-
Editorial
COVID-19 pandemic
Rev Bras Ter Intensiva. 2020;32(1):1-1
Abstract
EditorialCOVID-19 pandemic
Rev Bras Ter Intensiva. 2020;32(1):1-1
DOI 10.5935/0103-507X.20200001
Views0Once again, a disease advances and worries everyone. Unlike other epidemics and thanks to advances in science, this flu was considered distinct, its etiological agent isolated and identified, and new detection tests were developed in record time. So far there are no effective vaccines or active antiviral drugs for SARS-2, the coronavirus responsible for the […]See moreViews0

Abstract
EditorialCOVID-19 pandemic
Rev Bras Ter Intensiva. 2020;32(1):1-1
DOI 10.5935/0103-507X.20200001
Views0Once again, a disease advances and worries everyone. Unlike other epidemics and thanks to advances in science, this flu was considered distinct, its etiological agent isolated and identified, and new detection tests were developed in record time. So far there are no effective vaccines or active antiviral drugs for SARS-2, the coronavirus responsible for the […]See more -
Special Article
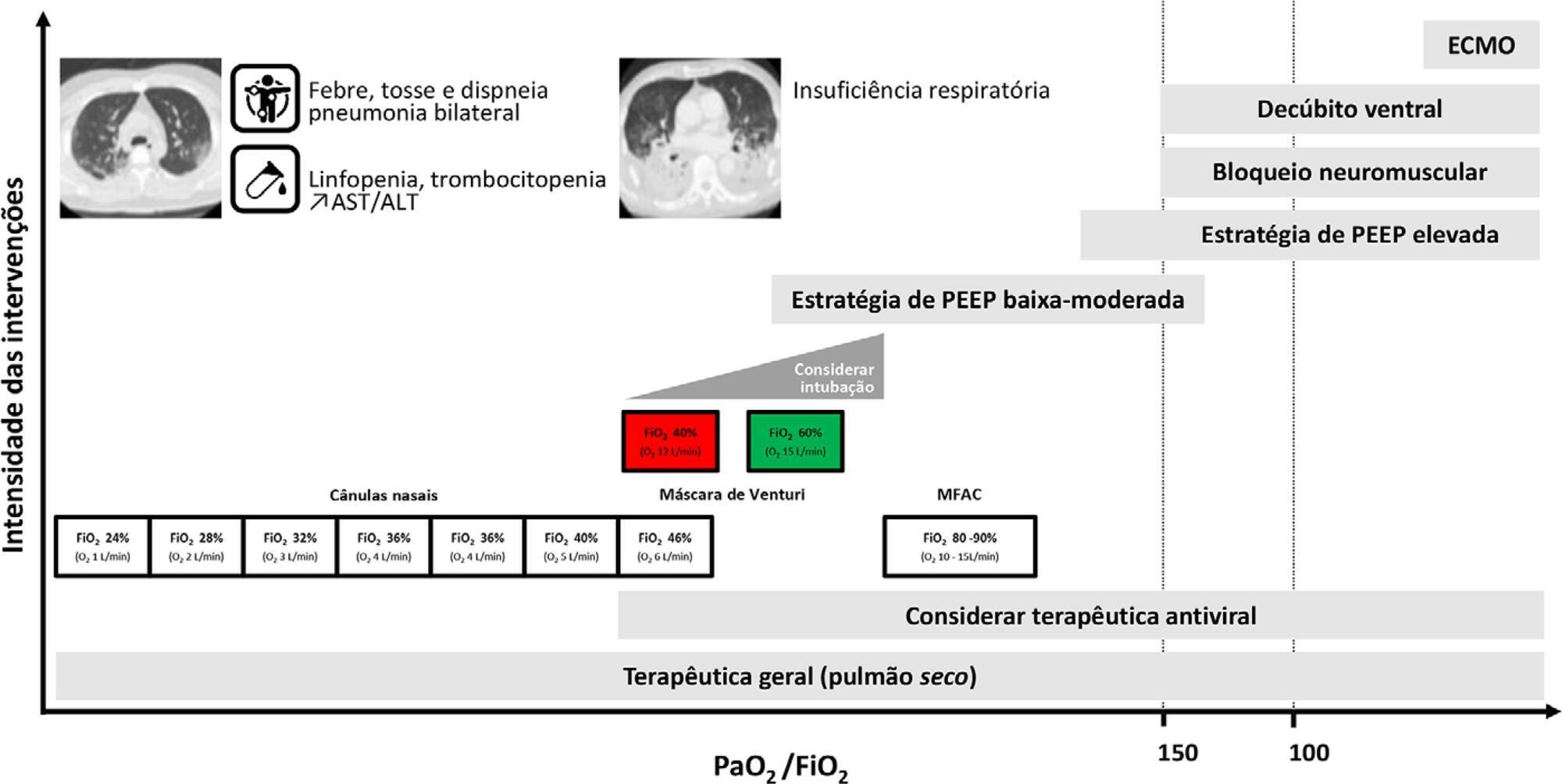
Recommendations from the Sociedade Portuguesa de Cuidados Intensivos and Infection & Sepsis Group for intensive care approach to COVID-19
Rev Bras Ter Intensiva. 2020;32(1):2-10
Abstract
Special ArticleRecommendations from the Sociedade Portuguesa de Cuidados Intensivos and Infection & Sepsis Group for intensive care approach to COVID-19
Rev Bras Ter Intensiva. 2020;32(1):2-10
DOI 10.5935/0103-507X.20200002
Views0See moreABSTRACT
Current COVID-19 epidemics was declared on December 31, 2019 at the Wuhan city seafood market, rapidly spreading throughout China, and later reaching several countries (mainly South Korea, Japan, Italy and Iran) and, since March 1, reaching Portugal. Most of the infected patients present with mild symptoms, not requiring hospitalization. Among those admitted to the hospital, 6% to 10% require admission to the intensive care unit. These recommendations are aimed to support the organization of intensive care services to respond COVID-19, providing optimized care to the patient and protection for healthcare professionals.
Views0Abstract
Special ArticleRecommendations from the Sociedade Portuguesa de Cuidados Intensivos and Infection & Sepsis Group for intensive care approach to COVID-19
Rev Bras Ter Intensiva. 2020;32(1):2-10
DOI 10.5935/0103-507X.20200002
Views0See moreABSTRACT
Current COVID-19 epidemics was declared on December 31, 2019 at the Wuhan city seafood market, rapidly spreading throughout China, and later reaching several countries (mainly South Korea, Japan, Italy and Iran) and, since March 1, reaching Portugal. Most of the infected patients present with mild symptoms, not requiring hospitalization. Among those admitted to the hospital, 6% to 10% require admission to the intensive care unit. These recommendations are aimed to support the organization of intensive care services to respond COVID-19, providing optimized care to the patient and protection for healthcare professionals.
-
Commentary
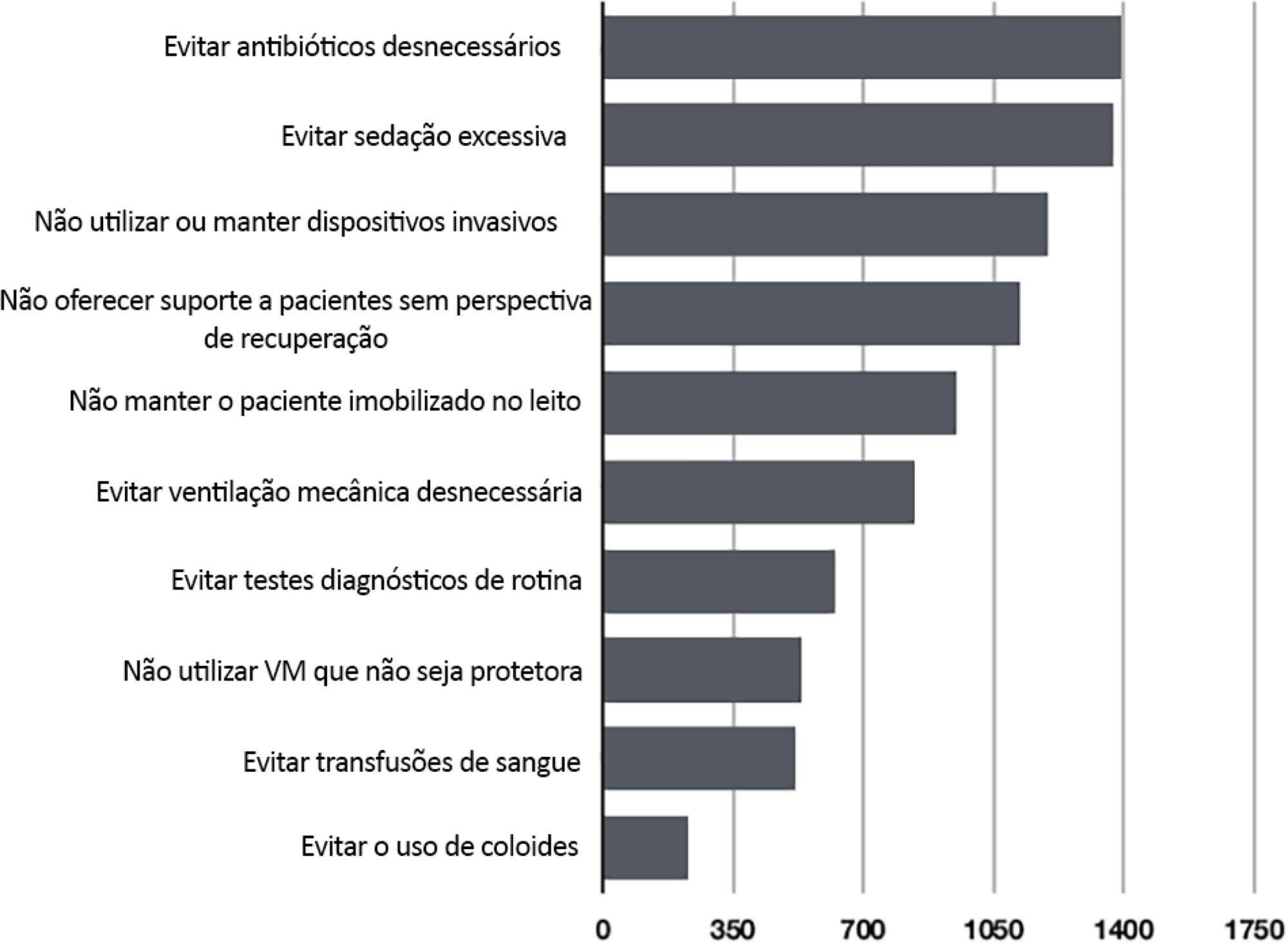
Choosing Wisely in intensive care medicine
Rev Bras Ter Intensiva. 2020;32(1):11-13
Abstract
Views1Abstract
-
Commentary
What every intensivist needs to know about subsyndromal delirium in the intensive care unit
Rev Bras Ter Intensiva. 2020;32(1):14-16
Abstract
CommentaryWhat every intensivist needs to know about subsyndromal delirium in the intensive care unit
Rev Bras Ter Intensiva. 2020;32(1):14-16
DOI 10.5935/0103-507X.20200004
Views0IntroductionSeveral studies have described the negative outcomes associated with delirium in the short or long term,(,) but not every form of delirium has the same prognosis. The duration and severity of delirium have been found to be the main factors associated with worse outcomes.(,) In fact, a very short delirium duration seems to have little […]See moreViews0Abstract
CommentaryWhat every intensivist needs to know about subsyndromal delirium in the intensive care unit
Rev Bras Ter Intensiva. 2020;32(1):14-16
DOI 10.5935/0103-507X.20200004
Views0IntroductionSeveral studies have described the negative outcomes associated with delirium in the short or long term,(,) but not every form of delirium has the same prognosis. The duration and severity of delirium have been found to be the main factors associated with worse outcomes.(,) In fact, a very short delirium duration seems to have little […]See more -
Original Article
Epidemiology and outcome of high-surgical-risk patients admitted to an intensive care unit in Brazil
- João Manoel Silva Júnior
 ,
, - Renato Carneiro de Freitas Chaves ,
- Thiago Domingos Corrêa ,
- Murillo Santucci Cesar de Assunção ,
- Henrique Tadashi Katayama, [ … ],
- Suzana Margareth Ajeje Lobo
Abstract
Original ArticleEpidemiology and outcome of high-surgical-risk patients admitted to an intensive care unit in Brazil
Rev Bras Ter Intensiva. 2020;32(1):17-27
DOI 10.5935/0103-507X.20200005
- João Manoel Silva Júnior ,
- Renato Carneiro de Freitas Chaves ,
- Thiago Domingos Corrêa ,
- Murillo Santucci Cesar de Assunção ,
- Henrique Tadashi Katayama,
- Fabio Eduardo Bosso,
- Cristina Prata Amendola,
- Ary Serpa Neto ,
- Luiz Marcelo Sá Malbouisson,
- Neymar Elias de Oliveira,
- Viviane Cordeiro Veiga ,
- Salomón Soriano Ordinola Rojas,
- Natalia Fioravante Postalli,
- Thais Kawagoe Alvarisa,
- Bruno Melo Nobrega de Lucena,
- Raphael Augusto Gomes de Oliveira,
- Luciana Coelho Sanches,
- Ulysses Vasconcellos de Andrade e Silva,
- Antonio Paulo Nassar Junior ,
- Álvaro Réa-Neto,
- Alexandre Amaral,
- José Mário Teles,
- Flávio Geraldo Rezende de Freitas,
- Antônio Tonete Bafi,
- Eduardo Souza Pacheco,
- Fernando José Ramos,
- José Mauro Vieira Júnior,
- Maria Augusta Santos Rahe Pereira,
- Fábio Sartori Schwerz,
- Giovanna Padoa de Menezes,
- Danielle Dourado Magalhães,
- Cristine Pilati Pileggi Castro,
- Sabrina Frighetto Henrich,
- Diogo Oliveira Toledo,
- Bruna Fernanda Camargo Silva Parra,
- Fernando Suparregui Dias ,
- Luiza Zerman,
- Fernanda Formolo,
- Marciano de Sousa Nobrega,
- Claudio Piras,
- Stéphanie de Barros Piras,
- Rodrigo Conti,
- Paulo Lisboa Bittencourt,
- Ricardo Azevedo Cruz D’Oliveira,
- André Ricardo de Oliveira Estrela,
- Mirella Cristine de Oliveira,
- Fernanda Baeumle Reese,
- Jarbas da Silva Motta Júnior,
- Bruna Martins Dzivielevski da Câmara,
- Paula Geraldes David-João,
- Luana Alves Tannous,
- Viviane Bernardes de Oliveira Chaiben,
- Lorena Macedo Araújo Miranda,
- José Arthur dos Santos Brasil,
- Rafael Alexandre de Oliveira Deucher,
- Marcos Henrique Borges Ferreira,
- Denner Luiz Vilela,
- Guilherme Cincinato de Almeida,
- Wagner Luis Nedel ,
- Matheus Golenia dos Passos,
- Luiz Gustavo Marin,
- Wilson de Oliveira Filho,
- Raoni Machado Coutinho,
- Michele Cristina Lima de Oliveira,
- Gilberto Friedman,
- André Meregalli,
- Jorge Amilton Höher,
- Afonso José Celente Soares,
- Suzana Margareth Ajeje Lobo
Views1ABSTRACT
Objective:
To define the epidemiological profile and the main determinants of morbidity and mortality in noncardiac high surgical risk patients in Brazil.
Methods:
This was a prospective, observational and multicenter study. All noncardiac surgical patients admitted to intensive care units, i.e., those considered high risk, within a 1-month period were evaluated and monitored daily for a maximum of 7 days in the intensive care unit to determine complications. The 28-day postoperative, intensive care unit and hospital mortality rates were evaluated.
Results:
Twenty-nine intensive care units participated in the study. Surgeries were performed in 25,500 patients, of whom 904 (3.5%) were high-risk (95% confidence interval – 95%CI 3.3% – 3.8%) and were included in the study. Of the participating patients, 48.3% were from private intensive care units, and 51.7% were from public intensive care units. The length of stay in the intensive care unit was 2.0 (1.0 – 4.0) days, and the length of hospital stay was 9.5 (5.4 – 18.6) days. The complication rate was 29.9% (95%CI 26.4 – 33.7), and the 28-day postoperative mortality rate was 9.6% (95%CI 7.4 – 12.1). The independent risk factors for complications were the Simplified Acute Physiology Score 3 (SAPS 3; odds ratio – OR = 1.02; 95%CI 1.01 – 1.03) and Sequential Organ Failure Assessment Score (SOFA) on admission to the intensive care unit (OR = 1.17; 95%CI 1.09 – 1.25), surgical time (OR = 1.001, 95%CI 1.000 – 1.002) and emergency surgeries (OR = 1.93, 95%CI, 1.10 – 3.38). In addition, there were associations with 28-day mortality (OR = 1.032; 95%CI 1.011 – 1.052), SAPS 3 (OR = 1.041; 95%CI 1.107 – 1.279), SOFA (OR = 1.175, 95%CI 1.069 – 1.292) and emergency surgeries (OR = 2.509; 95%CI 1.040 – 6.051).
Conclusion:
Higher prognostic scores, elderly patients, longer surgical times and emergency surgeries were strongly associated with higher 28-day mortality and more complications during the intensive care unit stay.
Keywords:BrazilIntensive care unitspostoperative carePostoperative complications/mortalitySurgical procedures, operative/epidemiologySurgical procedures, operative/mortalitySee moreViews1Abstract
Original ArticleEpidemiology and outcome of high-surgical-risk patients admitted to an intensive care unit in Brazil
Rev Bras Ter Intensiva. 2020;32(1):17-27
DOI 10.5935/0103-507X.20200005
- João Manoel Silva Júnior ,
- Renato Carneiro de Freitas Chaves ,
- Thiago Domingos Corrêa ,
- Murillo Santucci Cesar de Assunção ,
- Henrique Tadashi Katayama,
- Fabio Eduardo Bosso,
- Cristina Prata Amendola,
- Ary Serpa Neto ,
- Luiz Marcelo Sá Malbouisson,
- Neymar Elias de Oliveira,
- Viviane Cordeiro Veiga ,
- Salomón Soriano Ordinola Rojas,
- Natalia Fioravante Postalli,
- Thais Kawagoe Alvarisa,
- Bruno Melo Nobrega de Lucena,
- Raphael Augusto Gomes de Oliveira,
- Luciana Coelho Sanches,
- Ulysses Vasconcellos de Andrade e Silva,
- Antonio Paulo Nassar Junior ,
- Álvaro Réa-Neto,
- Alexandre Amaral,
- José Mário Teles,
- Flávio Geraldo Rezende de Freitas,
- Antônio Tonete Bafi,
- Eduardo Souza Pacheco,
- Fernando José Ramos,
- José Mauro Vieira Júnior,
- Maria Augusta Santos Rahe Pereira,
- Fábio Sartori Schwerz,
- Giovanna Padoa de Menezes,
- Danielle Dourado Magalhães,
- Cristine Pilati Pileggi Castro,
- Sabrina Frighetto Henrich,
- Diogo Oliveira Toledo,
- Bruna Fernanda Camargo Silva Parra,
- Fernando Suparregui Dias ,
- Luiza Zerman,
- Fernanda Formolo,
- Marciano de Sousa Nobrega,
- Claudio Piras,
- Stéphanie de Barros Piras,
- Rodrigo Conti,
- Paulo Lisboa Bittencourt,
- Ricardo Azevedo Cruz D’Oliveira,
- André Ricardo de Oliveira Estrela,
- Mirella Cristine de Oliveira,
- Fernanda Baeumle Reese,
- Jarbas da Silva Motta Júnior,
- Bruna Martins Dzivielevski da Câmara,
- Paula Geraldes David-João,
- Luana Alves Tannous,
- Viviane Bernardes de Oliveira Chaiben,
- Lorena Macedo Araújo Miranda,
- José Arthur dos Santos Brasil,
- Rafael Alexandre de Oliveira Deucher,
- Marcos Henrique Borges Ferreira,
- Denner Luiz Vilela,
- Guilherme Cincinato de Almeida,
- Wagner Luis Nedel ,
- Matheus Golenia dos Passos,
- Luiz Gustavo Marin,
- Wilson de Oliveira Filho,
- Raoni Machado Coutinho,
- Michele Cristina Lima de Oliveira,
- Gilberto Friedman,
- André Meregalli,
- Jorge Amilton Höher,
- Afonso José Celente Soares,
- Suzana Margareth Ajeje Lobo
Views1ABSTRACT
Objective:
To define the epidemiological profile and the main determinants of morbidity and mortality in noncardiac high surgical risk patients in Brazil.
