-
Special Article
Guidelines for the pharmacological treatment of COVID-19. The task-force/consensus guideline of the Brazilian Association of Intensive Care Medicine, the Brazilian Society of Infectious Diseases and the Brazilian Society of Pulmonology and Tisiology
- Maicon Falavigna
 ,
, - Verônica Colpani,
- Cinara Stein,
- Luciano Cesar Pontes Azevedo,
- Angela Maria Bagattini, [ … ],
- Felipe Dal-Pizzol
Abstract
Special ArticleGuidelines for the pharmacological treatment of COVID-19. The task-force/consensus guideline of the Brazilian Association of Intensive Care Medicine, the Brazilian Society of Infectious Diseases and the Brazilian Society of Pulmonology and Tisiology
Rev Bras Ter Intensiva. 2020;32(2):166-196
DOI 10.5935/0103-507X.20200039
- Maicon Falavigna ,
- Verônica Colpani,
- Cinara Stein,
- Luciano Cesar Pontes Azevedo,
- Angela Maria Bagattini,
- Gabriela Vilela de Brito,
- José Miguel Chatkin,
- Sergio Cimerman,
- Mirian de Freitas Dal Ben Corradi,
- Clovis Arns da Cunha,
- Flávia Cordeiro de Medeiros,
- Haliton Alves de Oliveira Junior,
- Leandro Genehr Fritscher,
- Marcelo Basso Gazzana,
- Débora Dalmas Gräf,
- Lays Pires Marra,
- Jessica Yumi Matuoka,
- Michelle Silva Nunes ,
- Daniela Vianna Pachito,
- Cássia Garcia Moraes Pagano,
- Patrícia do Carmo Silva Parreira,
- Rachel Riera,
- Amilton Silva Júnior,
- Bruno de Melo Tavares,
- Alexandre Prehn Zavascki,
- Regis Goulart Rosa ,
- Felipe Dal-Pizzol
Views0See moreABSTRACT
Introduction:
Different therapies are currently used, considered, or proposed for the treatment of COVID-19; for many of those therapies, no appropriate assessment of effectiveness and safety was performed. This document aims to provide scientifically available evidence-based information in a transparent interpretation, to subsidize decisions related to the pharmacological therapy of COVID-19 in Brazil.
Methods:
A group of 27 experts and methodologists integrated a task-force formed by professionals from the Brazilian Association of Intensive Care Medicine (Associação de Medicina Intensiva Brasileira – AMIB), the Brazilian Society of Infectious Diseases (Sociedad Brasileira de Infectologia – SBI) and the Brazilian Society of Pulmonology and Tisiology (Sociedade Brasileira de Pneumologia e Tisiologia – SBPT). Rapid systematic reviews, updated on April 28, 2020, were conducted. The assessment of the quality of evidence and the development of recommendations followed the GRADE system. The recommendations were written on May 5, 8, and 13, 2020.
Results:
Eleven recommendations were issued based on low or very-low level evidence. We do not recommend the routine use of hydroxychloroquine, chloroquine, azithromycin, lopinavir/ritonavir, corticosteroids, or tocilizumab for the treatment of COVID-19. Prophylactic heparin should be used in hospitalized patients, however, no anticoagulation should be provided for patients without a specific clinical indication. Antibiotics and oseltamivir should only be considered for patients with suspected bacterial or influenza coinfection, respectively.
Conclusion:
So far no pharmacological intervention was proven effective and safe to warrant its use in the routine treatment of COVID-19 patients; therefore such patients should ideally be treated in the context of clinical trials. The recommendations herein provided will be revised continuously aiming to capture newly generated evidence.
Views0

Abstract
Special ArticleGuidelines for the pharmacological treatment of COVID-19. The task-force/consensus guideline of the Brazilian Association of Intensive Care Medicine, the Brazilian Society of Infectious Diseases and the Brazilian Society of Pulmonology and Tisiology
Rev Bras Ter Intensiva. 2020;32(2):166-196
DOI 10.5935/0103-507X.20200039
- Maicon Falavigna ,
- Verônica Colpani,
- Cinara Stein,
- Luciano Cesar Pontes Azevedo,
- Angela Maria Bagattini,
- Gabriela Vilela de Brito,
- José Miguel Chatkin,
- Sergio Cimerman,
- Mirian de Freitas Dal Ben Corradi,
- Clovis Arns da Cunha,
- Flávia Cordeiro de Medeiros,
- Haliton Alves de Oliveira Junior,
- Leandro Genehr Fritscher,
- Marcelo Basso Gazzana,
- Débora Dalmas Gräf,
- Lays Pires Marra,
- Jessica Yumi Matuoka,
- Michelle Silva Nunes ,
- Daniela Vianna Pachito,
- Cássia Garcia Moraes Pagano,
- Patrícia do Carmo Silva Parreira,
- Rachel Riera,
- Amilton Silva Júnior,
- Bruno de Melo Tavares,
- Alexandre Prehn Zavascki,
- Regis Goulart Rosa ,
- Felipe Dal-Pizzol
Views0See moreABSTRACT
Introduction:
Different therapies are currently used, considered, or proposed for the treatment of COVID-19; for many of those therapies, no appropriate assessment of effectiveness and safety was performed. This document aims to provide scientifically available evidence-based information in a transparent interpretation, to subsidize decisions related to the pharmacological therapy of COVID-19 in Brazil.
Methods:
A group of 27 experts and methodologists integrated a task-force formed by professionals from the Brazilian Association of Intensive Care Medicine (Associação de Medicina Intensiva Brasileira – AMIB), the Brazilian Society of Infectious Diseases (Sociedad Brasileira de Infectologia – SBI) and the Brazilian Society of Pulmonology and Tisiology (Sociedade Brasileira de Pneumologia e Tisiologia – SBPT). Rapid systematic reviews, updated on April 28, 2020, were conducted. The assessment of the quality of evidence and the development of recommendations followed the GRADE system. The recommendations were written on May 5, 8, and 13, 2020.
Results:
Eleven recommendations were issued based on low or very-low level evidence. We do not recommend the routine use of hydroxychloroquine, chloroquine, azithromycin, lopinavir/ritonavir, corticosteroids, or tocilizumab for the treatment of COVID-19. Prophylactic heparin should be used in hospitalized patients, however, no anticoagulation should be provided for patients without a specific clinical indication. Antibiotics and oseltamivir should only be considered for patients with suspected bacterial or influenza coinfection, respectively.
Conclusion:
So far no pharmacological intervention was proven effective and safe to warrant its use in the routine treatment of COVID-19 patients; therefore such patients should ideally be treated in the context of clinical trials. The recommendations herein provided will be revised continuously aiming to capture newly generated evidence.
- Maicon Falavigna
-
Commentary
coagulation profile in severe COVID-19 patients: what do we know so far?
Rev Bras Ter Intensiva. 2020;32(2):197-199
Abstract
Commentarycoagulation profile in severe COVID-19 patients: what do we know so far?
