Lactic acid Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2020;32(1):99-107
DOI 10.5935/0103-507X.20200015
To assess whether fluid overload in fluid therapy is a prognostic factor for patients with septic shock when adjusted for lactate clearance goals.
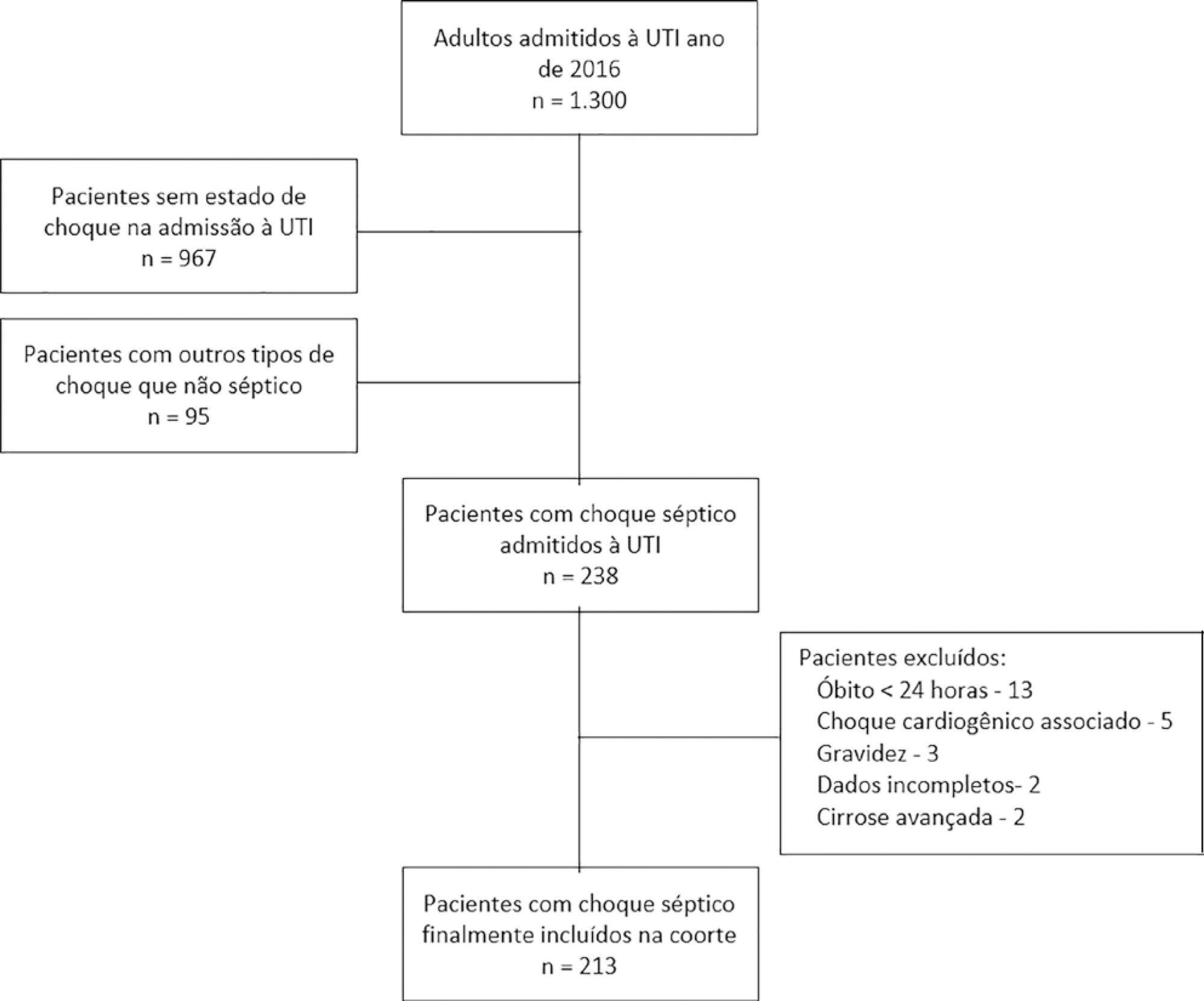
This was a retrospective cohort study conducted at a level IV care hospital in Bogotá, Colombia. A cohort of patients with septic shock was assembled. Their characteristics and fluid balance were documented. The patients were stratified by exposure levels according to the magnitude of fluid overload by body weight after 24 hours of therapy. Mortality was determined at 30 days, and an unconditional logistic regression model was created, adjusting for confounders. The statistical significance was established at p ≤ 0.05.
