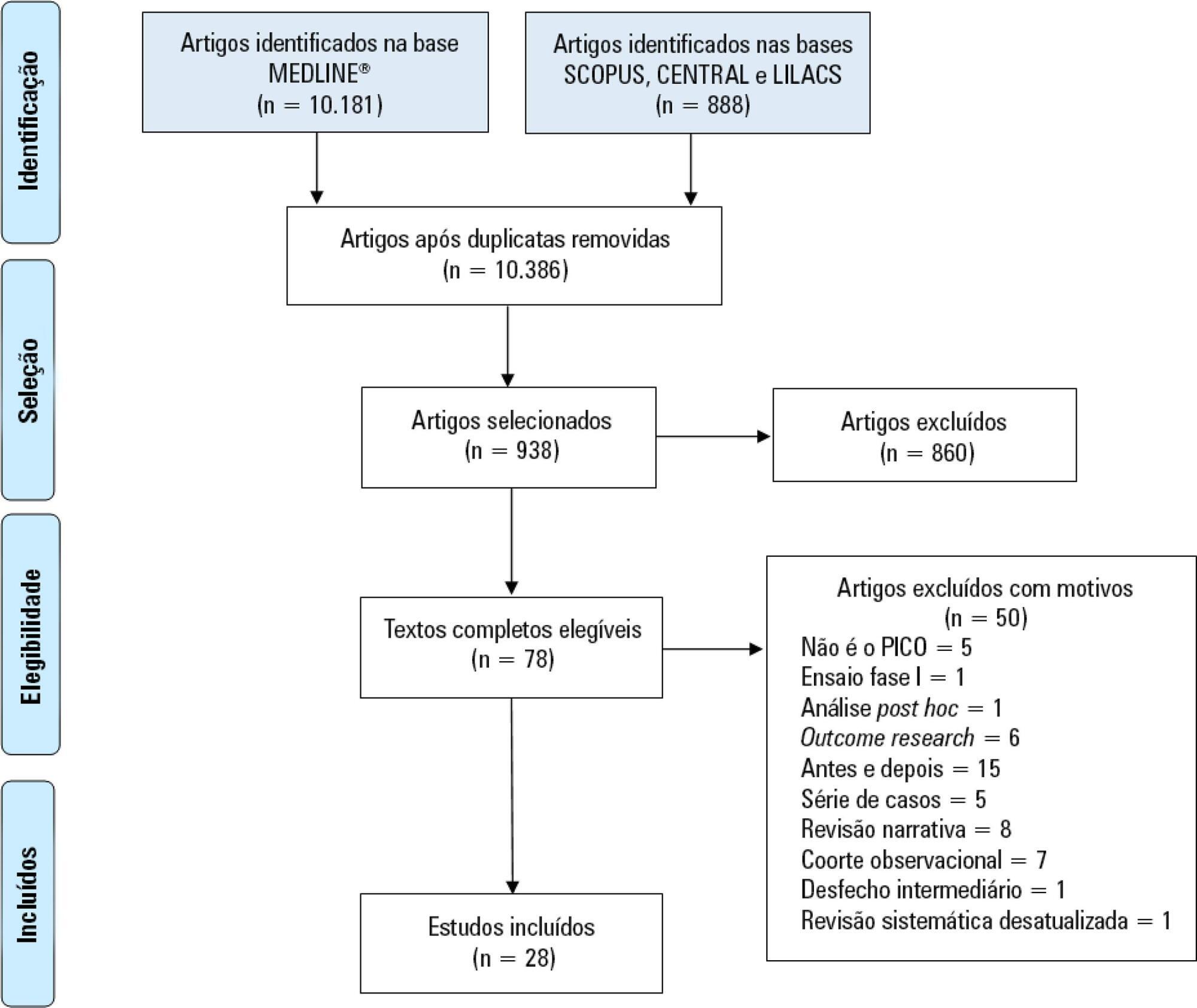
- Esperidião Elias Aquim
-
Commentary
What every intensivist should know about Big Data and targeted machine learning in the intensive care unit
Rev Bras Ter Intensiva. 2019;31(4):444-446
Abstract
CommentaryWhat every intensivist should know about Big Data and targeted machine learning in the intensive care unit
Rev Bras Ter Intensiva. 2019;31(4):444-446
DOI 10.5935/0103-507X.20190069
Views1The increasing importance of Big Data in healthcareThe conjunction of increasingly available access to big medical data and of substantial progress in machine learning (ML) and artificial intelligence (AI) has created new, unforeseen opportunities for data science in healthcare. Big Data is described as having at least three distinct characteristics, volume, velocity, and variety, but […]See moreViews1Abstract
CommentaryWhat every intensivist should know about Big Data and targeted machine learning in the intensive care unit
Rev Bras Ter Intensiva. 2019;31(4):444-446
DOI 10.5935/0103-507X.20190069
Views1The increasing importance of Big Data in healthcareThe conjunction of increasingly available access to big medical data and of substantial progress in machine learning (ML) and artificial intelligence (AI) has created new, unforeseen opportunities for data science in healthcare. Big Data is described as having at least three distinct characteristics, volume, velocity, and variety, but […]See more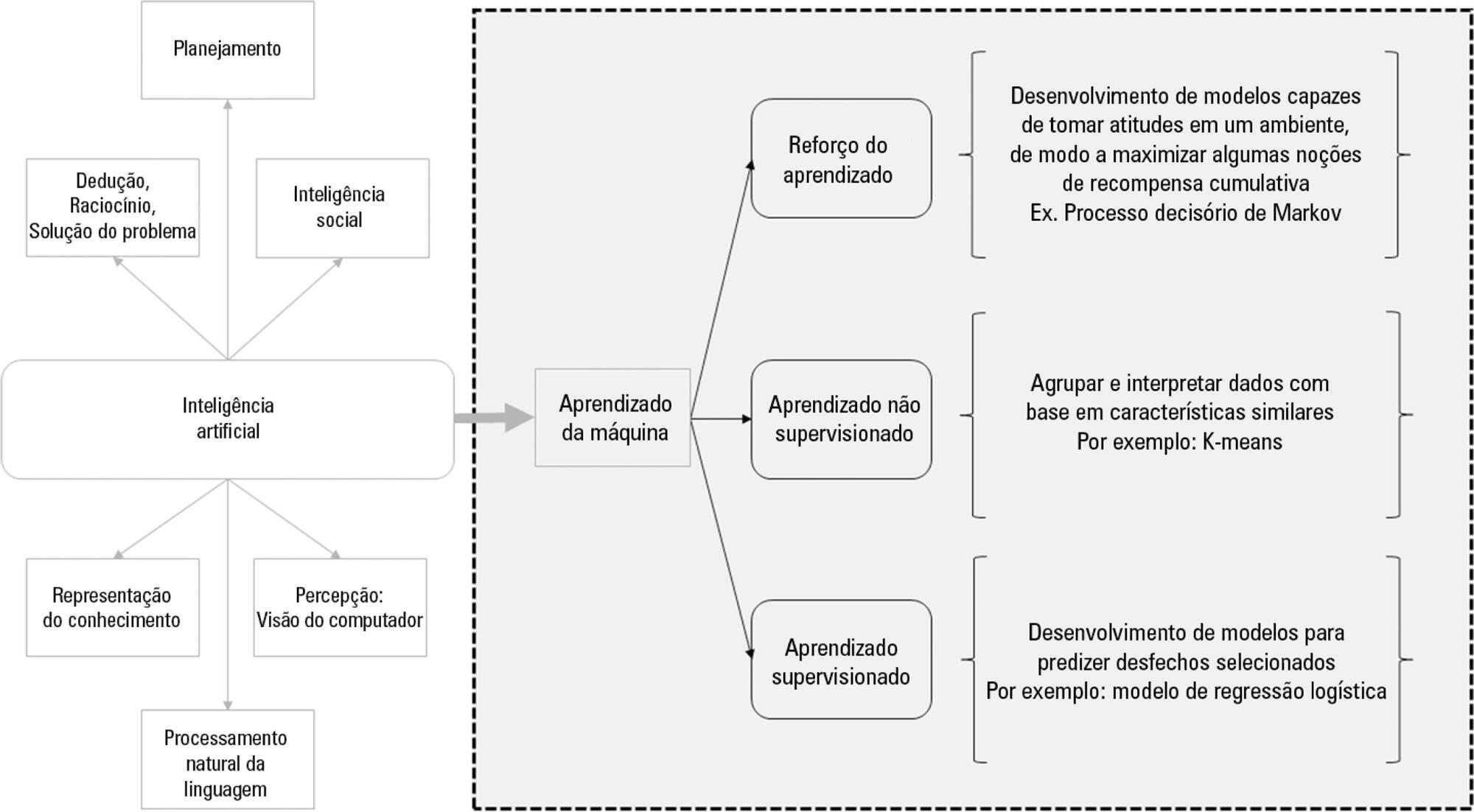
-
Original Articles
Pain management protocol implementation and opioid consumption in critical care: an interrupted time series analysis
- Bruno Adler Maccagnan Pinheiro Besen ,
- Antonio Paulo Nassar Júnior ,
- Fábio Holanda Lacerda,
- Carla Marchini Dias da Silva,
- Vanessa Tota de Souza, [ … ],
- Lucas Fernandes de Oliveira
Abstract
Original ArticlesPain management protocol implementation and opioid consumption in critical care: an interrupted time series analysis
Rev Bras Ter Intensiva. 2019;31(4):447-455
DOI 10.5935/0103-507X.20190085
- Bruno Adler Maccagnan Pinheiro Besen ,
- Antonio Paulo Nassar Júnior ,
- Fábio Holanda Lacerda,
- Carla Marchini Dias da Silva,
- Vanessa Tota de Souza,
- Eliana Vieira do Nascimento Martins,
- Ana Tarina Alvarez Lopes,
- Carlos Eduardo Brandão,
- Lucas Fernandes de Oliveira
Views1See moreABSTRACT
Objective:
To evaluate the impact of an opioid-sparing pain management protocol on overall opioid consumption and clinical outcomes.
Methods:
This was a single-center, quasi-experimental, retrospective, before and after cohort study. We used an interrupted time series to analyze changes in the levels and trends of the utilization of different analgesics. We used bivariate comparisons in the before and after cohorts as well as logistic regression and quantile regression for adjusted estimates.
Results:
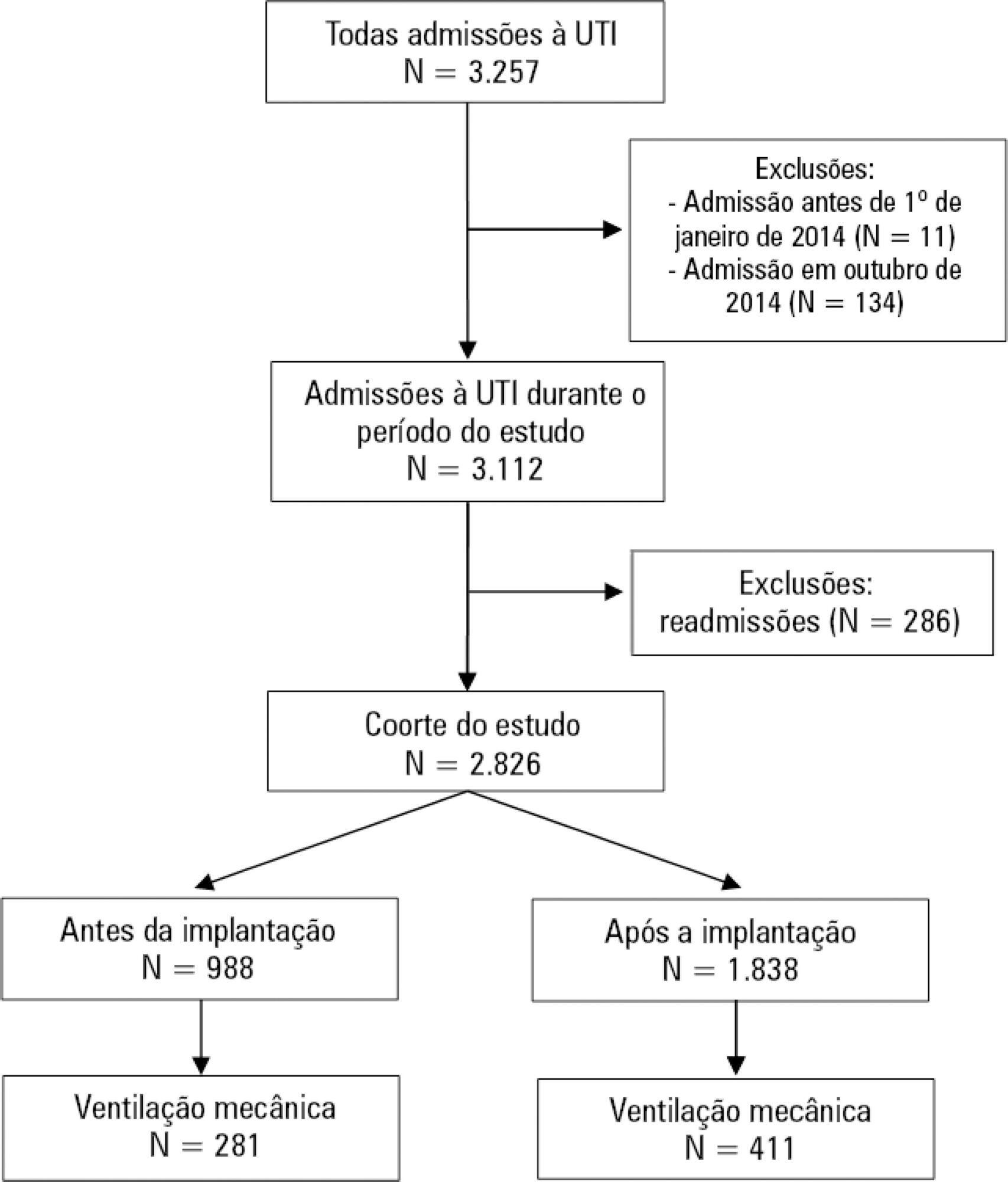
We included 988 patients in the preintervention period and 1,838 in the postintervention period. Fentanyl consumption was slightly increasing before the intervention (β = 16; 95%CI 7 – 25; p = 0.002) but substantially decreased in level with the intervention (β = – 128; 95%CI -195 – -62; p = 0.001) and then progressively decreased (β = – 24; 95%CI -35 – -13; p < 0.001). There was an increasing trend in the utilization of dipyrone. The mechanical ventilation duration was significantly lower (median difference: - 1 day; 95%CI -1 - 0; p < 0.001), especially for patients who were mechanically ventilated for a longer time (50th percentile difference: -0.78; 95%CI -1.51 – -0.05; p = 0.036; 75th percentile difference: -2.23; 95%CI -3.47 – -0.98; p < 0.001).
Conclusion:
A pain management protocol could reduce the intensive care unit consumption of fentanyl. This strategy was associated with a shorter mechanical ventilation duration.
Views1Abstract
Original ArticlesPain management protocol implementation and opioid consumption in critical care: an interrupted time series analysis
Rev Bras Ter Intensiva. 2019;31(4):447-455
DOI 10.5935/0103-507X.20190085
- Bruno Adler Maccagnan Pinheiro Besen ,
- Antonio Paulo Nassar Júnior ,
- Fábio Holanda Lacerda,
- Carla Marchini Dias da Silva,
- Vanessa Tota de Souza,
- Eliana Vieira do Nascimento Martins,
- Ana Tarina Alvarez Lopes,
- Carlos Eduardo Brandão,
- Lucas Fernandes de Oliveira
Views1See moreABSTRACT
Objective:
To evaluate the impact of an opioid-sparing pain management protocol on overall opioid consumption and clinical outcomes.
Methods:
This was a single-center, quasi-experimental, retrospective, before and after cohort study. We used an interrupted time series to analyze changes in the levels and trends of the utilization of different analgesics. We used bivariate comparisons in the before and after cohorts as well as logistic regression and quantile regression for adjusted estimates.
Results:
We included 988 patients in the preintervention period and 1,838 in the postintervention period. Fentanyl consumption was slightly increasing before the intervention (β = 16; 95%CI 7 – 25; p = 0.002) but substantially decreased in level with the intervention (β = – 128; 95%CI -195 – -62; p = 0.001) and then progressively decreased (β = – 24; 95%CI -35 – -13; p < 0.001). There was an increasing trend in the utilization of dipyrone. The mechanical ventilation duration was significantly lower (median difference: - 1 day; 95%CI -1 - 0; p < 0.001), especially for patients who were mechanically ventilated for a longer time (50th percentile difference: -0.78; 95%CI -1.51 – -0.05; p = 0.036; 75th percentile difference: -2.23; 95%CI -3.47 – -0.98; p < 0.001).
Conclusion:
A pain management protocol could reduce the intensive care unit consumption of fentanyl. This strategy was associated with a shorter mechanical ventilation duration.