Rev Bras Ter Intensiva. 2020;32(2):197-199
DOI 10.5935/0103-507X.20200031
Views0Severe coronavirus disease 2019 (COVID-19) patients may present with single organ failure, but some of them progress to more systemic and multiple organ dysfunctions. One of the most significant markers of poor prognosis in those patients is the development of coagulopathy. These critically ill patients may have abnormal coagulation parameters, which may lead to hypercoagulability […]See moreViews0Abstract
Commentarycoagulation profile in severe COVID-19 patients: what do we know so far?
Rev Bras Ter Intensiva. 2020;32(2):197-199
DOI 10.5935/0103-507X.20200031
Views0Severe coronavirus disease 2019 (COVID-19) patients may present with single organ failure, but some of them progress to more systemic and multiple organ dysfunctions. One of the most significant markers of poor prognosis in those patients is the development of coagulopathy. These critically ill patients may have abnormal coagulation parameters, which may lead to hypercoagulability […]See more -
Commentary
Shared decision-making in the context of COVID-19
Rev Bras Ter Intensiva. 2020;32(2):200-202
Abstract
CommentaryShared decision-making in the context of COVID-19
Rev Bras Ter Intensiva. 2020;32(2):200-202
DOI 10.5935/0103-507X.20200034
Views0Shared decision-makingShared decision-making finds support in the ethical principle of beneficence and nonmaleficence. It aims to involve patients and/or family members in decisions related to clinical care and should be part of clinical practice. Shared decision-making means respecting the autonomy of patients and ensuring care that is consistent with their values and preferences. Therefore, the […]See moreViews0Abstract
CommentaryShared decision-making in the context of COVID-19
Rev Bras Ter Intensiva. 2020;32(2):200-202
DOI 10.5935/0103-507X.20200034
Views0Shared decision-makingShared decision-making finds support in the ethical principle of beneficence and nonmaleficence. It aims to involve patients and/or family members in decisions related to clinical care and should be part of clinical practice. Shared decision-making means respecting the autonomy of patients and ensuring care that is consistent with their values and preferences. Therefore, the […]See more -
Commentary
How to evaluate intensive care unit performance during the COVID-19 pandemic
Rev Bras Ter Intensiva. 2020;32(2):203-206
Abstract
CommentaryHow to evaluate intensive care unit performance during the COVID-19 pandemic
Rev Bras Ter Intensiva. 2020;32(2):203-206
DOI 10.5935/0103-507X.20200040
Views0CONCLUSIONMeasuring the ICU performance was never so important neither so difficult as during the COVID-19 pandemic. While few data on prognostic scores is available, therefore limiting the use of more traditional metrics, ICUs should focus on measuring indirect performance parameters, especially analyzing case-mix, outcomes, and the rate of adherence to best practices.[…]See moreViews0Abstract
CommentaryHow to evaluate intensive care unit performance during the COVID-19 pandemic
Rev Bras Ter Intensiva. 2020;32(2):203-206
DOI 10.5935/0103-507X.20200040
Views0CONCLUSIONMeasuring the ICU performance was never so important neither so difficult as during the COVID-19 pandemic. While few data on prognostic scores is available, therefore limiting the use of more traditional metrics, ICUs should focus on measuring indirect performance parameters, especially analyzing case-mix, outcomes, and the rate of adherence to best practices.[…]See more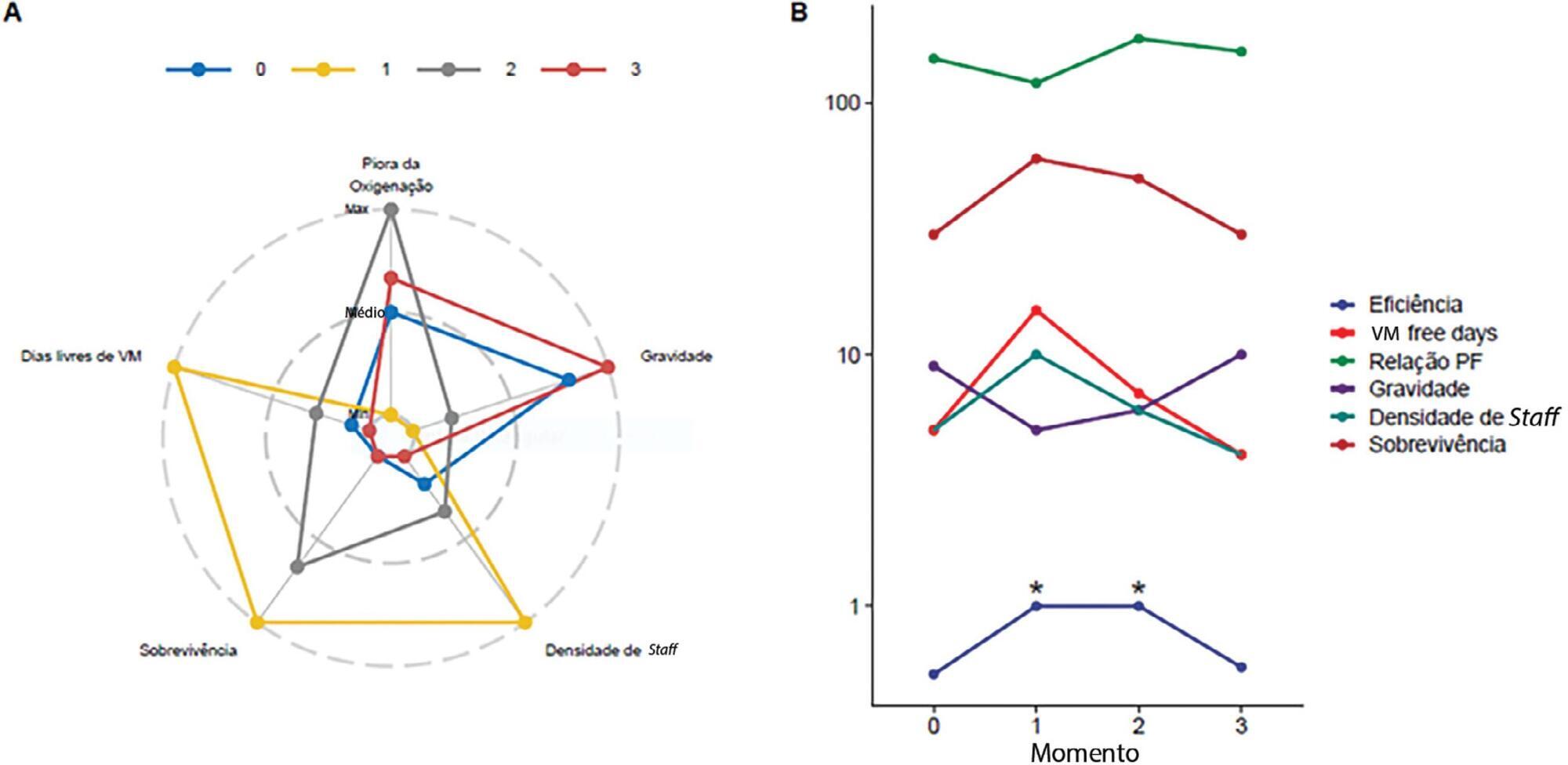
-
Commentary
What every intensivist must know about antimicrobial stewardship: its pitfalls and its challenges
Rev Bras Ter Intensiva. 2020;32(2):207-212
Abstract
CommentaryWhat every intensivist must know about antimicrobial stewardship: its pitfalls and its challenges
Rev Bras Ter Intensiva. 2020;32(2):207-212
DOI 10.5935/0103-507X.20200037
Views0Antimicrobial stewardship should not be performed addressing cost containment as the main purposeThe absence of a universal definition for AMS combined with the lack of international guidance and standards are among the many barriers to the implementation of these programs globally. The purpose of AMS is to promote the optimal/prudent/responsible use of antibiotics to optimize […]See moreViews0Abstract
CommentaryWhat every intensivist must know about antimicrobial stewardship: its pitfalls and its challenges
Rev Bras Ter Intensiva. 2020;32(2):207-212
DOI 10.5935/0103-507X.20200037