Methods:
This was a prospective, observational and multicenter study. All noncardiac surgical patients admitted to intensive care units, i.e., those considered high risk, within a 1-month period were evaluated and monitored daily for a maximum of 7 days in the intensive care unit to determine complications. The 28-day postoperative, intensive care unit and hospital mortality rates were evaluated.
Results:
Twenty-nine intensive care units participated in the study. Surgeries were performed in 25,500 patients, of whom 904 (3.5%) were high-risk (95% confidence interval – 95%CI 3.3% – 3.8%) and were included in the study. Of the participating patients, 48.3% were from private intensive care units, and 51.7% were from public intensive care units. The length of stay in the intensive care unit was 2.0 (1.0 – 4.0) days, and the length of hospital stay was 9.5 (5.4 – 18.6) days. The complication rate was 29.9% (95%CI 26.4 – 33.7), and the 28-day postoperative mortality rate was 9.6% (95%CI 7.4 – 12.1). The independent risk factors for complications were the Simplified Acute Physiology Score 3 (SAPS 3; odds ratio – OR = 1.02; 95%CI 1.01 – 1.03) and Sequential Organ Failure Assessment Score (SOFA) on admission to the intensive care unit (OR = 1.17; 95%CI 1.09 – 1.25), surgical time (OR = 1.001, 95%CI 1.000 – 1.002) and emergency surgeries (OR = 1.93, 95%CI, 1.10 – 3.38). In addition, there were associations with 28-day mortality (OR = 1.032; 95%CI 1.011 – 1.052), SAPS 3 (OR = 1.041; 95%CI 1.107 – 1.279), SOFA (OR = 1.175, 95%CI 1.069 – 1.292) and emergency surgeries (OR = 2.509; 95%CI 1.040 – 6.051).
Conclusion:
Higher prognostic scores, elderly patients, longer surgical times and emergency surgeries were strongly associated with higher 28-day mortality and more complications during the intensive care unit stay.
Keywords:BrazilIntensive care unitspostoperative carePostoperative complications/mortalitySurgical procedures, operative/epidemiologySurgical procedures, operative/mortalitySee more
- João Manoel Silva Júnior
-
Original Article
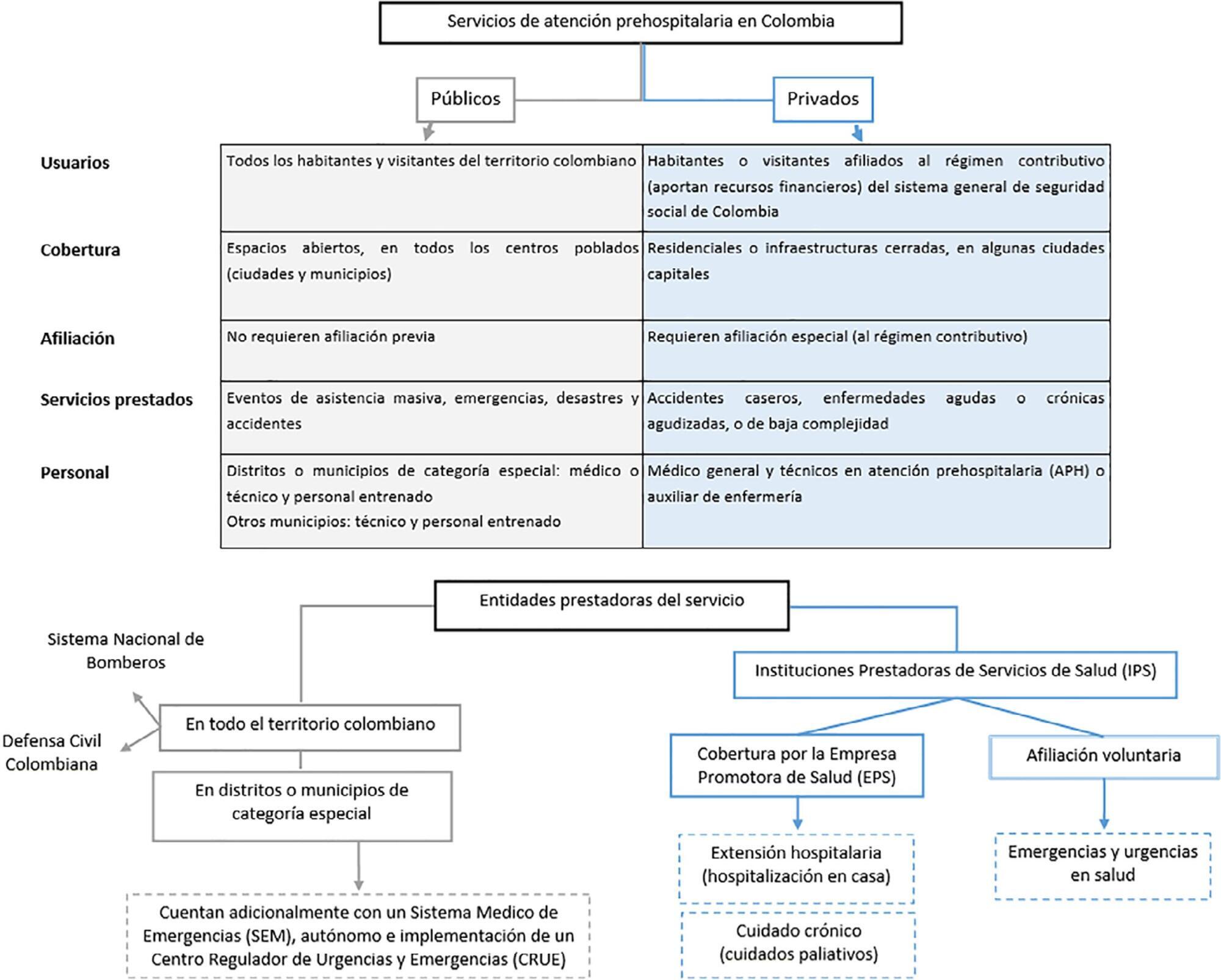
Epidemiology of septic shock in prehospital medical services in five Colombian cities
- Diana Carolina López-Medina ,
- Marcela Henao-Perez,
- Jaime Arenas-Andrade,
- Emel David Hinestroza-Marín,
- Fabián Alberto Jaimes-Barragán, [ … ],
- Oscar Iván Quirós-Gómez
Abstract
Original ArticleEpidemiology of septic shock in prehospital medical services in five Colombian cities
Rev Bras Ter Intensiva. 2020;32(1):28-36
DOI 10.5935/0103-507X.20200006
- Diana Carolina López-Medina ,
- Marcela Henao-Perez,
- Jaime Arenas-Andrade,
- Emel David Hinestroza-Marín,
- Fabián Alberto Jaimes-Barragán,
- Oscar Iván Quirós-Gómez
Views0See moreABSTRACT
Objective:
To explore the association between demographic and clinical factors and the presentation of septic shock in patients treated by prehospital emergency services in five Colombian cities between 2015 and 2016.
Methods:
This was a cross-sectional study with retrospective data collection. Clinical and demographic data were collected from the medical records of patients diagnosed with sepsis who received prehospital care in five Colombian cities in 2015 and 2016. The diagnosis of septic shock was checked in 20% of the cases, generating two analyzed scenarios: observed and verified. Data were analyzed using the chi-square test, Student’s t test and an adjusted logistic regression model. Covariates with p < 0.05 were considered significant.
Results:
There was a higher frequency of septic shock in women (62.6%) and in individuals older than 80 years (64.5%), but these were not differentiating factors for septic shock. The most common source of infection was the urinary tract. In the observed scenario, age over 60 (prevalence ratio (PR): 3.22; 95% confidence interval (CI): 1.45 – 35.01) and history of cancer (PR: 1.20; 95%CI: 1.2 – 12.87) were the characteristics associated with septic shock, whereas in the verified scenario, chronic obstructive pulmonary disease (PR: 1.99; 95%CI: 1.26 – 7.14), history of cancer (PR: 1.15; 95%CI: 1.11 – 6.62) and presence of hypovolemia (PR: 1.41; 95%CI: 1.02 – 5.50) were observed.
Conclusion:
The most important risk factors for septic shock in prehospital care patients in five Colombian cities were oncological and pulmonary diseases and hypovolemia.
Views0Abstract
Original ArticleEpidemiology of septic shock in prehospital medical services in five Colombian cities
Rev Bras Ter Intensiva. 2020;32(1):28-36
DOI 10.5935/0103-507X.20200006
- Diana Carolina López-Medina ,
- Marcela Henao-Perez,
- Jaime Arenas-Andrade,
- Emel David Hinestroza-Marín,
- Fabián Alberto Jaimes-Barragán,
- Oscar Iván Quirós-Gómez
Views0See moreABSTRACT
Objective:
To explore the association between demographic and clinical factors and the presentation of septic shock in patients treated by prehospital emergency services in five Colombian cities between 2015 and 2016.
Methods:
This was a cross-sectional study with retrospective data collection. Clinical and demographic data were collected from the medical records of patients diagnosed with sepsis who received prehospital care in five Colombian cities in 2015 and 2016. The diagnosis of septic shock was checked in 20% of the cases, generating two analyzed scenarios: observed and verified. Data were analyzed using the chi-square test, Student’s t test and an adjusted logistic regression model. Covariates with p < 0.05 were considered significant.
Results:
There was a higher frequency of septic shock in women (62.6%) and in individuals older than 80 years (64.5%), but these were not differentiating factors for septic shock. The most common source of infection was the urinary tract. In the observed scenario, age over 60 (prevalence ratio (PR): 3.22; 95% confidence interval (CI): 1.45 – 35.01) and history of cancer (PR: 1.20; 95%CI: 1.2 – 12.87) were the characteristics associated with septic shock, whereas in the verified scenario, chronic obstructive pulmonary disease (PR: 1.99; 95%CI: 1.26 – 7.14), history of cancer (PR: 1.15; 95%CI: 1.11 – 6.62) and presence of hypovolemia (PR: 1.41; 95%CI: 1.02 – 5.50) were observed.
Conclusion:
The most important risk factors for septic shock in prehospital care patients in five Colombian cities were oncological and pulmonary diseases and hypovolemia.
- Diana Carolina López-Medina
-
Original Article
Adherence to a stress ulcer prophylaxis protocol by critically ill patients: a prospective cohort study
- Yuri de Albuquerque Pessoa dos Santos ,
- Mauricio Staib Younes-Ibrahim,
- Lucas Lonardoni Crozatti,
- Dante Raglione ,
- Luis Carlos Maia Cardozo Junior, [ … ],
- Pedro Vitale Mendes
Abstract
Original ArticleAdherence to a stress ulcer prophylaxis protocol by critically ill patients: a prospective cohort study
Rev Bras Ter Intensiva. 2020;32(1):37-42
DOI 10.5935/0103-507X.20200007
- Yuri de Albuquerque Pessoa dos Santos ,
- Mauricio Staib Younes-Ibrahim,
- Lucas Lonardoni Crozatti,
- Dante Raglione ,
- Luis Carlos Maia Cardozo Junior,
- Bruno Adler Maccagnan Pinheiro Besen ,
- Leandro Utino Taniguchi ,
- Marcelo Park,
- Pedro Vitale Mendes
Views0ABSTRACT
Objective:
To evaluate adherence to the stress ulcer prophylaxis protocol in critically ill patients at a tertiary university hospital.
Methods:
In this prospective cohort study, we included all adult patients admitted to the medical and surgical intensive care units of an academic tertiary hospital. Our sole exclusion criterion was upper gastrointestinal bleeding at intensive care unit admission. We collected baseline variables and stress ulcer prophylaxis indications according to the institutional protocol and use of prophylaxis. Our primary outcome was adherence to the stress ulcer prophylaxis protocol. Secondary outcomes were appropriate use of stress ulcer prophylaxis, upper gastrointestinal bleeding incidence and factors associated with appropriate use of stress ulcer prophylaxis.
Results:
Two hundred thirty-four patients were enrolled from July 2nd through July 31st, 2018. Patients were 52 ± 20 years old, 125 (53%) were surgical patients, and the mean SAPS 3 was 52 ± 20. In the longitudinal follow-up, 1499 patient-days were studied; 1069 patient-days had stress ulcer prophylaxis indications, and 777 patient-days contained prophylaxis use (73% stress ulcer prophylaxis protocol adherence). Of the 430 patient-days without stress ulcer prophylaxis indications, 242 involved prophylaxis (56% inappropriate stress ulcer prophylaxis use). The overall appropriate use of stress ulcer prophylaxis was 64%. Factors associated with proper stress ulcer prophylaxis prescription were mechanical ventilation OR 2.13 (95%CI 1.64 – 2.75) and coagulopathy OR 2.77 (95%CI 1.66 – 4.60). The upper gastrointestinal bleeding incidence was 12.8%.
Conclusion:
Adherence to the stress ulcer prophylaxis protocol was low and inappropriate use of stress ulcer prophylaxis was frequent in this cohort of critically ill patients.
Keywords:Anti-ulcer agentsCritical careCritical illnessGastrointestinal hemorrhagePeptic ulcerTherapeutic adherence complianceSee moreViews0Abstract
Original ArticleAdherence to a stress ulcer prophylaxis protocol by critically ill patients: a prospective cohort study
Rev Bras Ter Intensiva. 2020;32(1):37-42
DOI 10.5935/0103-507X.20200007
- Yuri de Albuquerque Pessoa dos Santos ,
- Mauricio Staib Younes-Ibrahim,
- Lucas Lonardoni Crozatti,
- Dante Raglione ,
- Luis Carlos Maia Cardozo Junior,
- Bruno Adler Maccagnan Pinheiro Besen ,
- Leandro Utino Taniguchi ,
- Marcelo Park,
- Pedro Vitale Mendes
Views0ABSTRACT
Objective:
To evaluate adherence to the stress ulcer prophylaxis protocol in critically ill patients at a tertiary university hospital.
Methods:
In this prospective cohort study, we included all adult patients admitted to the medical and surgical intensive care units of an academic tertiary hospital. Our sole exclusion criterion was upper gastrointestinal bleeding at intensive care unit admission. We collected baseline variables and stress ulcer prophylaxis indications according to the institutional protocol and use of prophylaxis. Our primary outcome was adherence to the stress ulcer prophylaxis protocol. Secondary outcomes were appropriate use of stress ulcer prophylaxis, upper gastrointestinal bleeding incidence and factors associated with appropriate use of stress ulcer prophylaxis.
Results:
Two hundred thirty-four patients were enrolled from July 2nd through July 31st, 2018. Patients were 52 ± 20 years old, 125 (53%) were surgical patients, and the mean SAPS 3 was 52 ± 20. In the longitudinal follow-up, 1499 patient-days were studied; 1069 patient-days had stress ulcer prophylaxis indications, and 777 patient-days contained prophylaxis use (73% stress ulcer prophylaxis protocol adherence). Of the 430 patient-days without stress ulcer prophylaxis indications, 242 involved prophylaxis (56% inappropriate stress ulcer prophylaxis use). The overall appropriate use of stress ulcer prophylaxis was 64%. Factors associated with proper stress ulcer prophylaxis prescription were mechanical ventilation OR 2.13 (95%CI 1.64 – 2.75) and coagulopathy OR 2.77 (95%CI 1.66 – 4.60). The upper gastrointestinal bleeding incidence was 12.8%.
Conclusion:
Adherence to the stress ulcer prophylaxis protocol was low and inappropriate use of stress ulcer prophylaxis was frequent in this cohort of critically ill patients.
Keywords:Anti-ulcer agentsCritical careCritical illnessGastrointestinal hemorrhagePeptic ulcerTherapeutic adherence complianceSee more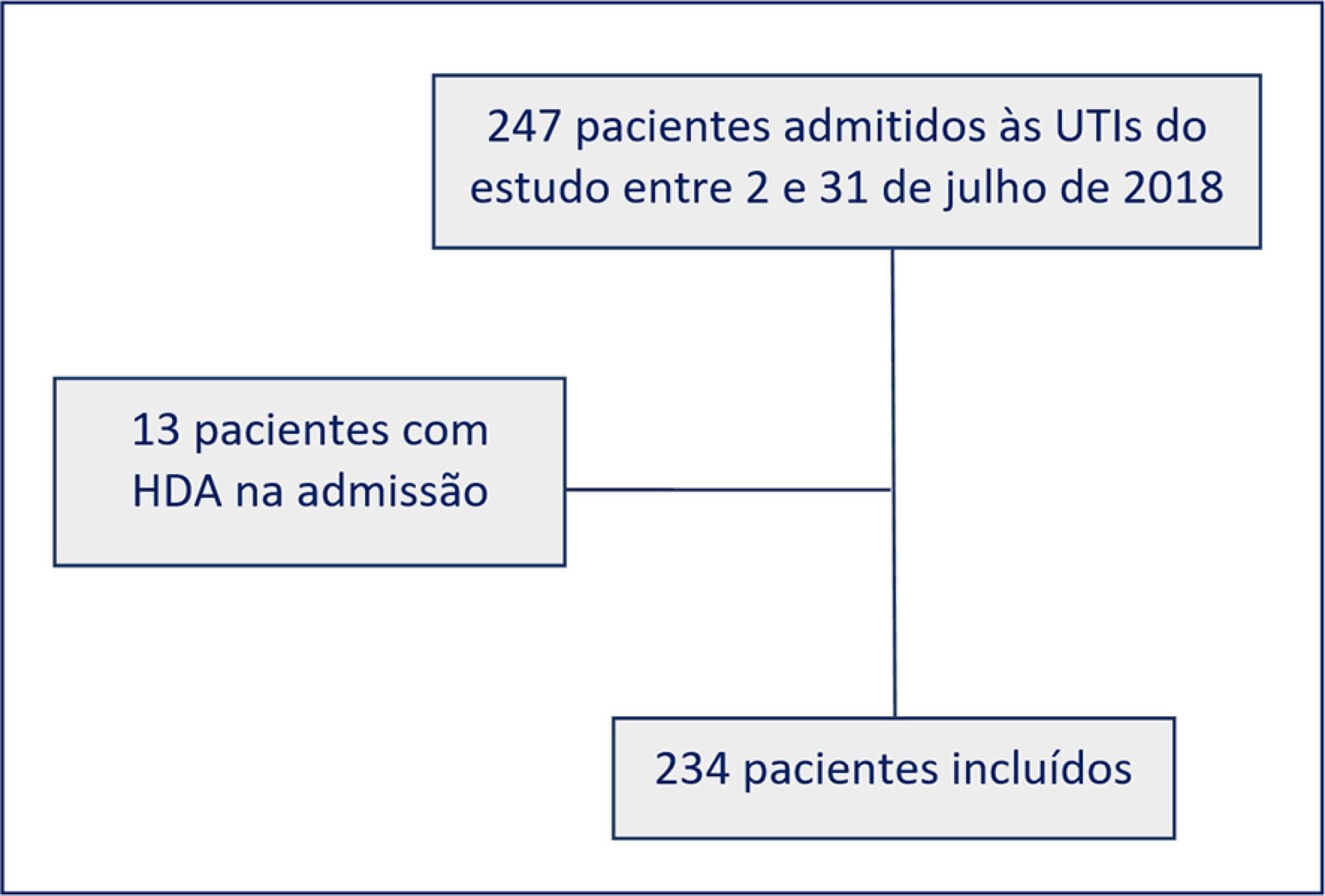
- Yuri de Albuquerque Pessoa dos Santos
-
Original Article
Mortality analysis of adult burn patients in Uruguay
Rev Bras Ter Intensiva. 2020;32(1):43-48
Abstract
Original ArticleMortality analysis of adult burn patients in Uruguay
Rev Bras Ter Intensiva. 2020;32(1):43-48
DOI 10.5935/0103-507X.20200008
Views0See moreABSTRACT
Objective:
To determine the independent risk factors associated with mortality in adult burn patients.
Methods:
This was a retrospective, observational study performed at the Centro Nacional de Queimados do Uruguai. All patients with skin burns admitted to the unit since its opening on July 1, 1995 through December 31, 2018 were included. The demographic data, burn profiles, length of stay, mechanical ventilation duration and hospital mortality were studied. A multivariate logistic regression was used to identify the risk factors for mortality. The standardized mortality ratio was calculated by dividing the number of observed deaths by the number of expected deaths (according to the Abbreviated Burn Severity Index).