- Bruno Adler Maccagnan Pinheiro Besen
-
Original Articles
Rehabilitation through virtual reality: physical activity of patients admitted to the intensive care unit
Rev Bras Ter Intensiva. 2019;31(4):456-463
Abstract
Original ArticlesRehabilitation through virtual reality: physical activity of patients admitted to the intensive care unit
Rev Bras Ter Intensiva. 2019;31(4):456-463
DOI 10.5935/0103-507X.20190078
Views1See moreABSTRACT
Objective:
To evaluate the level of activity that Nintendo WiiTM can elicit in intensive care unit patients and its associated safety and patient satisfaction.
Methods:
Experimental, single-center study performed at a tertiary care hospital. Patients ≥ 18 years old who were admitted to the intensive care unit, participated in videogames as part of their physical therapy sessions and did not have mobility restrictions were included. Th exclusion criteria were the inability to comprehend instructions and the inability to follow simple commands. We included n = 60 patients and performed 100 sessions. We used the Nintendo WiiTM gaming system in the sessions. An accelerometer measured the level of physical activity of patients while they played videogames. We evaluated the level of activity, the modified Borg scale scores, the adverse events and the responses to a questionnaire on satisfaction with the activity.
Results:
One hundred physical therapy sessions were analyzed. When the patients played the videogame, they reached a light level of activity for 59% of the session duration and a moderate level of activity for 38% of the session duration. No adverse events occurred. A total of 86% of the patients reported that they would like to play the videogame in their future physical therapy sessions.
Conclusion:
Virtual rehabilitation elicited light to moderate levels of activity in intensive care unit patients. This therapy is a safe tool and is likely to be chosen by the patient during physical therapy.
Views1Abstract
Original ArticlesRehabilitation through virtual reality: physical activity of patients admitted to the intensive care unit
Rev Bras Ter Intensiva. 2019;31(4):456-463
DOI 10.5935/0103-507X.20190078
Views1See moreABSTRACT
Objective:
To evaluate the level of activity that Nintendo WiiTM can elicit in intensive care unit patients and its associated safety and patient satisfaction.
Methods:
Experimental, single-center study performed at a tertiary care hospital. Patients ≥ 18 years old who were admitted to the intensive care unit, participated in videogames as part of their physical therapy sessions and did not have mobility restrictions were included. Th exclusion criteria were the inability to comprehend instructions and the inability to follow simple commands. We included n = 60 patients and performed 100 sessions. We used the Nintendo WiiTM gaming system in the sessions. An accelerometer measured the level of physical activity of patients while they played videogames. We evaluated the level of activity, the modified Borg scale scores, the adverse events and the responses to a questionnaire on satisfaction with the activity.
Results:
One hundred physical therapy sessions were analyzed. When the patients played the videogame, they reached a light level of activity for 59% of the session duration and a moderate level of activity for 38% of the session duration. No adverse events occurred. A total of 86% of the patients reported that they would like to play the videogame in their future physical therapy sessions.
Conclusion:
Virtual rehabilitation elicited light to moderate levels of activity in intensive care unit patients. This therapy is a safe tool and is likely to be chosen by the patient during physical therapy.

-
Original Articles
Reliability of skeletal muscle ultrasound in critically ill trauma patients
- Luciana Vieira,
- Lara Patrícia Bastos Rocha ,
- Sunita Mathur,
- Larissa Santana,
- Priscilla Flávia de Melo, [ … ],
- Gerson Cipriano Jr.
Abstract
Original ArticlesReliability of skeletal muscle ultrasound in critically ill trauma patients
Rev Bras Ter Intensiva. 2019;31(4):464-473
DOI 10.5935/0103-507X.20190072
- Luciana Vieira,
- Lara Patrícia Bastos Rocha ,
- Sunita Mathur,
- Larissa Santana,
- Priscilla Flávia de Melo,
- Vinicius Zacarias Maldaner da Silva,
- João Luiz Quaglioti Durigan,
- Gerson Cipriano Jr.
Views0ABSTRACT
Objective:
To evaluate the safety and feasibility of the ultrasound assessment of quadriceps in the emergency setting. To assess the intra- and interrater reliability for the acquisition and analysis of ultrasound images of muscle thickness and echogenicity in critically ill trauma patients between health professionals with different levels of expertise.
Methods:
Diagnostic accuracy study. Two examiners (expert and novice) acquired ultrasound images from ten patients; an experienced, blinded analyst quantified the images. In a separate group of ten patients, two analysts (expert and novice) quantified quadriceps muscle thickness and echogenicity (square or trace method) from images acquired by one examiner.
Results:
Excellent reliability was found for image acquisition and analysis (intraclass correlation coefficients > 0.987; p < 0.001). The standard error of the measurement values ranged from 0.01 - 0.06cm for muscle thickness and from 0.75 - 2.04 arbitrary units for muscle echogenicity. The coefficients of variation were < 6% for thickness and echogenicity. The echogenicity values were higher when using the square technique than when using the tracing technique (p = 0.003).
Conclusion:
Ultrasound is safe, feasible, and reliable for muscle assessment in critically ill trauma patients, regardless of the assessor’s level of expertise.
Keywords:Diagnostic techniques and proceduresEmergency departmentMuscular atrophy/diagnostic imagingTrauma/diagnostic imaginguadriceps muscle/diagnostic imagingUltrasonographySee moreViews0Abstract
Original ArticlesReliability of skeletal muscle ultrasound in critically ill trauma patients
Rev Bras Ter Intensiva. 2019;31(4):464-473
DOI 10.5935/0103-507X.20190072
- Luciana Vieira,
- Lara Patrícia Bastos Rocha ,
- Sunita Mathur,
- Larissa Santana,
- Priscilla Flávia de Melo,
- Vinicius Zacarias Maldaner da Silva,
- João Luiz Quaglioti Durigan,
- Gerson Cipriano Jr.
Views0ABSTRACT
Objective:
To evaluate the safety and feasibility of the ultrasound assessment of quadriceps in the emergency setting. To assess the intra- and interrater reliability for the acquisition and analysis of ultrasound images of muscle thickness and echogenicity in critically ill trauma patients between health professionals with different levels of expertise.
Methods:
Diagnostic accuracy study. Two examiners (expert and novice) acquired ultrasound images from ten patients; an experienced, blinded analyst quantified the images. In a separate group of ten patients, two analysts (expert and novice) quantified quadriceps muscle thickness and echogenicity (square or trace method) from images acquired by one examiner.
Results:
Excellent reliability was found for image acquisition and analysis (intraclass correlation coefficients > 0.987; p < 0.001). The standard error of the measurement values ranged from 0.01 - 0.06cm for muscle thickness and from 0.75 - 2.04 arbitrary units for muscle echogenicity. The coefficients of variation were < 6% for thickness and echogenicity. The echogenicity values were higher when using the square technique than when using the tracing technique (p = 0.003).
Conclusion:
Ultrasound is safe, feasible, and reliable for muscle assessment in critically ill trauma patients, regardless of the assessor’s level of expertise.
Keywords:Diagnostic techniques and proceduresEmergency departmentMuscular atrophy/diagnostic imagingTrauma/diagnostic imaginguadriceps muscle/diagnostic imagingUltrasonographySee more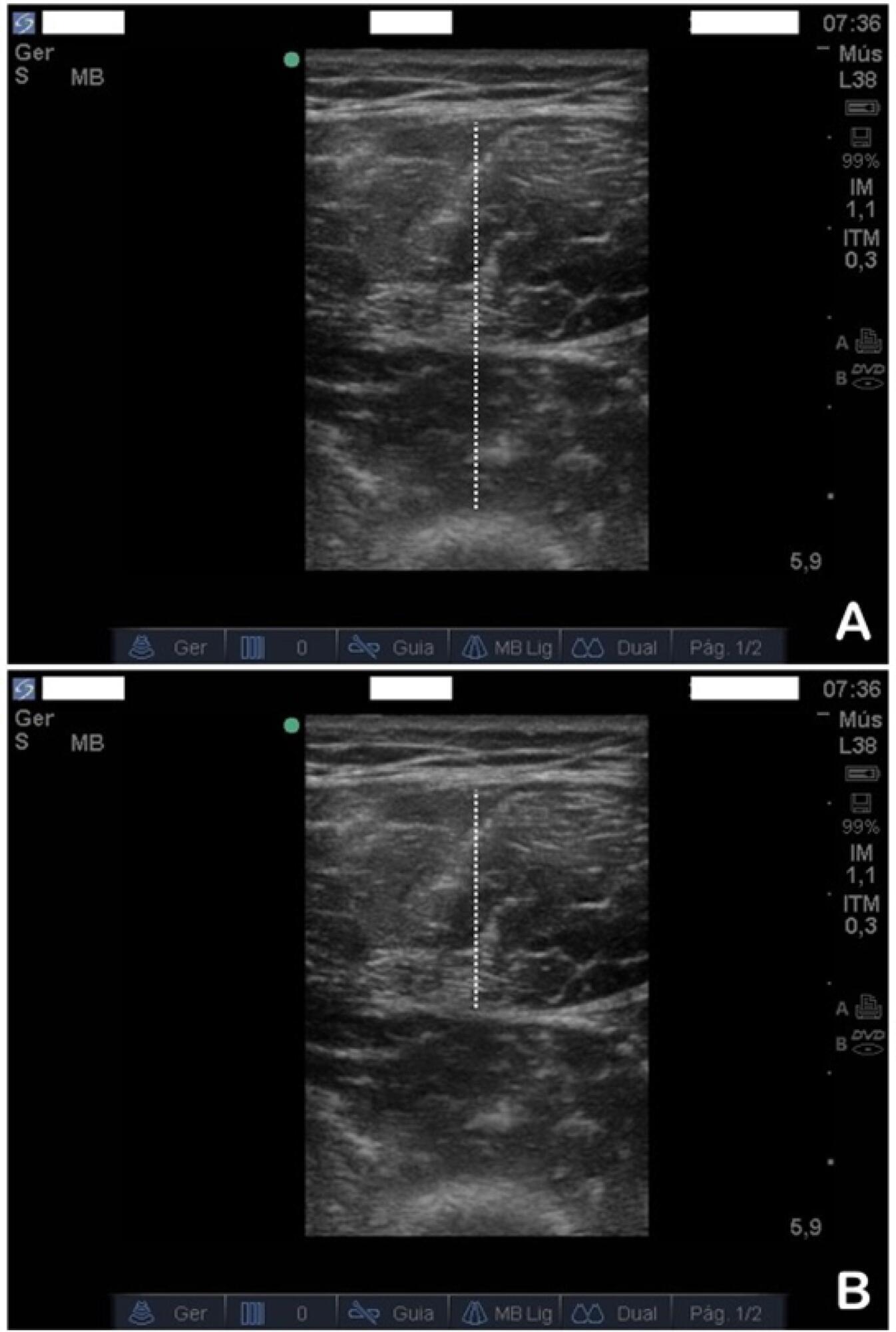
-
Original Articles
Cardiac output measured by transthoracic echocardiography and Swan-Ganz catheter. A comparative study in mechanically ventilated patients with high positive end-expiratory pressure
- José Gorrasi ,
- Arturo Pazos,
- Lucia Florio,
- Carlos Américo,
- Natalia Lluberas, [ … ],
- Ricardo Lluberas
Abstract
Original ArticlesCardiac output measured by transthoracic echocardiography and Swan-Ganz catheter. A comparative study in mechanically ventilated patients with high positive end-expiratory pressure
Rev Bras Ter Intensiva. 2019;31(4):474-482
DOI 10.5935/0103-507X.20190073
- José Gorrasi ,
- Arturo Pazos,
- Lucia Florio,
- Carlos Américo,
- Natalia Lluberas,
- Gabriel Parma,
- Ricardo Lluberas
Views0ABSTRACT
Objective:
To compare cardiac output measurements by transthoracic echocardiography and a pulmonary artery catheter in mechanically ventilated patients with high positive end-expiratory pressure. To evaluate the effect of tricuspid regurgitation.
Methods:
Sixteen mechanically ventilated patients were studied. Cardiac output was measured by pulmonary artery catheterization and transthoracic echocardiography. Measurements were performed at different levels of positive end-expiratory pressure (10cmH2O, 15cmH2O, and 20cmH2O). The effect of tricuspid regurgitation on cardiac output measurement was evaluated. The intraclass correlation coefficient was studied; the mean error and limits of agreement were studied with the Bland-Altman plot. The error rate was calculated.
Results:
Forty-four pairs of cardiac output measurements were obtained. An intraclass correlation coefficient of 0.908 was found (p < 0.001). The mean error was 0.44L/min for cardiac output values between 5 and 13L/min. The limits of agreement were 3.25L/min and -2.37L/min. With tricuspid insufficiency, the intraclass correlation coefficient was 0.791, and without tricuspid insufficiency, 0.935. Tricuspid insufficiency increased the error rate from 32% to 52%.
Conclusions:
In patients with high positive end-expiratory pressure, cardiac output measurement by transthoracic echocardiography is comparable to that with a pulmonary artery catheter. Tricuspid regurgitation influences the intraclass correlation coefficient. In patients with high positive end-expiratory pressure, the use of transthoracic echocardiography to measure cardiac output is comparable to invasive measures.
Keywords:Cardiac outputEchocardiographyHemodynamic monitoringPositive end-expiratory pressurePulmonary Artery CatheterRespiration, artificialSee moreViews0Abstract
Original ArticlesCardiac output measured by transthoracic echocardiography and Swan-Ganz catheter. A comparative study in mechanically ventilated patients with high positive end-expiratory pressure
Rev Bras Ter Intensiva. 2019;31(4):474-482
DOI 10.5935/0103-507X.20190073
- José Gorrasi ,
- Arturo Pazos,
- Lucia Florio,
- Carlos Américo,
- Natalia Lluberas,
- Gabriel Parma,
- Ricardo Lluberas
Views0ABSTRACT
Objective:
To compare cardiac output measurements by transthoracic echocardiography and a pulmonary artery catheter in mechanically ventilated patients with high positive end-expiratory pressure. To evaluate the effect of tricuspid regurgitation.
Methods:
Sixteen mechanically ventilated patients were studied. Cardiac output was measured by pulmonary artery catheterization and transthoracic echocardiography. Measurements were performed at different levels of positive end-expiratory pressure (10cmH2O, 15cmH2O, and 20cmH2O). The effect of tricuspid regurgitation on cardiac output measurement was evaluated. The intraclass correlation coefficient was studied; the mean error and limits of agreement were studied with the Bland-Altman plot. The error rate was calculated.
Results:
Forty-four pairs of cardiac output measurements were obtained. An intraclass correlation coefficient of 0.908 was found (p < 0.001). The mean error was 0.44L/min for cardiac output values between 5 and 13L/min. The limits of agreement were 3.25L/min and -2.37L/min. With tricuspid insufficiency, the intraclass correlation coefficient was 0.791, and without tricuspid insufficiency, 0.935. Tricuspid insufficiency increased the error rate from 32% to 52%.
Conclusions:
In patients with high positive end-expiratory pressure, cardiac output measurement by transthoracic echocardiography is comparable to that with a pulmonary artery catheter. Tricuspid regurgitation influences the intraclass correlation coefficient. In patients with high positive end-expiratory pressure, the use of transthoracic echocardiography to measure cardiac output is comparable to invasive measures.