Views0Antimicrobial stewardship should not be performed addressing cost containment as the main purposeThe absence of a universal definition for AMS combined with the lack of international guidance and standards are among the many barriers to the implementation of these programs globally. The purpose of AMS is to promote the optimal/prudent/responsible use of antibiotics to optimize […]See more -
Original Article
Progression of confirmed COVID-19 cases after the implementation of control measures
- Bianca Brandão de Paula Antunes ,
- Igor Tona Peres,
- Fernanda Araújo Baião ,
- Otavio Tavares Ranzani,
- Leonardo dos Santos Lourenço Bastos, [ … ],
- Fernando Augusto Bozza
Abstract
Original ArticleProgression of confirmed COVID-19 cases after the implementation of control measures
Rev Bras Ter Intensiva. 2020;32(2):213-223
DOI 10.5935/0103-507X.20200028
- Bianca Brandão de Paula Antunes ,
- Igor Tona Peres,
- Fernanda Araújo Baião ,
- Otavio Tavares Ranzani,
- Leonardo dos Santos Lourenço Bastos,
- Amanda de Araújo Batista da Silva,
- Guilherme Faveret Garcia de Souza,
- Janaina Figueira Marchesi,
- Leila Figueiredo Dantas ,
- Soraida Aguilar Vargas,
- Paula Maçaira,
- Silvio Hamacher,
- Fernando Augusto Bozza
Views0ABSTRACT
Objective:
To analyse the measures adopted by countries that have shown control over the transmission of coronavirus disease 2019 (COVID-19) and how each curve of accumulated cases behaved after the implementation of those measures.
Methods:
The methodology adopted for this study comprises three phases: systemizing control measures adopted by different countries, identifying structural breaks in the growth of the number of cases for those countries, and analyzing Brazilian data in particular.
Results:
We noted that China (excluding Hubei Province), Hubei Province, and South Korea have been effective in their deceleration of the growth rates of COVID-19 cases. The effectiveness of the measures taken by these countries could be seen after 1 to 2 weeks of their application. In Italy and Spain, control measures at the national level were taken at a late stage of the epidemic, which could have contributed to the high propagation of COVID-19. In Brazil, Rio de Janeiro and São Paulo adopted measures that could be effective in slowing the propagation of the virus. However, we only expect to see their effects on the growth of the curve in the coming days.
Conclusion:
Our results may help decisionmakers in countries in relatively early stages of the epidemic, especially Brazil, understand the importance of control measures in decelerating the growth curve of confirmed cases.
Keywords:Control measureCoronavirus infections/prevention & controlCOVID-19Decision makeInfection control/methodsPandemics/prevention & controlSee moreViews0Abstract
Original ArticleProgression of confirmed COVID-19 cases after the implementation of control measures
Rev Bras Ter Intensiva. 2020;32(2):213-223
DOI 10.5935/0103-507X.20200028
- Bianca Brandão de Paula Antunes ,
- Igor Tona Peres,
- Fernanda Araújo Baião ,
- Otavio Tavares Ranzani,
- Leonardo dos Santos Lourenço Bastos,
- Amanda de Araújo Batista da Silva,
- Guilherme Faveret Garcia de Souza,
- Janaina Figueira Marchesi,
- Leila Figueiredo Dantas ,
- Soraida Aguilar Vargas,
- Paula Maçaira,
- Silvio Hamacher,
- Fernando Augusto Bozza
Views0ABSTRACT
Objective:
To analyse the measures adopted by countries that have shown control over the transmission of coronavirus disease 2019 (COVID-19) and how each curve of accumulated cases behaved after the implementation of those measures.
Methods:
The methodology adopted for this study comprises three phases: systemizing control measures adopted by different countries, identifying structural breaks in the growth of the number of cases for those countries, and analyzing Brazilian data in particular.
Results:
We noted that China (excluding Hubei Province), Hubei Province, and South Korea have been effective in their deceleration of the growth rates of COVID-19 cases. The effectiveness of the measures taken by these countries could be seen after 1 to 2 weeks of their application. In Italy and Spain, control measures at the national level were taken at a late stage of the epidemic, which could have contributed to the high propagation of COVID-19. In Brazil, Rio de Janeiro and São Paulo adopted measures that could be effective in slowing the propagation of the virus. However, we only expect to see their effects on the growth of the curve in the coming days.
Conclusion:
Our results may help decisionmakers in countries in relatively early stages of the epidemic, especially Brazil, understand the importance of control measures in decelerating the growth curve of confirmed cases.