Results:
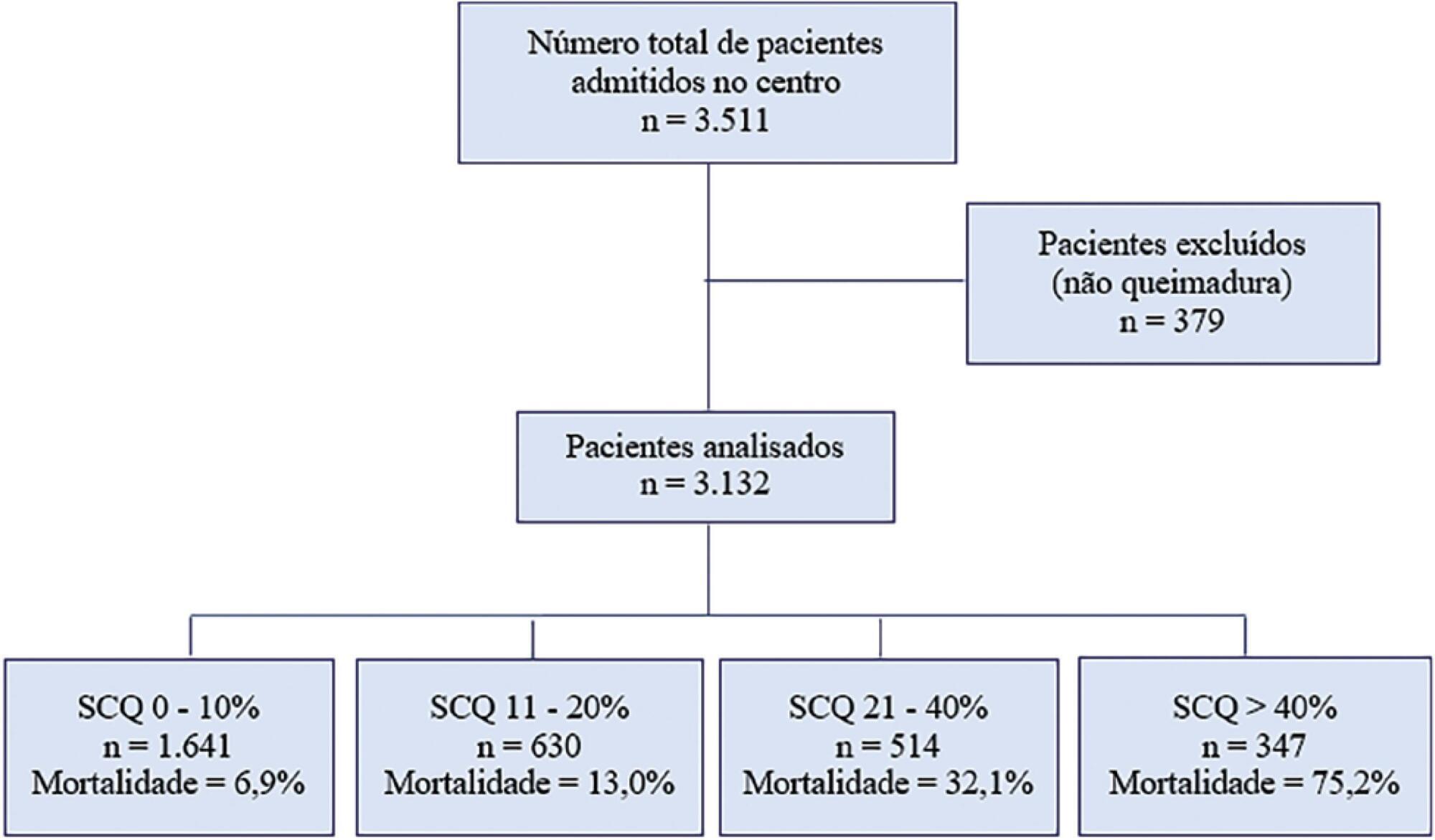
During the study period, 3,132 patients were included. The median total body surface area burned was 10% (3%-22%). The Abbreviated Burn Severity Index was 6 (4 – 7). Invasive mechanical ventilation was required in 60% of the patients for a median duration of 6 (3 – 16) days. The median length of stay in the unit was 17 (7 – 32) days. The global mortality was 19.9%. Crude mortality and standardized mortality ratio decreased from 1995 through 2018. The global standardized mortality ratio was 0.99. A need for mechanical ventilation (OR 8.80; 95%CI 5.68 – 13.62), older age (OR 1.07 per year; 95%CI 1.06 – 1.09), total body surface area burned (OR 1.05 per 1%; 95%CI 1.03 – 1.08) and extension of third-degree burns (OR 1.05 per 1%; 95%CI 1.03 – 1.07) were independent risk factors for mortality.
Conclusion:
The need for mechanical ventilation, older age and burn extension were independent risk factors for mortality in the burned adult Uruguayan population.
Views0Abstract
Original ArticleMortality analysis of adult burn patients in Uruguay
Rev Bras Ter Intensiva. 2020;32(1):43-48
DOI 10.5935/0103-507X.20200008
Views0See moreABSTRACT
Objective:
To determine the independent risk factors associated with mortality in adult burn patients.
Methods:
This was a retrospective, observational study performed at the Centro Nacional de Queimados do Uruguai. All patients with skin burns admitted to the unit since its opening on July 1, 1995 through December 31, 2018 were included. The demographic data, burn profiles, length of stay, mechanical ventilation duration and hospital mortality were studied. A multivariate logistic regression was used to identify the risk factors for mortality. The standardized mortality ratio was calculated by dividing the number of observed deaths by the number of expected deaths (according to the Abbreviated Burn Severity Index).
Results:
During the study period, 3,132 patients were included. The median total body surface area burned was 10% (3%-22%). The Abbreviated Burn Severity Index was 6 (4 – 7). Invasive mechanical ventilation was required in 60% of the patients for a median duration of 6 (3 – 16) days. The median length of stay in the unit was 17 (7 – 32) days. The global mortality was 19.9%. Crude mortality and standardized mortality ratio decreased from 1995 through 2018. The global standardized mortality ratio was 0.99. A need for mechanical ventilation (OR 8.80; 95%CI 5.68 – 13.62), older age (OR 1.07 per year; 95%CI 1.06 – 1.09), total body surface area burned (OR 1.05 per 1%; 95%CI 1.03 – 1.08) and extension of third-degree burns (OR 1.05 per 1%; 95%CI 1.03 – 1.07) were independent risk factors for mortality.
Conclusion:
The need for mechanical ventilation, older age and burn extension were independent risk factors for mortality in the burned adult Uruguayan population.
-
Original Article
Acute-on-chronic liver failure syndrome – clinical results from an intensive care unit in a liver transplant center
Rev Bras Ter Intensiva. 2020;32(1):49-57
Abstract
Original ArticleAcute-on-chronic liver failure syndrome – clinical results from an intensive care unit in a liver transplant center
Rev Bras Ter Intensiva. 2020;32(1):49-57
DOI 10.5935/0103-507X.20200009
Views0ABSTRACT
Objective:
To characterize a cohort of acute-on-chronic liver failure patients in Intensive Care and to analyze the all-cause 28-day mortality risk factors assessed at ICU admission and day 3.
Methods:
This was a retrospective cohort study of consecutive patients admitted to the intensive care unit between March 2013 and December 2016.
Results:
Seventy-one patients were included. The median age was 59 (51 – 64) years, and 81.7% of patients were male. Alcohol consumption alone (53.5%) was the most frequent etiology of cirrhosis and infection (53.5%) was the most common acute-on-chronic liver failure precipitating event. At intensive care unit admission, the clinical severity scores were APACHE II 21 (16 – 23), CLIF-SOFA 13 (11 – 15), Child-Pugh 12 (10 – 13) and MELD 27 (20 – 32). The acute-on-chronic liver failure scores were no-acute-on-chronic liver failure: 11.3%; one: 14.1%; two: 28.2% and three: 46.5%; and the number of organ failures was one: 4.2%; two: 42.3%; three: 32.4%; four: 16.9%; and five: 4.2%. Liver transplantation was performed in 15.5% of patients. The twenty-eight-day mortality rate was 56.3%, and the in-ICU mortality rate was 49.3%. Organ failure at intensive care unit admission (p = 0.02; OR 2.1; 95%CI 1.2 – 3.9), lactate concentration on day 3 (p = 0.02; OR 6.3; 95%CI 1.4 – 28.6) and the international normalized ratio on day 3 (p = 0.03; OR 10.2; 95%CI 1.3 – 82.8) were independent risk factors.
Conclusion:
Acute-on-chronic liver failure patients presented with high clinical severity and mortality rates. The number of organ failures at intensive care unit admission and the lactate and international normalized ratio on day 3 were independent risk factors for 28-day mortality. We consider intensive care essential for acute-on-chronic liver failure patients and timely liver transplant was vital for selected patients.
Keywords:CirrhosisCritical illnessInternational normalized ratioLactateMultiple organ failureTreatment outcomeSee moreViews0Abstract
Original ArticleAcute-on-chronic liver failure syndrome – clinical results from an intensive care unit in a liver transplant center
Rev Bras Ter Intensiva. 2020;32(1):49-57
DOI 10.5935/0103-507X.20200009
Views0ABSTRACT
Objective:
To characterize a cohort of acute-on-chronic liver failure patients in Intensive Care and to analyze the all-cause 28-day mortality risk factors assessed at ICU admission and day 3.
Methods:
This was a retrospective cohort study of consecutive patients admitted to the intensive care unit between March 2013 and December 2016.
Results:
Seventy-one patients were included. The median age was 59 (51 – 64) years, and 81.7% of patients were male. Alcohol consumption alone (53.5%) was the most frequent etiology of cirrhosis and infection (53.5%) was the most common acute-on-chronic liver failure precipitating event. At intensive care unit admission, the clinical severity scores were APACHE II 21 (16 – 23), CLIF-SOFA 13 (11 – 15), Child-Pugh 12 (10 – 13) and MELD 27 (20 – 32). The acute-on-chronic liver failure scores were no-acute-on-chronic liver failure: 11.3%; one: 14.1%; two: 28.2% and three: 46.5%; and the number of organ failures was one: 4.2%; two: 42.3%; three: 32.4%; four: 16.9%; and five: 4.2%. Liver transplantation was performed in 15.5% of patients. The twenty-eight-day mortality rate was 56.3%, and the in-ICU mortality rate was 49.3%. Organ failure at intensive care unit admission (p = 0.02; OR 2.1; 95%CI 1.2 – 3.9), lactate concentration on day 3 (p = 0.02; OR 6.3; 95%CI 1.4 – 28.6) and the international normalized ratio on day 3 (p = 0.03; OR 10.2; 95%CI 1.3 – 82.8) were independent risk factors.
Conclusion:
Acute-on-chronic liver failure patients presented with high clinical severity and mortality rates. The number of organ failures at intensive care unit admission and the lactate and international normalized ratio on day 3 were independent risk factors for 28-day mortality. We consider intensive care essential for acute-on-chronic liver failure patients and timely liver transplant was vital for selected patients.
Keywords:CirrhosisCritical illnessInternational normalized ratioLactateMultiple organ failureTreatment outcomeSee more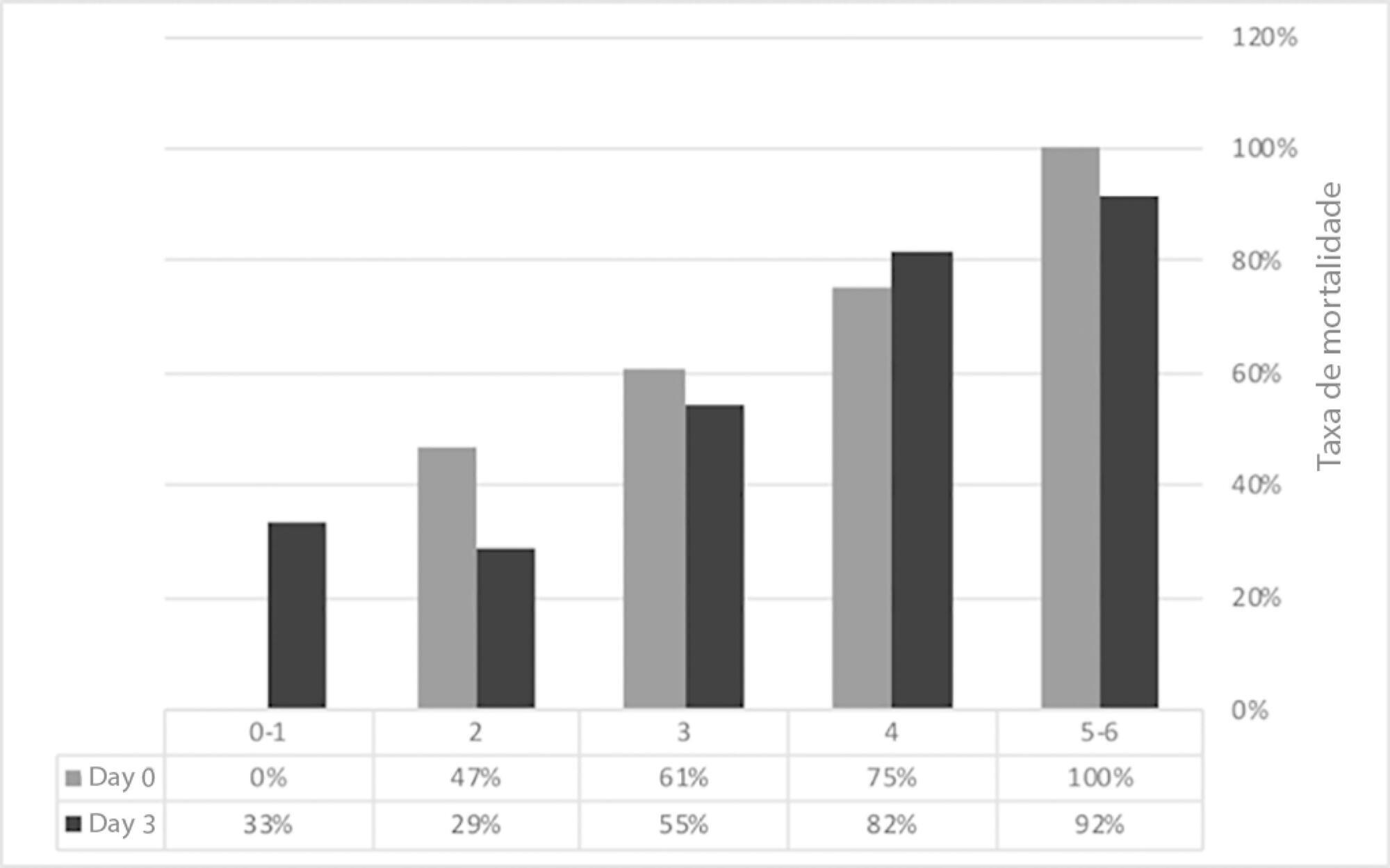
-
Original Article
Pretreatment with adalimumab reduces ventilator-induced lung injury in an experimental model
- Enrique Correger ,
- Josefina Marcos,
- Graciela Laguens,
- Pablo Stringa,
- Pablo Cardinal-Fernández, [ … ],
- Lluis Blanch
Abstract
Original ArticlePretreatment with adalimumab reduces ventilator-induced lung injury in an experimental model
Rev Bras Ter Intensiva. 2020;32(1):58-65
DOI 10.5935/0103-507X.20200010
- Enrique Correger ,
- Josefina Marcos,
- Graciela Laguens,
- Pablo Stringa,
- Pablo Cardinal-Fernández,
- Lluis Blanch
Views0ABSTRACT
Objective:
To determine whether adalimumab administration before mechanical ventilation reduces ventilator-induced lung injury (VILI).
Methods:
Eighteen rats randomized into 3 groups underwent mechanical ventilation for 3 hours with a fraction of inspired oxygen = 0.40% including a low tidal volume group (n = 6), where tidal volume = 8mL/kg and positive end-expiratory pressure = 5cmH2O; a high tidal volume group (n = 6), where tidal volume = 35mL/kg and positive end-expiratory pressure = 0; and a pretreated + high tidal volume group (n = 6) where adalimumab (100ug/kg) was administered intraperitoneally 24 hours before mechanical ventilation + tidal volume = 35mL/kg and positive end-expiratory pressure = 0. ANOVA was used to compare histological damage (ATS 2010 Lung Injury Scoring System), pulmonary edema, lung compliance, arterial partial pressure of oxygen, and mean arterial pressure among the groups.
Results:
After 3 hours of ventilation, the mean histological lung injury score was higher in the high tidal volume group than in the low tidal volume group (0.030 versus 0.0051, respectively, p = 0.003). The high tidal volume group showed diminished lung compliance at 3 hours (p = 0.04) and hypoxemia (p = 0,018 versus control). Pretreated HVt group had an improved histological score, mainly due to a significant reduction in leukocyte infiltration (p = 0.003).
Conclusion:
Histological examination after 3 hours of injurious ventilation revealed ventilator-induced lung injury in the absence of measurable changes in lung mechanics or oxygenation; administering adalimumab before mechanical ventilation reduced lung edema and histological damage.
Keywords:Adalimumab/administration & dosageRespiration, artificialrespiratory failureVentilator-induced lung injurySee moreViews0Abstract
Original ArticlePretreatment with adalimumab reduces ventilator-induced lung injury in an experimental model
Rev Bras Ter Intensiva. 2020;32(1):58-65
DOI 10.5935/0103-507X.20200010
- Enrique Correger ,
- Josefina Marcos,
- Graciela Laguens,
- Pablo Stringa,
- Pablo Cardinal-Fernández,
- Lluis Blanch
Views0ABSTRACT
Objective:
To determine whether adalimumab administration before mechanical ventilation reduces ventilator-induced lung injury (VILI).
Methods:
Eighteen rats randomized into 3 groups underwent mechanical ventilation for 3 hours with a fraction of inspired oxygen = 0.40% including a low tidal volume group (n = 6), where tidal volume = 8mL/kg and positive end-expiratory pressure = 5cmH2O; a high tidal volume group (n = 6), where tidal volume = 35mL/kg and positive end-expiratory pressure = 0; and a pretreated + high tidal volume group (n = 6) where adalimumab (100ug/kg) was administered intraperitoneally 24 hours before mechanical ventilation + tidal volume = 35mL/kg and positive end-expiratory pressure = 0. ANOVA was used to compare histological damage (ATS 2010 Lung Injury Scoring System), pulmonary edema, lung compliance, arterial partial pressure of oxygen, and mean arterial pressure among the groups.
Results:
After 3 hours of ventilation, the mean histological lung injury score was higher in the high tidal volume group than in the low tidal volume group (0.030 versus 0.0051, respectively, p = 0.003). The high tidal volume group showed diminished lung compliance at 3 hours (p = 0.04) and hypoxemia (p = 0,018 versus control). Pretreated HVt group had an improved histological score, mainly due to a significant reduction in leukocyte infiltration (p = 0.003).
Conclusion:
Histological examination after 3 hours of injurious ventilation revealed ventilator-induced lung injury in the absence of measurable changes in lung mechanics or oxygenation; administering adalimumab before mechanical ventilation reduced lung edema and histological damage.