Keywords:Cardiac outputEchocardiographyHemodynamic monitoringPositive end-expiratory pressurePulmonary Artery CatheterRespiration, artificialSee more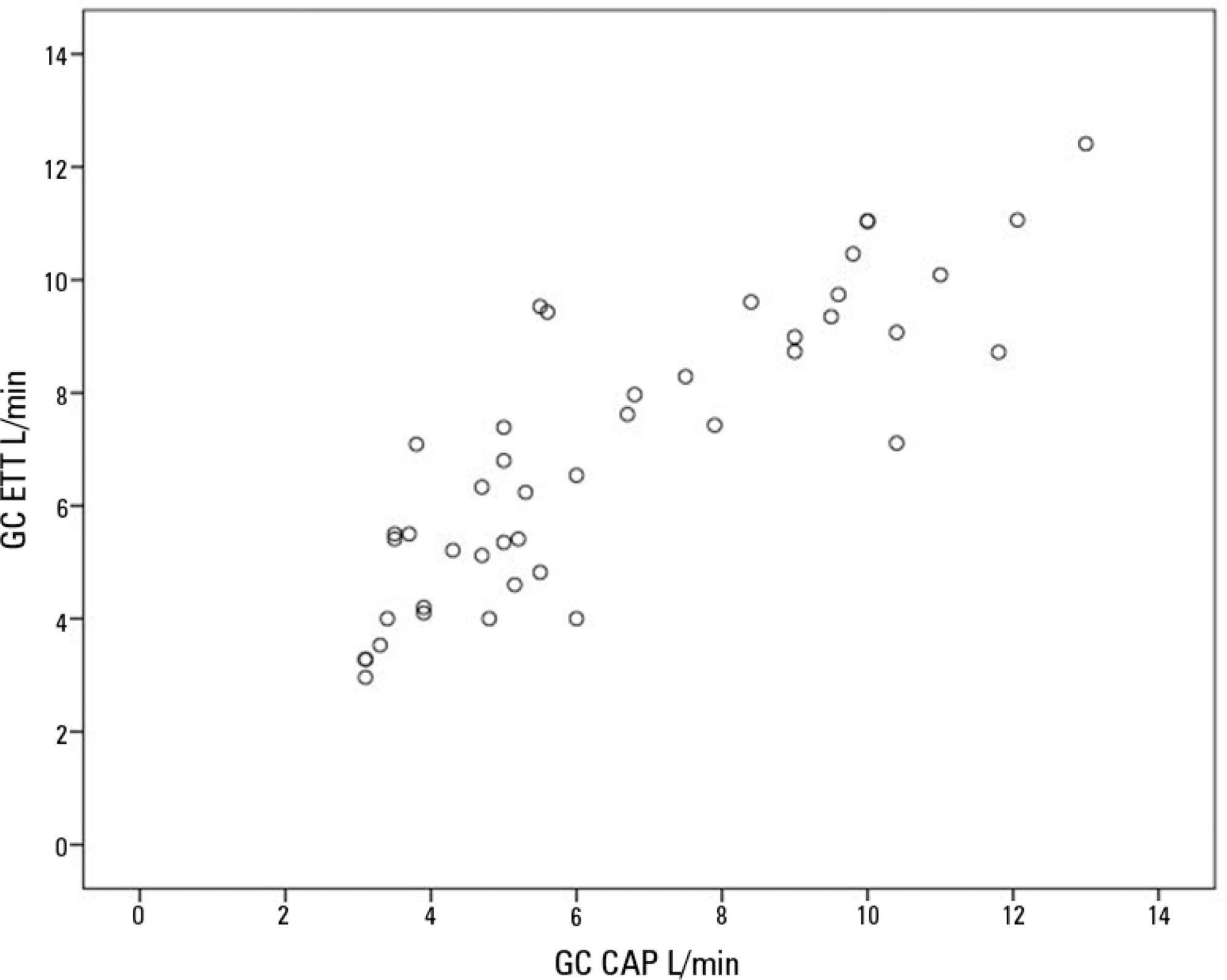
- José Gorrasi
-
Original Articles
Effect of PEEP on inspiratory resistance components in patients with acute respiratory distress syndrome ventilated at low tidal volume
- Sebastian Fredes ,
- Emilio Steinberg ,
- Norberto Tiribelli,
- Analia Santa Maria,
- Mariana Berté, [ … ],
- Santiago Ilutovich
Abstract
Original ArticlesEffect of PEEP on inspiratory resistance components in patients with acute respiratory distress syndrome ventilated at low tidal volume
Rev Bras Ter Intensiva. 2019;31(4):483-489
DOI 10.5935/0103-507X.20190071
- Sebastian Fredes ,
- Emilio Steinberg ,
- Norberto Tiribelli,
- Analia Santa Maria,
- Mariana Berté,
- Nicolás Segura,
- Diego Noval,
- Santiago Ilutovich
Views0ABSTRACT
Objective:
To describe the behavior of inspiratory resistance components when positive end-expiratory pressure (PEEP) increases in patients with acute respiratory distress syndrome under a protective ventilation strategy.
Methods:
In volume-controlled mode, at 6mL/kg and constant flow, end-inspiratory occlusions were performed at 0, 5 10, 15 and 20cmH2O PEEP. Peak, initial and plateau pressure values were assessed, calculating the maximum, minimum and differential resistances. The results were compared by repeated measures analysis of variance (ANOVA) with post hoc Bonferroni correction, considering p < 0.05 significant.
Results:
The highest maximum resistance was observed at the lowest PEEP levels. The values for 10 and 15cmH2O PEEP significantly differed from those for 5 and 0cmH2O PEEP, whereas that for 20cmH2O PEEP only significantly differed from that for 0cmH2O PEEP (p < 0.05). The minimum resistance behaved similarly to the maximum resistance; the values for PEEP levels from 10cmH2O to 20cmH2O significantly differed from those for 0 and 5cmH2O PEEP (p < 0.05). Differential resistance showed the opposite variation to the maximum and minimum resistances. The only PEEP level that showed significant differences from 0 and 5cmH2O PEEP was 20cmH2O PEEP. Significant differences were also found between 15 and 5cmH2O PEEP (p < 0.05).
Conclusions:
During protective ventilation in patients with acute respiratory distress syndrome, the maximum resistance of the respiratory system decreases with PEEP, reflecting the minimum resistance response, whereas differential resistance increases with PEEP.
Keywords:Continuous positive airway pressureRespiration, artificialRespiratory distress syndrome, adultSee moreViews0Abstract
Original ArticlesEffect of PEEP on inspiratory resistance components in patients with acute respiratory distress syndrome ventilated at low tidal volume
Rev Bras Ter Intensiva. 2019;31(4):483-489
DOI 10.5935/0103-507X.20190071
- Sebastian Fredes ,
- Emilio Steinberg ,
- Norberto Tiribelli,
- Analia Santa Maria,
- Mariana Berté,
- Nicolás Segura,
- Diego Noval,
- Santiago Ilutovich
Views0ABSTRACT
Objective:
To describe the behavior of inspiratory resistance components when positive end-expiratory pressure (PEEP) increases in patients with acute respiratory distress syndrome under a protective ventilation strategy.
Methods:
In volume-controlled mode, at 6mL/kg and constant flow, end-inspiratory occlusions were performed at 0, 5 10, 15 and 20cmH2O PEEP. Peak, initial and plateau pressure values were assessed, calculating the maximum, minimum and differential resistances. The results were compared by repeated measures analysis of variance (ANOVA) with post hoc Bonferroni correction, considering p < 0.05 significant.
Results:
The highest maximum resistance was observed at the lowest PEEP levels. The values for 10 and 15cmH2O PEEP significantly differed from those for 5 and 0cmH2O PEEP, whereas that for 20cmH2O PEEP only significantly differed from that for 0cmH2O PEEP (p < 0.05). The minimum resistance behaved similarly to the maximum resistance; the values for PEEP levels from 10cmH2O to 20cmH2O significantly differed from those for 0 and 5cmH2O PEEP (p < 0.05). Differential resistance showed the opposite variation to the maximum and minimum resistances. The only PEEP level that showed significant differences from 0 and 5cmH2O PEEP was 20cmH2O PEEP. Significant differences were also found between 15 and 5cmH2O PEEP (p < 0.05).
Conclusions:
During protective ventilation in patients with acute respiratory distress syndrome, the maximum resistance of the respiratory system decreases with PEEP, reflecting the minimum resistance response, whereas differential resistance increases with PEEP.
Keywords:Continuous positive airway pressureRespiration, artificialRespiratory distress syndrome, adultSee more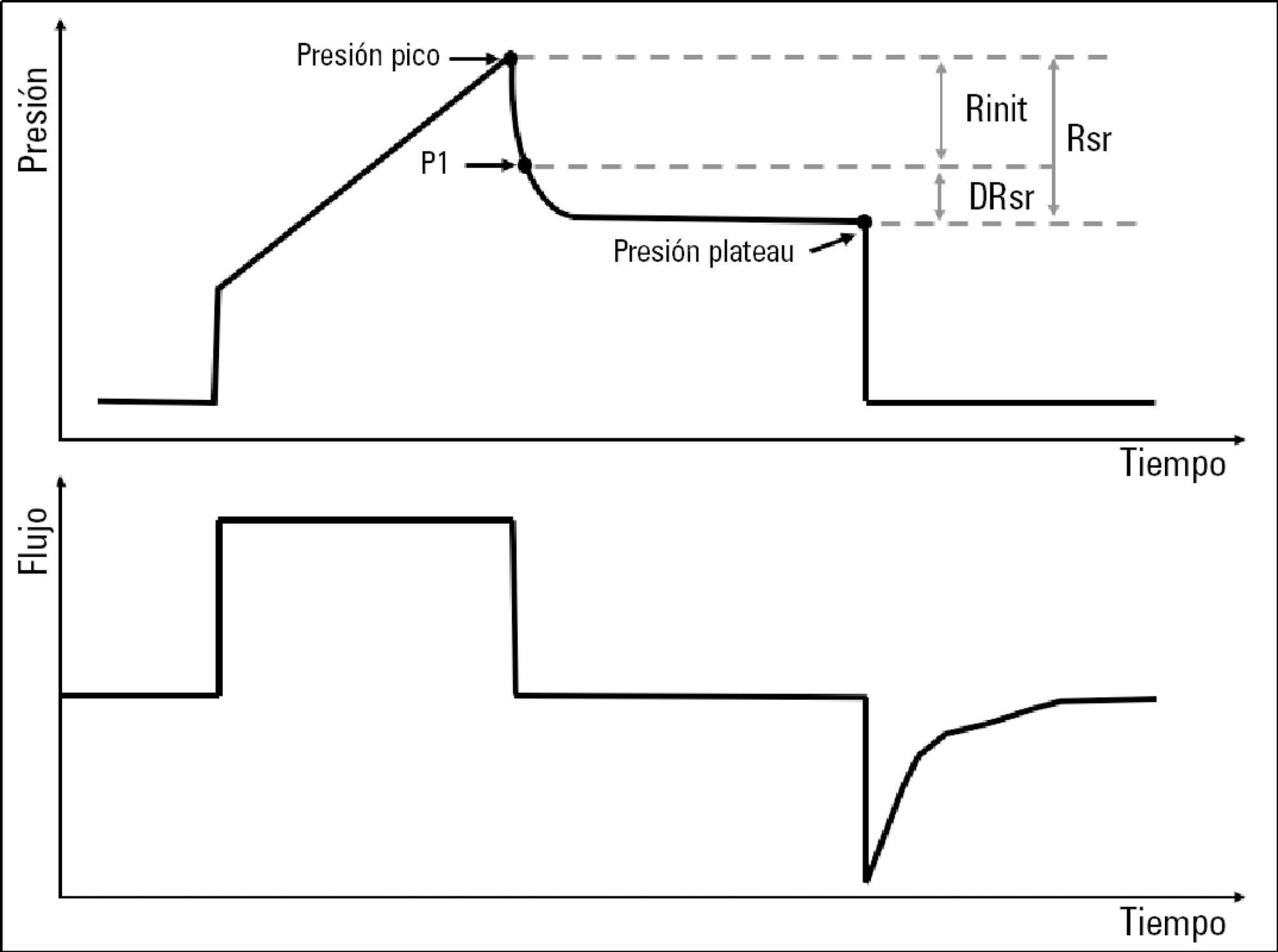
- Sebastian Fredes
-
Original Articles
Complementarity of modified NUTRIC score with or without C-reactive protein and subjective global assessment in predicting mortality in critically ill patients
- Manoela Lima Oliveira,
- Daren Keith Heyland,
- Flávia Moraes Silva ,
- Estela Iraci Rabito ,
- Mariane Rosa, [ … ],
- Aline Marcadenti
Abstract
Original ArticlesComplementarity of modified NUTRIC score with or without C-reactive protein and subjective global assessment in predicting mortality in critically ill patients
Rev Bras Ter Intensiva. 2019;31(4):490-496
DOI 10.5935/0103-507X.20190086
- Manoela Lima Oliveira,
- Daren Keith Heyland,
- Flávia Moraes Silva ,
- Estela Iraci Rabito ,
- Mariane Rosa,
- Micheli da Silva Tarnowski,
- Daieni Fernandes,
- Aline Marcadenti
Views1ABSTRACT
Objective:
To evaluate the concordance between the modified NUTRIC and NUTRIC with C-reactive protein instruments in identifying nutritional risk patients and predicting mortality in critically ill patients. The risk of death in patient groups was also investigated according to nutritional risk and malnutrition detected by subjective global assessment.
Methods:
A cohort study of patients admitted to an intensive care unit. Nutritional risk was assessed by modified NUTRIC and a version of NUTRIC with C-reactive protein. Subjective global assessment was applied to diagnose malnutrition. Kappa statistics were calculated, and an ROC curve was constructed considering modified NUTRIC as a reference. The predictive validity was assessed considering mortality in 28 days (whether in the intensive care unit or after discharge) as the outcome.
Results:
A total of 130 patients were studied (63.05 ± 16.46 years, 53.8% males). According to NUTRIC with C-reactive protein, 34.4% were classified as having a high score, while 28.5% of patients had this classification with modified NUTRIC. According to SGA 48.1% of patients were malnourished. There was excellent agreement between modified NUTRIC and NUTRIC with C-reactive protein (Kappa = 0.88, p < 0.001). The area under the ROC curve was equal to 0.942 (0.881 - 1.000) for NUTRIC with C-reactive protein. The risk of death within 28 days was increased in patients with high modified NUTRIC (HR = 1.827; 95%CI 1.029 - 3.244; p = 0.040) and NUTRIC with C-reactive protein (HR = 2.685; 95%CI 1.423 - 5.064; p = 0.002) scores. A high risk of death was observed in patients with high nutritional risk and malnutrition, independent of the version of the NUTRIC score applied.
Conclusion:
An excellent agreement between modified NUTRIC and NUTRIC with C-reactive protein was observed. In addition, combining NUTRIC and subjective global assessment may increase the accuracy of predicting mortality in critically ill patients.
Keywords:Critical careinflammationIntensive care unitsMortalityNutritionnutritional assessmentScreeningSee moreViews1Abstract
Original ArticlesComplementarity of modified NUTRIC score with or without C-reactive protein and subjective global assessment in predicting mortality in critically ill patients
Rev Bras Ter Intensiva. 2019;31(4):490-496
DOI 10.5935/0103-507X.20190086
- Manoela Lima Oliveira,
- Daren Keith Heyland,
- Flávia Moraes Silva ,
- Estela Iraci Rabito ,
- Mariane Rosa,
- Micheli da Silva Tarnowski,
- Daieni Fernandes,
- Aline Marcadenti
Views1ABSTRACT
Objective:
To evaluate the concordance between the modified NUTRIC and NUTRIC with C-reactive protein instruments in identifying nutritional risk patients and predicting mortality in critically ill patients. The risk of death in patient groups was also investigated according to nutritional risk and malnutrition detected by subjective global assessment.
Methods:
A cohort study of patients admitted to an intensive care unit. Nutritional risk was assessed by modified NUTRIC and a version of NUTRIC with C-reactive protein. Subjective global assessment was applied to diagnose malnutrition. Kappa statistics were calculated, and an ROC curve was constructed considering modified NUTRIC as a reference. The predictive validity was assessed considering mortality in 28 days (whether in the intensive care unit or after discharge) as the outcome.
Results:
A total of 130 patients were studied (63.05 ± 16.46 years, 53.8% males). According to NUTRIC with C-reactive protein, 34.4% were classified as having a high score, while 28.5% of patients had this classification with modified NUTRIC. According to SGA 48.1% of patients were malnourished. There was excellent agreement between modified NUTRIC and NUTRIC with C-reactive protein (Kappa = 0.88, p < 0.001). The area under the ROC curve was equal to 0.942 (0.881 - 1.000) for NUTRIC with C-reactive protein. The risk of death within 28 days was increased in patients with high modified NUTRIC (HR = 1.827; 95%CI 1.029 - 3.244; p = 0.040) and NUTRIC with C-reactive protein (HR = 2.685; 95%CI 1.423 - 5.064; p = 0.002) scores. A high risk of death was observed in patients with high nutritional risk and malnutrition, independent of the version of the NUTRIC score applied.
Conclusion:
An excellent agreement between modified NUTRIC and NUTRIC with C-reactive protein was observed. In addition, combining NUTRIC and subjective global assessment may increase the accuracy of predicting mortality in critically ill patients.
Keywords:Critical careinflammationIntensive care unitsMortalityNutritionnutritional assessmentScreeningSee more -
Original Articles
Association between electromyographical findings and intensive care unit mortality among mechanically ventilated acute respiratory distress syndrome patients under profound sedation
- Cassiano Teixeira ,
- Régis Goulart Rosa ,
- Juçara Gasparetto Maccari,
- Augusto Savi,
- Francisco Telechea Rotta
Abstract
Original ArticlesAssociation between electromyographical findings and intensive care unit mortality among mechanically ventilated acute respiratory distress syndrome patients under profound sedation
Rev Bras Ter Intensiva. 2019;31(4):497-503
DOI 10.5935/0103-507X.20190087
- Cassiano Teixeira ,
- Régis Goulart Rosa ,
- Juçara Gasparetto Maccari,
- Augusto Savi,
- Francisco Telechea Rotta
Views0ABSTRACT
Objective:
To evaluate whether electromyographical findings could predict intensive care unit mortality among mechanically ventilated septic patients under profound sedation.
Methods:
A prospective cohort study that consecutively enrolled moderate-severe acute respiratory distress syndrome (partial pressure of oxygen/fraction of inspired oxygen < 200) patients who were ≥ 18 years of age, dependent on mechanical ventilation for ≥ 7 days, and under profound sedation (Richmond Agitation Sedation Scale ≤ -4) was conducted. Electromyographic studies of the limbs were performed in all patients between the 7th and the 10th day of mechanical ventilation. Sensory nerve action potentials were recorded from the median and sural nerves. The compound muscle action potentials were recorded from the median (abductor pollicis brevis muscle) and common peroneal (extensor digitorum brevis muscle) nerves.