Keywords:Control measureCoronavirus infections/prevention & controlCOVID-19Decision makeInfection control/methodsPandemics/prevention & controlSee more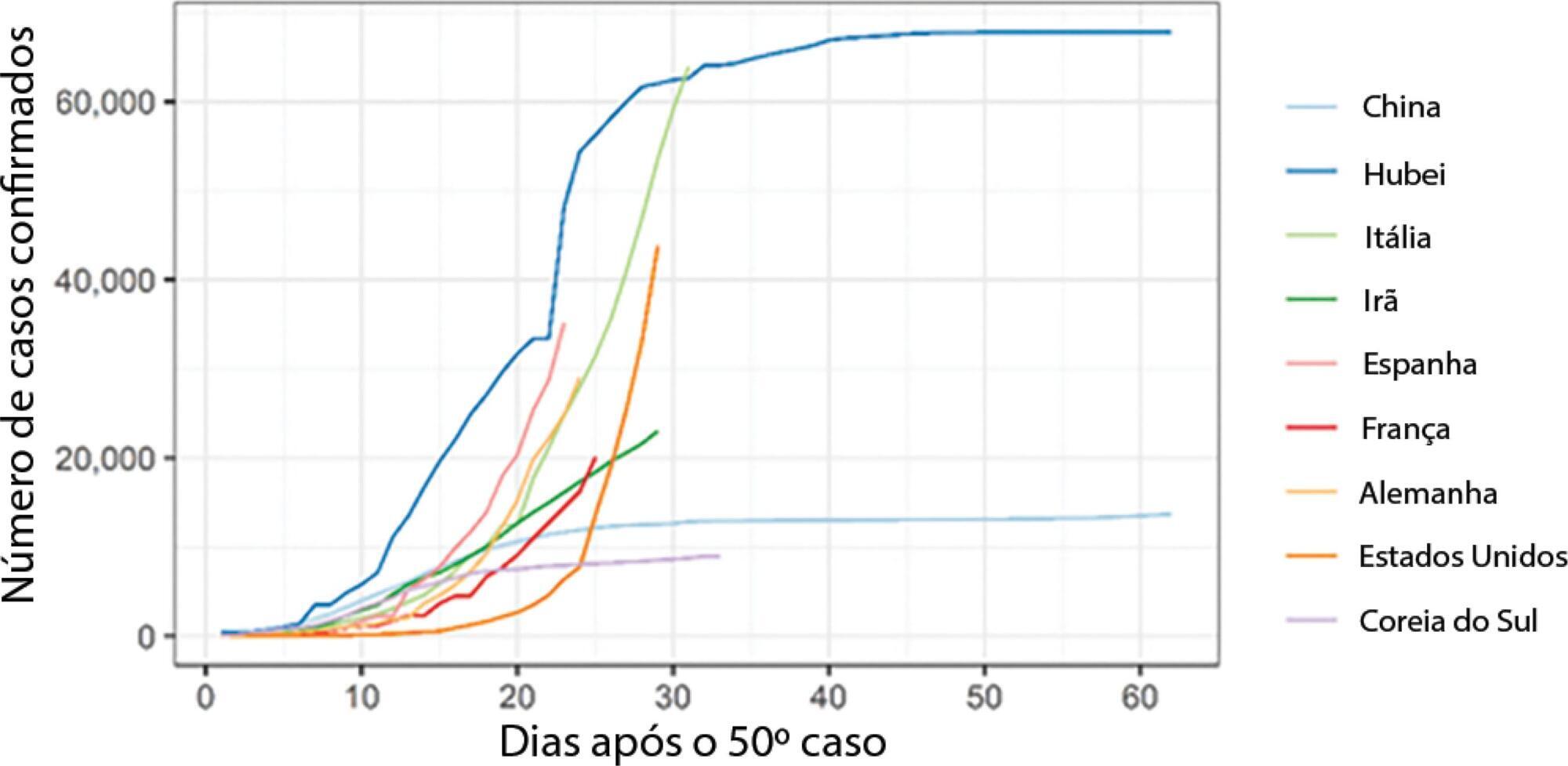
- Bianca Brandão de Paula Antunes
-
Original Article
Analysis of COVID-19 under-reporting in Brazil
- Marcelo Freitas do Prado,
- Bianca Brandão de Paula Antunes ,
- Leonardo dos Santos Lourenço Bastos,
- Igor Tona Peres,
- Amanda de Araújo Batista da Silva, [ … ],
- Fernando Augusto Bozza
Abstract
Original ArticleAnalysis of COVID-19 under-reporting in Brazil
Rev Bras Ter Intensiva. 2020;32(2):224-228
DOI 10.5935/0103-507X.20200030
- Marcelo Freitas do Prado,
- Bianca Brandão de Paula Antunes ,
- Leonardo dos Santos Lourenço Bastos,
- Igor Tona Peres,
- Amanda de Araújo Batista da Silva,
- Leila Figueiredo Dantas ,
- Fernanda Araújo Baião ,
- Paula Maçaira ,
- Silvio Hamacher,
- Fernando Augusto Bozza
Views5ABSTRACT
Objective:
To estimate the reporting rates of coronavirus disease 2019 (COVID-19) cases for Brazil as a whole and states.
Methods:
We estimated the actual number of COVID-19 cases using the reported number of deaths in Brazil and each state, and the expected case-fatality ratio from the World Health Organization. Brazil’s expected case-fatality ratio was also adjusted by the population’s age pyramid. Therefore, the notification rate can be defined as the number of confirmed cases (notified by the Ministry of Health) divided by the number of expected cases (estimated from the number of deaths).
Results:
The reporting rate for COVID-19 in Brazil was estimated at 9.2% (95%CI 8.8% – 9.5%), with all the states presenting rates below 30%. São Paulo and Rio de Janeiro, the most populated states in Brazil, showed small reporting rates (8.9% and 7.2%, respectively). The highest reporting rate occurred in Roraima (31.7%) and the lowest in Paraiba (3.4%).
Conclusion:
The results indicated that the reporting of confirmed cases in Brazil is much lower as compared to other countries we analyzed. Therefore, decision-makers, including the government, fail to know the actual dimension of the pandemic, which may interfere with the determination of control measures.
Keywords:BrazilCoronavirus infectionsCOVID-19MortalityPandemics/statistics & numerical dataReporting of healthcare dataSee moreViews5Abstract
Original ArticleAnalysis of COVID-19 under-reporting in Brazil
Rev Bras Ter Intensiva. 2020;32(2):224-228
DOI 10.5935/0103-507X.20200030
- Marcelo Freitas do Prado,
- Bianca Brandão de Paula Antunes ,
- Leonardo dos Santos Lourenço Bastos,
- Igor Tona Peres,
- Amanda de Araújo Batista da Silva,
- Leila Figueiredo Dantas ,
- Fernanda Araújo Baião ,
- Paula Maçaira ,
- Silvio Hamacher,
- Fernando Augusto Bozza
Views5ABSTRACT
Objective:
To estimate the reporting rates of coronavirus disease 2019 (COVID-19) cases for Brazil as a whole and states.
Methods:
We estimated the actual number of COVID-19 cases using the reported number of deaths in Brazil and each state, and the expected case-fatality ratio from the World Health Organization. Brazil’s expected case-fatality ratio was also adjusted by the population’s age pyramid. Therefore, the notification rate can be defined as the number of confirmed cases (notified by the Ministry of Health) divided by the number of expected cases (estimated from the number of deaths).
Results:
The reporting rate for COVID-19 in Brazil was estimated at 9.2% (95%CI 8.8% – 9.5%), with all the states presenting rates below 30%. São Paulo and Rio de Janeiro, the most populated states in Brazil, showed small reporting rates (8.9% and 7.2%, respectively). The highest reporting rate occurred in Roraima (31.7%) and the lowest in Paraiba (3.4%).
Conclusion:
The results indicated that the reporting of confirmed cases in Brazil is much lower as compared to other countries we analyzed. Therefore, decision-makers, including the government, fail to know the actual dimension of the pandemic, which may interfere with the determination of control measures.