There were 213 patients with septic shock, and 60.8% had a lactate clearance ≥ 50% after treatment. Ninety-seven (46%) patients developed fluid overload ≥ 5%, and only 30 (13%) developed overload ≥ 10%. Patients exhibiting fluid overload ≥ 5% received an average of 6227mL of crystalloids (SD ± 5838mL) in 24 hours, compared to 3978mL (SD ± 3728mL) among unexposed patients (p = 0.000). The patients who developed fluid overload were treated with mechanical ventilation (70.7% versus 50.8%) (p = 0.003), albumin (74.7% versus 55.2%) (p = 0.003) and corticosteroids (53.5% versus 35.0%) (p = 0.006) more frequently than those who did not develop fluid overload. In the multivariable analysis, cumulative fluid balance was not associated with mortality (OR 1.03; 95%CI 0.89 - 1.20).
Adjusting for the severity of the condition and adequate lactate clearance, cumulative fluid balance was not associated with increased mortality in this Latin American cohort of septic patients.
Abstract
Rev Bras Ter Intensiva. 2020;32(1):99-107
DOI 10.5935/0103-507X.20200015
To assess whether fluid overload in fluid therapy is a prognostic factor for patients with septic shock when adjusted for lactate clearance goals.
This was a retrospective cohort study conducted at a level IV care hospital in Bogotá, Colombia. A cohort of patients with septic shock was assembled. Their characteristics and fluid balance were documented. The patients were stratified by exposure levels according to the magnitude of fluid overload by body weight after 24 hours of therapy. Mortality was determined at 30 days, and an unconditional logistic regression model was created, adjusting for confounders. The statistical significance was established at p ≤ 0.05.
There were 213 patients with septic shock, and 60.8% had a lactate clearance ≥ 50% after treatment. Ninety-seven (46%) patients developed fluid overload ≥ 5%, and only 30 (13%) developed overload ≥ 10%. Patients exhibiting fluid overload ≥ 5% received an average of 6227mL of crystalloids (SD ± 5838mL) in 24 hours, compared to 3978mL (SD ± 3728mL) among unexposed patients (p = 0.000). The patients who developed fluid overload were treated with mechanical ventilation (70.7% versus 50.8%) (p = 0.003), albumin (74.7% versus 55.2%) (p = 0.003) and corticosteroids (53.5% versus 35.0%) (p = 0.006) more frequently than those who did not develop fluid overload. In the multivariable analysis, cumulative fluid balance was not associated with mortality (OR 1.03; 95%CI 0.89 - 1.20).
Adjusting for the severity of the condition and adequate lactate clearance, cumulative fluid balance was not associated with increased mortality in this Latin American cohort of septic patients.
Abstract
Rev Bras Ter Intensiva. 2013;25(4):270-278
DOI 10.5935/0103-507X.20130047
The current definition of severe sepsis and septic shock includes a heterogeneous profile of patients. Although the prognostic value of hyperlactatemia is well established, hyperlactatemia is observed in patients with and without shock. The present study aimed to compare the prognosis of septic patients by stratifying them according to two factors: hyperlactatemia and persistent hypotension.