Results:
Seventeen patients were enrolled during the seven months of the study. Nine patients (53%) had electromyographic signs of critical illness myopathy or neuropathy. The risk of death during the intensive care unit stay was increased in patients with electromyographical signs of critical illness myopathy or neuropathy in comparison to those without these diagnostics (77.7% versus 12.5%, log-rank p = 0.02).
Conclusion:
Electromyographical signs of critical illness myopathy or neuropathy between the 7th and the 10th day of mechanical ventilation may be associated with intensive care unit mortality among moderate-severe acute respiratory distress syndrome patients under profound sedation, in whom clinical strength assessment is not possible.
Keywords:Critical illnessElectromyographyIntensive care unitsMortalityPolyneuropathiesPrognosisRespiration, artificialRespiratory distress syndromesedationSee moreViews0Abstract
Original ArticlesAssociation between electromyographical findings and intensive care unit mortality among mechanically ventilated acute respiratory distress syndrome patients under profound sedation
Rev Bras Ter Intensiva. 2019;31(4):497-503
DOI 10.5935/0103-507X.20190087
- Cassiano Teixeira ,
- Régis Goulart Rosa ,
- Juçara Gasparetto Maccari,
- Augusto Savi,
- Francisco Telechea Rotta
Views0ABSTRACT
Objective:
To evaluate whether electromyographical findings could predict intensive care unit mortality among mechanically ventilated septic patients under profound sedation.
Methods:
A prospective cohort study that consecutively enrolled moderate-severe acute respiratory distress syndrome (partial pressure of oxygen/fraction of inspired oxygen < 200) patients who were ≥ 18 years of age, dependent on mechanical ventilation for ≥ 7 days, and under profound sedation (Richmond Agitation Sedation Scale ≤ -4) was conducted. Electromyographic studies of the limbs were performed in all patients between the 7th and the 10th day of mechanical ventilation. Sensory nerve action potentials were recorded from the median and sural nerves. The compound muscle action potentials were recorded from the median (abductor pollicis brevis muscle) and common peroneal (extensor digitorum brevis muscle) nerves.
Results:
Seventeen patients were enrolled during the seven months of the study. Nine patients (53%) had electromyographic signs of critical illness myopathy or neuropathy. The risk of death during the intensive care unit stay was increased in patients with electromyographical signs of critical illness myopathy or neuropathy in comparison to those without these diagnostics (77.7% versus 12.5%, log-rank p = 0.02).
Conclusion:
Electromyographical signs of critical illness myopathy or neuropathy between the 7th and the 10th day of mechanical ventilation may be associated with intensive care unit mortality among moderate-severe acute respiratory distress syndrome patients under profound sedation, in whom clinical strength assessment is not possible.
Keywords:Critical illnessElectromyographyIntensive care unitsMortalityPolyneuropathiesPrognosisRespiration, artificialRespiratory distress syndromesedationSee more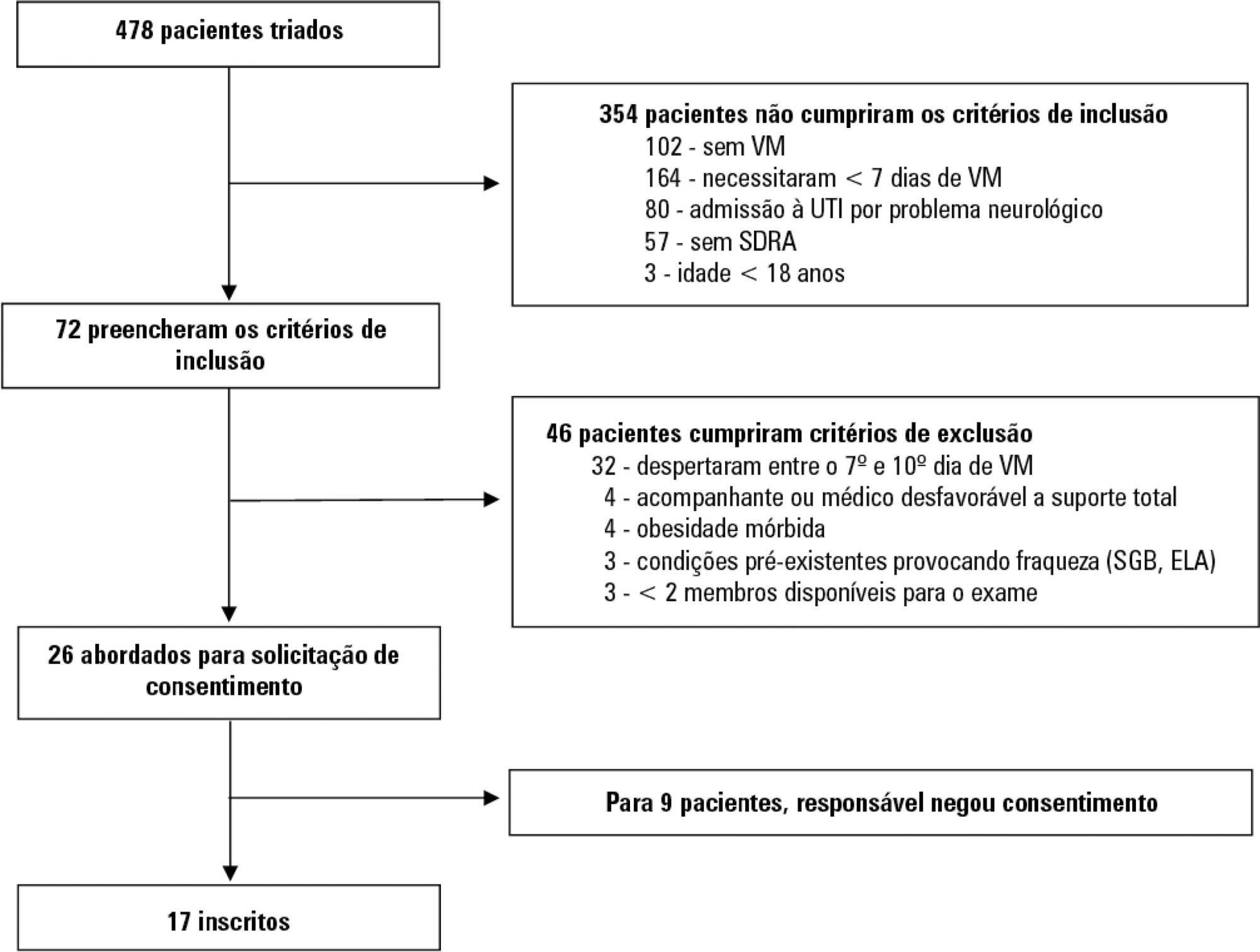
- Cassiano Teixeira
-
Original Articles
Risk factors for protein-caloric inadequacy in patients in an intensive care unit
- Celso Gustavo Ritter ,
- Irla Maiara Silva Medeiros,
- Cláudia Sena de Pádua,
- Fernanda Raphael Escobar Gimenes,
- Patrícia Rezende do Prado
Abstract
Original ArticlesRisk factors for protein-caloric inadequacy in patients in an intensive care unit
Rev Bras Ter Intensiva. 2019;31(4):504-510
DOI 10.5935/0103-507X.20190067
- Celso Gustavo Ritter ,
- Irla Maiara Silva Medeiros,
- Cláudia Sena de Pádua,
- Fernanda Raphael Escobar Gimenes,
- Patrícia Rezende do Prado
Views0ABSTRACT
Objective:
To evaluate the risk factors for protein-caloric inadequacy in critically ill patients.
Methods:
Prospective cohort study of patients hospitalized in an adult intensive care unit between February and November 2017. Patients were followed for 7 days. The conditional probability of inadequacy was calculated using the Kaplan-Meier method and the 95% log-rank test. To assess the risk of inadequacy, crude and adjusted hazard ratios (HR) were calculated using Cox regression with a 95% confidence interval.
Results:
Of the 130 patients, 63.8% were male, 73.8% were <60 years of age, and 49.2% were diagnosed with trauma. The mean APACHE II score was 24 points, and 70.0% of the patients had a protein-caloric adequacy >80%. In the univariate analysis, the significant variables for inadequacy were use of vasoactive drugs, interruptions of diet and failure to initiate nutrition early. In the final model, patients who presented with vomiting/gastric residue (adjusted HR = 22.5; 95%CI 5.14 – 98.87) and fasting for extubation (adjusted HR = 14.75; 95%CI 3.59 – 60.63) and for examinations and interventions (adjusted HR = 12.46; 95%CI 4.52 – 34.36) had a higher risk of not achieving protein-caloric adequacy.
Conclusion:
Achievement of nutritional goals > 80.0% occurred in 70.0% of patients. The risk factors for protein-caloric inadequacy were nutritional interruptions, especially due to vomiting/gastric residue and fasting for extubation, exams and surgical procedures.
Keywords:Critical illnessenteral nutritionIntensive care unitsnutrition assessmentnutrition therapyNutrition, public healthrisk factorsSee moreViews0Abstract
Original ArticlesRisk factors for protein-caloric inadequacy in patients in an intensive care unit
Rev Bras Ter Intensiva. 2019;31(4):504-510
DOI 10.5935/0103-507X.20190067
- Celso Gustavo Ritter ,
- Irla Maiara Silva Medeiros,
- Cláudia Sena de Pádua,
- Fernanda Raphael Escobar Gimenes,
- Patrícia Rezende do Prado
Views0ABSTRACT
Objective:
To evaluate the risk factors for protein-caloric inadequacy in critically ill patients.
Methods:
Prospective cohort study of patients hospitalized in an adult intensive care unit between February and November 2017. Patients were followed for 7 days. The conditional probability of inadequacy was calculated using the Kaplan-Meier method and the 95% log-rank test. To assess the risk of inadequacy, crude and adjusted hazard ratios (HR) were calculated using Cox regression with a 95% confidence interval.
Results:
Of the 130 patients, 63.8% were male, 73.8% were <60 years of age, and 49.2% were diagnosed with trauma. The mean APACHE II score was 24 points, and 70.0% of the patients had a protein-caloric adequacy >80%. In the univariate analysis, the significant variables for inadequacy were use of vasoactive drugs, interruptions of diet and failure to initiate nutrition early. In the final model, patients who presented with vomiting/gastric residue (adjusted HR = 22.5; 95%CI 5.14 – 98.87) and fasting for extubation (adjusted HR = 14.75; 95%CI 3.59 – 60.63) and for examinations and interventions (adjusted HR = 12.46; 95%CI 4.52 – 34.36) had a higher risk of not achieving protein-caloric adequacy.
Conclusion:
Achievement of nutritional goals > 80.0% occurred in 70.0% of patients. The risk factors for protein-caloric inadequacy were nutritional interruptions, especially due to vomiting/gastric residue and fasting for extubation, exams and surgical procedures.
Keywords:Critical illnessenteral nutritionIntensive care unitsnutrition assessmentnutrition therapyNutrition, public healthrisk factorsSee more - Celso Gustavo Ritter
-
Original Articles
Characteristics and predictors of chronic critical illness in the intensive care unit
- Fernanda Perito Aguiar,
- Glauco Adrieno Westphal ,
- Michelli Marcela Dadam,
- Elisa Cristina Correia Mota,
- Felipe Pfutzenreuter, [ … ],
- Paulo Henrique Condeixa França
Abstract
Original ArticlesCharacteristics and predictors of chronic critical illness in the intensive care unit
Rev Bras Ter Intensiva. 2019;31(4):511-520
DOI 10.5935/0103-507X.20190088
- Fernanda Perito Aguiar,
- Glauco Adrieno Westphal ,
- Michelli Marcela Dadam,
- Elisa Cristina Correia Mota,
- Felipe Pfutzenreuter,
- Paulo Henrique Condeixa França
Views1See moreABSTRACT
Objective:
To characterize patients with chronic critical illness and identify predictors of development of chronic critical illness.
Methods:
Prospective data was collected for 1 year in the intensive care unit of a general hospital in Southern Brazil. Three logistic regression models were constructed to identify factors associated with chronic critical illness.
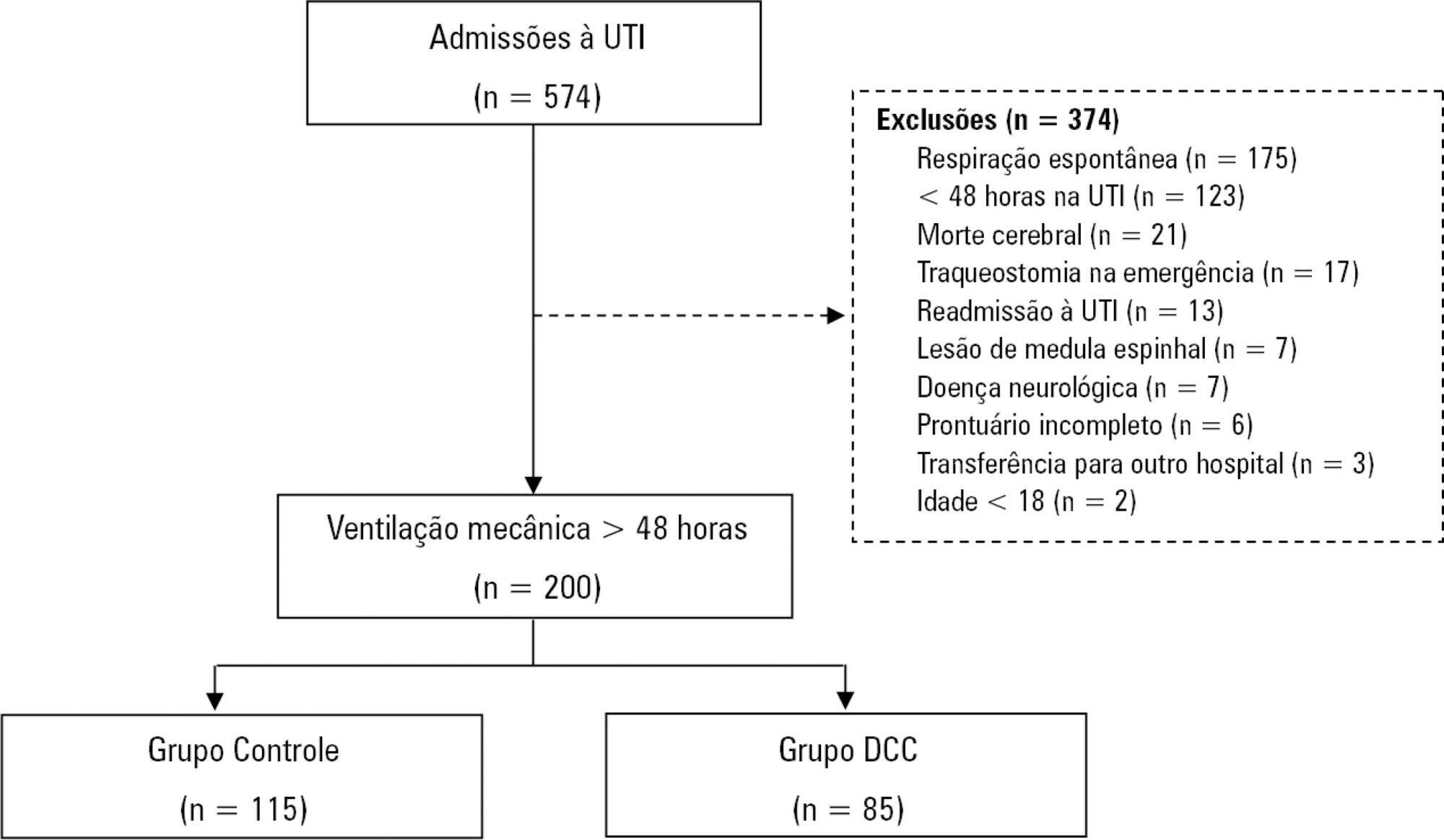
Results:
Among the 574 subjects admitted to the intensive care unit, 200 were submitted to mechanical ventilation. Of these patients, 85 (43.5%) developed chronic critical illness, composing 14.8% of all the patients admitted to the intensive care unit. The regression model that evaluated the association of chronic critical illness with conditions present prior to intensive care unit admission identified chronic renal failure in patients undergoing hemodialysis (OR 3.57; p = 0.04) and a neurological diagnosis at hospital admission (OR 2.25; p = 0.008) as independent factors. In the model that evaluated the association of chronic critical illness with situations that occurred during intensive care unit stay, muscle weakness (OR 2.86; p = 0.01) and pressure ulcers (OR 9.54; p < 0.001) had the strongest associations. In the global multivariate analysis (that assessed previous factors and situations that occurred in the intensive care unit), hospital admission due to neurological diseases (OR 2.61; p = 0.03) and the development of pressure ulcers (OR 9.08; p < 0.001) had the strongest associations.
Conclusion:
The incidence of chronic critical illness in this study was similar to that observed in other studies and had a strong association with the diagnosis of neurological diseases at hospital admission and chronic renal failure in patients undergoing hemodialysis, as well as complications developed during hospitalization, such as pressure ulcers and muscle weakness.