Keywords:BrazilCoronavirus infectionsCOVID-19MortalityPandemics/statistics & numerical dataReporting of healthcare dataSee more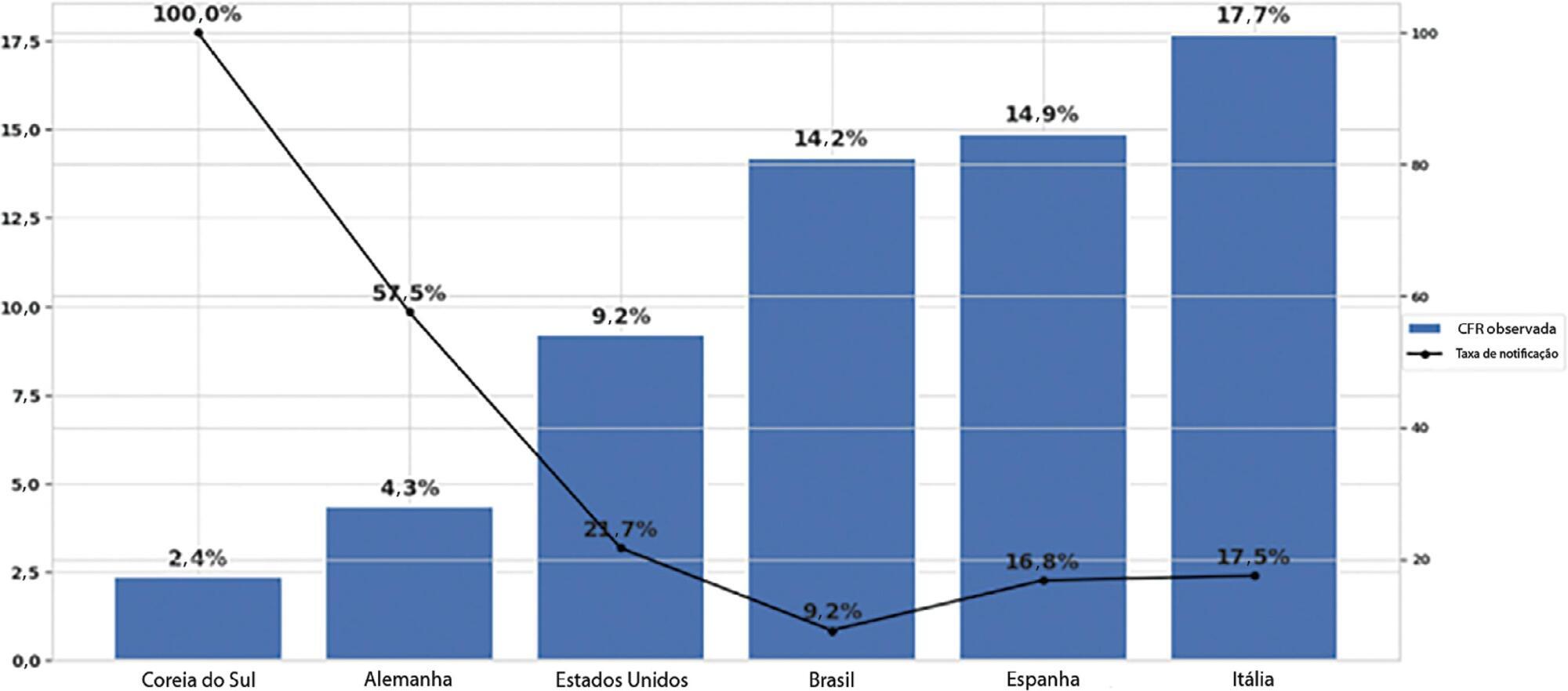
-
Original Article
Characteristics and short-term outcomes of patients with esophageal cancer with unplanned intensive care unit admissions: a retrospective cohort study
- Isabel Cristina Lima de Freitas,
- Dryelen Moreira de Assis,
- Cristina Prata Amendola,
- Diana da Silva Russo,
- Ana Paula Pierre de Moraes, [ … ],
- Antonio Paulo Nassar Júnior
Abstract
Original ArticleCharacteristics and short-term outcomes of patients with esophageal cancer with unplanned intensive care unit admissions: a retrospective cohort study
Rev Bras Ter Intensiva. 2020;32(2):229-234
DOI 10.5935/0103-507X.20200041
- Isabel Cristina Lima de Freitas,
- Dryelen Moreira de Assis,
- Cristina Prata Amendola,
- Diana da Silva Russo,
- Ana Paula Pierre de Moraes,
- Pedro Caruso,
- Antonio Paulo Nassar Júnior
Views0ABSTRACT
Objective:
To depict the clinical presentation and outcomes of a cohort of critically ill patients with esophageal cancer.
Methods:
We carried out a multicenter retrospective study that included patients with esophageal cancer admitted to intensive care units with acute illness between September 2009 and December 2017. We collected the demographic and clinical characteristics of all included patients, as well as organ-support measures and hospital outcomes. We performed logistic regression analysis to identify independent factors associated with in-hospital mortality.
Results:
Of 226 patients included in the study, 131 (58.0%) patients died before hospital discharge. Squamous cell carcinoma was more frequent than adenocarcinoma, and 124 (54.9%) patients had metastatic cancer. The main reasons for admission were sepsis/septic shock and acute respiratory failure. Mechanical ventilation (OR = 6.18; 95%CI 2.86 – 13.35) and metastatic disease (OR = 7.10; 95%CI 3.35 – 15.05) were independently associated with in-hospital mortality.
Conclusion:
In this cohort of patients with esophageal cancer admitted to intensive care units with acute illness, the in-hospital mortality rate was very high. The requirement for invasive mechanical ventilation and metastatic disease were independent prognostic factors and should be considered in discussions about the short-term outcomes of these patients.
Keywords:Critical careCritical care outcomesepidemiologyEsophageal neoplasmsMortalityPrognosisRespiration, artificialSee moreViews0Abstract
Original ArticleCharacteristics and short-term outcomes of patients with esophageal cancer with unplanned intensive care unit admissions: a retrospective cohort study
Rev Bras Ter Intensiva. 2020;32(2):229-234
DOI 10.5935/0103-507X.20200041
- Isabel Cristina Lima de Freitas,
- Dryelen Moreira de Assis,
- Cristina Prata Amendola,
- Diana da Silva Russo,
- Ana Paula Pierre de Moraes,
- Pedro Caruso,
- Antonio Paulo Nassar Júnior
Views0ABSTRACT
Objective:
To depict the clinical presentation and outcomes of a cohort of critically ill patients with esophageal cancer.
Methods:
We carried out a multicenter retrospective study that included patients with esophageal cancer admitted to intensive care units with acute illness between September 2009 and December 2017. We collected the demographic and clinical characteristics of all included patients, as well as organ-support measures and hospital outcomes. We performed logistic regression analysis to identify independent factors associated with in-hospital mortality.
Results:
Of 226 patients included in the study, 131 (58.0%) patients died before hospital discharge. Squamous cell carcinoma was more frequent than adenocarcinoma, and 124 (54.9%) patients had metastatic cancer. The main reasons for admission were sepsis/septic shock and acute respiratory failure. Mechanical ventilation (OR = 6.18; 95%CI 2.86 – 13.35) and metastatic disease (OR = 7.10; 95%CI 3.35 – 15.05) were independently associated with in-hospital mortality.
Conclusion:
In this cohort of patients with esophageal cancer admitted to intensive care units with acute illness, the in-hospital mortality rate was very high. The requirement for invasive mechanical ventilation and metastatic disease were independent prognostic factors and should be considered in discussions about the short-term outcomes of these patients.