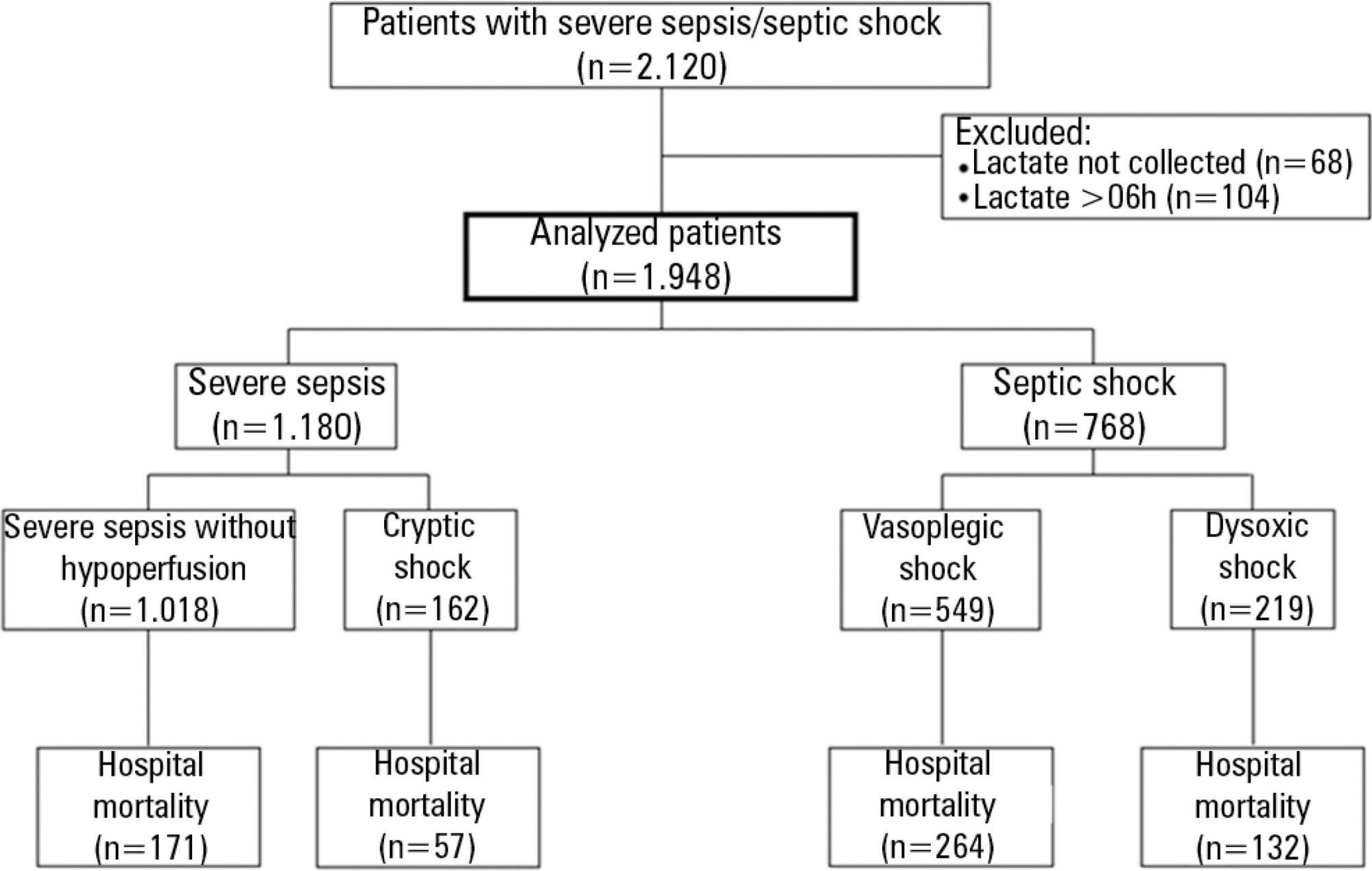
The present study is a secondary analysis of an observational study conducted in ten hospitals in Brazil (Rede Amil - SP). Septic patients with initial lactate measurements in the first 6 hours of diagnosis were included and divided into 4 groups according to hyperlactatemia (lactate >4mmol/L) and persistent hypotension: (1) severe sepsis (without both criteria); (2) cryptic shock (hyperlactatemia without persistent hypotension); (3) vasoplegic shock (persistent hypotension without hyperlactatemia); and (4) dysoxic shock (both criteria).
In total, 1,948 patients were analyzed, and the sepsis group represented 52% of the patients, followed by 28% with vasoplegic shock, 12% with dysoxic shock and 8% with cryptic shock. Survival at 28 days differed among the groups (p<0.001). Survival was highest among the severe sepsis group (69%, p<0.001 versus others), similar in the cryptic and vasoplegic shock groups (53%, p=0.39), and lowest in the dysoxic shock group (38%, p<0.001 versus others). In the adjusted analysis, the survival at 28 days remained different among the groups (p<0.001) and the dysoxic shock group exhibited the highest hazard ratio (HR=2.99, 95%CI 2.21-4.05).