Keywords:Adalimumab/administration & dosageRespiration, artificialrespiratory failureVentilator-induced lung injurySee more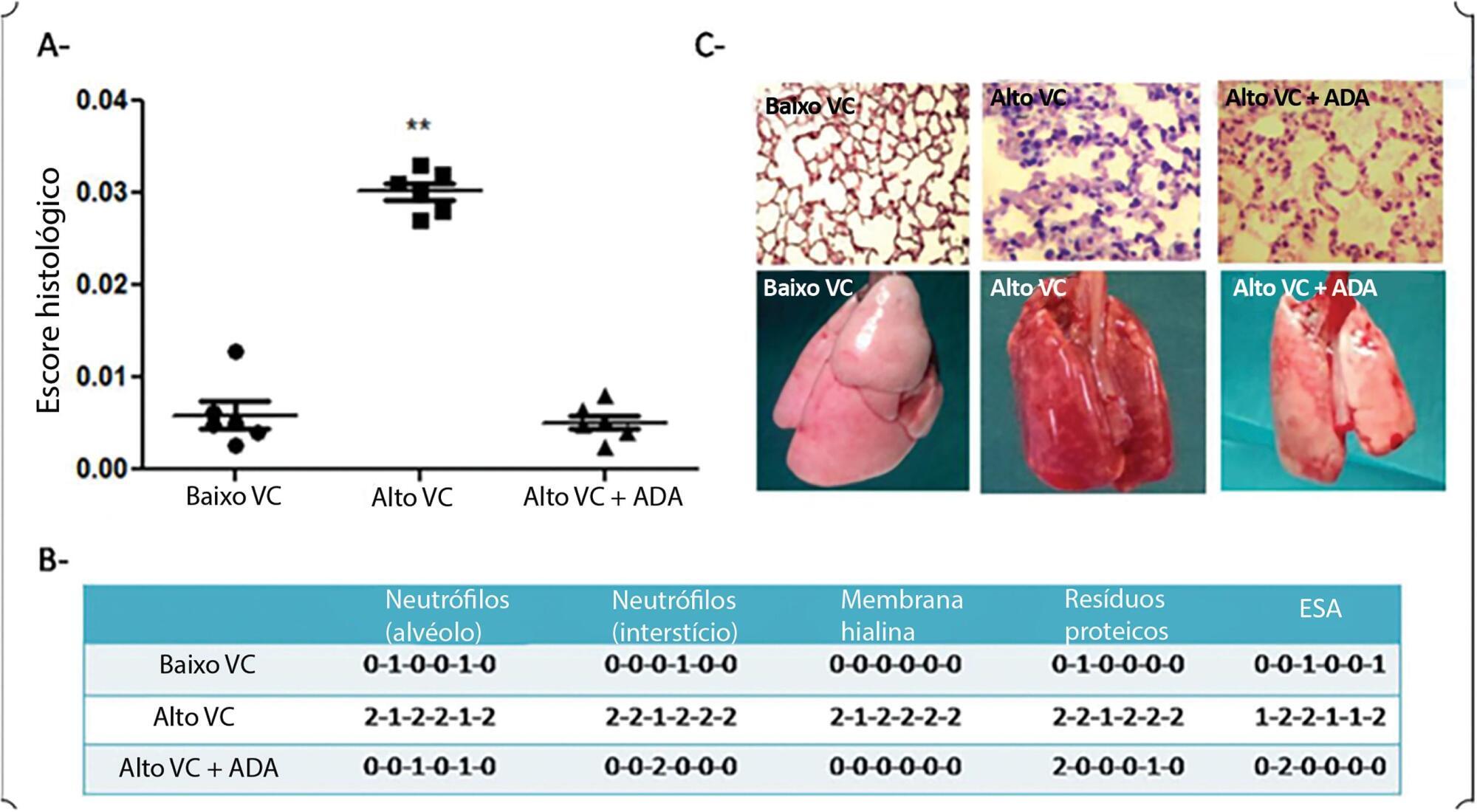
- Enrique Correger
-
Original Article
Temporal assessment of neonatal pain after airway aspiration
- Isabelle Leandro Gimenez,
- Rafaella Fintelman Rodrigues,
- Marcella Campos de Faria Oliveira,
- Beatriz Alves Rezende Santos,
- Vanessa da Silva Neves Moreira Arakaki, [ … ],
- Halina Cidrini Ferreira
Abstract
Original ArticleTemporal assessment of neonatal pain after airway aspiration
Rev Bras Ter Intensiva. 2020;32(1):66-71
DOI 10.5935/0103-507X.20200011
- Isabelle Leandro Gimenez,
- Rafaella Fintelman Rodrigues,
- Marcella Campos de Faria Oliveira,
- Beatriz Alves Rezende Santos,
- Vanessa da Silva Neves Moreira Arakaki,
- Rosana Silva dos Santos,
- Rodrigo Tosta Peres,
- Clemax Couto Sant’Anna,
- Halina Cidrini Ferreira
Views0ABSTRACT
Objective:
To temporally assess a painful stimulus in premature infants using 3 neonatal pain scales.
Methods:
A total of 83 premature infants were observed during airway aspiration by 3 evaluators (E1, E2 and E3) using 3 pain assessment scales (Neonatal Facial Coding System – NFCS; Neonatal Infant Pain Scale – NIPS; and Premature Infant Pain Profile – PIPP) at 5 time points: T1 (before airway aspiration), T2 (during airway aspiration), T3 (1 minute after airway aspiration), T4 (3 minutes after airway aspiration), and T5 (5 minutes after airway aspiration). Light’s Kappa (agreement among examiners and among scales at each time point) and the McNemar test (comparison among time points) were used considering p < 0.05.
Results:
There was a significant difference between the 3 examiners for T1 and T2 using the 3 scales. In T3, pain was observed in 22.9%/E1, 28.9%/E2, and 24.1%/E3 according to the NFCS; 22.9%/E1, 21.7%/E2, and 16.9%/E3 according to the NIPS; and 49.4%/E1, 53.9%/E2, and 47%/E3 according to the PIPP. There was a difference between T1 and T3 using the 3 scales, except for 2 examiners for the PIPP (E2: p = 0.15/E3: p = 0.17). Comparing T4 and T5 to T1, there was no difference in the 3 scales.
Conclusion:
Premature infants required at least 3 minutes to return to their initial state of rest (no pain).
Keywords:Infant, prematurePainPain measurementReproducibility of resultsSuctionSurveys and questionnairesSee moreViews0Abstract
Original ArticleTemporal assessment of neonatal pain after airway aspiration
Rev Bras Ter Intensiva. 2020;32(1):66-71
DOI 10.5935/0103-507X.20200011
- Isabelle Leandro Gimenez,
- Rafaella Fintelman Rodrigues,
- Marcella Campos de Faria Oliveira,
- Beatriz Alves Rezende Santos,
- Vanessa da Silva Neves Moreira Arakaki,
- Rosana Silva dos Santos,
- Rodrigo Tosta Peres,
- Clemax Couto Sant’Anna,
- Halina Cidrini Ferreira
Views0ABSTRACT
Objective:
To temporally assess a painful stimulus in premature infants using 3 neonatal pain scales.
Methods:
A total of 83 premature infants were observed during airway aspiration by 3 evaluators (E1, E2 and E3) using 3 pain assessment scales (Neonatal Facial Coding System – NFCS; Neonatal Infant Pain Scale – NIPS; and Premature Infant Pain Profile – PIPP) at 5 time points: T1 (before airway aspiration), T2 (during airway aspiration), T3 (1 minute after airway aspiration), T4 (3 minutes after airway aspiration), and T5 (5 minutes after airway aspiration). Light’s Kappa (agreement among examiners and among scales at each time point) and the McNemar test (comparison among time points) were used considering p < 0.05.
Results:
There was a significant difference between the 3 examiners for T1 and T2 using the 3 scales. In T3, pain was observed in 22.9%/E1, 28.9%/E2, and 24.1%/E3 according to the NFCS; 22.9%/E1, 21.7%/E2, and 16.9%/E3 according to the NIPS; and 49.4%/E1, 53.9%/E2, and 47%/E3 according to the PIPP. There was a difference between T1 and T3 using the 3 scales, except for 2 examiners for the PIPP (E2: p = 0.15/E3: p = 0.17). Comparing T4 and T5 to T1, there was no difference in the 3 scales.
Conclusion:
Premature infants required at least 3 minutes to return to their initial state of rest (no pain).
Keywords:Infant, prematurePainPain measurementReproducibility of resultsSuctionSurveys and questionnairesSee more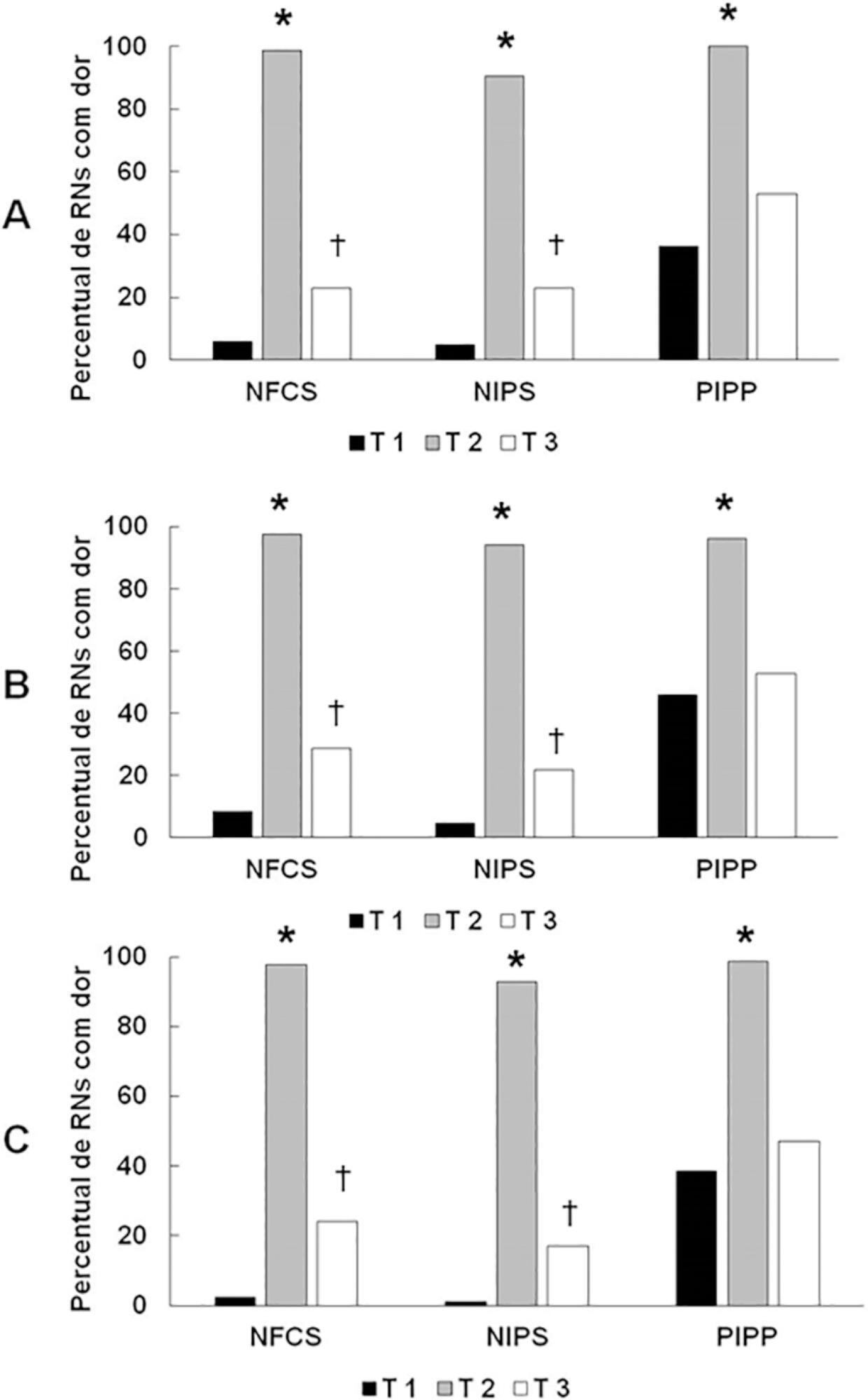
-
Original Article
Intensive care inequity in Rio de Janeiro: the effect of spatial distribution of health services on severe acute respiratory infection
- Sandro Javier Bedoya-Pacheco,
- Romeu Ferreira Emygdio,
- José Antônio Sena do Nascimento,
- Jorge André Marques Bravo ,
- Fernando Augusto Bozza
Abstract
Original ArticleIntensive care inequity in Rio de Janeiro: the effect of spatial distribution of health services on severe acute respiratory infection
Rev Bras Ter Intensiva. 2020;32(1):72-80
DOI 10.5935/0103-507X.20200012
- Sandro Javier Bedoya-Pacheco,
- Romeu Ferreira Emygdio,
- José Antônio Sena do Nascimento,
- Jorge André Marques Bravo ,
- Fernando Augusto Bozza
Views2ABSTRACT
Objective:
To analyze the distribution of adult intensive care units according to geographic region and health sector in Rio de Janeiro and to investigate severe acute respiratory infection mortality in the public sector and its association with critical care capacity in the public sector.
Methods:
We evaluated the variation in intensive care availability and severe acute respiratory infection mortality in the public sector across different areas of the city in 2014. We utilized databases from the National Registry of Health Establishments, the Brazilian Institute of Geography and Statistics, the National Mortality Information System and the Hospital Admission Information System.
Results:
There is a wide range of intensive care unit beds per capita (from 4.0 intensive care unit beds per 100,000 people in public hospitals in the West Zone to 133.6 intensive care unit beds per 100,000 people in private hospitals in the Center Zone) in the city of Rio de Janeiro. The private sector accounts for almost 75% of the intensive care unit bed supply. The more developed areas of the city concentrate most of the intensive care unit services. Map-based spatial analysis shows a lack of intensive care unit beds in vast territorial extensions in the less developed regions of the city. There is an inverse correlation (r = -0.829; 95%CI -0.946 to -0.675) between public intensive care unit beds per capita in different health planning areas of the city and severe acute respiratory infection mortality in public hospitals.
Conclusion:
Our results show a disproportionate intensive care unit bed provision across the city of Rio de Janeiro and the need for a rational distribution of intensive care.
Keywords:Health status disparitiesIntensive care units/organization & administrationQuality of health careRespiratory tract infectionsSee moreViews2Abstract
Original ArticleIntensive care inequity in Rio de Janeiro: the effect of spatial distribution of health services on severe acute respiratory infection
Rev Bras Ter Intensiva. 2020;32(1):72-80
DOI 10.5935/0103-507X.20200012
- Sandro Javier Bedoya-Pacheco,
- Romeu Ferreira Emygdio,
- José Antônio Sena do Nascimento,
- Jorge André Marques Bravo ,
- Fernando Augusto Bozza
Views2ABSTRACT
Objective:
To analyze the distribution of adult intensive care units according to geographic region and health sector in Rio de Janeiro and to investigate severe acute respiratory infection mortality in the public sector and its association with critical care capacity in the public sector.
Methods:
We evaluated the variation in intensive care availability and severe acute respiratory infection mortality in the public sector across different areas of the city in 2014. We utilized databases from the National Registry of Health Establishments, the Brazilian Institute of Geography and Statistics, the National Mortality Information System and the Hospital Admission Information System.
Results:
There is a wide range of intensive care unit beds per capita (from 4.0 intensive care unit beds per 100,000 people in public hospitals in the West Zone to 133.6 intensive care unit beds per 100,000 people in private hospitals in the Center Zone) in the city of Rio de Janeiro. The private sector accounts for almost 75% of the intensive care unit bed supply. The more developed areas of the city concentrate most of the intensive care unit services. Map-based spatial analysis shows a lack of intensive care unit beds in vast territorial extensions in the less developed regions of the city. There is an inverse correlation (r = -0.829; 95%CI -0.946 to -0.675) between public intensive care unit beds per capita in different health planning areas of the city and severe acute respiratory infection mortality in public hospitals.
Conclusion:
Our results show a disproportionate intensive care unit bed provision across the city of Rio de Janeiro and the need for a rational distribution of intensive care.
Keywords:Health status disparitiesIntensive care units/organization & administrationQuality of health careRespiratory tract infectionsSee more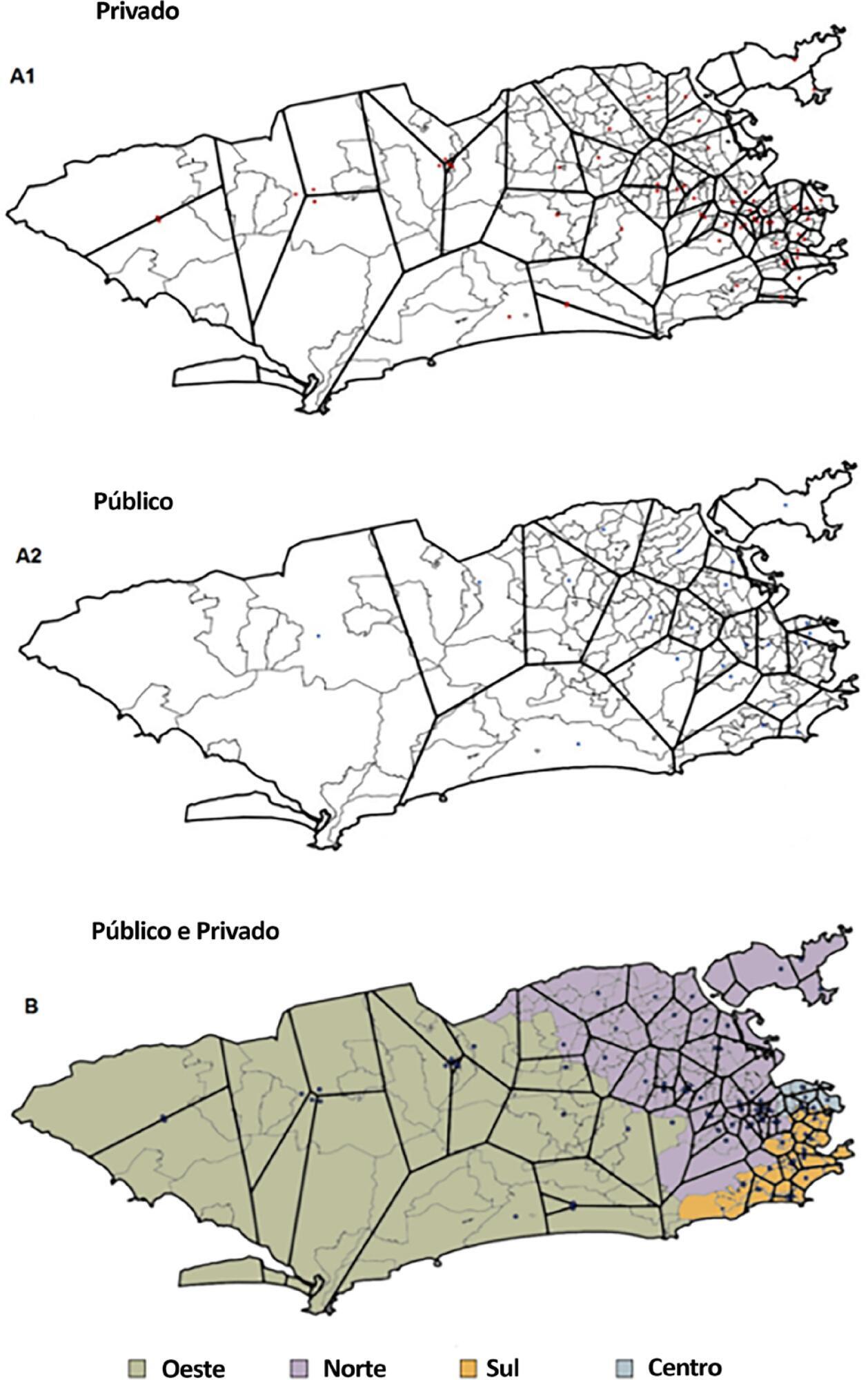
-
Original Article
Titration and characteristics of pressure-support ventilation use in Argentina: an online cross-sectional survey study
- Joaquin Pérez ,
- Javier Hernán Dorado,
- Ana Carolina Papazian,
- Maricel Berastegui,
- Daniela Inés Gilgado, [ … ],
- Matías Accoce
Abstract
Original ArticleTitration and characteristics of pressure-support ventilation use in Argentina: an online cross-sectional survey study
Rev Bras Ter Intensiva. 2020;32(1):81-91
DOI 10.5935/0103-507X.20200013
- Joaquin Pérez ,
- Javier Hernán Dorado,
- Ana Carolina Papazian,
- Maricel Berastegui,
- Daniela Inés Gilgado,
- Gimena Paola Cardoso,
- Cristian Cesio,
- Matías Accoce
Views1ABSTRACT
Objective:
To identify common practices related to the use and titration of pressure-support ventilation (PC-CSV – pressure control-continuous spontaneous ventilation) in patients under mechanical ventilation and to analyze diagnostic criteria for over-assistance and under-assistance. The secondary objective was to compare the responses provided by physician, physiotherapists and nurses related to diagnostic criteria for over-assistance and under-assistance.