Keywords:Critical careCritical care outcomesepidemiologyEsophageal neoplasmsMortalityPrognosisRespiration, artificialSee more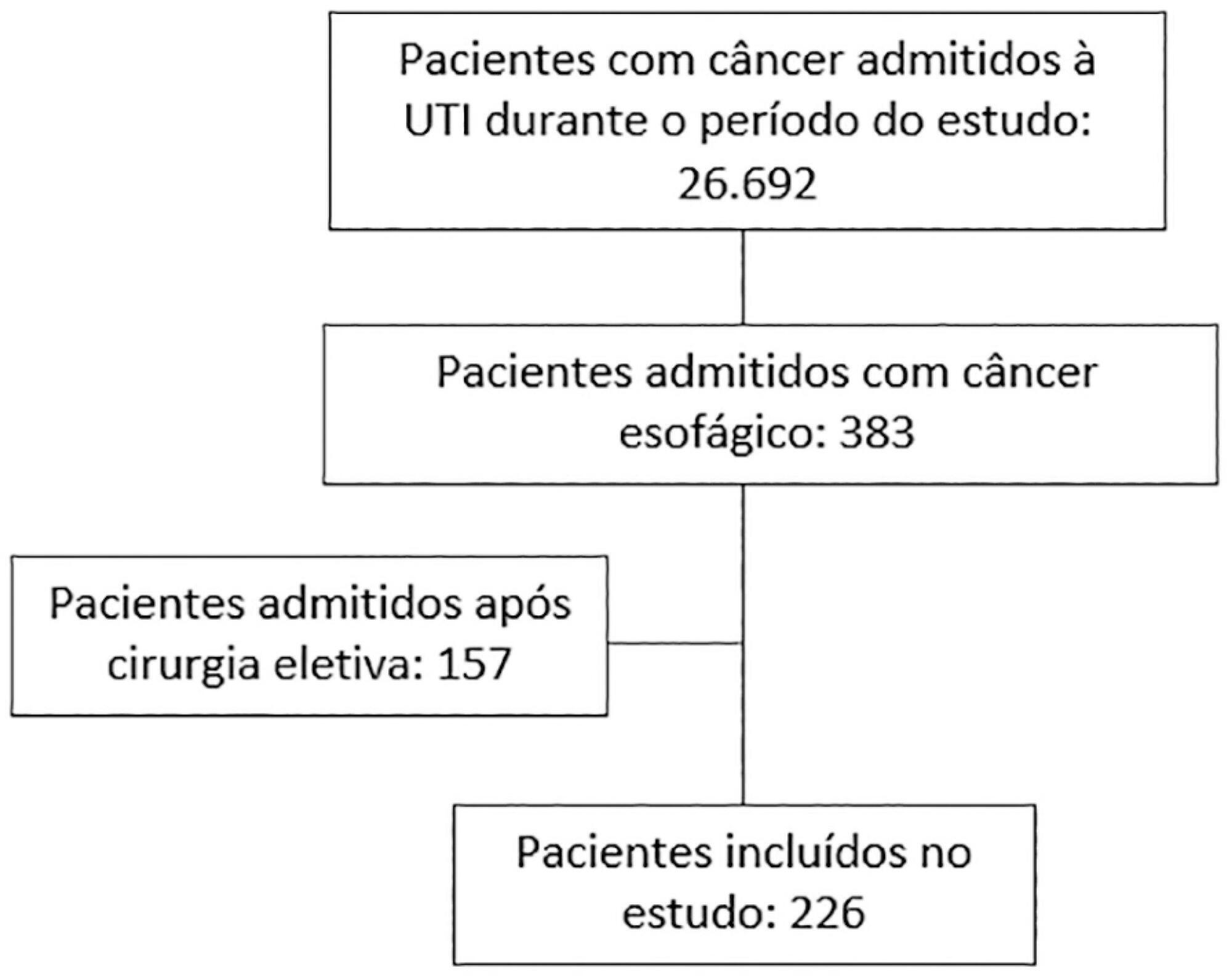
-
Original Article
Frequency and characterization of the use of cuffed tracheal tubes in neonatal and pediatric intensive care units in Brazil
- João Paulo Berti Buzzi Rodrigues,
- Suzi Laine Longo dos Santos Bacci,
- Janser Moura Pereira,
- Cíntia Johnston,
- Vivian Mara Gonçalves de Oliveira Azevedo
Abstract
Original ArticleFrequency and characterization of the use of cuffed tracheal tubes in neonatal and pediatric intensive care units in Brazil
Rev Bras Ter Intensiva. 2020;32(2):235-243
DOI 10.5935/0103-507X.20200038
- João Paulo Berti Buzzi Rodrigues,
- Suzi Laine Longo dos Santos Bacci,
- Janser Moura Pereira,
- Cíntia Johnston,
- Vivian Mara Gonçalves de Oliveira Azevedo
Views0ABSTRACT
Objective:
To identify the neonatal, pediatric and mixed (neonatal and pediatric) intensive care units in Brazil that use cuffed tracheal tubes in clinical practice and to describe the characteristics related to the use of protocols and monitoring.
Methods:
To identify the intensive care units in Brazil, the Ministry of Health’s National Registry of Health Facilities was accessed, and information was collected on 693 registered intensive care units. This was an analytical cross-sectional survey conducted through electronic questionnaires sent to 298 neonatal, pediatric and mixed intensive care units in Brazil.
Results:
This study analyzed 146 questionnaires (49.3% from neonatal intensive care units, 35.6% from pediatric intensive care units and 15.1% from mixed pediatric intensive care units). Most of the participating units (78/146) used cuffed tracheal tubes, with a predominance of use in pediatric intensive care units (52/78). Most of the units that used cuffed tracheal tubes applied a cuff pressure monitoring protocol (45/78). The use of cuff monitoring protocols was observed in intensive care units with a physical therapy service exclusive to the unit (38/61) and in those with a physical therapist present 24 hours/day (25/45). The most frequent cause of extubation failure related to the use of cuffed tracheal tubes in pediatric intensive care units was upper airway obstruction.
Conclusion:
In this survey, the use of cuffed tracheal tubes and the application of a cuff pressure monitoring protocol was predominant in pediatric intensive care units. The use of a monitoring protocol was more common in intensive care units that had a physical therapist who was exclusive to the unit and was present 24 hours/day.
Keywords:CannulaInfantIntensive care units, neonatalIntensive care units, pediatricIntubation, intratracheal/instrumentationNewbornTracheaSee moreViews0Abstract
Original ArticleFrequency and characterization of the use of cuffed tracheal tubes in neonatal and pediatric intensive care units in Brazil
Rev Bras Ter Intensiva. 2020;32(2):235-243
DOI 10.5935/0103-507X.20200038
- João Paulo Berti Buzzi Rodrigues,
- Suzi Laine Longo dos Santos Bacci,
- Janser Moura Pereira,
- Cíntia Johnston,
- Vivian Mara Gonçalves de Oliveira Azevedo
Views0ABSTRACT
Objective:
To identify the neonatal, pediatric and mixed (neonatal and pediatric) intensive care units in Brazil that use cuffed tracheal tubes in clinical practice and to describe the characteristics related to the use of protocols and monitoring.
Methods:
To identify the intensive care units in Brazil, the Ministry of Health’s National Registry of Health Facilities was accessed, and information was collected on 693 registered intensive care units. This was an analytical cross-sectional survey conducted through electronic questionnaires sent to 298 neonatal, pediatric and mixed intensive care units in Brazil.