The definition of sepsis includes four different profiles if we consider the presence of hyperlactatemia. Further studies are needed to better characterize septic patients, to understand the etiology and to design adequate targeted treatments.
Abstract
Rev Bras Ter Intensiva. 2013;25(4):270-278
DOI 10.5935/0103-507X.20130047
The current definition of severe sepsis and septic shock includes a heterogeneous profile of patients. Although the prognostic value of hyperlactatemia is well established, hyperlactatemia is observed in patients with and without shock. The present study aimed to compare the prognosis of septic patients by stratifying them according to two factors: hyperlactatemia and persistent hypotension.
The present study is a secondary analysis of an observational study conducted in ten hospitals in Brazil (Rede Amil - SP). Septic patients with initial lactate measurements in the first 6 hours of diagnosis were included and divided into 4 groups according to hyperlactatemia (lactate >4mmol/L) and persistent hypotension: (1) severe sepsis (without both criteria); (2) cryptic shock (hyperlactatemia without persistent hypotension); (3) vasoplegic shock (persistent hypotension without hyperlactatemia); and (4) dysoxic shock (both criteria).
In total, 1,948 patients were analyzed, and the sepsis group represented 52% of the patients, followed by 28% with vasoplegic shock, 12% with dysoxic shock and 8% with cryptic shock. Survival at 28 days differed among the groups (p<0.001). Survival was highest among the severe sepsis group (69%, p<0.001 versus others), similar in the cryptic and vasoplegic shock groups (53%, p=0.39), and lowest in the dysoxic shock group (38%, p<0.001 versus others). In the adjusted analysis, the survival at 28 days remained different among the groups (p<0.001) and the dysoxic shock group exhibited the highest hazard ratio (HR=2.99, 95%CI 2.21-4.05).
The definition of sepsis includes four different profiles if we consider the presence of hyperlactatemia. Further studies are needed to better characterize septic patients, to understand the etiology and to design adequate targeted treatments.
Abstract
Rev Bras Ter Intensiva. 2012;24(2):184-187
DOI 10.1590/S0103-507X2012000200015
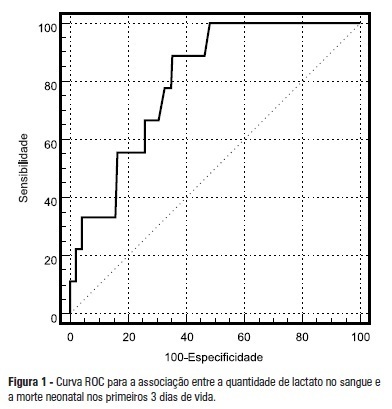
OBJECTIVE: To assess the correlation between plasma lactate concentrations in the first 6 hours of life and early neonatal mortality. METHODS: The patients were divided in 2 groups based on the cutoff point, obtained from a receiver operating characteristic (ROC) curve, of the plasma lactate concentration that best predicted neonatal mortality during the first 3 days of life. The differences between groups and the correlations between the investigated variables and the plasma lactate concentrations measured in the first 6 hours of life were analyzed using the Chi-square, Student's t, or Mann-Whitney tests and logistic regression. RESULTS: The best cutoff point of the plasma lactate concentration as determined by the ROC curve for death during the first 3 days of life was 4.2 mmol/L. The investigated groups differed with regards to the average birth weight, which was lower in the group with serum lactate levels > 4.2 mmol/L, and the match between birth weight and gestational age, where the group with serum lactate levels > 4.2 mmol/L exhibited a higher number of newborns small for their gestational age. Seizures, intracranial hemorrhage, and death during the first 3 days of life occurred more frequently in the group with serum lactate levels > 4.2 mmol/L. CONCLUSION: In the investigated samples, the presence of plasma lactate concentrations > 4.2 mmol/L in the first 6 hours of life correlated with neonatal death during the first 3 days of life, a higher frequency of neurologic morbidity, and newborns that were small for their gestational age.