Methods:
An online survey was conducted using the Survey Monkey tool. Physicians, nurses and physiotherapists from Argentina with access to PC-CSV in their usual clinical practice were included.
Results:
A total of 509 surveys were collected from October to December 2018. Of these, 74.1% were completed by physiotherapists. A total of 77.6% reported using PC-CSV to initiate the partial ventilatory support phase, and 43.8% of respondents select inspiratory pressure support level based on tidal volume. The main objective for selecting positive end-expiratory pressure (PEEP) level was to decrease the work of breathing. High tidal volume was the primary variable for detecting over-assistance, while the use of accessory respiratory muscles was the most commonly chosen for under-assistance. Discrepancies were observed between physicians and physiotherapists in relation to the diagnostic criteria for over-assistance.
Conclusion:
The most commonly used mode to initiate the partial ventilatory support phase was PC-CSV. The most frequently selected variable to guide the titration of inspiratory pressure support level was tidal volume, and the main objective of PEEP was to decrease the work of breathing. Over-assistance was detected primarily by high tidal volume, while under-assistance by accessory respiratory muscles activation. Discrepancies were observed among professions in relation to the diagnostic criteria for over-assistance, but not for under-assistance.
Keywords:Health care surveysIntensive care unitsInteractive ventilatory supportPositive-pressure ventilationRespiration, artificialSee moreViews1Abstract
Original ArticleTitration and characteristics of pressure-support ventilation use in Argentina: an online cross-sectional survey study
Rev Bras Ter Intensiva. 2020;32(1):81-91
DOI 10.5935/0103-507X.20200013
- Joaquin Pérez ,
- Javier Hernán Dorado,
- Ana Carolina Papazian,
- Maricel Berastegui,
- Daniela Inés Gilgado,
- Gimena Paola Cardoso,
- Cristian Cesio,
- Matías Accoce
Views1ABSTRACT
Objective:
To identify common practices related to the use and titration of pressure-support ventilation (PC-CSV – pressure control-continuous spontaneous ventilation) in patients under mechanical ventilation and to analyze diagnostic criteria for over-assistance and under-assistance. The secondary objective was to compare the responses provided by physician, physiotherapists and nurses related to diagnostic criteria for over-assistance and under-assistance.
Methods:
An online survey was conducted using the Survey Monkey tool. Physicians, nurses and physiotherapists from Argentina with access to PC-CSV in their usual clinical practice were included.
Results:
A total of 509 surveys were collected from October to December 2018. Of these, 74.1% were completed by physiotherapists. A total of 77.6% reported using PC-CSV to initiate the partial ventilatory support phase, and 43.8% of respondents select inspiratory pressure support level based on tidal volume. The main objective for selecting positive end-expiratory pressure (PEEP) level was to decrease the work of breathing. High tidal volume was the primary variable for detecting over-assistance, while the use of accessory respiratory muscles was the most commonly chosen for under-assistance. Discrepancies were observed between physicians and physiotherapists in relation to the diagnostic criteria for over-assistance.
Conclusion:
The most commonly used mode to initiate the partial ventilatory support phase was PC-CSV. The most frequently selected variable to guide the titration of inspiratory pressure support level was tidal volume, and the main objective of PEEP was to decrease the work of breathing. Over-assistance was detected primarily by high tidal volume, while under-assistance by accessory respiratory muscles activation. Discrepancies were observed among professions in relation to the diagnostic criteria for over-assistance, but not for under-assistance.
Keywords:Health care surveysIntensive care unitsInteractive ventilatory supportPositive-pressure ventilationRespiration, artificialSee more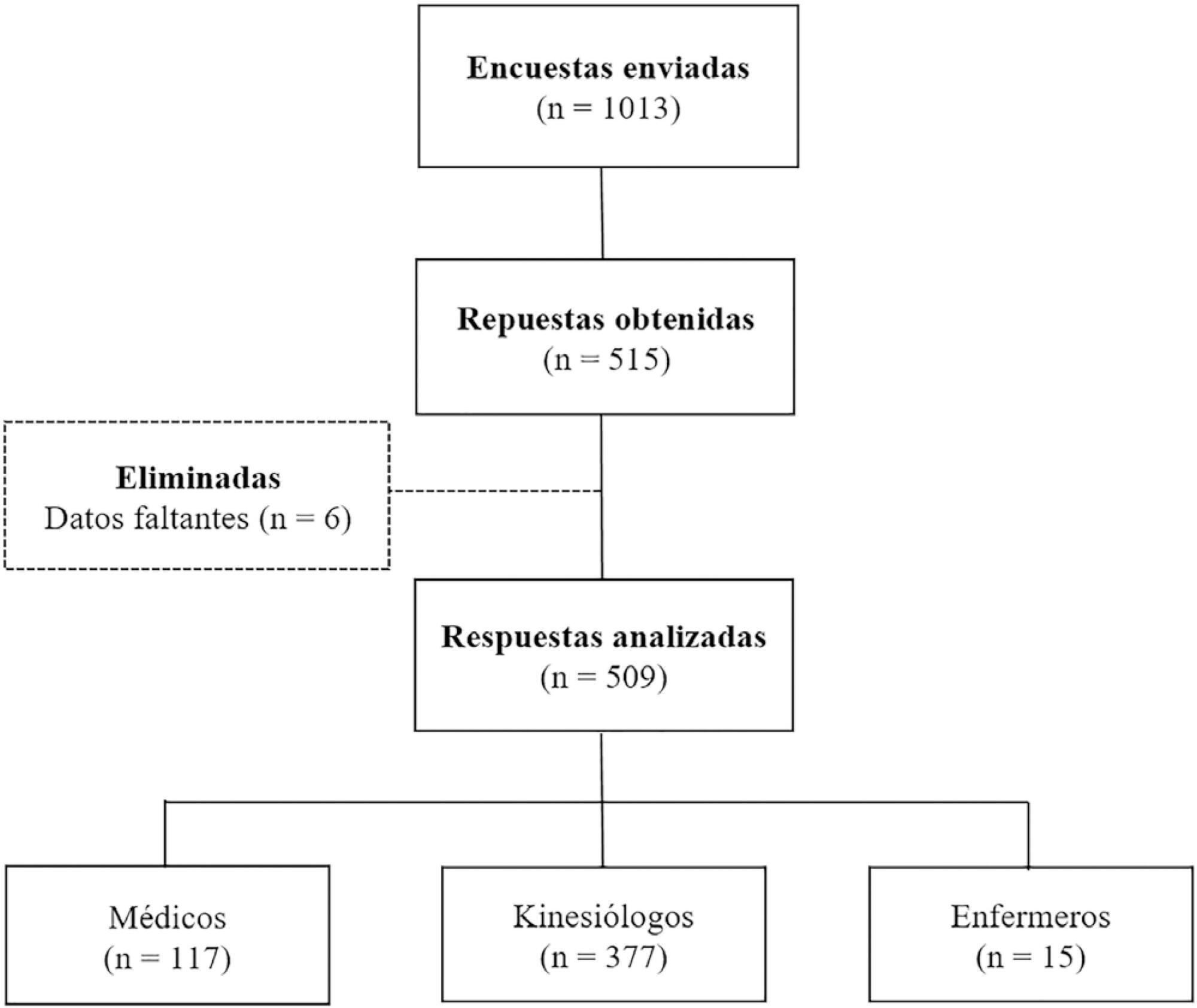
- Joaquin Pérez
-
Original Article
Adverse outcomes of delayed intensive care unit
Rev Bras Ter Intensiva. 2020;32(1):92-98
Abstract
Original ArticleAdverse outcomes of delayed intensive care unit
Rev Bras Ter Intensiva. 2020;32(1):92-98
DOI 10.5935/0103-507X.20200014
Views1See moreABSTRACT
Objective:
To examine the impact of delayed transfer from the emergency room into the intensive care unit on the length of intensive care unit stay and death.
Methods:
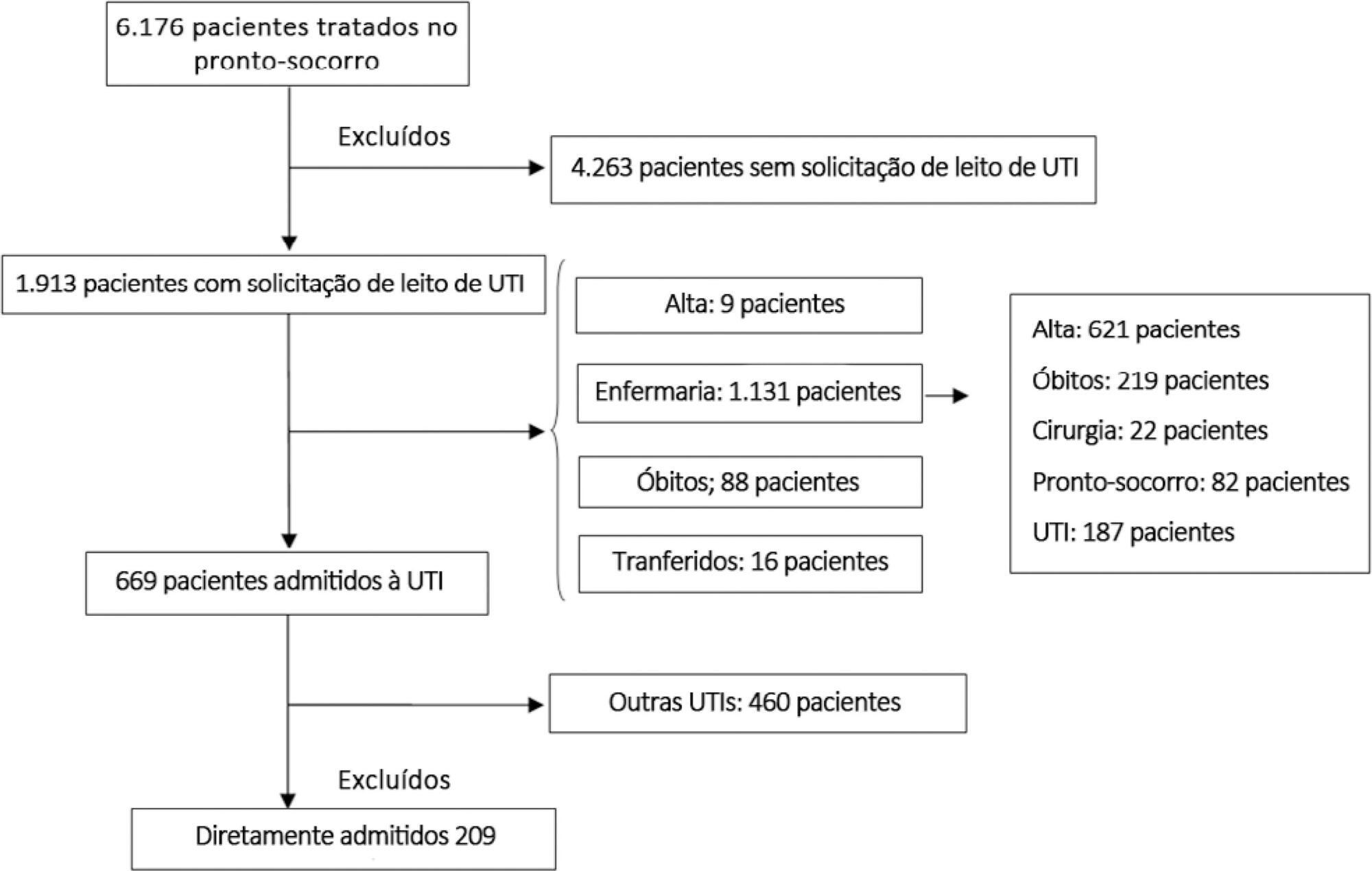
This prospective, cohort study performed in a tertiary academic hospital obtained data from 1913 patients admitted to the emergency room with a documented request for admission into the intensive care unit. The patients admitted directly into the medical-surgical intensive care unit (n = 209) were categorized into tertiles according to their waiting time for intensive care unit admission (Group 1: < 637 min, Group 2: 637 to 1602 min, and Group 3: > 1602 min). Patients who stayed in the intensive care unit for longer than 3.2 days (median time of intensive care unit length of stay of all patients) were considered as having a prolonged intensive care unit stay.
Results:
A total of 6,176 patients were treated in the emergency room during the study period, among whom 1,913 (31%) required a bed in the intensive care unit. The median length of stay in the emergency room was 17 hours [9 to 33 hours]. Hospitalization for infection/sepsis was an independent predictor of prolonged intensive care unit stay (OR 2.75 95%CI 1.38 – 5.48, p = 0.004), but waiting time for intensive care unit admission was not. The mortality rate was higher in Group 3 (38%) than in Group 1 (31%) but the difference was not statistically significant.
Conclusion:
Delayed admission into the intensive care unit from the emergency room did not result in an increased intensive care unit stay or mortality.
Views1Abstract
Original ArticleAdverse outcomes of delayed intensive care unit
Rev Bras Ter Intensiva. 2020;32(1):92-98
DOI 10.5935/0103-507X.20200014
Views1See moreABSTRACT
Objective:
To examine the impact of delayed transfer from the emergency room into the intensive care unit on the length of intensive care unit stay and death.
Methods:
This prospective, cohort study performed in a tertiary academic hospital obtained data from 1913 patients admitted to the emergency room with a documented request for admission into the intensive care unit. The patients admitted directly into the medical-surgical intensive care unit (n = 209) were categorized into tertiles according to their waiting time for intensive care unit admission (Group 1: < 637 min, Group 2: 637 to 1602 min, and Group 3: > 1602 min). Patients who stayed in the intensive care unit for longer than 3.2 days (median time of intensive care unit length of stay of all patients) were considered as having a prolonged intensive care unit stay.
Results:
A total of 6,176 patients were treated in the emergency room during the study period, among whom 1,913 (31%) required a bed in the intensive care unit. The median length of stay in the emergency room was 17 hours [9 to 33 hours]. Hospitalization for infection/sepsis was an independent predictor of prolonged intensive care unit stay (OR 2.75 95%CI 1.38 – 5.48, p = 0.004), but waiting time for intensive care unit admission was not. The mortality rate was higher in Group 3 (38%) than in Group 1 (31%) but the difference was not statistically significant.
Conclusion:
Delayed admission into the intensive care unit from the emergency room did not result in an increased intensive care unit stay or mortality.
-
Original Article
Fluid overload in patients with septic shock and lactate clearance as a therapeutic goal: a retrospective cohort study
Rev Bras Ter Intensiva. 2020;32(1):99-107
Abstract
Original ArticleFluid overload in patients with septic shock and lactate clearance as a therapeutic goal: a retrospective cohort study
Rev Bras Ter Intensiva. 2020;32(1):99-107
DOI 10.5935/0103-507X.20200015
Views0See moreABSTRACT
Objective:
To assess whether fluid overload in fluid therapy is a prognostic factor for patients with septic shock when adjusted for lactate clearance goals.
Methods:
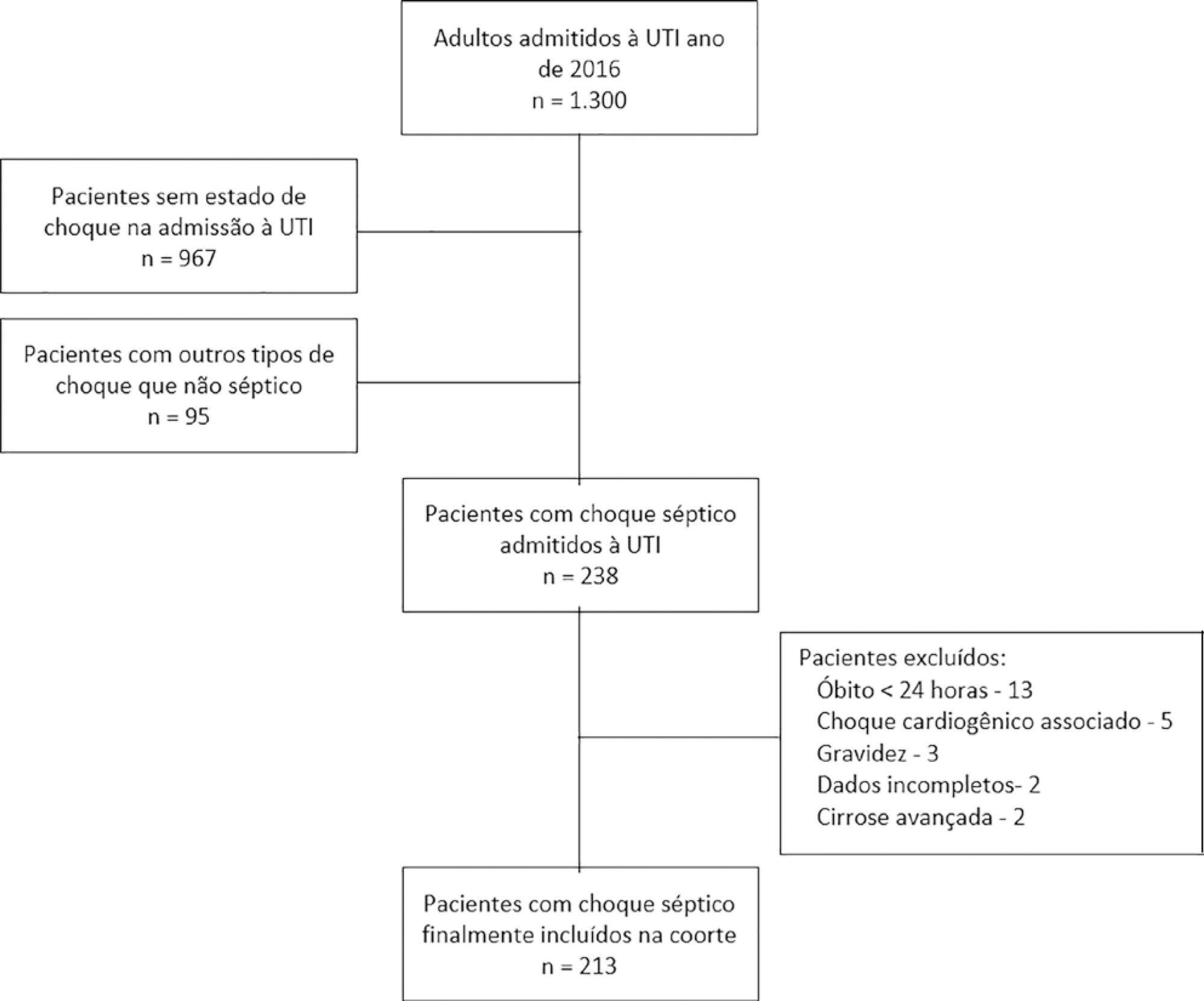
This was a retrospective cohort study conducted at a level IV care hospital in Bogotá, Colombia. A cohort of patients with septic shock was assembled. Their characteristics and fluid balance were documented. The patients were stratified by exposure levels according to the magnitude of fluid overload by body weight after 24 hours of therapy. Mortality was determined at 30 days, and an unconditional logistic regression model was created, adjusting for confounders. The statistical significance was established at p ≤ 0.05.
Results:
There were 213 patients with septic shock, and 60.8% had a lactate clearance ≥ 50% after treatment. Ninety-seven (46%) patients developed fluid overload ≥ 5%, and only 30 (13%) developed overload ≥ 10%. Patients exhibiting fluid overload ≥ 5% received an average of 6227mL of crystalloids (SD ± 5838mL) in 24 hours, compared to 3978mL (SD ± 3728mL) among unexposed patients (p = 0.000). The patients who developed fluid overload were treated with mechanical ventilation (70.7% versus 50.8%) (p = 0.003), albumin (74.7% versus 55.2%) (p = 0.003) and corticosteroids (53.5% versus 35.0%) (p = 0.006) more frequently than those who did not develop fluid overload. In the multivariable analysis, cumulative fluid balance was not associated with mortality (OR 1.03; 95%CI 0.89 – 1.20).
Conclusions:
Adjusting for the severity of the condition and adequate lactate clearance, cumulative fluid balance was not associated with increased mortality in this Latin American cohort of septic patients.
Views0Abstract
Original ArticleFluid overload in patients with septic shock and lactate clearance as a therapeutic goal: a retrospective cohort study
Rev Bras Ter Intensiva. 2020;32(1):99-107
DOI 10.5935/0103-507X.20200015
Views0See moreABSTRACT
Objective:
To assess whether fluid overload in fluid therapy is a prognostic factor for patients with septic shock when adjusted for lactate clearance goals.