Views1Abstract
Original ArticlesCharacteristics and predictors of chronic critical illness in the intensive care unit
Rev Bras Ter Intensiva. 2019;31(4):511-520
DOI 10.5935/0103-507X.20190088
- Fernanda Perito Aguiar,
- Glauco Adrieno Westphal ,
- Michelli Marcela Dadam,
- Elisa Cristina Correia Mota,
- Felipe Pfutzenreuter,
- Paulo Henrique Condeixa França
Views1See moreABSTRACT
Objective:
To characterize patients with chronic critical illness and identify predictors of development of chronic critical illness.
Methods:
Prospective data was collected for 1 year in the intensive care unit of a general hospital in Southern Brazil. Three logistic regression models were constructed to identify factors associated with chronic critical illness.
Results:
Among the 574 subjects admitted to the intensive care unit, 200 were submitted to mechanical ventilation. Of these patients, 85 (43.5%) developed chronic critical illness, composing 14.8% of all the patients admitted to the intensive care unit. The regression model that evaluated the association of chronic critical illness with conditions present prior to intensive care unit admission identified chronic renal failure in patients undergoing hemodialysis (OR 3.57; p = 0.04) and a neurological diagnosis at hospital admission (OR 2.25; p = 0.008) as independent factors. In the model that evaluated the association of chronic critical illness with situations that occurred during intensive care unit stay, muscle weakness (OR 2.86; p = 0.01) and pressure ulcers (OR 9.54; p < 0.001) had the strongest associations. In the global multivariate analysis (that assessed previous factors and situations that occurred in the intensive care unit), hospital admission due to neurological diseases (OR 2.61; p = 0.03) and the development of pressure ulcers (OR 9.08; p < 0.001) had the strongest associations.
Conclusion:
The incidence of chronic critical illness in this study was similar to that observed in other studies and had a strong association with the diagnosis of neurological diseases at hospital admission and chronic renal failure in patients undergoing hemodialysis, as well as complications developed during hospitalization, such as pressure ulcers and muscle weakness.
-
Original Articles
Assessment of the measurement properties of the Brazilian versions of the Functional Status Score for the ICU and the Functional Independence Measure in critically ill patients in the intensive care unit
Rev Bras Ter Intensiva. 2019;31(4):521-528
Abstract
Original ArticlesAssessment of the measurement properties of the Brazilian versions of the Functional Status Score for the ICU and the Functional Independence Measure in critically ill patients in the intensive care unit
Rev Bras Ter Intensiva. 2019;31(4):521-528
DOI 10.5935/0103-507X.20190065
Views1See moreABSTRACT
Objective:
To compare the measurement properties (internal consistency, intra and interrater reliability, construct validity, and ceiling and floor effects) of the Functional Status Score for the ICU (FSS-ICU) and the Functional Independence Measure (FIM-motor domain).
Methods:
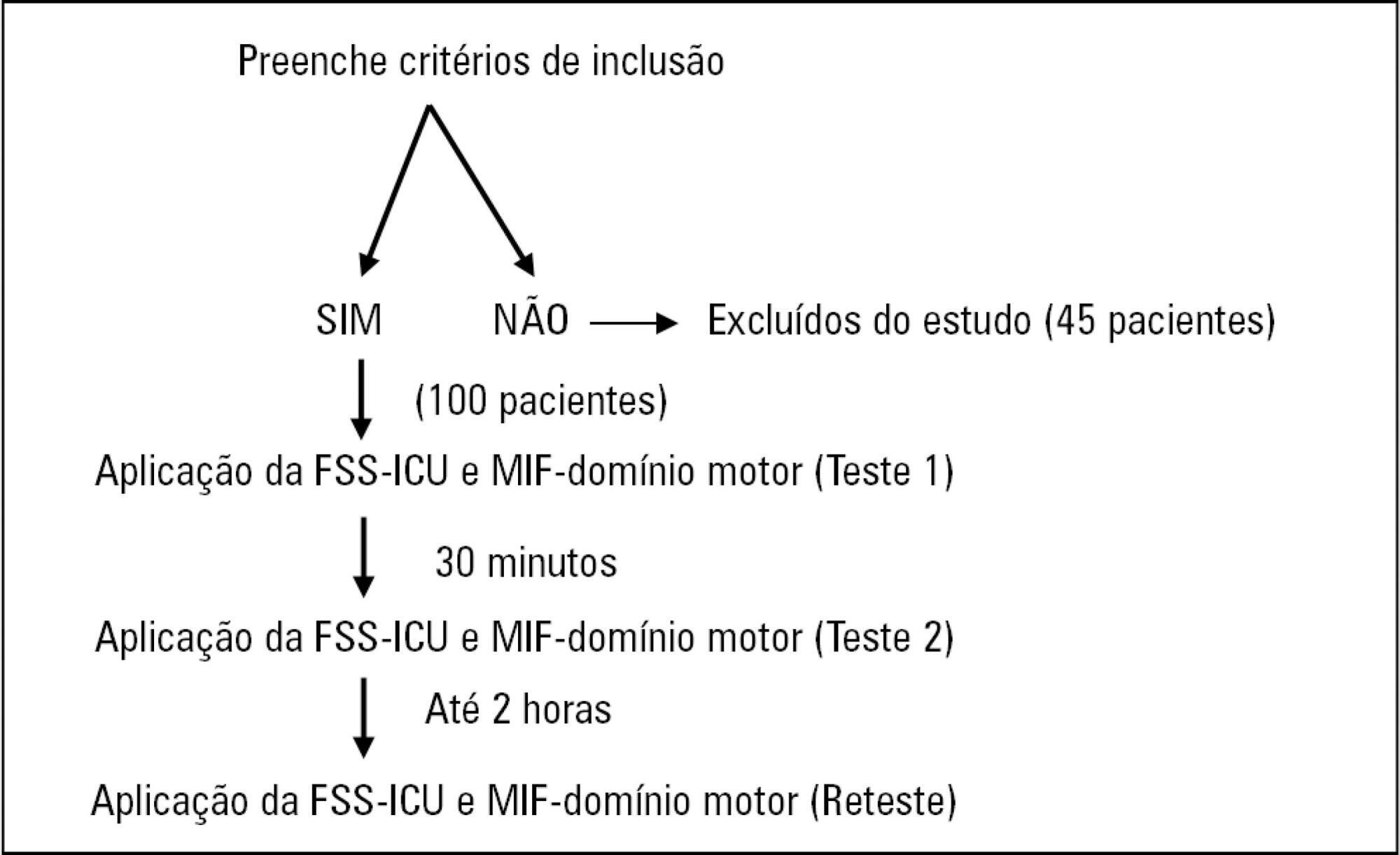
In this study of measurement properties, the FSS-ICU and FIM were applied to 100 patients (72.1 ± 15.9 years; 53% male; Sequential Organ Failure Assessment = 11.0 ± 3.5 points, Simplified Acute Physiology Score 3 = 50.2 ± 16.8 points) in an intensive care unit at baseline and after 2 hours by physiotherapist 1 (test and retest) and 30 minutes after baseline by physiotherapist 2. The measurement properties evaluated were internal consistency (Cronbach’s alpha), intra- and interrater reliability (intraclass correlation coefficient), agreement (standard error of measurement) and minimum detectable change at a 90% confidence level, ceiling and floor effects (frequency of maximum and minimum scores) and construct validity (Pearson’s correlation).
Results:
The FSS-ICU and FIM presented adequate internal consistency (Cronbach’s alpha, FSS-ICU = 0.95 and FIM = 0.86), intra-and interrater reliability for overall FSS-ICU and FIM score (ICC > 0.75), agreement (minimum detectable change at a 90% confidence level: FSS-ICU and FIM = 1.0 point; standard error of measurement: FSS-ICU = 2% and FIM = 1%) and construct validity (r = 0.94; p < 0.001). However, the FSS-ICU and FIM presented ceiling effects (maximum score for 16% of patients for the FSS-ICU and 18% for the FIM).
Conclusion:
The FSS-ICU and FIM present adequate measurement properties to assess functionality in critically ill patients, although they present ceiling effects.
Views1Abstract
Original ArticlesAssessment of the measurement properties of the Brazilian versions of the Functional Status Score for the ICU and the Functional Independence Measure in critically ill patients in the intensive care unit
Rev Bras Ter Intensiva. 2019;31(4):521-528
DOI 10.5935/0103-507X.20190065
Views1See moreABSTRACT
Objective:
To compare the measurement properties (internal consistency, intra and interrater reliability, construct validity, and ceiling and floor effects) of the Functional Status Score for the ICU (FSS-ICU) and the Functional Independence Measure (FIM-motor domain).
Methods:
In this study of measurement properties, the FSS-ICU and FIM were applied to 100 patients (72.1 ± 15.9 years; 53% male; Sequential Organ Failure Assessment = 11.0 ± 3.5 points, Simplified Acute Physiology Score 3 = 50.2 ± 16.8 points) in an intensive care unit at baseline and after 2 hours by physiotherapist 1 (test and retest) and 30 minutes after baseline by physiotherapist 2. The measurement properties evaluated were internal consistency (Cronbach’s alpha), intra- and interrater reliability (intraclass correlation coefficient), agreement (standard error of measurement) and minimum detectable change at a 90% confidence level, ceiling and floor effects (frequency of maximum and minimum scores) and construct validity (Pearson’s correlation).
Results:
The FSS-ICU and FIM presented adequate internal consistency (Cronbach’s alpha, FSS-ICU = 0.95 and FIM = 0.86), intra-and interrater reliability for overall FSS-ICU and FIM score (ICC > 0.75), agreement (minimum detectable change at a 90% confidence level: FSS-ICU and FIM = 1.0 point; standard error of measurement: FSS-ICU = 2% and FIM = 1%) and construct validity (r = 0.94; p < 0.001). However, the FSS-ICU and FIM presented ceiling effects (maximum score for 16% of patients for the FSS-ICU and 18% for the FIM).
Conclusion:
The FSS-ICU and FIM present adequate measurement properties to assess functionality in critically ill patients, although they present ceiling effects.
-
Original Articles
Patient functionality and walking speed after discharge from the intensive care unit
Rev Bras Ter Intensiva. 2019;31(4):529-535
Abstract
Original ArticlesPatient functionality and walking speed after discharge from the intensive care unit
Rev Bras Ter Intensiva. 2019;31(4):529-535
DOI 10.5935/0103-507X.20190066
Views0ABSTRACT
Objective:
To measure and compare the functionality of patients after discharge from the intensive care unit and at the time of hospital discharge.
Methods:
Quantitative study of a prospective cohort performed between August of 2016 and December of 2017 at a university hospital. A 10-meter walk test was performed at 2 timepoints: after discharge from the intensive care unit and prior to hospital discharge. The data were analyzed using Student’s t-test and Pearson or Spearman correlation. Statistical Package for Social Science (SPSS) version 21.0 was used for the analysis, and p ≤ 0.05 was adopted as the level of significance.
Results:
Forty patients, with a mean age of 57.1 ± 12.2 years and with a predominance of males (60%), were evaluated. For the post-intensive care unit test, a mean speed of 0.48m/s was observed, and for the pre-hospital discharge test, there was an increase to 0.71m/s, evidencing functional evolution during the hospital stay (p < 0.001).
Conclusion:
There was significant improvement in walking speed at the time of hospital discharge when compared to the walking speed at the time of intensive care unit discharge.
Keywords:Critical careEarly ambulationExerciseIntensive care unitsMuscle strengthPatient carePatient dischargeWalk testSee moreViews0Abstract
Original ArticlesPatient functionality and walking speed after discharge from the intensive care unit
Rev Bras Ter Intensiva. 2019;31(4):529-535
DOI 10.5935/0103-507X.20190066
Views0ABSTRACT
Objective:
To measure and compare the functionality of patients after discharge from the intensive care unit and at the time of hospital discharge.
Methods:
Quantitative study of a prospective cohort performed between August of 2016 and December of 2017 at a university hospital. A 10-meter walk test was performed at 2 timepoints: after discharge from the intensive care unit and prior to hospital discharge. The data were analyzed using Student’s t-test and Pearson or Spearman correlation. Statistical Package for Social Science (SPSS) version 21.0 was used for the analysis, and p ≤ 0.05 was adopted as the level of significance.
Results:
Forty patients, with a mean age of 57.1 ± 12.2 years and with a predominance of males (60%), were evaluated. For the post-intensive care unit test, a mean speed of 0.48m/s was observed, and for the pre-hospital discharge test, there was an increase to 0.71m/s, evidencing functional evolution during the hospital stay (p < 0.001).
Conclusion:
There was significant improvement in walking speed at the time of hospital discharge when compared to the walking speed at the time of intensive care unit discharge.
Keywords:Critical careEarly ambulationExerciseIntensive care unitsMuscle strengthPatient carePatient dischargeWalk testSee more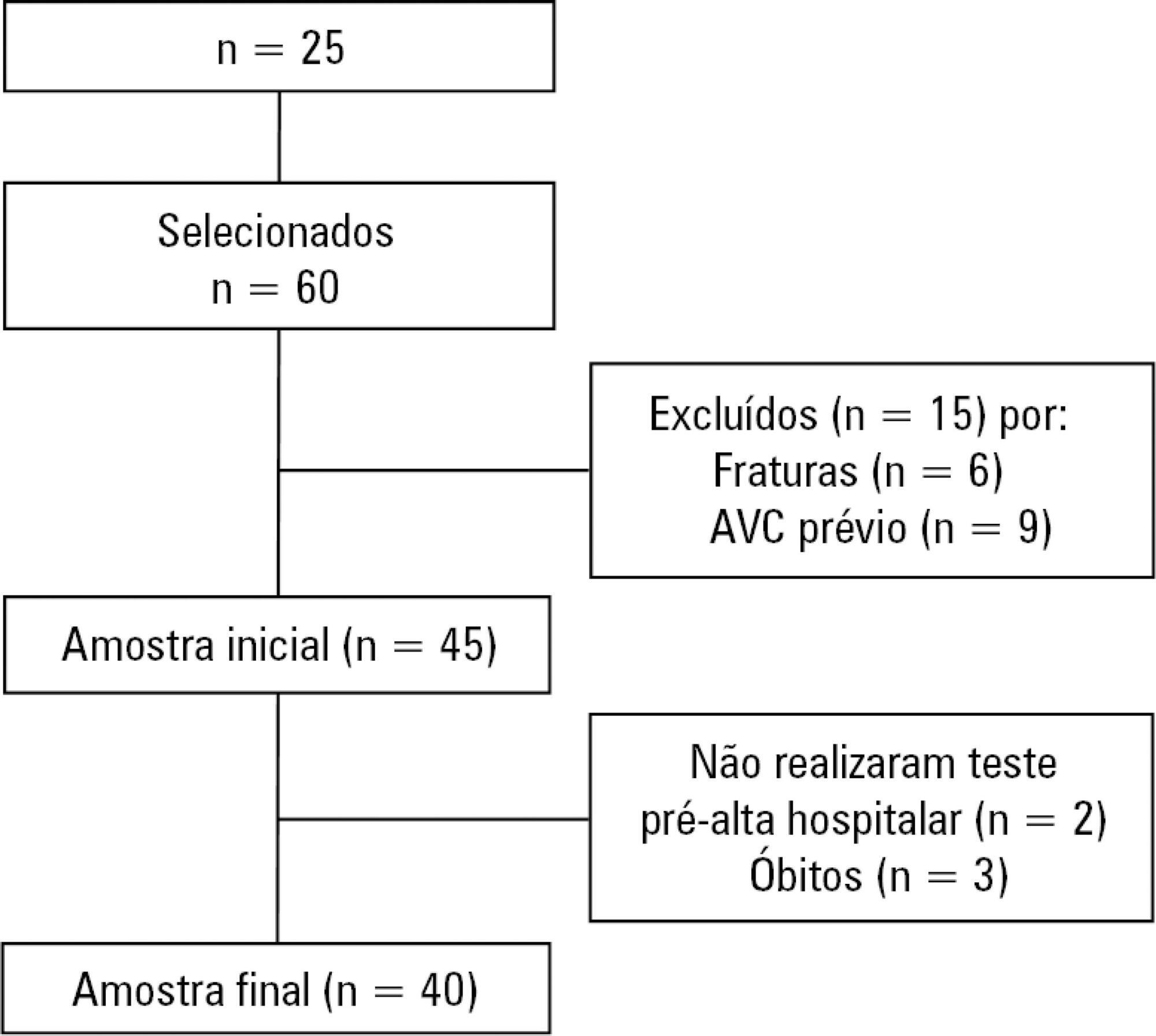
-
Original Articles
Delirium in cancer patients admitted to the intensive care unit: a retrospective study
Rev Bras Ter Intensiva. 2019;31(4):536-540
Abstract
Original ArticlesDelirium in cancer patients admitted to the intensive care unit: a retrospective study
Rev Bras Ter Intensiva. 2019;31(4):536-540
DOI 10.5935/0103-507X.20190064
Views0ABSTRACT
Objective:
To describe the occurrence of delirium in cancer patients admitted to the intensive care unit according to clinical and demographic characteristics.
Methods:
A retrospective study was conducted with 135 adults admitted to the intensive care unit of a public cancer hospital in the city of Rio de Janeiro, Brazil, between January and March 2016. Fisher’s exact test and the linear association test were used to identify statistically significant associations between the occurrence of delirium and categorical and ordinal variables, respectively, considering a p-value < 0.05.
