Acute coronary syndrome Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2020;32(1):149-152
DOI 10.5935/0103-507X.20200021
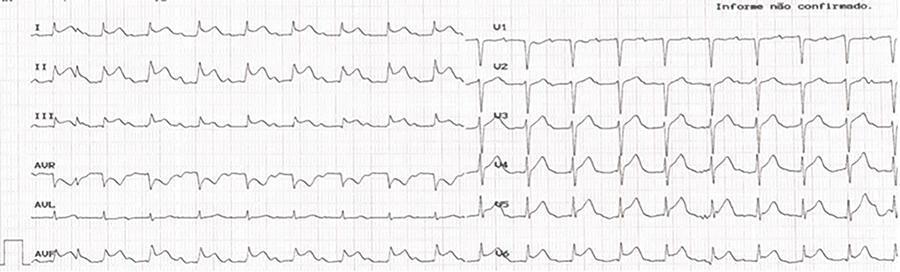
Kounis syndrome, while an acute coronary syndrome, occurs in the context of a hypersensitivity reaction, allergies, or anaphylaxis and is subdivided into three types: coronary spasm in normal arteries, instability of plaques in atherosclerotic coronary arteries, and thrombosis of coronary stents. Herein, the case of a 73-year-old patient who, after administration of amoxicillin/clavulanic acid, went into cardiorespiratory arrest with evidence of ST-T segment elevation on electrocardiogram is reported. Coronarography revealed no obstructive lesions, and spontaneous resolution of electrocardiographic abnormalities was observed. A review of anamnesis with the family revealed a previous allergy to penicillin. The tryptase dosage was strongly positive. Kounis syndrome type 2 was diagnosed, and the clinical outcome was good.
Abstract
Rev Bras Ter Intensiva. 2020;32(1):149-152
DOI 10.5935/0103-507X.20200021
Kounis syndrome, while an acute coronary syndrome, occurs in the context of a hypersensitivity reaction, allergies, or anaphylaxis and is subdivided into three types: coronary spasm in normal arteries, instability of plaques in atherosclerotic coronary arteries, and thrombosis of coronary stents. Herein, the case of a 73-year-old patient who, after administration of amoxicillin/clavulanic acid, went into cardiorespiratory arrest with evidence of ST-T segment elevation on electrocardiogram is reported. Coronarography revealed no obstructive lesions, and spontaneous resolution of electrocardiographic abnormalities was observed. A review of anamnesis with the family revealed a previous allergy to penicillin. The tryptase dosage was strongly positive. Kounis syndrome type 2 was diagnosed, and the clinical outcome was good.
Abstract
Rev Bras Ter Intensiva. 2016;28(4):405-412
DOI 10.5935/0103-507X.20160065
To compare patients without previously diagnosed cardiovascular risk factors) and patients with one or more risk factors admitted with acute coronary syndrome.
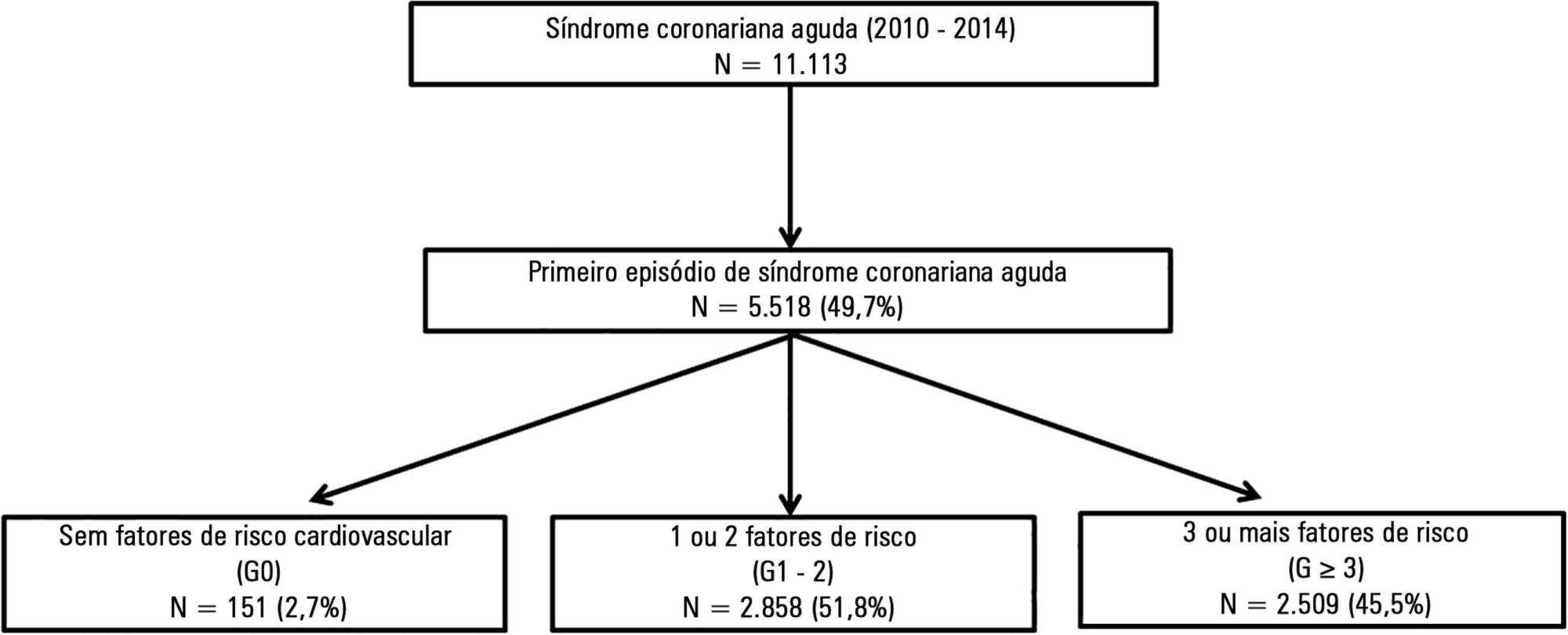
This was a retrospective analysis of patients admitted with first episode of acute coronary syndrome without previous heart disease, who were included in a national acute coronary syndrome registry. The patients were divided according to the number of risk factors, as follows: 0 risk factor (G0), 1 or 2 risk factors (G1 - 2) and 3 or more risk factors (G ≥ 3). Comparative analysis was performed between the three groups, and independent predictors of cardiac arrest and death were studied.