Methods:
This was a retrospective cohort study conducted at a level IV care hospital in Bogotá, Colombia. A cohort of patients with septic shock was assembled. Their characteristics and fluid balance were documented. The patients were stratified by exposure levels according to the magnitude of fluid overload by body weight after 24 hours of therapy. Mortality was determined at 30 days, and an unconditional logistic regression model was created, adjusting for confounders. The statistical significance was established at p ≤ 0.05.
Results:
There were 213 patients with septic shock, and 60.8% had a lactate clearance ≥ 50% after treatment. Ninety-seven (46%) patients developed fluid overload ≥ 5%, and only 30 (13%) developed overload ≥ 10%. Patients exhibiting fluid overload ≥ 5% received an average of 6227mL of crystalloids (SD ± 5838mL) in 24 hours, compared to 3978mL (SD ± 3728mL) among unexposed patients (p = 0.000). The patients who developed fluid overload were treated with mechanical ventilation (70.7% versus 50.8%) (p = 0.003), albumin (74.7% versus 55.2%) (p = 0.003) and corticosteroids (53.5% versus 35.0%) (p = 0.006) more frequently than those who did not develop fluid overload. In the multivariable analysis, cumulative fluid balance was not associated with mortality (OR 1.03; 95%CI 0.89 – 1.20).
Conclusions:
Adjusting for the severity of the condition and adequate lactate clearance, cumulative fluid balance was not associated with increased mortality in this Latin American cohort of septic patients.
-
Original Article
Stratification to predict the response to antioxidant
- Cristiane Ritter,
- Larissa Constantino,
- Monique Michels ,
- Renata Casagrande Gonçalves,
- Cassiana Fraga, [ … ],
- Felipe Dal-Pizzol
Abstract
Original ArticleStratification to predict the response to antioxidant
Rev Bras Ter Intensiva. 2020;32(1):108-114
DOI 10.5935/0103-507X.20200016
- Cristiane Ritter,
- Larissa Constantino,
- Monique Michels ,
- Renata Casagrande Gonçalves,
- Cassiana Fraga,
- Danusa Damásio,
- Felipe Dal-Pizzol
Views1See moreABSTRACT
Objective:
To examine the effectiveness of stratification to identify and target antioxidant therapy for animal models of lethal sepsis and in patients who develop sustained hypotension.
Methods:
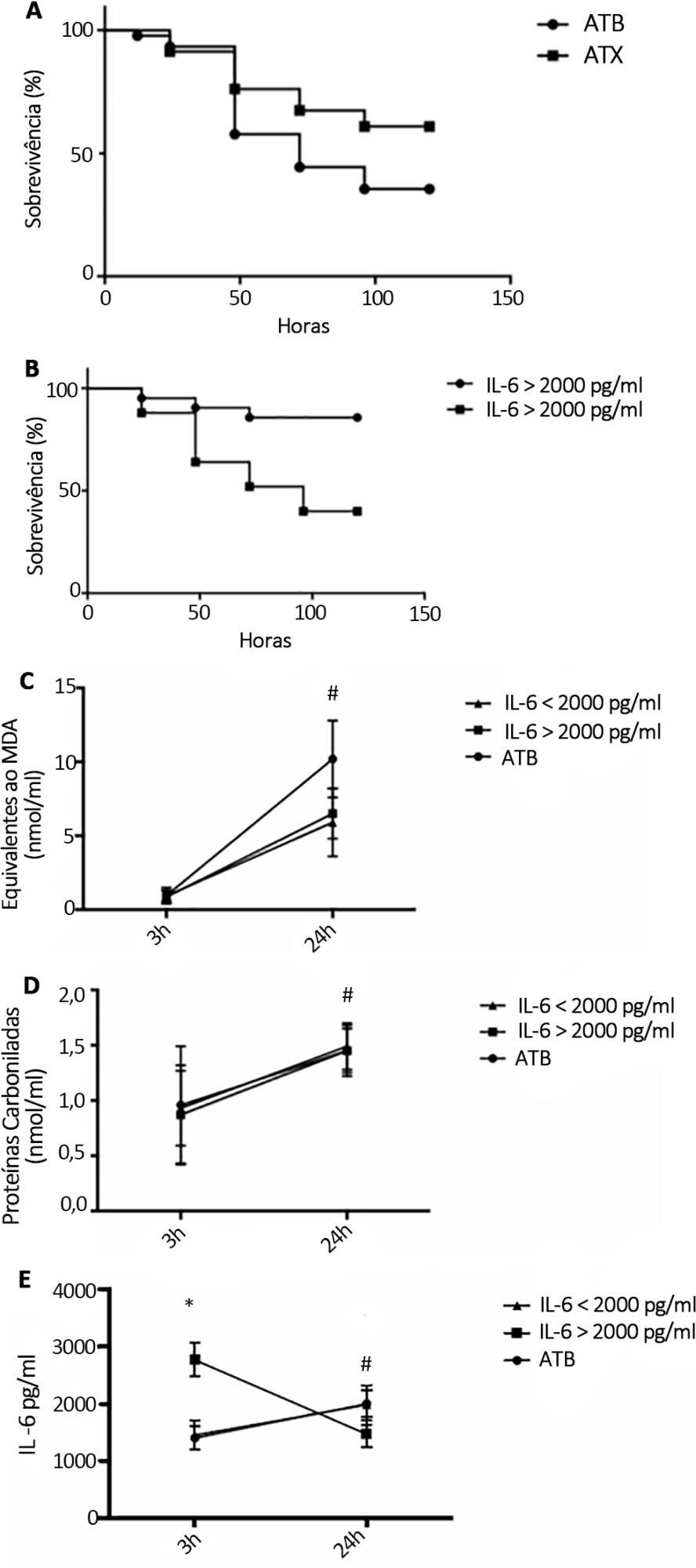
Rats were subjected to sepsis induced by cecal ligation and puncture. Animals were divided into two groups: those with high and low plasma levels of interleukin-6. Following stratification, N-acetylcysteine plus deferoxamine or saline was administered to animals starting 3 and 12 hours after surgery. N-Acetylcysteine plus deferoxamine or placebo was administered within 12 hours of meeting the inclusion criteria in hypotensive patients.
Results:
N-Acetylcysteine plus deferoxamine increased survival in the cecal ligation and puncture model when administered 3 and 12 hours after sepsis induction. When dividing animals that received antioxidants using plasma interleukin-6 levels, the protective effect was observed only in those animals with high IL-6 levels. The antioxidant effect of N-acetylcysteine + deferoxamine was similar in the two groups, but a significant decrease in plasma interleukin-6 levels was observed in the high-interleukin-6-level group. Compared with patients treated with antioxidants in the low-interleukin-6 subgroup, those in the high-interleukin-6 subgroup had a lower incidence of acute kidney injury but were not different in terms of acute kidney injury severity or intensive care unit mortality.
Conclusion:
Targeting antioxidant therapy to a high inflammatory phenotype would select a responsive population.
Views1Abstract
Original ArticleStratification to predict the response to antioxidant
Rev Bras Ter Intensiva. 2020;32(1):108-114
DOI 10.5935/0103-507X.20200016
- Cristiane Ritter,
- Larissa Constantino,
- Monique Michels ,
- Renata Casagrande Gonçalves,
- Cassiana Fraga,
- Danusa Damásio,
- Felipe Dal-Pizzol
Views1See moreABSTRACT
Objective:
To examine the effectiveness of stratification to identify and target antioxidant therapy for animal models of lethal sepsis and in patients who develop sustained hypotension.
Methods:
Rats were subjected to sepsis induced by cecal ligation and puncture. Animals were divided into two groups: those with high and low plasma levels of interleukin-6. Following stratification, N-acetylcysteine plus deferoxamine or saline was administered to animals starting 3 and 12 hours after surgery. N-Acetylcysteine plus deferoxamine or placebo was administered within 12 hours of meeting the inclusion criteria in hypotensive patients.
Results:
N-Acetylcysteine plus deferoxamine increased survival in the cecal ligation and puncture model when administered 3 and 12 hours after sepsis induction. When dividing animals that received antioxidants using plasma interleukin-6 levels, the protective effect was observed only in those animals with high IL-6 levels. The antioxidant effect of N-acetylcysteine + deferoxamine was similar in the two groups, but a significant decrease in plasma interleukin-6 levels was observed in the high-interleukin-6-level group. Compared with patients treated with antioxidants in the low-interleukin-6 subgroup, those in the high-interleukin-6 subgroup had a lower incidence of acute kidney injury but were not different in terms of acute kidney injury severity or intensive care unit mortality.
Conclusion:
Targeting antioxidant therapy to a high inflammatory phenotype would select a responsive population.
-
Review Article
Central venous minus arterial carbon dioxide pressure to arterial minus central venous oxygen content ratio as an indicator of tissue oxygenation: a narrative review
Rev Bras Ter Intensiva. 2020;32(1):115-122
Abstract
Review ArticleCentral venous minus arterial carbon dioxide pressure to arterial minus central venous oxygen content ratio as an indicator of tissue oxygenation: a narrative review
Rev Bras Ter Intensiva. 2020;32(1):115-122
DOI 10.5935/0103-507X.20200017
Views0See moreABSTRACT
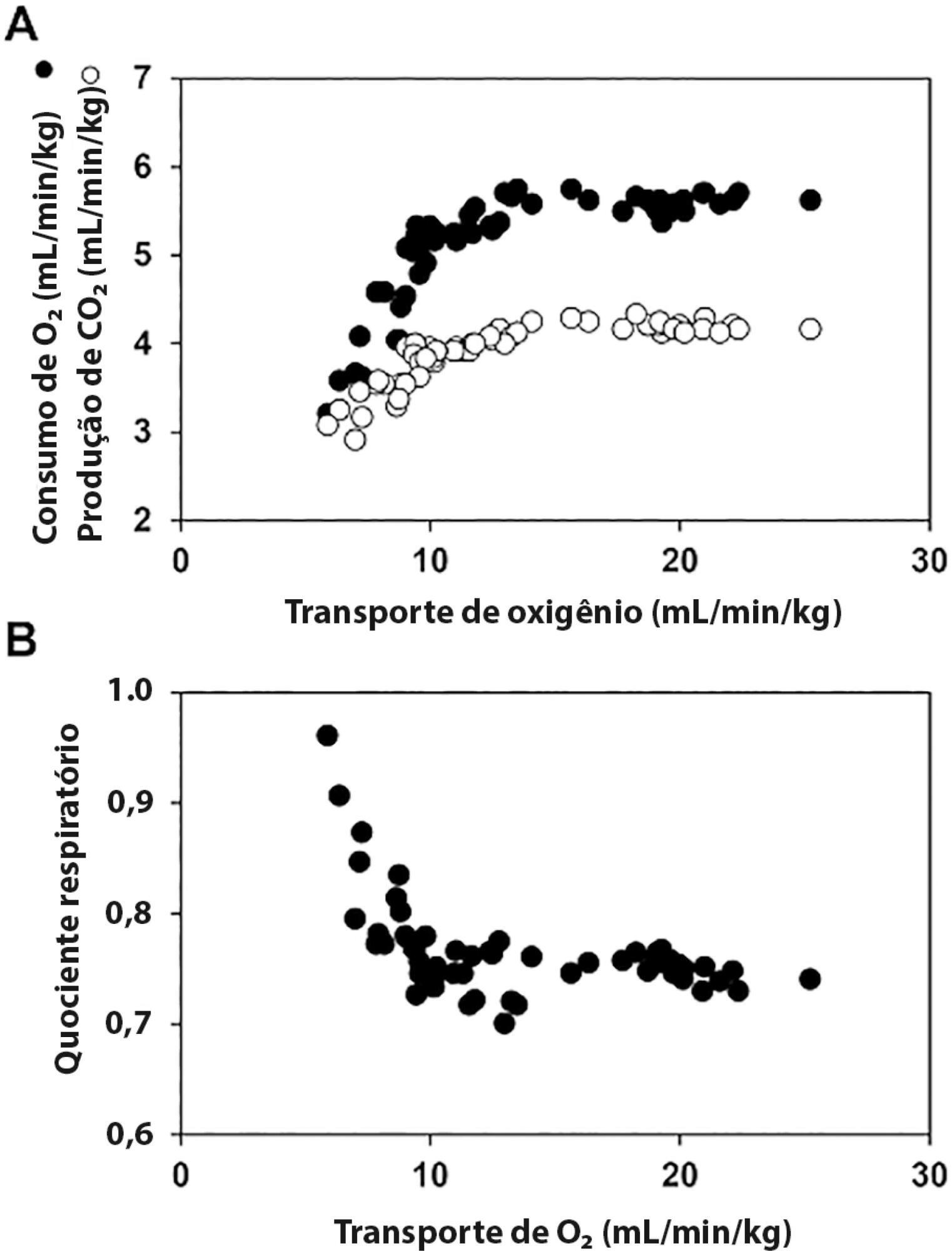
The central venous minus arterial carbon dioxide pressure to arterial minus central venous oxygen content ratio (Pcv-aCO2/Ca-cvO2) has been proposed as a surrogate for respiratory quotient and an indicator of tissue oxygenation. Some small observational studies have found that a Pcv-aCO2/Ca-cvO2 > 1.4 was associated with hyperlactatemia, oxygen supply dependency, and increased mortality. Moreover, Pcv-aCO2/Ca-cvO2 has been incorporated into algorithms for tissue oxygenation evaluation and resuscitation. However, the evidence for these recommendations is quite limited and of low quality. The goal of this narrative review was to analyze the methodological bases, the pathophysiologic foundations, and the experimental and clinical evidence supporting the use of Pcv-aCO2/Ca-cvO2 as a surrogate for respiratory quotient. Physiologically, the increase in respiratory quotient secondary to critical reductions in oxygen transport is a life-threatening and dramatic event. Nevertheless, this event is easily noticeable and probably does not require further monitoring. Since the beginning of anaerobic metabolism is indicated by the sudden increase in respiratory quotient and the normal range of respiratory quotient is wide, the use of a defined cutoff of 1.4 for Pcv-aCO2/Ca-cvO2 is meaningless. Experimental studies have shown that Pcv-aCO2/Ca-cvO2 is more dependent on factors that modify the dissociation of carbon dioxide from hemoglobin than on respiratory quotient and that respiratory quotient and Pcv-aCO2/Ca-cvO2 may have distinct behaviors. Studies performed in critically ill patients have shown controversial results regarding the ability of Pcv-aCO2/Ca-cvO2 to predict outcome, hyperlactatemia, microvascular abnormalities, and oxygen supply dependency. A randomized controlled trial also showed that Pcv-aCO2/Ca-cvO2 is useless as a goal of resuscitation. Pcv-aCO2/Ca-cvO2 should be carefully interpreted in critically ill patients.
Views0Abstract
Review ArticleCentral venous minus arterial carbon dioxide pressure to arterial minus central venous oxygen content ratio as an indicator of tissue oxygenation: a narrative review
Rev Bras Ter Intensiva. 2020;32(1):115-122
DOI 10.5935/0103-507X.20200017
Views0See moreABSTRACT
The central venous minus arterial carbon dioxide pressure to arterial minus central venous oxygen content ratio (Pcv-aCO2/Ca-cvO2) has been proposed as a surrogate for respiratory quotient and an indicator of tissue oxygenation. Some small observational studies have found that a Pcv-aCO2/Ca-cvO2 > 1.4 was associated with hyperlactatemia, oxygen supply dependency, and increased mortality. Moreover, Pcv-aCO2/Ca-cvO2 has been incorporated into algorithms for tissue oxygenation evaluation and resuscitation. However, the evidence for these recommendations is quite limited and of low quality. The goal of this narrative review was to analyze the methodological bases, the pathophysiologic foundations, and the experimental and clinical evidence supporting the use of Pcv-aCO2/Ca-cvO2 as a surrogate for respiratory quotient. Physiologically, the increase in respiratory quotient secondary to critical reductions in oxygen transport is a life-threatening and dramatic event. Nevertheless, this event is easily noticeable and probably does not require further monitoring. Since the beginning of anaerobic metabolism is indicated by the sudden increase in respiratory quotient and the normal range of respiratory quotient is wide, the use of a defined cutoff of 1.4 for Pcv-aCO2/Ca-cvO2 is meaningless. Experimental studies have shown that Pcv-aCO2/Ca-cvO2 is more dependent on factors that modify the dissociation of carbon dioxide from hemoglobin than on respiratory quotient and that respiratory quotient and Pcv-aCO2/Ca-cvO2 may have distinct behaviors. Studies performed in critically ill patients have shown controversial results regarding the ability of Pcv-aCO2/Ca-cvO2 to predict outcome, hyperlactatemia, microvascular abnormalities, and oxygen supply dependency. A randomized controlled trial also showed that Pcv-aCO2/Ca-cvO2 is useless as a goal of resuscitation. Pcv-aCO2/Ca-cvO2 should be carefully interpreted in critically ill patients.
-
Review Article
Clinical prediction models for acute kidney injury
Rev Bras Ter Intensiva. 2020;32(1):123-132
Abstract
Review ArticleClinical prediction models for acute kidney injury
Rev Bras Ter Intensiva. 2020;32(1):123-132
DOI 10.5935/0103-507X.20200018
Views2See moreABSTRACT
Objective:
To report on the currently available prediction models for the development of acute kidney injury in heterogeneous adult intensive care units.
Methods:
A systematic review of clinical prediction models for acute kidney injury in adult intensive care unit populations was carried out. PubMed® was searched for publications reporting on the development of a novel prediction model, validation of an established model, or impact of an existing prediction model for early acute kidney injury diagnosis in intensive care units.
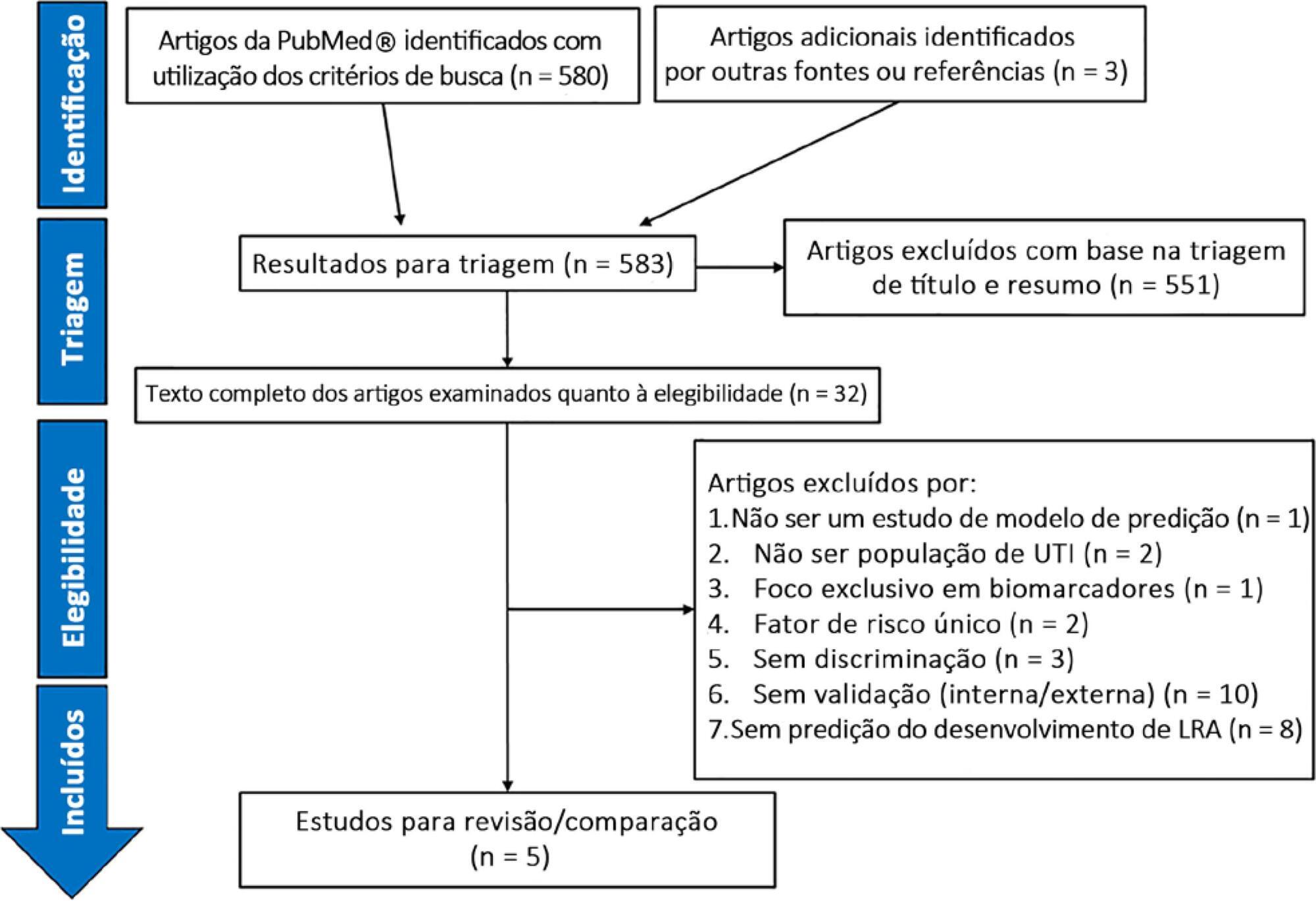
Results:
We screened 583 potentially relevant articles. Among the 32 remaining articles in the first selection, only 5 met the inclusion criteria. The nonstandardized adaptations that were made to define baseline serum creatinine when the preadmission value was missing led to heterogeneous definitions of the outcome. Commonly included predictors were sepsis, age, and serum creatinine level. The final models included between 5 and 19 risk factors. The areas under the Receiver Operating Characteristic curves to predict acute kidney injury development in the internal validation cohorts ranged from 0.78 to 0.88. Only two studies were externally validated.