Abstract
Rev Bras Ter Intensiva. 2012;24(2):184-187
DOI 10.1590/S0103-507X2012000200015
OBJECTIVE: To assess the correlation between plasma lactate concentrations in the first 6 hours of life and early neonatal mortality. METHODS: The patients were divided in 2 groups based on the cutoff point, obtained from a receiver operating characteristic (ROC) curve, of the plasma lactate concentration that best predicted neonatal mortality during the first 3 days of life. The differences between groups and the correlations between the investigated variables and the plasma lactate concentrations measured in the first 6 hours of life were analyzed using the Chi-square, Student's t, or Mann-Whitney tests and logistic regression. RESULTS: The best cutoff point of the plasma lactate concentration as determined by the ROC curve for death during the first 3 days of life was 4.2 mmol/L. The investigated groups differed with regards to the average birth weight, which was lower in the group with serum lactate levels > 4.2 mmol/L, and the match between birth weight and gestational age, where the group with serum lactate levels > 4.2 mmol/L exhibited a higher number of newborns small for their gestational age. Seizures, intracranial hemorrhage, and death during the first 3 days of life occurred more frequently in the group with serum lactate levels > 4.2 mmol/L. CONCLUSION: In the investigated samples, the presence of plasma lactate concentrations > 4.2 mmol/L in the first 6 hours of life correlated with neonatal death during the first 3 days of life, a higher frequency of neurologic morbidity, and newborns that were small for their gestational age.
Abstract
Rev Bras Ter Intensiva. 2006;18(1):22-26
DOI 10.1590/S0103-507X2006000100005
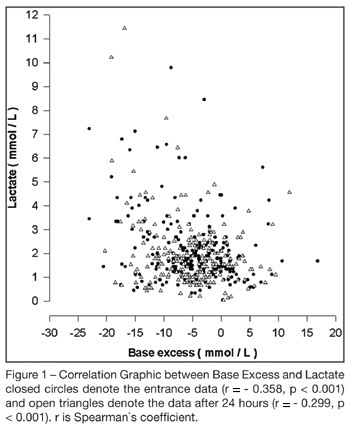
BACKGROUND AND OBJECTIVES: To correlate standard base excess (SBE) with serum lactate level and demonstrate the independent prognostic significance of each one. METHODS: In a retrospective study, we retrieved data from 333 patients of our prospectively collected database of 7-bed medical intensive care unit of a 1800-bed university hospital. RESULTS: The results have shown a poor correlation between SBE and lactate, r = - 0.358, p < 0.001, and an independent prognostic significance of each one when analyzed concomitantly, odds ratio (95% Confidence interval) = 0.996 (0.992 - 0.999) to standard base excess and 1.000 (1.000 - 1.002) to lactate at entrance; and odds ratio (95% Confidence interval ) = 0.990 (0.985 - 0.994) to standard base excess and 1.003 (1.001 - 1.005) to lactate after 24 hours. The accuracy of standard base excess was close to lactate to determine in-intensive care unit death. CONCLUSIONS: The lactic component of the metabolic acidosis is not the major determinant of standard base excess. Serum lactate and SBE are independent outcome predictors in critically ill patients.
Abstract
Rev Bras Ter Intensiva. 2006;18(1):22-26
DOI 10.1590/S0103-507X2006000100005
BACKGROUND AND OBJECTIVES: To correlate standard base excess (SBE) with serum lactate level and demonstrate the independent prognostic significance of each one. METHODS: In a retrospective study, we retrieved data from 333 patients of our prospectively collected database of 7-bed medical intensive care unit of a 1800-bed university hospital. RESULTS: The results have shown a poor correlation between SBE and lactate, r = - 0.358, p < 0.001, and an independent prognostic significance of each one when analyzed concomitantly, odds ratio (95% Confidence interval) = 0.996 (0.992 - 0.999) to standard base excess and 1.000 (1.000 - 1.002) to lactate at entrance; and odds ratio (95% Confidence interval ) = 0.990 (0.985 - 0.994) to standard base excess and 1.003 (1.001 - 1.005) to lactate after 24 hours. The accuracy of standard base excess was close to lactate to determine in-intensive care unit death. CONCLUSIONS: The lactic component of the metabolic acidosis is not the major determinant of standard base excess. Serum lactate and SBE are independent outcome predictors in critically ill patients.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (116) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)