A total of 5,518 patients were studied, of which 72.2% were male and the mean age was 64 ± 14 years. G0 had a greater incidence of ST-segment elevation myocardial infarction, with the left anterior descending artery being the most frequently involved vessel, and a lower prevalence of multivessel disease. Even though G0 had a lower Killip class (96% in Killip I; p < 0.001) and higher ejection fraction (G0 56 ± 10% versus G1 - 2 and G ≥ 3 53 ± 12%; p = 0.024) on admission, there was a significant higher incidence of cardiac arrest. Multivariate analysis identified the absence of risk factors as an independent predictor of cardiac arrest (OR 2.78; p = 0.019). Hospital mortality was slightly higher in G0, although this difference was not significant. By Cox regression analysis, the number of risk factors was found not to be associated with mortality. Predictors of death at 1 year follow up included age (OR 1.05; p < 0.001), ST-segment elevation myocardial infarction (OR 1.94; p = 0.003) and ejection fraction < 50% (OR 2.34; p < 0.001).
Even though the group without risk factors was composed of younger patients with fewer comorbidities, better left ventricular function and less extensive coronary disease, the absence of risk factors was an independent predictor of cardiac arrest.
Abstract
Rev Bras Ter Intensiva. 2016;28(4):405-412
DOI 10.5935/0103-507X.20160065
To compare patients without previously diagnosed cardiovascular risk factors) and patients with one or more risk factors admitted with acute coronary syndrome.
This was a retrospective analysis of patients admitted with first episode of acute coronary syndrome without previous heart disease, who were included in a national acute coronary syndrome registry. The patients were divided according to the number of risk factors, as follows: 0 risk factor (G0), 1 or 2 risk factors (G1 - 2) and 3 or more risk factors (G ≥ 3). Comparative analysis was performed between the three groups, and independent predictors of cardiac arrest and death were studied.
A total of 5,518 patients were studied, of which 72.2% were male and the mean age was 64 ± 14 years. G0 had a greater incidence of ST-segment elevation myocardial infarction, with the left anterior descending artery being the most frequently involved vessel, and a lower prevalence of multivessel disease. Even though G0 had a lower Killip class (96% in Killip I; p < 0.001) and higher ejection fraction (G0 56 ± 10% versus G1 - 2 and G ≥ 3 53 ± 12%; p = 0.024) on admission, there was a significant higher incidence of cardiac arrest. Multivariate analysis identified the absence of risk factors as an independent predictor of cardiac arrest (OR 2.78; p = 0.019). Hospital mortality was slightly higher in G0, although this difference was not significant. By Cox regression analysis, the number of risk factors was found not to be associated with mortality. Predictors of death at 1 year follow up included age (OR 1.05; p < 0.001), ST-segment elevation myocardial infarction (OR 1.94; p = 0.003) and ejection fraction < 50% (OR 2.34; p < 0.001).
Even though the group without risk factors was composed of younger patients with fewer comorbidities, better left ventricular function and less extensive coronary disease, the absence of risk factors was an independent predictor of cardiac arrest.