Conclusion:
Clinical prediction models for acute kidney injury can help in applying more timely preventive interventions to the right patients. However, in intensive care unit populations, few models have been externally validated. In addition, heterogeneous definitions for acute kidney injury and evaluation criteria and the lack of impact analysis hamper a thorough comparison of existing models. Future research is needed to validate the established models and to analyze their clinical impact before they can be applied in clinical practice.
Views2Abstract
Review ArticleClinical prediction models for acute kidney injury
Rev Bras Ter Intensiva. 2020;32(1):123-132
DOI 10.5935/0103-507X.20200018
Views2See moreABSTRACT
Objective:
To report on the currently available prediction models for the development of acute kidney injury in heterogeneous adult intensive care units.
Methods:
A systematic review of clinical prediction models for acute kidney injury in adult intensive care unit populations was carried out. PubMed® was searched for publications reporting on the development of a novel prediction model, validation of an established model, or impact of an existing prediction model for early acute kidney injury diagnosis in intensive care units.
Results:
We screened 583 potentially relevant articles. Among the 32 remaining articles in the first selection, only 5 met the inclusion criteria. The nonstandardized adaptations that were made to define baseline serum creatinine when the preadmission value was missing led to heterogeneous definitions of the outcome. Commonly included predictors were sepsis, age, and serum creatinine level. The final models included between 5 and 19 risk factors. The areas under the Receiver Operating Characteristic curves to predict acute kidney injury development in the internal validation cohorts ranged from 0.78 to 0.88. Only two studies were externally validated.
Conclusion:
Clinical prediction models for acute kidney injury can help in applying more timely preventive interventions to the right patients. However, in intensive care unit populations, few models have been externally validated. In addition, heterogeneous definitions for acute kidney injury and evaluation criteria and the lack of impact analysis hamper a thorough comparison of existing models. Future research is needed to validate the established models and to analyze their clinical impact before they can be applied in clinical practice.
-
Review Article
Administration of enteral nutrition in the prone position, gastric residual volume and other clinical outcomes in critically ill patients: a systematic review
Rev Bras Ter Intensiva. 2020;32(1):133-142
Abstract
Review ArticleAdministration of enteral nutrition in the prone position, gastric residual volume and other clinical outcomes in critically ill patients: a systematic review
Rev Bras Ter Intensiva. 2020;32(1):133-142
DOI 10.5935/0103-507X.20200019
Views0ABSTRACT
This systematic review of longitudinal studies aimed to evaluate the effect of enteral feeding of critically ill adult and pediatric patients in the prone position on gastric residual volume and other clinical outcomes. A literature search was conducted in the databases PubMed, Scopus and Embase using terms related to population and intervention. Two independent reviewers analyzed the titles and abstracts, and data collection was performed using a standardized form. Discrepancies were resolved by a third reviewer. The methodological quality of the studies was evaluated considering the potential for systematic errors, and the data were qualitatively analyzed. Four studies with adult patients and one with preterm patients were included. The gastric residual volume was evaluated as the main outcome: three studies did not show differences in the gastric residual volume between the prone and supine positions (p > 0.05), while one study showed a higher gastric residual volume during enteral feeding in the prone position (27.6mL versus 10.6mL; p < 0.05), and another group observed a greater gastric residual volume in the supine position (reduction of the gastric residual volume by 23.3% in the supine position versus 43.9% in the prone position; p < 0.01). Two studies evaluated the frequency of vomiting; one study found that it was higher in the prone position (30 versus 26 episodes; p < 0.001), while the other study found no significant difference (p > 0.05). The incidence of aspiration pneumonia and death were evaluated in one study, with no difference between groups (p > 0.05). The literature on the administration of enteral feeding in the prone position in critically ill patients is sparse and of limited quality, and the results regarding gastric residual volume are contradictory. Observational studies with appropriate sample sizes should be conducted to support conclusions on the subject.
Keywords:Critical illnessenteral nutritionGastrointestinal contentsnutrition therapyPneumoniaProne positionSee moreViews0Abstract
Review ArticleAdministration of enteral nutrition in the prone position, gastric residual volume and other clinical outcomes in critically ill patients: a systematic review
Rev Bras Ter Intensiva. 2020;32(1):133-142
DOI 10.5935/0103-507X.20200019
Views0ABSTRACT
This systematic review of longitudinal studies aimed to evaluate the effect of enteral feeding of critically ill adult and pediatric patients in the prone position on gastric residual volume and other clinical outcomes. A literature search was conducted in the databases PubMed, Scopus and Embase using terms related to population and intervention. Two independent reviewers analyzed the titles and abstracts, and data collection was performed using a standardized form. Discrepancies were resolved by a third reviewer. The methodological quality of the studies was evaluated considering the potential for systematic errors, and the data were qualitatively analyzed. Four studies with adult patients and one with preterm patients were included. The gastric residual volume was evaluated as the main outcome: three studies did not show differences in the gastric residual volume between the prone and supine positions (p > 0.05), while one study showed a higher gastric residual volume during enteral feeding in the prone position (27.6mL versus 10.6mL; p < 0.05), and another group observed a greater gastric residual volume in the supine position (reduction of the gastric residual volume by 23.3% in the supine position versus 43.9% in the prone position; p < 0.01). Two studies evaluated the frequency of vomiting; one study found that it was higher in the prone position (30 versus 26 episodes; p < 0.001), while the other study found no significant difference (p > 0.05). The incidence of aspiration pneumonia and death were evaluated in one study, with no difference between groups (p > 0.05). The literature on the administration of enteral feeding in the prone position in critically ill patients is sparse and of limited quality, and the results regarding gastric residual volume are contradictory. Observational studies with appropriate sample sizes should be conducted to support conclusions on the subject.
Keywords:Critical illnessenteral nutritionGastrointestinal contentsnutrition therapyPneumoniaProne positionSee more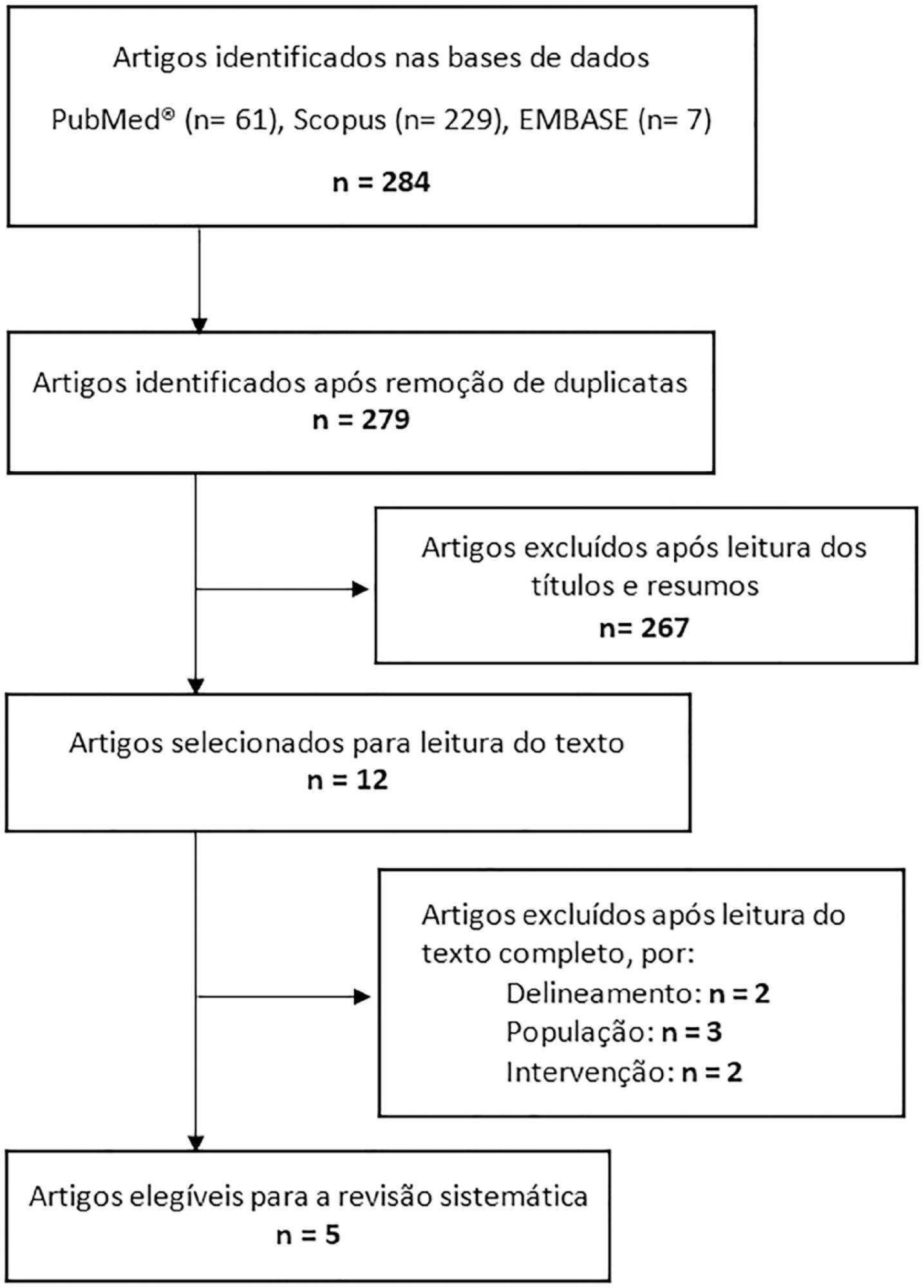
-
Case Report
Extracorporeal carbon dioxide removal with continuous renal replacement therapy. Case description and literature review
Rev Bras Ter Intensiva. 2020;32(1):143-148
Abstract
Case ReportExtracorporeal carbon dioxide removal with continuous renal replacement therapy. Case description and literature review
Rev Bras Ter Intensiva. 2020;32(1):143-148
DOI 10.5935/0103-507X.20200020
Views0See moreABSTRACT
In recent years and due, in part, to technological advances, the use of extracorporeal carbon dioxide removal systems paired with the use of extracorporeal membrane oxygenation has resurfaced. However, studies are lacking that establish its indications and evidence to support its use. These systems efficiently eliminate carbon dioxide in patients with hypercapnic respiratory failure using small-bore cannula, usually double-lumen cannula with a small membrane lung surface area. Currently, we have several systems with different types of membranes and sizes. Pump-driven veno-venous systems generate fewer complications than do arteriovenous systems. Both require systemic anticoagulation. The “lung-kidney” support system, by combining a removal system with hemofiltration, simultaneously eliminates carbon dioxide and performs continuous extrarenal replacement. We describe our initial experience with a combined system for extracorporeal carbon dioxide removal-continuous extrarenal replacement in a lung transplant patients with hypercapnic respiratory failure, barotrauma and associated acute renal failure. The most important technical aspects, the effectiveness of the system for the elimination of carbon dioxide and a review of the literature are described.
Views0Abstract
Case ReportExtracorporeal carbon dioxide removal with continuous renal replacement therapy. Case description and literature review
Rev Bras Ter Intensiva. 2020;32(1):143-148
DOI 10.5935/0103-507X.20200020
Views0See moreABSTRACT
In recent years and due, in part, to technological advances, the use of extracorporeal carbon dioxide removal systems paired with the use of extracorporeal membrane oxygenation has resurfaced. However, studies are lacking that establish its indications and evidence to support its use. These systems efficiently eliminate carbon dioxide in patients with hypercapnic respiratory failure using small-bore cannula, usually double-lumen cannula with a small membrane lung surface area. Currently, we have several systems with different types of membranes and sizes. Pump-driven veno-venous systems generate fewer complications than do arteriovenous systems. Both require systemic anticoagulation. The “lung-kidney” support system, by combining a removal system with hemofiltration, simultaneously eliminates carbon dioxide and performs continuous extrarenal replacement. We describe our initial experience with a combined system for extracorporeal carbon dioxide removal-continuous extrarenal replacement in a lung transplant patients with hypercapnic respiratory failure, barotrauma and associated acute renal failure. The most important technical aspects, the effectiveness of the system for the elimination of carbon dioxide and a review of the literature are described.
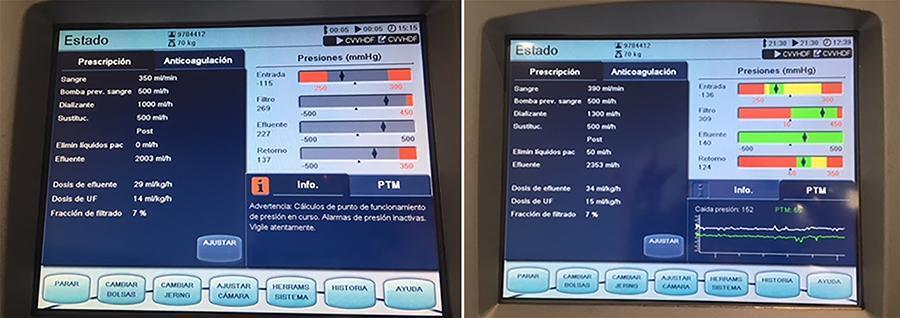
-
Case Report
Kounis syndrome. Apropos of a clinical case
Rev Bras Ter Intensiva. 2020;32(1):149-152
Abstract
Case ReportKounis syndrome. Apropos of a clinical case
Rev Bras Ter Intensiva. 2020;32(1):149-152
DOI 10.5935/0103-507X.20200021
- Pedro Duarte ,
- Joana Costa,
- Cátia Serena,
- Carla Almeida,
- Sandra Gouveia,
- César Lourenço ,
- Humberto Costa,
- Clara Paiva
Views0See moreABSTRACT
Kounis syndrome, while an acute coronary syndrome, occurs in the context of a hypersensitivity reaction, allergies, or anaphylaxis and is subdivided into three types: coronary spasm in normal arteries, instability of plaques in atherosclerotic coronary arteries, and thrombosis of coronary stents. Herein, the case of a 73-year-old patient who, after administration of amoxicillin/clavulanic acid, went into cardiorespiratory arrest with evidence of ST-T segment elevation on electrocardiogram is reported. Coronarography revealed no obstructive lesions, and spontaneous resolution of electrocardiographic abnormalities was observed. A review of anamnesis with the family revealed a previous allergy to penicillin. The tryptase dosage was strongly positive. Kounis syndrome type 2 was diagnosed, and the clinical outcome was good.
Views0Abstract
Case ReportKounis syndrome. Apropos of a clinical case
Rev Bras Ter Intensiva. 2020;32(1):149-152
DOI 10.5935/0103-507X.20200021
- Pedro Duarte ,
- Joana Costa,
- Cátia Serena,
- Carla Almeida,
- Sandra Gouveia,
- César Lourenço ,
- Humberto Costa,
- Clara Paiva
Views0See moreABSTRACT
Kounis syndrome, while an acute coronary syndrome, occurs in the context of a hypersensitivity reaction, allergies, or anaphylaxis and is subdivided into three types: coronary spasm in normal arteries, instability of plaques in atherosclerotic coronary arteries, and thrombosis of coronary stents. Herein, the case of a 73-year-old patient who, after administration of amoxicillin/clavulanic acid, went into cardiorespiratory arrest with evidence of ST-T segment elevation on electrocardiogram is reported. Coronarography revealed no obstructive lesions, and spontaneous resolution of electrocardiographic abnormalities was observed. A review of anamnesis with the family revealed a previous allergy to penicillin. The tryptase dosage was strongly positive. Kounis syndrome type 2 was diagnosed, and the clinical outcome was good.