Results:
The overall occurrence of delirium was 39.3%. Delirium was more frequent among individuals aged 60 years or older and those who required extensive assistance or were bedbound, were admitted to the intensive care unit for clinical reasons, were using sedative drugs, were undergoing chemotherapy, and those who remained 8 or more days in the intensive care unit. Considering only patients on mechanical ventilation, the overall occurrence of delirium was 64.6%, and only a length of stay in the intensive care unit ≥ 8 days showed a statistically significant association with delirium.
Conclusion:
The occurrence of delirium in critically ill cancer patients is high. When only those on mechanical ventilation are considered, the occurrence of delirium is even greater.
Keywords:Delirium/epidemiologyDrug-related side effects and adverse reactionsIntensive care unitsNeoplasms/complicationsRespiration, artificialSee moreViews0Abstract
Original ArticlesDelirium in cancer patients admitted to the intensive care unit: a retrospective study
Rev Bras Ter Intensiva. 2019;31(4):536-540
DOI 10.5935/0103-507X.20190064
Views0ABSTRACT
Objective:
To describe the occurrence of delirium in cancer patients admitted to the intensive care unit according to clinical and demographic characteristics.
Methods:
A retrospective study was conducted with 135 adults admitted to the intensive care unit of a public cancer hospital in the city of Rio de Janeiro, Brazil, between January and March 2016. Fisher’s exact test and the linear association test were used to identify statistically significant associations between the occurrence of delirium and categorical and ordinal variables, respectively, considering a p-value < 0.05.
Results:
The overall occurrence of delirium was 39.3%. Delirium was more frequent among individuals aged 60 years or older and those who required extensive assistance or were bedbound, were admitted to the intensive care unit for clinical reasons, were using sedative drugs, were undergoing chemotherapy, and those who remained 8 or more days in the intensive care unit. Considering only patients on mechanical ventilation, the overall occurrence of delirium was 64.6%, and only a length of stay in the intensive care unit ≥ 8 days showed a statistically significant association with delirium.
Conclusion:
The occurrence of delirium in critically ill cancer patients is high. When only those on mechanical ventilation are considered, the occurrence of delirium is even greater.
Keywords:Delirium/epidemiologyDrug-related side effects and adverse reactionsIntensive care unitsNeoplasms/complicationsRespiration, artificialSee more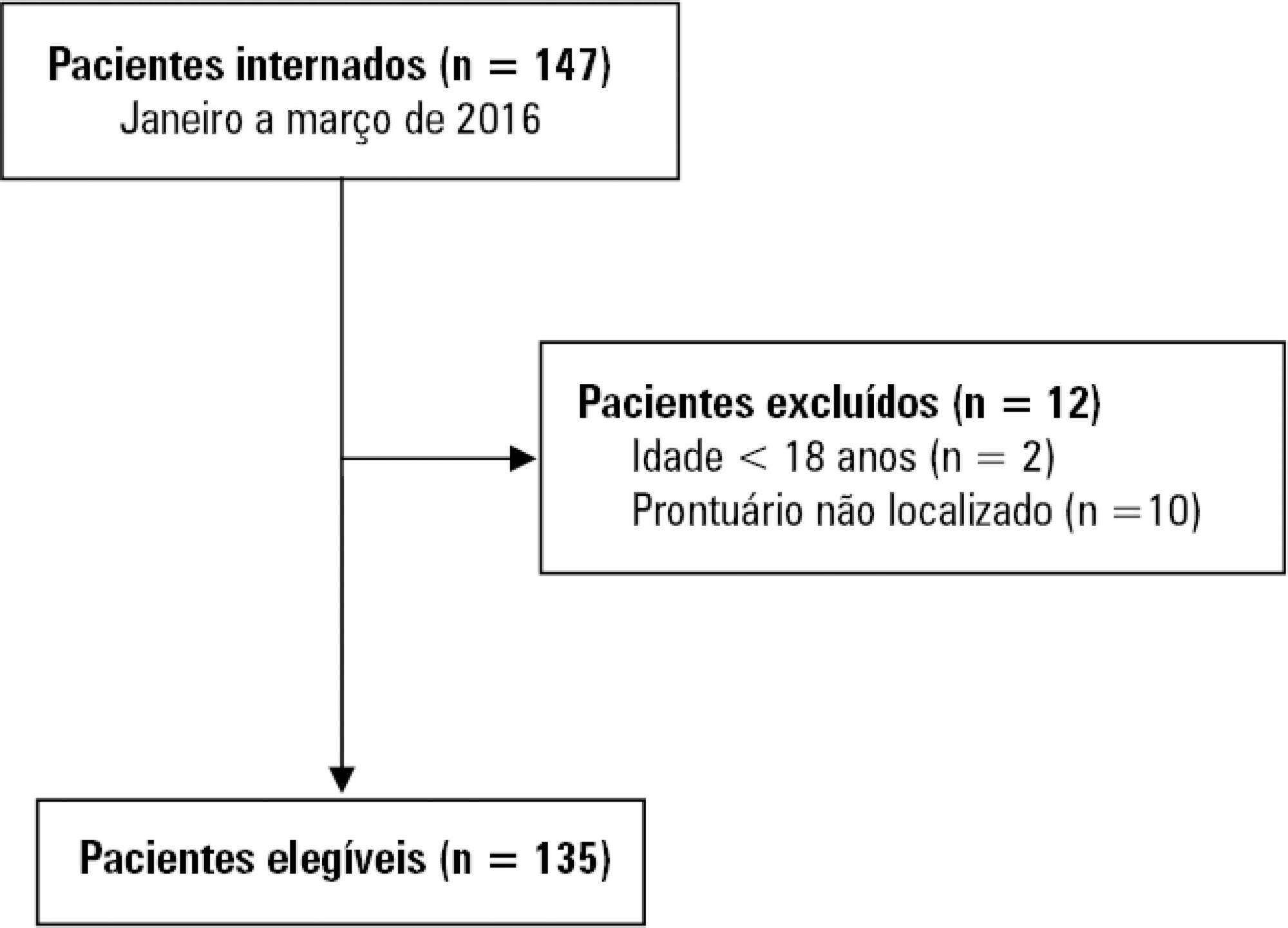
-
Review Articles
Ventilator-associated tracheobronchitis: an update
- Jorge Ibrain Figueira Salluh,
- Vicente Cés de Souza-Dantas ,
- Ignacio Martin-Loeches,
- Thiago Costa Lisboa,
- Ligia Sarmet Cunha Farah Rabello, [ … ],
- Pedro Póvoa
Abstract
Review ArticlesVentilator-associated tracheobronchitis: an update
Rev Bras Ter Intensiva. 2019;31(4):541-547
DOI 10.5935/0103-507X.20190079
- Jorge Ibrain Figueira Salluh,
- Vicente Cés de Souza-Dantas ,
- Ignacio Martin-Loeches,
- Thiago Costa Lisboa,
- Ligia Sarmet Cunha Farah Rabello,
- Saad Nseir ,
- Pedro Póvoa
Views0ABSTRACT
Ventilator-associated lower respiratory tract infection is one of the most frequent complications in mechanically ventilated patients. Ventilator-associated tracheobronchitis has been considered a disease that does not warrant antibiotic treatment by the medical community for many years. In the last decade, several studies have shown that tracheobronchitis could be considered an intermediate process that leads to ventilator-associated pneumonia. Furthermore, ventilator-associated tracheobronchitis has a limited impact on overall mortality but shows a significant association with increased patient costs, length of stay, antibiotic use, and duration of mechanical ventilation. Although we still need clear evidence, especially concerning treatment modalities, the present study on ventilator-associated tracheobronchitis highlights that there are important impacts of including this condition in clinical management and epidemiological and infection surveillance.
Keywords:Critical careHealthcare-associated pneumoniaMortalityNosocomial infectionPneumoniaPneumonia, ventilator-associatedVentilator-associated tracheobronchitisSee moreViews0Abstract
Review ArticlesVentilator-associated tracheobronchitis: an update
Rev Bras Ter Intensiva. 2019;31(4):541-547
DOI 10.5935/0103-507X.20190079
- Jorge Ibrain Figueira Salluh,
- Vicente Cés de Souza-Dantas ,
- Ignacio Martin-Loeches,
- Thiago Costa Lisboa,
- Ligia Sarmet Cunha Farah Rabello,
- Saad Nseir ,
- Pedro Póvoa
Views0ABSTRACT
Ventilator-associated lower respiratory tract infection is one of the most frequent complications in mechanically ventilated patients. Ventilator-associated tracheobronchitis has been considered a disease that does not warrant antibiotic treatment by the medical community for many years. In the last decade, several studies have shown that tracheobronchitis could be considered an intermediate process that leads to ventilator-associated pneumonia. Furthermore, ventilator-associated tracheobronchitis has a limited impact on overall mortality but shows a significant association with increased patient costs, length of stay, antibiotic use, and duration of mechanical ventilation. Although we still need clear evidence, especially concerning treatment modalities, the present study on ventilator-associated tracheobronchitis highlights that there are important impacts of including this condition in clinical management and epidemiological and infection surveillance.
Keywords:Critical careHealthcare-associated pneumoniaMortalityNosocomial infectionPneumoniaPneumonia, ventilator-associatedVentilator-associated tracheobronchitisSee more -
Review Articles
Extracorporeal membrane oxygenation for severe acute respiratory distress syndrome in adult patients: a systematic review and meta-analysis
- Pedro Vitale Mendes,
- Livia Maria Garcia Melro,
- Ho Yeh Li,
- Daniel Joelsons ,
- Rogerio Zigaib, [ … ],
- Marcelo Park
Abstract
Review ArticlesExtracorporeal membrane oxygenation for severe acute respiratory distress syndrome in adult patients: a systematic review and meta-analysis
Rev Bras Ter Intensiva. 2019;31(4):548-554
DOI 10.5935/0103-507X.20190077
- Pedro Vitale Mendes,
- Livia Maria Garcia Melro,
- Ho Yeh Li,
- Daniel Joelsons ,
- Rogerio Zigaib,
- José Mauro da Fonseca Pestana Ribeiro,
- Bruno Adler Maccagnan Pinheiro Besen ,
- Marcelo Park
Views0ABSTRACT
Objective:
The evidence of improved survival with the use of extracorporeal membrane oxygenation (ECMO) in acute respiratory distress syndrome is still uncertain.
Methods:
This systematic review and meta-analysis was registered in the PROSPERO database with the number CRD-42018098618. We performed a structured search of Medline, Lilacs, and ScienceDirect for randomized controlled trials evaluating the use of ECMO associated with (ultra)protective mechanical ventilation for severe acute respiratory failure in adult patients. We used the Cochrane risk of bias tool to evaluate the quality of the evidence. Our primary objective was to evaluate the effect of ECMO on the last reported mortality. Secondary outcomes were treatment failure, hospital length of stay and the need for renal replacement therapy in both groups.
Results:
Two randomized controlled studies were included in the meta-analysis, comprising 429 patients, of whom 214 were supported with ECMO. The most common reason for acute respiratory failure was pneumonia (60% – 65%). Respiratory ECMO support was associated with a reduction in last reported mortality and treatment failure with risk ratios (RR: 0.76; 95%CI 0.61 – 0.95 and RR: 0.68; 95%CI 0.55 – 0.85, respectively). Extracorporeal membrane oxygenation reduced the need for renal replacement therapy, with a RR of 0.88 (95%CI 0.77 – 0.99). Intensive care unit and hospital lengths of stay were longer in ECMO-supported patients, with an additional P50th 14.84 (P25th – P75th: 12.49 – 17.18) and P50th 29.80 (P25th – P75th: 26.04 – 33.56] days, respectively.
Conclusion:
Respiratory ECMO support in severe acute respiratory distress syndrome patients is associated with a reduced mortality rate and a reduced need for renal replacement therapy but a substantial increase in the lengths of stay in the intensive care unit and hospital. Our results may help bedside decision-making regarding ECMO initiation in patients with severe respiratory distress syndrome.
Keywords:Extracorporeal membrane oxygenationIntensive care unitsMeta-analysisRespiratory distress syndrome, adultRespiratory insufficiencySee moreViews0Abstract
Review ArticlesExtracorporeal membrane oxygenation for severe acute respiratory distress syndrome in adult patients: a systematic review and meta-analysis
Rev Bras Ter Intensiva. 2019;31(4):548-554
DOI 10.5935/0103-507X.20190077
- Pedro Vitale Mendes,
- Livia Maria Garcia Melro,
- Ho Yeh Li,
- Daniel Joelsons ,
- Rogerio Zigaib,
- José Mauro da Fonseca Pestana Ribeiro,
- Bruno Adler Maccagnan Pinheiro Besen ,
- Marcelo Park
Views0ABSTRACT
Objective:
The evidence of improved survival with the use of extracorporeal membrane oxygenation (ECMO) in acute respiratory distress syndrome is still uncertain.
Methods:
This systematic review and meta-analysis was registered in the PROSPERO database with the number CRD-42018098618. We performed a structured search of Medline, Lilacs, and ScienceDirect for randomized controlled trials evaluating the use of ECMO associated with (ultra)protective mechanical ventilation for severe acute respiratory failure in adult patients. We used the Cochrane risk of bias tool to evaluate the quality of the evidence. Our primary objective was to evaluate the effect of ECMO on the last reported mortality. Secondary outcomes were treatment failure, hospital length of stay and the need for renal replacement therapy in both groups.
Results:
Two randomized controlled studies were included in the meta-analysis, comprising 429 patients, of whom 214 were supported with ECMO. The most common reason for acute respiratory failure was pneumonia (60% – 65%). Respiratory ECMO support was associated with a reduction in last reported mortality and treatment failure with risk ratios (RR: 0.76; 95%CI 0.61 – 0.95 and RR: 0.68; 95%CI 0.55 – 0.85, respectively). Extracorporeal membrane oxygenation reduced the need for renal replacement therapy, with a RR of 0.88 (95%CI 0.77 – 0.99). Intensive care unit and hospital lengths of stay were longer in ECMO-supported patients, with an additional P50th 14.84 (P25th – P75th: 12.49 – 17.18) and P50th 29.80 (P25th – P75th: 26.04 – 33.56] days, respectively.
Conclusion:
Respiratory ECMO support in severe acute respiratory distress syndrome patients is associated with a reduced mortality rate and a reduced need for renal replacement therapy but a substantial increase in the lengths of stay in the intensive care unit and hospital. Our results may help bedside decision-making regarding ECMO initiation in patients with severe respiratory distress syndrome.
Keywords:Extracorporeal membrane oxygenationIntensive care unitsMeta-analysisRespiratory distress syndrome, adultRespiratory insufficiencySee more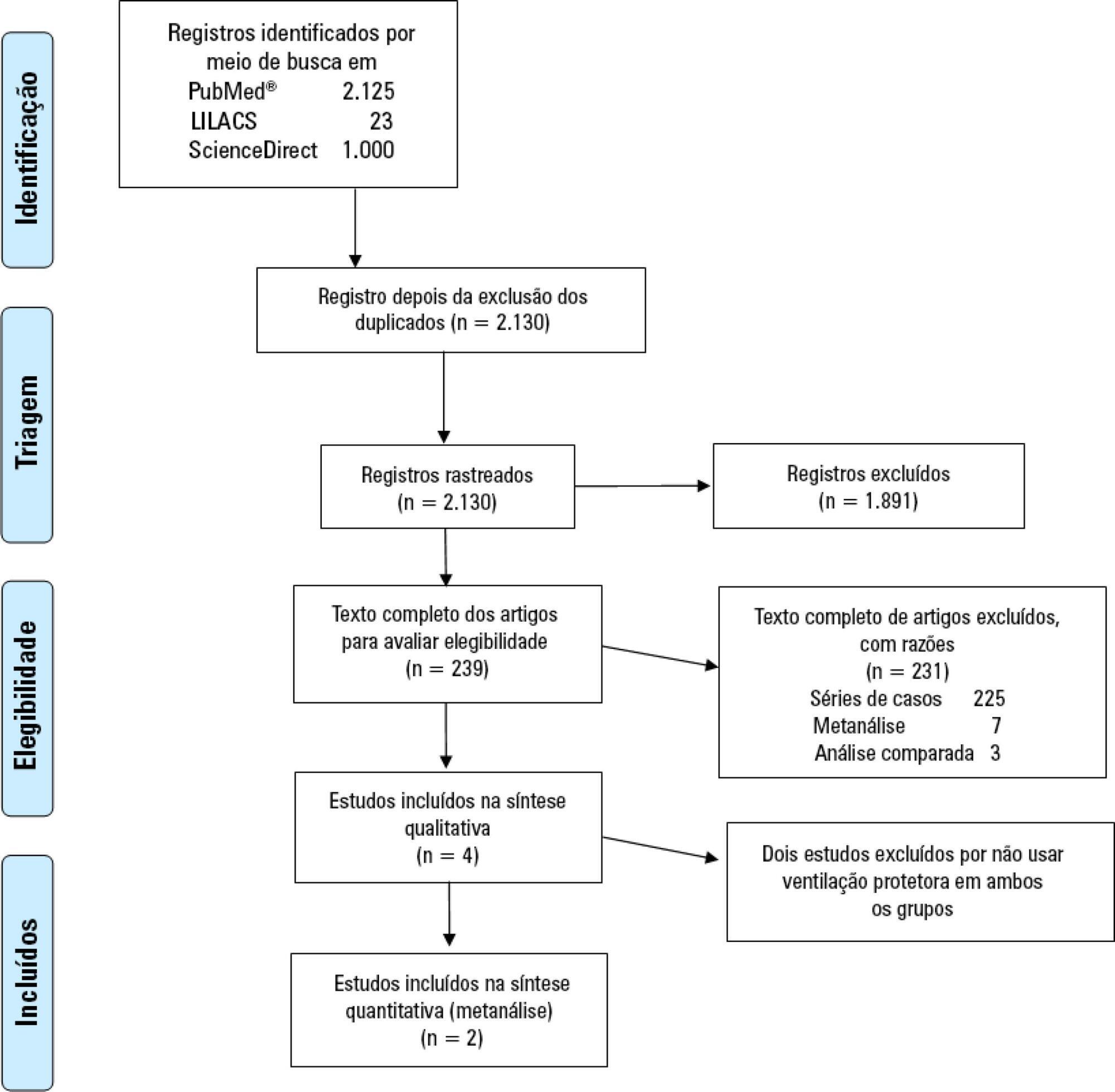
-
Review Articles
Acute respiratory distress syndrome: how do patients fare after the intensive care unit?