Results:
This study analyzed 146 questionnaires (49.3% from neonatal intensive care units, 35.6% from pediatric intensive care units and 15.1% from mixed pediatric intensive care units). Most of the participating units (78/146) used cuffed tracheal tubes, with a predominance of use in pediatric intensive care units (52/78). Most of the units that used cuffed tracheal tubes applied a cuff pressure monitoring protocol (45/78). The use of cuff monitoring protocols was observed in intensive care units with a physical therapy service exclusive to the unit (38/61) and in those with a physical therapist present 24 hours/day (25/45). The most frequent cause of extubation failure related to the use of cuffed tracheal tubes in pediatric intensive care units was upper airway obstruction.
Conclusion:
In this survey, the use of cuffed tracheal tubes and the application of a cuff pressure monitoring protocol was predominant in pediatric intensive care units. The use of a monitoring protocol was more common in intensive care units that had a physical therapist who was exclusive to the unit and was present 24 hours/day.
Keywords:CannulaInfantIntensive care units, neonatalIntensive care units, pediatricIntubation, intratracheal/instrumentationNewbornTracheaSee more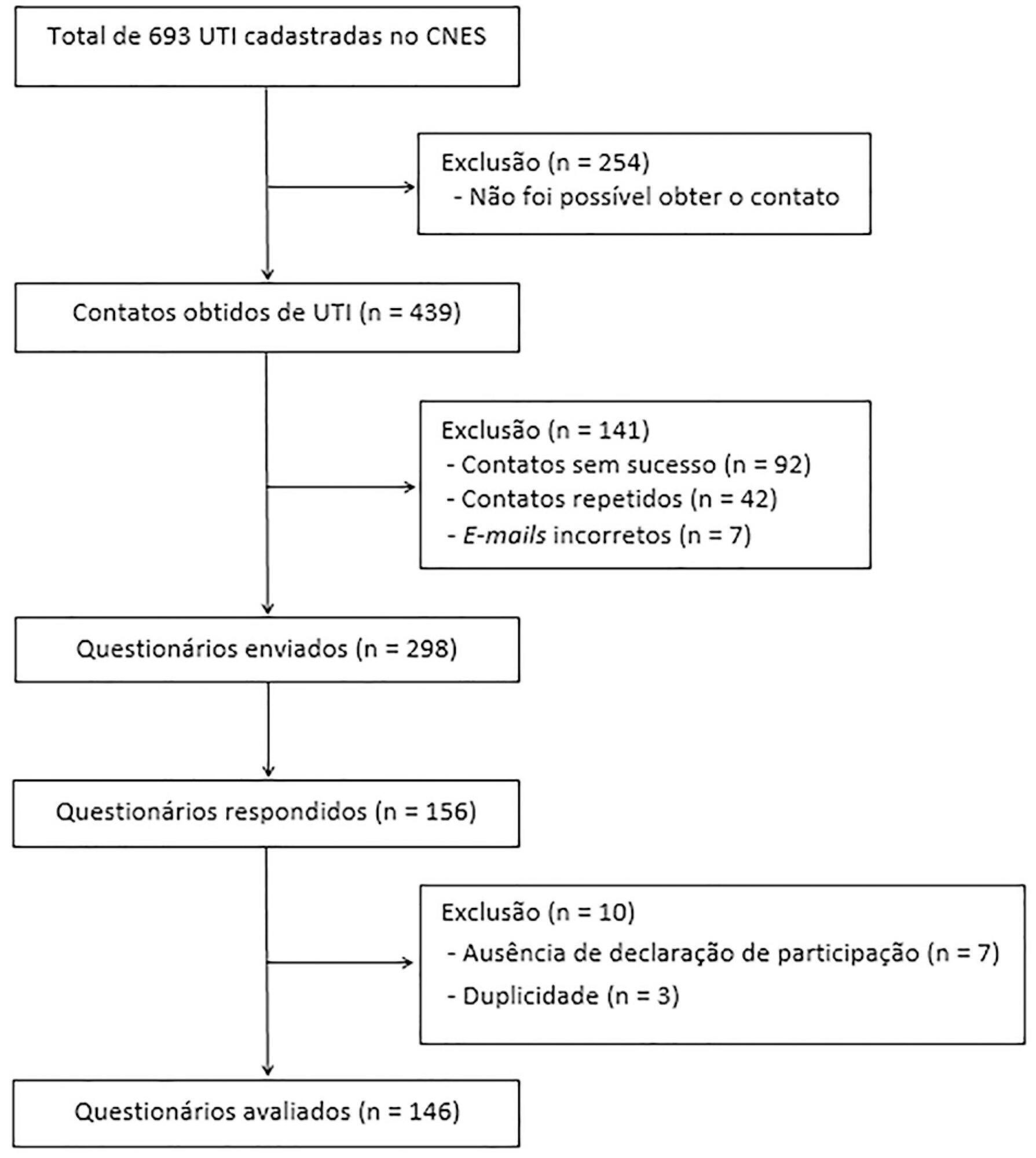
-
Original Article
Time to clearance of abdominal septic focus and mortality in patients with sepsis
- Rafael Barberena Moraes ,
- Thiago Ferreira Serafini,
- Josi Vidart,
- Miriane Melo Silveira Moretti,
- Jaqueline Sangiogo Haas, [ … ],
- Gilberto Friedman
Abstract
Original ArticleTime to clearance of abdominal septic focus and mortality in patients with sepsis
Rev Bras Ter Intensiva. 2020;32(2):245-250
DOI 10.5935/0103-507X.20200029
- Rafael Barberena Moraes ,
- Thiago Ferreira Serafini,
- Josi Vidart,
- Miriane Melo Silveira Moretti,
- Jaqueline Sangiogo Haas,
- Alan Pagnoncelli,
- Marco Aurélio Abreu Azeredo,
- Gilberto Friedman
Views1See moreABSTRACT
Objective:
To assess the relationship between time to focus clearance and hospital mortality in patients with sepsis and septic shock.