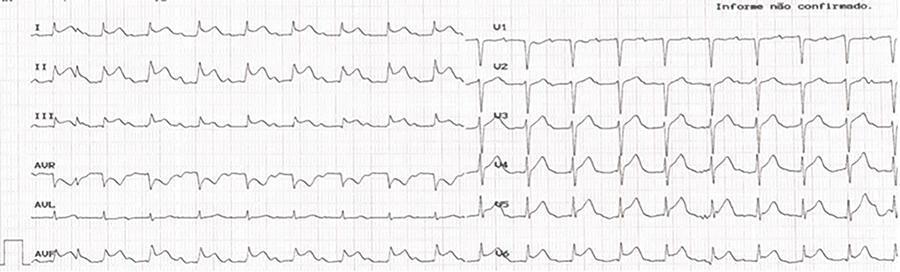
- Pedro Duarte
-
Letter to the Editor
Dorsal radial artery catheterization for invasive blood pressure monitoring
- Roosevelt Santos Nunes ,
- Camila Mussolin Tamaki,
- Heloisa Helena Robles Penha,
- Julia Carvalho Mafra Terra,
- Geraldo Luiz de Figueiredo, [ … ],
- Gil Cezar Alkmin Teixeira
Abstract
Letter to the EditorDorsal radial artery catheterization for invasive blood pressure monitoring
Rev Bras Ter Intensiva. 2020;32(1):153-155
DOI 10.5935/0103-507X.20200022
- Roosevelt Santos Nunes ,
- Camila Mussolin Tamaki,
- Heloisa Helena Robles Penha,
- Julia Carvalho Mafra Terra,
- Geraldo Luiz de Figueiredo,
- Gil Cezar Alkmin Teixeira
Views0To the EditorArterial catheterization is a common procedure in intensive care units, with the primary purposes of continuous blood pressure monitoring and frequent blood sample collection. Obtaining an arterial line is also critical for the use of minimally invasive hemodynamic monitoring.The radial artery is often the first choice for the placement of an arterial catheter, […]See moreViews0Abstract
Letter to the EditorDorsal radial artery catheterization for invasive blood pressure monitoring
Rev Bras Ter Intensiva. 2020;32(1):153-155
DOI 10.5935/0103-507X.20200022
- Roosevelt Santos Nunes ,
- Camila Mussolin Tamaki,
- Heloisa Helena Robles Penha,
- Julia Carvalho Mafra Terra,
- Geraldo Luiz de Figueiredo,
- Gil Cezar Alkmin Teixeira
Views0To the EditorArterial catheterization is a common procedure in intensive care units, with the primary purposes of continuous blood pressure monitoring and frequent blood sample collection. Obtaining an arterial line is also critical for the use of minimally invasive hemodynamic monitoring.The radial artery is often the first choice for the placement of an arterial catheter, […]See more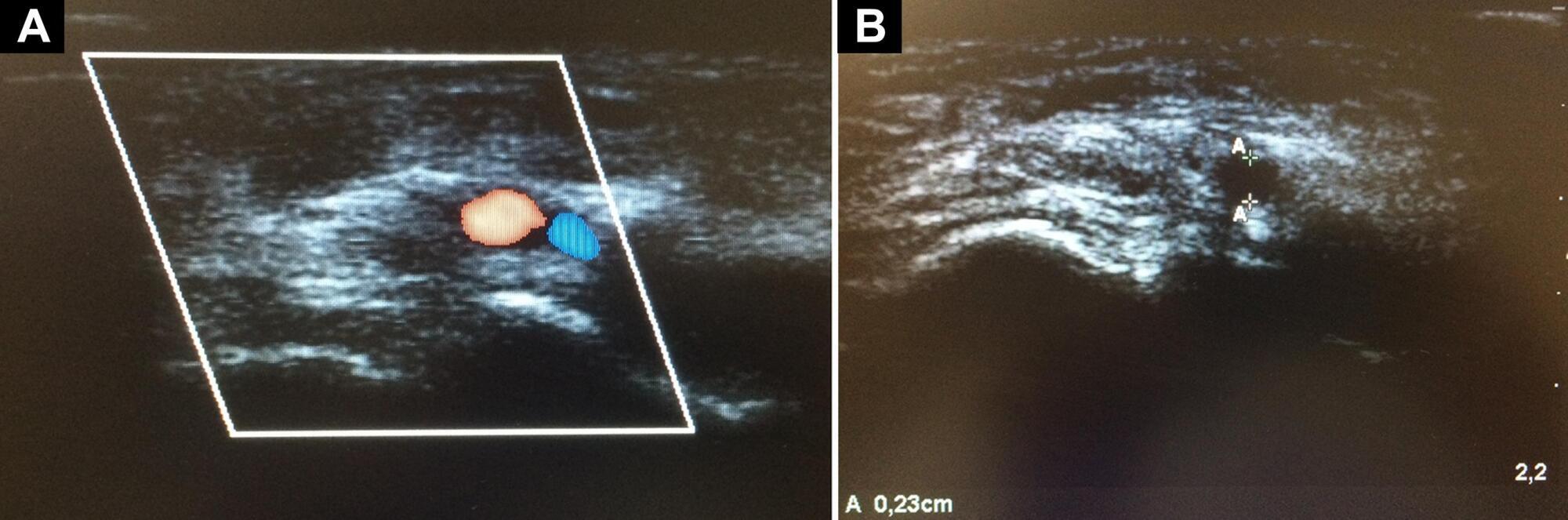
- Roosevelt Santos Nunes
-
Letter to the Editor
Variability in the rectus femoris muscle area and its association with clinical outcomes in critically ill patients: a prospective cohort study
Rev Bras Ter Intensiva. 2020;32(1):156-158
Abstract
Letter to the EditorVariability in the rectus femoris muscle area and its association with clinical outcomes in critically ill patients: a prospective cohort study
Rev Bras Ter Intensiva. 2020;32(1):156-158
DOI 10.5935/0103-507X.20200023
Views0To the Editor, Muscle weakness is a common complication in critically ill patients, with loss of muscle mass during hospitalization in the intensive care unit (ICU), which is enhanced by the magnitude of organ failure and is associated with long-term morbidity.(,) Rectus femoris muscle (RFM) ultrasound has emerged as a practical, easily performed and applied […]See moreViews0Abstract
Letter to the EditorVariability in the rectus femoris muscle area and its association with clinical outcomes in critically ill patients: a prospective cohort study
Rev Bras Ter Intensiva. 2020;32(1):156-158
DOI 10.5935/0103-507X.20200023
Views0To the Editor, Muscle weakness is a common complication in critically ill patients, with loss of muscle mass during hospitalization in the intensive care unit (ICU), which is enhanced by the magnitude of organ failure and is associated with long-term morbidity.(,) Rectus femoris muscle (RFM) ultrasound has emerged as a practical, easily performed and applied […]See more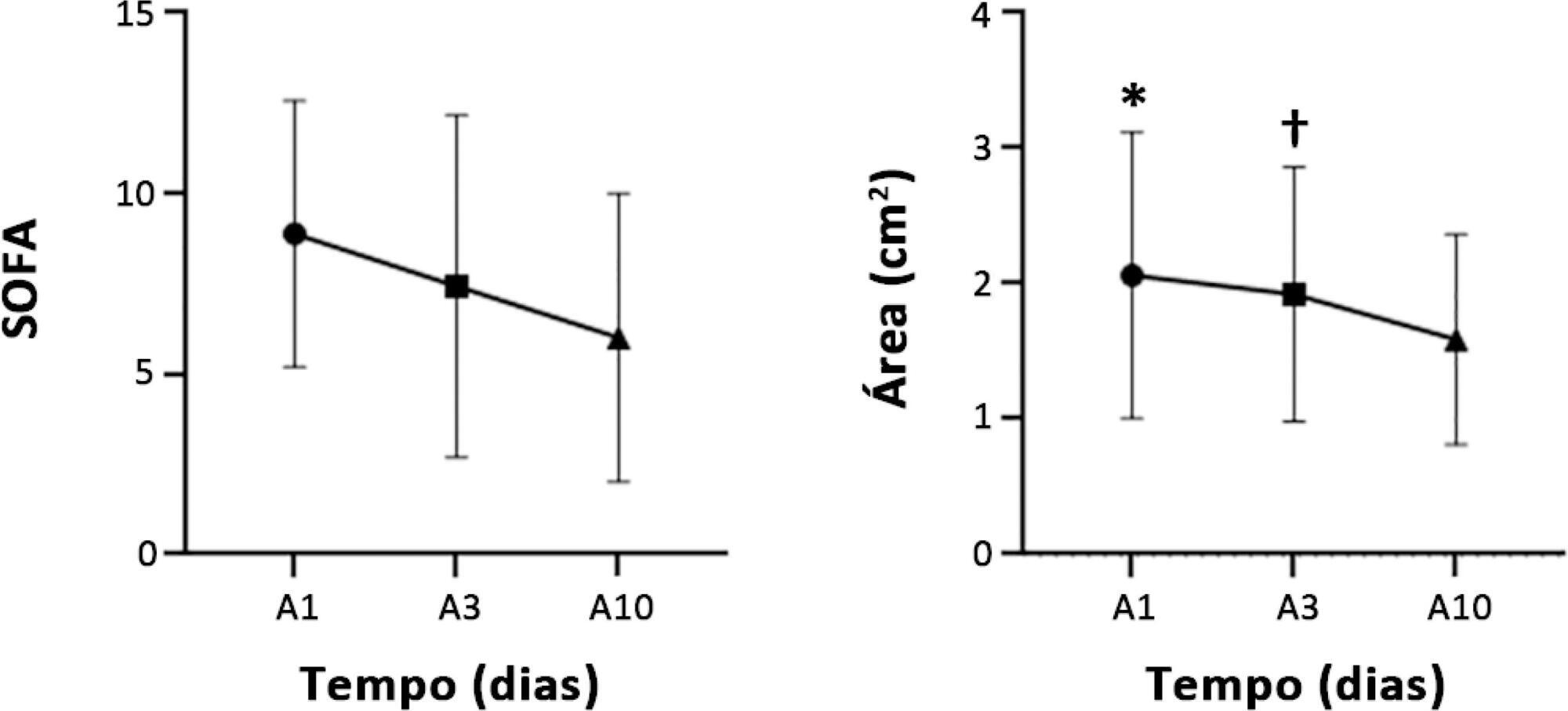
-
Letter to the Editor
Packed red blood cell transfusion trigger in the intensive care unit of a university hospital
- Maria Paulina Viana Miquilino ,
- Carlos Eduardo Cardoso,
- Victória Castello Branco Fernandes Martins,
- Sandra Mara Silva de Almeida,
- Aparecida Carmem de Oliveira, [ … ],
- Gerson Luiz de Macedo
Abstract
Letter to the EditorPacked red blood cell transfusion trigger in the intensive care unit of a university hospital
Rev Bras Ter Intensiva. 2020;32(1):159-160
DOI 10.5935/0103-507X.20200024
- Maria Paulina Viana Miquilino ,
- Carlos Eduardo Cardoso,
- Victória Castello Branco Fernandes Martins,
- Sandra Mara Silva de Almeida,
- Aparecida Carmem de Oliveira,
- Gerson Luiz de Macedo
Views0To the Editor,Anemia is a pathological condition with high prevalence and great importance in intensive care units (ICUs) because it increases mortality in critically ill patients. For this reason, the transfusion of packed red blood cells (PRBCs) is a routinely adopted practice, but the safe pre-transfusion hemoglobin (Hb) value indicative of transfusion is still discussed […]See moreViews0Abstract
Letter to the EditorPacked red blood cell transfusion trigger in the intensive care unit of a university hospital
Rev Bras Ter Intensiva. 2020;32(1):159-160
DOI 10.5935/0103-507X.20200024
- Maria Paulina Viana Miquilino ,
- Carlos Eduardo Cardoso,
- Victória Castello Branco Fernandes Martins,
- Sandra Mara Silva de Almeida,
- Aparecida Carmem de Oliveira,
- Gerson Luiz de Macedo
Views0To the Editor,Anemia is a pathological condition with high prevalence and great importance in intensive care units (ICUs) because it increases mortality in critically ill patients. For this reason, the transfusion of packed red blood cells (PRBCs) is a routinely adopted practice, but the safe pre-transfusion hemoglobin (Hb) value indicative of transfusion is still discussed […]See more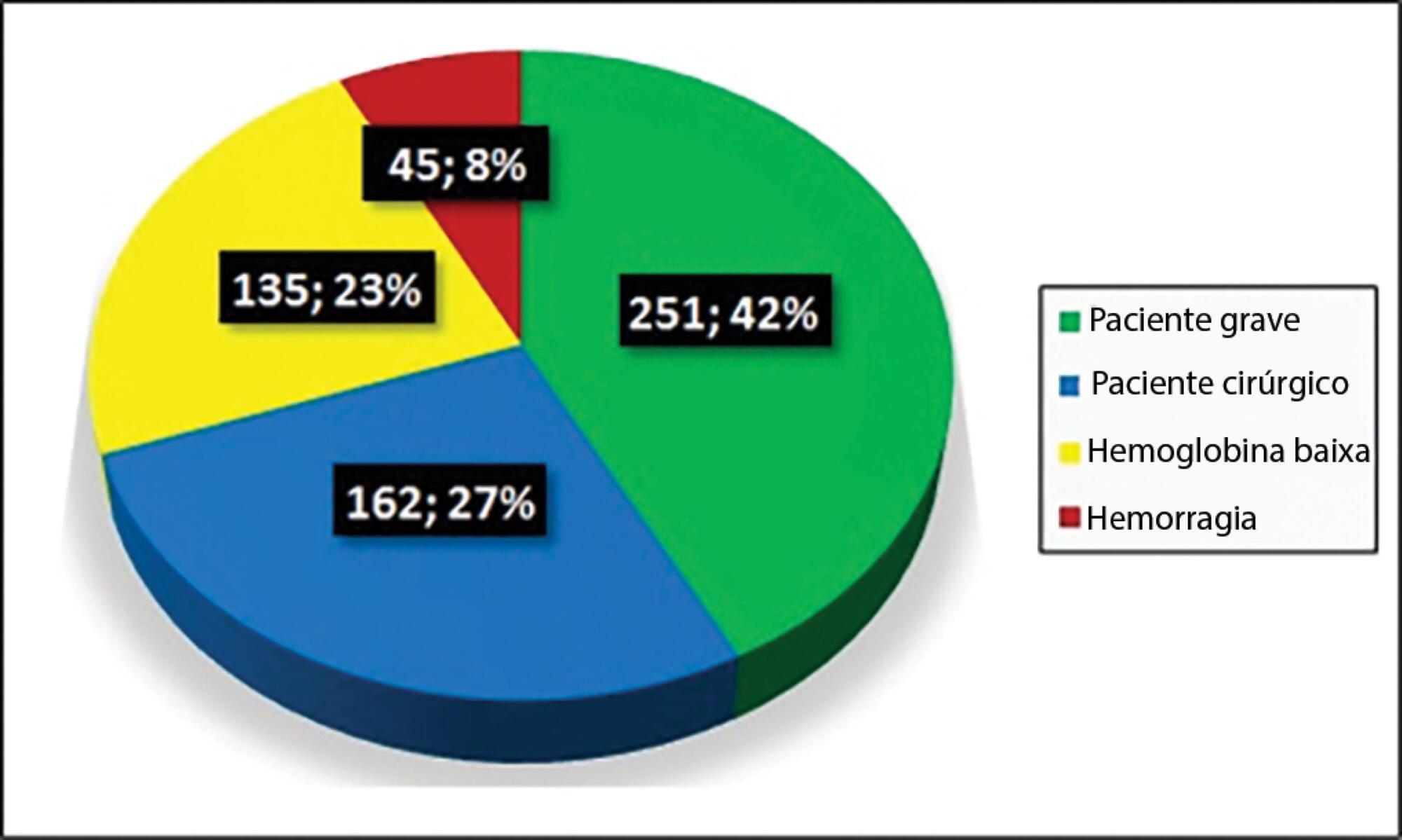
- Maria Paulina Viana Miquilino
-
Letter to the Editor
Brain abscess and odontogenic infection
- Renata Lanzoni de Oliveira,
- Regina Maria Raffaele,
- Mario Eduardo Baldo,
- Ellen Cristina Gaetti Jardim
Abstract
Letter to the EditorBrain abscess and odontogenic infection
Rev Bras Ter Intensiva. 2020;32(1):161-162
DOI 10.5935/0103-507X.20200025
- Renata Lanzoni de Oliveira,
- Regina Maria Raffaele,
- Mario Eduardo Baldo,
- Ellen Cristina Gaetti Jardim
Views0To the Editor, Odontogenic infections are typically limited to the dental alveolus or periodontium. However, when untreated, they can spread through fascial spaces, leading to more serious infections such as cavernous sinus thrombosis, airway obstruction, mediastinitis, endocarditis and brain abscess.() This is explained by the proximity of the upper roots to the maxillary sinus, which […]See moreViews0Abstract
Letter to the EditorBrain abscess and odontogenic infection
Rev Bras Ter Intensiva. 2020;32(1):161-162
DOI 10.5935/0103-507X.20200025
- Renata Lanzoni de Oliveira,
- Regina Maria Raffaele,
- Mario Eduardo Baldo,
- Ellen Cristina Gaetti Jardim
Views0To the Editor, Odontogenic infections are typically limited to the dental alveolus or periodontium. However, when untreated, they can spread through fascial spaces, leading to more serious infections such as cavernous sinus thrombosis, airway obstruction, mediastinitis, endocarditis and brain abscess.() This is explained by the proximity of the upper roots to the maxillary sinus, which […]See more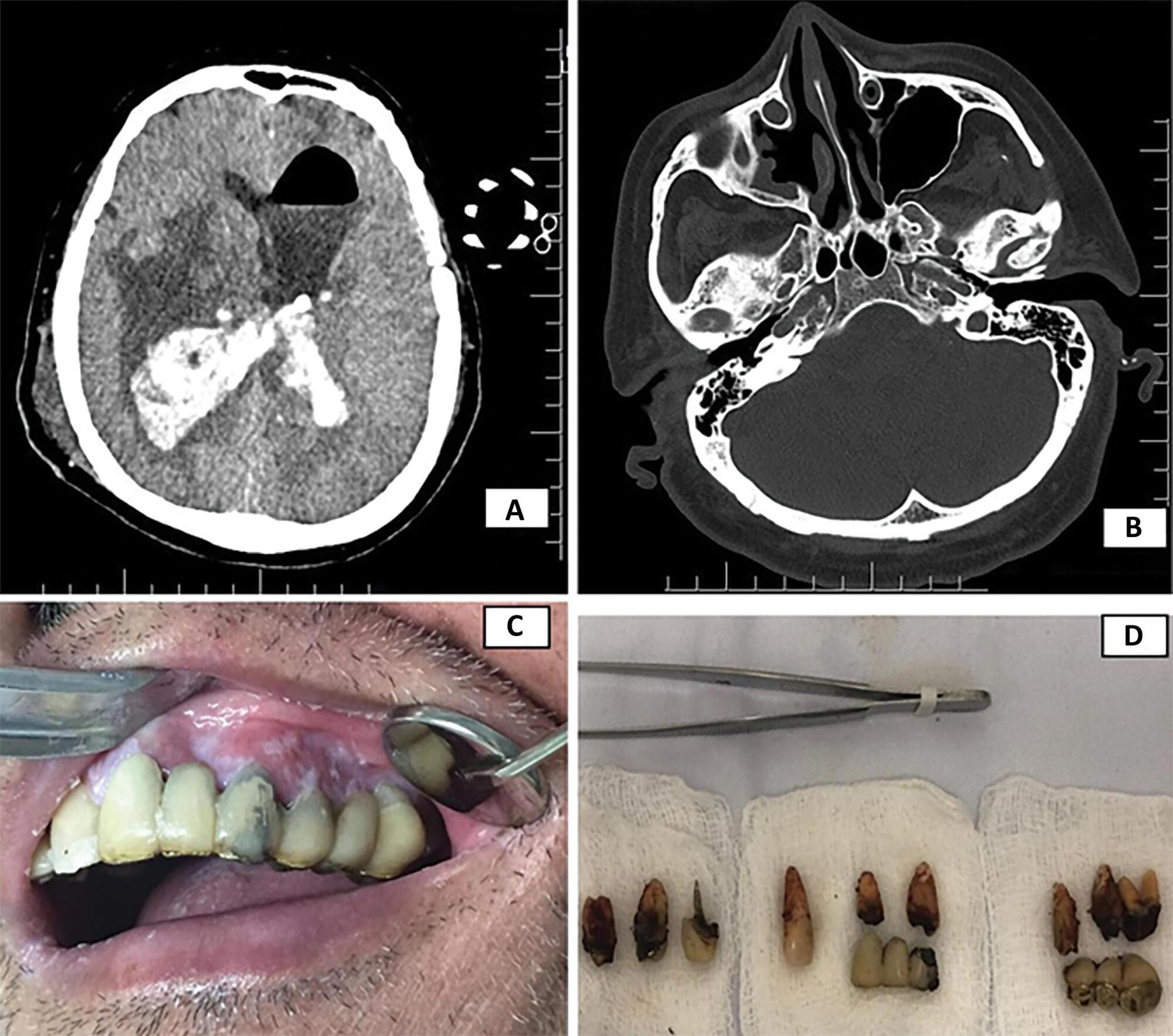
-
Letter to the Editor
To: Efficacy and safety of high-flow nasal cannula oxygen therapy in moderate acute hypercapnic respiratory failure
Rev Bras Ter Intensiva. 2020;32(1):163-164
Abstract
Letter to the EditorTo: Efficacy and safety of high-flow nasal cannula oxygen therapy in moderate acute hypercapnic respiratory failure
Rev Bras Ter Intensiva. 2020;32(1):163-164
DOI 10.5935/0103-507X.20200026
Views0To the Editor, We read with great interest the article “Efficacy and safety of high-flow nasal cannula oxygen therapy in moderate acute hypercapnic respiratory failure” by Yuste et al., where the use of high-flow nasal cannula (HFNC) is evaluated in patients with moderate hypercapnic respiratory failure (HRF).() We complement the authors for their exciting work; […]See moreViews0Abstract
Letter to the EditorTo: Efficacy and safety of high-flow nasal cannula oxygen therapy in moderate acute hypercapnic respiratory failure
Rev Bras Ter Intensiva. 2020;32(1):163-164
DOI 10.5935/0103-507X.20200026
Views0To the Editor, We read with great interest the article “Efficacy and safety of high-flow nasal cannula oxygen therapy in moderate acute hypercapnic respiratory failure” by Yuste et al., where the use of high-flow nasal cannula (HFNC) is evaluated in patients with moderate hypercapnic respiratory failure (HRF).() We complement the authors for their exciting work; […]See more -
Erratum
Erratum
Rev Bras Ter Intensiva. 2020;32(1):165-165
Abstract
ErratumErratum
Rev Bras Ter Intensiva. 2020;32(1):165-165
DOI 10.5935/0103-507X.20200027
Views1In the article Ventilator-associated tracheobronchitis: an update, with DOI number: 10.5935/0103-507X.20190079, published in the journal Revista Brasileira de Terapia Intensiva, 31(4):541-7, on page 541:Where it read:[…]See moreViews1Abstract
ErratumErratum
Rev Bras Ter Intensiva. 2020;32(1):165-165
DOI 10.5935/0103-507X.20200027
Views1In the article Ventilator-associated tracheobronchitis: an update, with DOI number: 10.5935/0103-507X.20190079, published in the journal Revista Brasileira de Terapia Intensiva, 31(4):541-7, on page 541:Where it read:[…]See more
Volume Articles - Critical Care Science (CCS)