Rev Bras Ter Intensiva. 2019;31(4):555-560
Abstract
Review ArticlesAcute respiratory distress syndrome: how do patients fare after the intensive care unit?
Rev Bras Ter Intensiva. 2019;31(4):555-560
DOI 10.5935/0103-507X.20190074
Views0See moreABSTRACT
Patients with acute respiratory distress syndrome require ventilation strategies that have been shown to be important for reducing short-term mortality, such as protective ventilation and prone position ventilation. However, patients who survive have a prolonged stay in both the intensive care unit and the hospital, and they experience a reduction in overall satisfaction with life (independence, acceptance and positive outlook) as well as decreased mental health (including anxiety, depression and posttraumatic stress disorder symptoms), physical health (impaired physical state and activities of daily living; fatigue and muscle weakness), social health and the ability to participate in social activities (including relationships with friends and family, hobbies and social gatherings).
Views0Abstract
Review ArticlesAcute respiratory distress syndrome: how do patients fare after the intensive care unit?
Rev Bras Ter Intensiva. 2019;31(4):555-560
DOI 10.5935/0103-507X.20190074
Views0See moreABSTRACT
Patients with acute respiratory distress syndrome require ventilation strategies that have been shown to be important for reducing short-term mortality, such as protective ventilation and prone position ventilation. However, patients who survive have a prolonged stay in both the intensive care unit and the hospital, and they experience a reduction in overall satisfaction with life (independence, acceptance and positive outlook) as well as decreased mental health (including anxiety, depression and posttraumatic stress disorder symptoms), physical health (impaired physical state and activities of daily living; fatigue and muscle weakness), social health and the ability to participate in social activities (including relationships with friends and family, hobbies and social gatherings).
-
Review Articles
Approach to the liver transplant early postoperative period: an institutional standpoint
- Beatriz Amaral,
- Madalena Vicente,
- Carla Sofia Maravilha Pereira,
- Teresa Araújo,
- Ana Ribeiro, [ … ],
- Paulo Marcelino
Abstract
Review ArticlesApproach to the liver transplant early postoperative period: an institutional standpoint
Rev Bras Ter Intensiva. 2019;31(4):561-570
DOI 10.5935/0103-507X.20190076
- Beatriz Amaral,
- Madalena Vicente,
- Carla Sofia Maravilha Pereira,
- Teresa Araújo,
- Ana Ribeiro,
- Rui Pereira ,
- Rui Perdigoto,
- Paulo Marcelino
Views0ABSTRACT
The liver transplant program in our center started in 1992, and post-liver transplant patients are still admitted to the intensive care unit. For the intensive care physician, a learning curve started then, skills were acquired, and a specific practice was established. Throughout this time, several concepts changed, improving the care of these patients. The practical approach varies between liver transplant centers, according to local specificities. Hence, we wanted to present our routine practice to stimulate the debate between dedicated teams, which can allow the introduction of new ideas and potentially improve each local standard of care.
Keywords:Intensive careLiver transplantationLiver/surgeryPerioperative period/adverse effectsPostoperative periodSee moreViews0Abstract
Review ArticlesApproach to the liver transplant early postoperative period: an institutional standpoint
Rev Bras Ter Intensiva. 2019;31(4):561-570
DOI 10.5935/0103-507X.20190076
- Beatriz Amaral,
- Madalena Vicente,
- Carla Sofia Maravilha Pereira,
- Teresa Araújo,
- Ana Ribeiro,
- Rui Pereira ,
- Rui Perdigoto,
- Paulo Marcelino
Views0ABSTRACT
The liver transplant program in our center started in 1992, and post-liver transplant patients are still admitted to the intensive care unit. For the intensive care physician, a learning curve started then, skills were acquired, and a specific practice was established. Throughout this time, several concepts changed, improving the care of these patients. The practical approach varies between liver transplant centers, according to local specificities. Hence, we wanted to present our routine practice to stimulate the debate between dedicated teams, which can allow the introduction of new ideas and potentially improve each local standard of care.
Keywords:Intensive careLiver transplantationLiver/surgeryPerioperative period/adverse effectsPostoperative periodSee more -
Review Articles
Behavioral Pain Scale and Critical Care Pain Observation Tool for pain evaluation in orotracheally tubed critical patients. A systematic review of the literature
Rev Bras Ter Intensiva. 2019;31(4):571-581
Abstract
Review ArticlesBehavioral Pain Scale and Critical Care Pain Observation Tool for pain evaluation in orotracheally tubed critical patients. A systematic review of the literature
Rev Bras Ter Intensiva. 2019;31(4):571-581
DOI 10.5935/0103-507X.20190070
Views0ABSTRACT
Objective:
Descrever a adequação de duas escalas comportamentais, a Behavioral Pain Scale e a Critical Care Pain Observation Tool, para a avaliação da dor em pacientes intubados orotraquealmente, internados em unidades de terapia intensiva.
Method:
Utilizando a metodologia recomendada pelo Centro Cochrane, foi realizada revisão sistemática da literatura, na base de dados eletrônica EBSCO host (CINAHL Complete, MEDLINE®Complete, Nursing & Allied Health Collection: Comprehensive, Cochrane Central Register of Controlled Trials, Cochrane Database of Systematic Reviews, Cochrane Methodology Register, Library, Information Science & Technology Abstracts, MedicLatina). Foram realizadas duas pesquisas com os seguintes termos em inglês no campo de pesquisa: “behavioral pain scale” AND “critical care pain observation tool” AND “behavioral pain scale” OR “critical care pain observation tool“. Dois revisores independentes realizaram a avaliação crítica, a extração e a síntese dos dados.
Results:
Foram incluídos 15 estudos que evidenciaram que a Behavioral Pain Scale e a Critical Care Pain Observation Tool eram duas escalas válidas e confiáveis para a avaliação da dor em pacientes intubados orotraquealmente e internados em unidade de terapia intensiva. As escalas apresentaram propriedades psicométricas semelhantes, bem como boa confiabilidade.
Conclusion:
Ambas as escalas são adequadas para a avaliação da dor em pacientes intubados orotraquealmente, internados em unidade de terapia intensiva, contudo, apresentam limitações em populações específicas como doentes vítimas de trauma, queimados e do foro neurocirurgico. É sugerida a realização de mais estudos sobre o tema e em populações específicas.
Keywords:Behavioral Pain ScaleCritical careCritical Care Pain Observation ToolCritical illnessPainPain measurementSee moreViews0Abstract
Review ArticlesBehavioral Pain Scale and Critical Care Pain Observation Tool for pain evaluation in orotracheally tubed critical patients. A systematic review of the literature
Rev Bras Ter Intensiva. 2019;31(4):571-581
DOI 10.5935/0103-507X.20190070
Views0ABSTRACT
Objective:
Descrever a adequação de duas escalas comportamentais, a Behavioral Pain Scale e a Critical Care Pain Observation Tool, para a avaliação da dor em pacientes intubados orotraquealmente, internados em unidades de terapia intensiva.
Method:
Utilizando a metodologia recomendada pelo Centro Cochrane, foi realizada revisão sistemática da literatura, na base de dados eletrônica EBSCO host (CINAHL Complete, MEDLINE®Complete, Nursing & Allied Health Collection: Comprehensive, Cochrane Central Register of Controlled Trials, Cochrane Database of Systematic Reviews, Cochrane Methodology Register, Library, Information Science & Technology Abstracts, MedicLatina). Foram realizadas duas pesquisas com os seguintes termos em inglês no campo de pesquisa: “behavioral pain scale” AND “critical care pain observation tool” AND “behavioral pain scale” OR “critical care pain observation tool“. Dois revisores independentes realizaram a avaliação crítica, a extração e a síntese dos dados.
Results:
Foram incluídos 15 estudos que evidenciaram que a Behavioral Pain Scale e a Critical Care Pain Observation Tool eram duas escalas válidas e confiáveis para a avaliação da dor em pacientes intubados orotraquealmente e internados em unidade de terapia intensiva. As escalas apresentaram propriedades psicométricas semelhantes, bem como boa confiabilidade.
Conclusion:
Ambas as escalas são adequadas para a avaliação da dor em pacientes intubados orotraquealmente, internados em unidade de terapia intensiva, contudo, apresentam limitações em populações específicas como doentes vítimas de trauma, queimados e do foro neurocirurgico. É sugerida a realização de mais estudos sobre o tema e em populações específicas.
Keywords:Behavioral Pain ScaleCritical careCritical Care Pain Observation ToolCritical illnessPainPain measurementSee more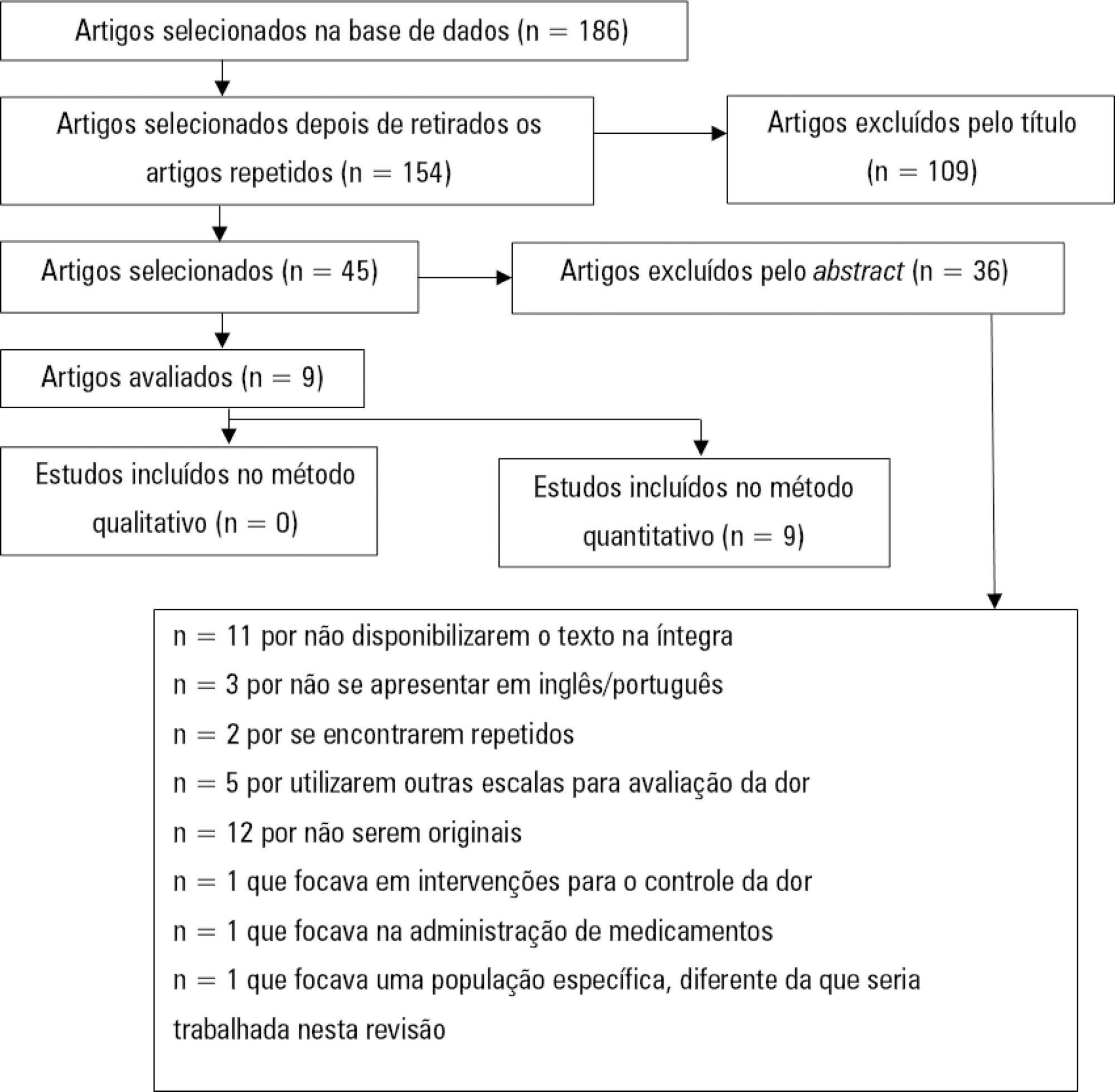
-
Case Reports
Multiple organ dysfunction caused by a foreign body in the esophagus
- Sasa Dragic ,
- Pedja Kovacevic,
- Danica Momcicevic,
- Jovana Cavka,
- Tijana Kovacevic, [ … ],
- Vlado Djajić
Abstract
Case ReportsMultiple organ dysfunction caused by a foreign body in the esophagus
Rev Bras Ter Intensiva. 2019;31(4):582-585
DOI 10.5935/0103-507X.20190075
- Sasa Dragic ,
- Pedja Kovacevic,
- Danica Momcicevic,
- Jovana Cavka,
- Tijana Kovacevic,
- Aleksandra Aleksic,
- Milka Jandric,
- Biljana Zljutro,
- Vlado Djajić
Views0See moreABSTRACT
We present the case of a 71-year-old patient who was admitted to the medical intensive care unit in a state of multiple organ dysfunction. After the fourth day of applying all needed life-saving measures (vasopressor stimulation, mechanical ventilation, continuous dialysis treatment, broad spectrum antibiotic therapy, and other supportive measures), nonspecific heteroanamnestic data revealed that the patient had been having a persistent difficulty in swallowing liquids and food for a few days prior to hospital admission. After performing additional radiological and endoscopic diagnostic procedures, a foreign body was detected; a steel wire that had a length of approximately 6cm and was bent in a half had penetrated the esophagus and was projected into the seventh neckline. We managed to evacuate the foreign body endoscopically without further complications, and we stabilized our patient using additional therapeutic measures as needed.
Views0Abstract
Case ReportsMultiple organ dysfunction caused by a foreign body in the esophagus
Rev Bras Ter Intensiva. 2019;31(4):582-585
DOI 10.5935/0103-507X.20190075
- Sasa Dragic ,
- Pedja Kovacevic,
- Danica Momcicevic,
- Jovana Cavka,
- Tijana Kovacevic,
- Aleksandra Aleksic,
- Milka Jandric,
- Biljana Zljutro,
- Vlado Djajić
Views0See moreABSTRACT
We present the case of a 71-year-old patient who was admitted to the medical intensive care unit in a state of multiple organ dysfunction. After the fourth day of applying all needed life-saving measures (vasopressor stimulation, mechanical ventilation, continuous dialysis treatment, broad spectrum antibiotic therapy, and other supportive measures), nonspecific heteroanamnestic data revealed that the patient had been having a persistent difficulty in swallowing liquids and food for a few days prior to hospital admission. After performing additional radiological and endoscopic diagnostic procedures, a foreign body was detected; a steel wire that had a length of approximately 6cm and was bent in a half had penetrated the esophagus and was projected into the seventh neckline. We managed to evacuate the foreign body endoscopically without further complications, and we stabilized our patient using additional therapeutic measures as needed.