Abstract
Rev Bras Ter Intensiva. 2012;24(4):352-356
DOI 10.1590/S0103-507X2012000400010
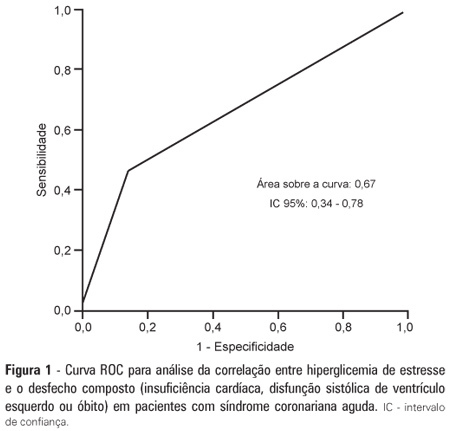
OBJECTIVE: To demonstrate the prevalence of stress hyperglycemia in a cohort of patients with acute coronary syndrome and to determine the correlation of stress hyperglycemia with death, heart failure and/or left ventricular systolic dysfunction during the intrahospital phase. METHODS: A prospective initial cohort study of hospitalized patients with acute coronary syndrome with or without ST segment elevation. The groups were compared to demonstrate the correlation between stress hyperglycemia and cardiovascular events. The chi-square test or Fisher's exact test and student's t-test were used to compare the groups with and without stress hyperglycemia. The variables with p<0.20 in the univariate analysis were submitted to logistic regression. RESULTS: In total, 363 patients with an average age of 12.45 ± 62.06 were studied. There was a predominance of males (64.2%). In total, 96 patients (26.4%) presented with stress hyperglycemia. There were no differences between the groups with or without stress hyperglycemia. The area under the ROC curve was 0.67 for the relationship between stress hyperglycemia and the composite outcome heart failure, left ventricular systolic dysfunction or death at the end of the hospital admission. The ROC curve proved that stress hyperglycemia was the predictor of the composite outcome (death, heart failure and/or ventricular dysfunction). The multivariate analysis did not indicate age, stress hyperglycemia or admission heart rate as risk factors. CONCLUSION: Stress hyperglycemia was common in the studied sample. In the univariate analysis, the presence of stress hyperglycemia was associated with such events as death, heart failure and/or intrahospital ventricular dysfunction in patients with acute coronary syndrome.
Abstract
Rev Bras Ter Intensiva. 2012;24(4):352-356
DOI 10.1590/S0103-507X2012000400010
OBJECTIVE: To demonstrate the prevalence of stress hyperglycemia in a cohort of patients with acute coronary syndrome and to determine the correlation of stress hyperglycemia with death, heart failure and/or left ventricular systolic dysfunction during the intrahospital phase. METHODS: A prospective initial cohort study of hospitalized patients with acute coronary syndrome with or without ST segment elevation. The groups were compared to demonstrate the correlation between stress hyperglycemia and cardiovascular events. The chi-square test or Fisher's exact test and student's t-test were used to compare the groups with and without stress hyperglycemia. The variables with p<0.20 in the univariate analysis were submitted to logistic regression. RESULTS: In total, 363 patients with an average age of 12.45 ± 62.06 were studied. There was a predominance of males (64.2%). In total, 96 patients (26.4%) presented with stress hyperglycemia. There were no differences between the groups with or without stress hyperglycemia. The area under the ROC curve was 0.67 for the relationship between stress hyperglycemia and the composite outcome heart failure, left ventricular systolic dysfunction or death at the end of the hospital admission. The ROC curve proved that stress hyperglycemia was the predictor of the composite outcome (death, heart failure and/or ventricular dysfunction). The multivariate analysis did not indicate age, stress hyperglycemia or admission heart rate as risk factors. CONCLUSION: Stress hyperglycemia was common in the studied sample. In the univariate analysis, the presence of stress hyperglycemia was associated with such events as death, heart failure and/or intrahospital ventricular dysfunction in patients with acute coronary syndrome.
Abstract
Rev Bras Ter Intensiva. 2012;24(3):284-293
DOI 10.1590/S0103-507X2012000300013
The development of antiplatelet and antithrombotic therapies, in addition to interventionist strategy, has resulted in great improvements in the outcomes of patients with non-ST-segment elevation acute coronary syndrome. Parallel to therapeutic advances, bleeding, which can be induced during management, increases the risk of recurrent ischemia, myocardial infarction and death. The present literature review describes the benefits and bleeding risks of each medication or intervention strategy and suggests guidelines for managing these patients.
Abstract
Rev Bras Ter Intensiva. 2012;24(3):284-293
DOI 10.1590/S0103-507X2012000300013
The development of antiplatelet and antithrombotic therapies, in addition to interventionist strategy, has resulted in great improvements in the outcomes of patients with non-ST-segment elevation acute coronary syndrome. Parallel to therapeutic advances, bleeding, which can be induced during management, increases the risk of recurrent ischemia, myocardial infarction and death. The present literature review describes the benefits and bleeding risks of each medication or intervention strategy and suggests guidelines for managing these patients.