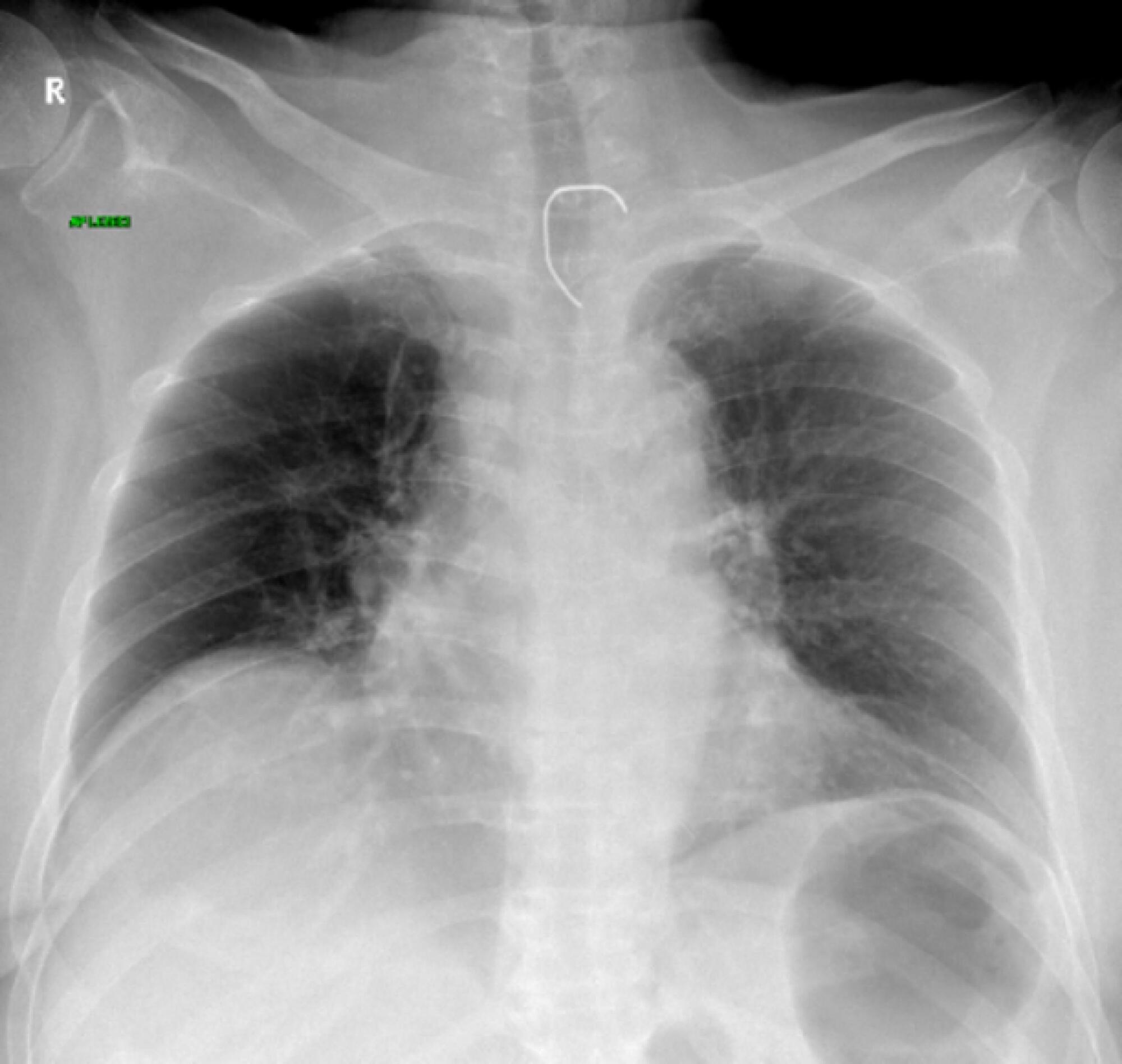
- Sasa Dragic
-
Case Reports
Diagnosis and treatment of streptococcal toxic shock syndrome in the pediatric intensive care unit: a case report
- Haroldo Teófilo de Carvalho ,
- José Roberto Fioretto,
- Cristiane Franco Ribeiro,
- Isabela Ortiz Laraia,
- Mario Ferreira Carpi
Abstract
Case ReportsDiagnosis and treatment of streptococcal toxic shock syndrome in the pediatric intensive care unit: a case report
Rev Bras Ter Intensiva. 2019;31(4):586-591
DOI 10.5935/0103-507X.20190068
- Haroldo Teófilo de Carvalho ,
- José Roberto Fioretto,
- Cristiane Franco Ribeiro,
- Isabela Ortiz Laraia,
- Mario Ferreira Carpi
Views0ABSTRACT
Among the infections caused by Streptococcus β hemolyticus from the Lancefield serogroup A, toxic shock syndrome is perhaps the most severe, and its mortality rate is high. Its clinical similarity to other forms of shock, especially septic shock, can often confuse the evaluator and interfere with the selection of the most appropriate therapy. This report aims to inform readers of the need to add this syndrome as a differential diagnosis in cases of shock, especially those with no well-defined clinical manifestations. For this purpose, we present the case of an infant with common flu-like symptoms who progressed rapidly with a rash, a reduced level of consciousness and clinical and laboratory signs of shock that required intensive support. In addition to cultures indicating the etiological agent, the appearance of exanthema and necrotizing fasciitis led to the diagnosis. However, less than 50% of cases present classic clinical signs of this entity. Penicillins combined with aminoglycosides are still the therapy of choice and are supported by a high level of evidence. Despite the severity of this patient’s presentation, the progression was satisfactory.
Keywords:Aminoglycosides/therapeutic useCombined modality therapyExanthemaFasciitis, necrotizingIntensive care units, pediatricPenicillins/therapeutic useShock, septic/diagnoisShock, septic/drug therapySee moreViews0Abstract
Case ReportsDiagnosis and treatment of streptococcal toxic shock syndrome in the pediatric intensive care unit: a case report
Rev Bras Ter Intensiva. 2019;31(4):586-591
DOI 10.5935/0103-507X.20190068
- Haroldo Teófilo de Carvalho ,
- José Roberto Fioretto,
- Cristiane Franco Ribeiro,
- Isabela Ortiz Laraia,
- Mario Ferreira Carpi
Views0ABSTRACT
Among the infections caused by Streptococcus β hemolyticus from the Lancefield serogroup A, toxic shock syndrome is perhaps the most severe, and its mortality rate is high. Its clinical similarity to other forms of shock, especially septic shock, can often confuse the evaluator and interfere with the selection of the most appropriate therapy. This report aims to inform readers of the need to add this syndrome as a differential diagnosis in cases of shock, especially those with no well-defined clinical manifestations. For this purpose, we present the case of an infant with common flu-like symptoms who progressed rapidly with a rash, a reduced level of consciousness and clinical and laboratory signs of shock that required intensive support. In addition to cultures indicating the etiological agent, the appearance of exanthema and necrotizing fasciitis led to the diagnosis. However, less than 50% of cases present classic clinical signs of this entity. Penicillins combined with aminoglycosides are still the therapy of choice and are supported by a high level of evidence. Despite the severity of this patient’s presentation, the progression was satisfactory.
Keywords:Aminoglycosides/therapeutic useCombined modality therapyExanthemaFasciitis, necrotizingIntensive care units, pediatricPenicillins/therapeutic useShock, septic/diagnoisShock, septic/drug therapySee more
- Haroldo Teófilo de Carvalho
-
Letters to the Editor
The sex gap among visitors during flexible intensive care unit visiting hours
- Silvana Pinto Hartmann,
- Larissa Jorge F. de Faria,
- Cassiano Teixeira ,
- Cristiane Souza dos Santos,
- Tiago Claro Maurer, [ … ],
- Regis Goulart Rosa
Abstract
Letters to the EditorThe sex gap among visitors during flexible intensive care unit visiting hours
Rev Bras Ter Intensiva. 2019;31(4):592-593
DOI 10.5935/0103-507X.20190089
- Silvana Pinto Hartmann,
- Larissa Jorge F. de Faria,
- Cassiano Teixeira ,
- Cristiane Souza dos Santos,
- Tiago Claro Maurer,
- Daiana Barbosa da Silva,
- Regis Goulart Rosa
Views0Dear Editor, Flexible intensive care unit (ICU) visiting hours are increasingly recognized as a means of enhancing patient- and family-centered care.(,) In addition to being safe and associated with better patient and family outcomes,(,) flexible visiting hours are an important approach to acknowledging and showing respect for the patient-family relationship during the course of critical […]See moreViews0Abstract
Letters to the EditorThe sex gap among visitors during flexible intensive care unit visiting hours
Rev Bras Ter Intensiva. 2019;31(4):592-593
DOI 10.5935/0103-507X.20190089
- Silvana Pinto Hartmann,
- Larissa Jorge F. de Faria,
- Cassiano Teixeira ,
- Cristiane Souza dos Santos,
- Tiago Claro Maurer,
- Daiana Barbosa da Silva,
- Regis Goulart Rosa
Views0Dear Editor, Flexible intensive care unit (ICU) visiting hours are increasingly recognized as a means of enhancing patient- and family-centered care.(,) In addition to being safe and associated with better patient and family outcomes,(,) flexible visiting hours are an important approach to acknowledging and showing respect for the patient-family relationship during the course of critical […]See more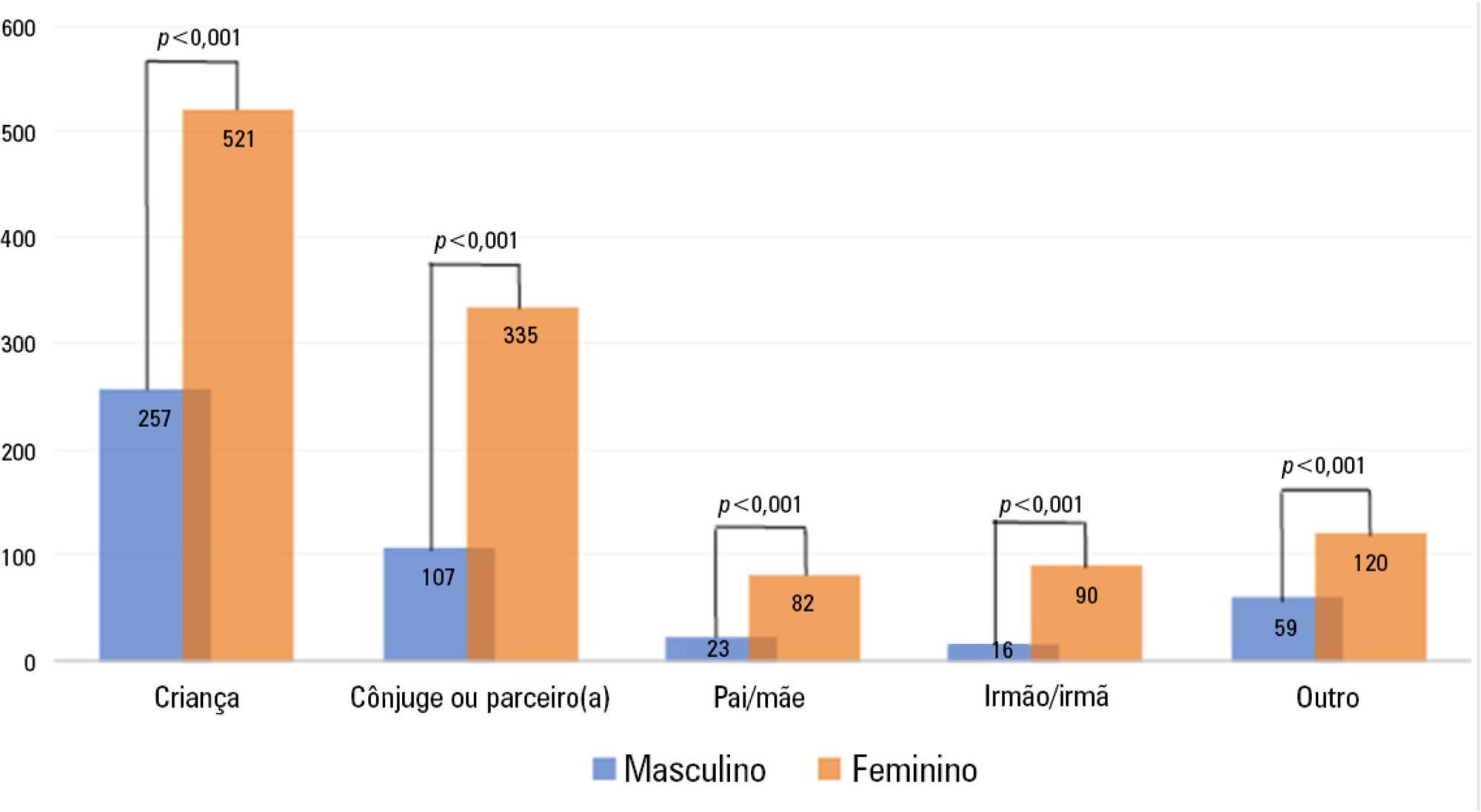
-
Letters to the Editor
To: Comparison of bronchial hygiene techniques in mechanically ventilated patients: a randomized clinical trial
Rev Bras Ter Intensiva. 2019;31(4):594-595
Abstract
Letters to the EditorTo: Comparison of bronchial hygiene techniques in mechanically ventilated patients: a randomized clinical trial
Rev Bras Ter Intensiva. 2019;31(4):594-595
DOI 10.5935/0103-507X.20190080
Views0To the Editor In this issue of Revista Brasileira de Terapia Intensiva , Naue et al.() present an interesting study. We would like to congratulate the authors for their relevant contribution to the scientific literature on the subject, but we need clarification on the study design and reporting.[…]See moreViews0Abstract
Letters to the EditorTo: Comparison of bronchial hygiene techniques in mechanically ventilated patients: a randomized clinical trial
Rev Bras Ter Intensiva. 2019;31(4):594-595
DOI 10.5935/0103-507X.20190080
Views0To the Editor In this issue of Revista Brasileira de Terapia Intensiva , Naue et al.() present an interesting study. We would like to congratulate the authors for their relevant contribution to the scientific literature on the subject, but we need clarification on the study design and reporting.[…]See more -
Letters to the Editor
To: The Perme scale score as a predictor of functional status and complications after discharge from the intensive care unit in patients undergoing liver transplantation
- Márcio Ferreira Camillis,
- Lucas Galant,
- Leonardo Miguel Correa Garcia,
- Ricardo Wickert,
- Priscila Cidade, [ … ],
- Cassiano Teixeira
Abstract
Letters to the EditorTo: The Perme scale score as a predictor of functional status and complications after discharge from the intensive care unit in patients undergoing liver transplantation
Rev Bras Ter Intensiva. 2019;31(4):598-599
DOI 10.5935/0103-507X.20190082
- Márcio Ferreira Camillis,
- Lucas Galant,
- Leonardo Miguel Correa Garcia,
- Ricardo Wickert,
- Priscila Cidade,
- Cassiano Teixeira
Views0To the Editor I would like to congratulate the authors responsible for the article entitled “The Perme scale score as a predictor of functional status and complications after discharge from the intensive care unit in patients undergoing liver transplantation”, the topic of which is extremely relevant to the academic community.()[…]See moreViews0Abstract
Letters to the EditorTo: The Perme scale score as a predictor of functional status and complications after discharge from the intensive care unit in patients undergoing liver transplantation
Rev Bras Ter Intensiva. 2019;31(4):598-599
DOI 10.5935/0103-507X.20190082
- Márcio Ferreira Camillis,
- Lucas Galant,
- Leonardo Miguel Correa Garcia,
- Ricardo Wickert,
- Priscila Cidade,
- Cassiano Teixeira
Views0To the Editor I would like to congratulate the authors responsible for the article entitled “The Perme scale score as a predictor of functional status and complications after discharge from the intensive care unit in patients undergoing liver transplantation”, the topic of which is extremely relevant to the academic community.()[…]See more -
Author’s Response
Reply to: The Perme scale score as a predictor of functional status and complications after discharge from the intensive care unit in patients undergoing liver transplantation
- Camila Santos Pereira,
- Alexandra Torres de Carvalho,
- Adriane Dal Bosco,
- Luiz Alberto Forgiarini Júnior
Abstract
Author’s ResponseReply to: The Perme scale score as a predictor of functional status and complications after discharge from the intensive care unit in patients undergoing liver transplantation
Rev Bras Ter Intensiva. 2019;31(4):600-601
DOI 10.5935/0103-507X.20190083
- Camila Santos Pereira,
- Alexandra Torres de Carvalho,
- Adriane Dal Bosco,
- Luiz Alberto Forgiarini Júnior
Views0To the Editor First, the authors are thankful for the comments and for the opportunity to clarify points of our study published in Revista Brasileira de Terapia Intensiva.() Our research line has involved investigating some functional assessment tools in different populations to identify functional behavior. In the study referred to above, we evaluated the use […]See moreViews0Abstract
Author’s ResponseReply to: The Perme scale score as a predictor of functional status and complications after discharge from the intensive care unit in patients undergoing liver transplantation
Rev Bras Ter Intensiva. 2019;31(4):600-601
DOI 10.5935/0103-507X.20190083
- Camila Santos Pereira,
- Alexandra Torres de Carvalho,
- Adriane Dal Bosco,
- Luiz Alberto Forgiarini Júnior
Views0To the Editor First, the authors are thankful for the comments and for the opportunity to clarify points of our study published in Revista Brasileira de Terapia Intensiva.() Our research line has involved investigating some functional assessment tools in different populations to identify functional behavior. In the study referred to above, we evaluated the use […]See more
Volume Articles - Critical Care Science (CCS)