Methods:
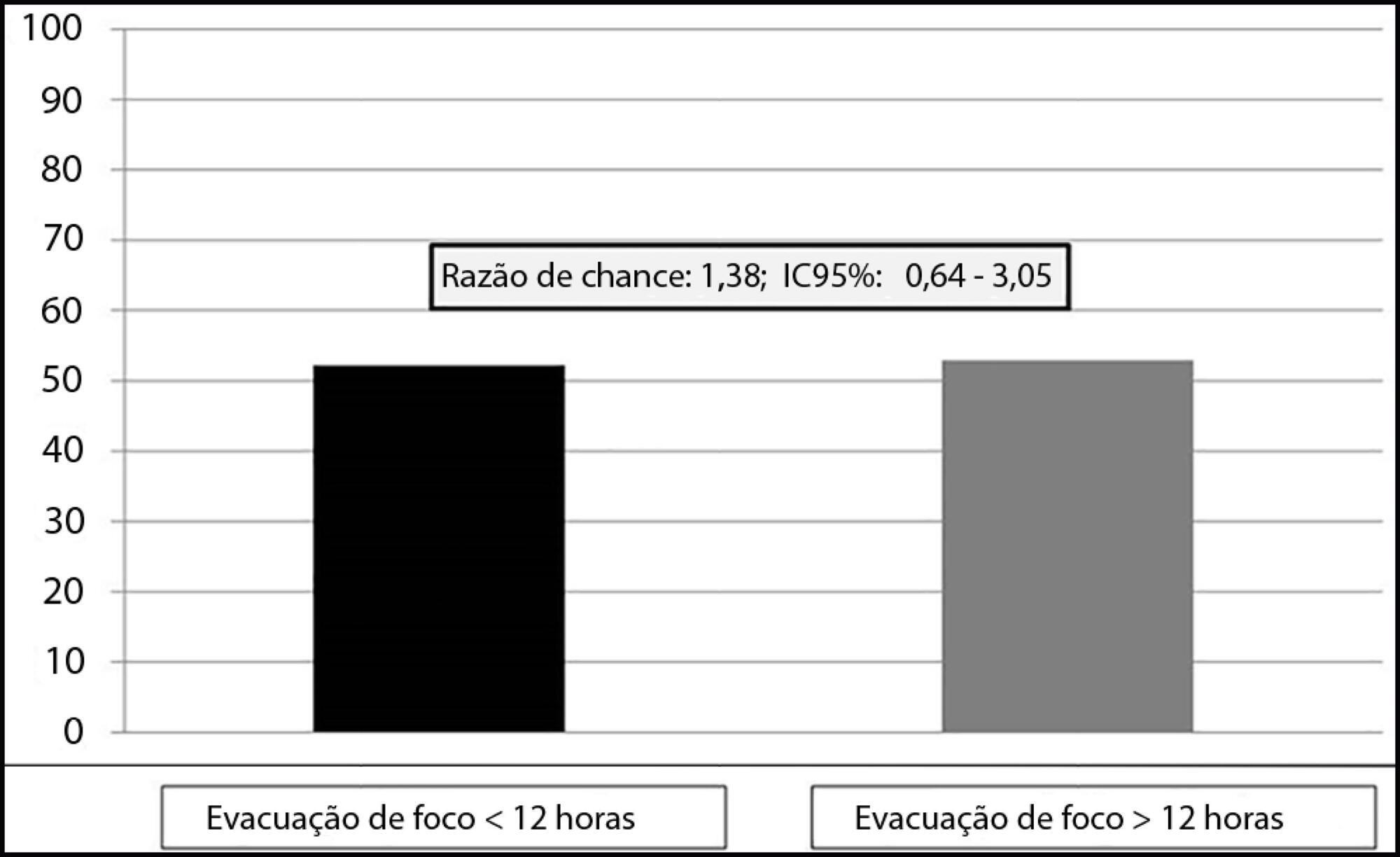
This was an observational, single-center study with a retrospective analysis of the time to clearance of abdominal septic focus. Patients were classified according to the time to focus clearance into an early (≤ 12 hours) or delayed (> 12 hours) group.
Results:
A total of 135 patients were evaluated. There was no association between time to focus clearance and hospital mortality (≤ 12 hours versus > 12 hours): 52.3% versus 52.9%, with p = 0.137.
Conclusion:
There was no difference in hospital mortality among patients with sepsis or septic shock who had an infectious focus evacuated before or after 12 hours after the diagnosis of sepsis.
Views1Abstract
Original ArticleTime to clearance of abdominal septic focus and mortality in patients with sepsis
Rev Bras Ter Intensiva. 2020;32(2):245-250
DOI 10.5935/0103-507X.20200029
- Rafael Barberena Moraes ,
- Thiago Ferreira Serafini,
- Josi Vidart,
- Miriane Melo Silveira Moretti,
- Jaqueline Sangiogo Haas,
- Alan Pagnoncelli,
- Marco Aurélio Abreu Azeredo,
- Gilberto Friedman
Views1See moreABSTRACT
Objective:
To assess the relationship between time to focus clearance and hospital mortality in patients with sepsis and septic shock.
Methods:
This was an observational, single-center study with a retrospective analysis of the time to clearance of abdominal septic focus. Patients were classified according to the time to focus clearance into an early (≤ 12 hours) or delayed (> 12 hours) group.
Results:
A total of 135 patients were evaluated. There was no association between time to focus clearance and hospital mortality (≤ 12 hours versus > 12 hours): 52.3% versus 52.9%, with p = 0.137.
Conclusion:
There was no difference in hospital mortality among patients with sepsis or septic shock who had an infectious focus evacuated before or after 12 hours after the diagnosis of sepsis.
- Rafael Barberena Moraes
-
Original Article
Burnout syndrome among healthcare professionals in intensive care units: a cross-sectional population-based study
- Maria Emília Miranda Alvares,
- Erika Barbara Abreu Fonseca Thomaz,
- Zeni Carvalho Lamy,
- Rachel Vilela de Abreu Haickel Nina,
- Marina Uchoa Lopes Pereira , [ … ],
- João Batista Santos Garcia
Abstract
Original ArticleBurnout syndrome among healthcare professionals in intensive care units: a cross-sectional population-based study
Rev Bras Ter Intensiva. 2020;32(2):251-260
DOI 10.5935/0103-507X.20200036
- Maria Emília Miranda Alvares,
- Erika Barbara Abreu Fonseca Thomaz,
- Zeni Carvalho Lamy,
- Rachel Vilela de Abreu Haickel Nina,
- Marina Uchoa Lopes Pereira ,
- João Batista Santos Garcia
Views0ABSTRACT
Objective:
To assess the prevalence of and factors associated with Burnout syndrome among intensive care unit professionals.
Methods:
In this cross-sectional population-based study, a questionnaire assessing sociodemographic, behavioral, and occupational data was administered to 241 nurses and physicians working in 17 public intensive care units in São Luis (MA), Brazil. The Maslach Burnout Inventory – Human Services Survey was used to identify Burnout syndrome based on Maslach’s and Grunfeld’s criteria. The prevalence of each dimension of the syndrome was estimated with a 95% confidence interval. Associations were estimated by the odds ratios via multiple logistic regression analyses (α = 5%).
Results:
The prevalence of Burnout syndrome was 0.41% (0.01 – 2.29) according to Maslach’s criteria and 36.9% (30.82 – 43.36) according to Grunfeld’s criteria. Infant intensive care unit professionals were more likely to develop emotional exhaustion than other intensive care professionals (OR = 3.16). Respondents over the age of 35 were less likely to develop emotional exhaustion (OR = 0.32) and depersonalization (OR = 0.06). Longer working hours in intensive care units were associated with a reduced sense of personal accomplishment (OR = 1.13). Among nurses, males had a lower sense of professional accomplishment, and not exercising regularly was associated with more emotional exhaustion and less depersonalization. Among physicians, working in infant and cardiology intensive care units made them less likely to have a reduced sense of personal accomplishment, and physicians without a postgraduate degree who worked in intensive care units had a higher chance of having a lower sense of personal accomplishment.
Conclusion:
This study demonstrated the low prevalence of Burnout syndrome. Most of the professionals reported low levels for each dimension of Burnout, including low levels of emotional exhaustion, low levels of depersonalization, and a lower likelihood of having a reduced sense of personal accomplishment. Nurses and physicians have different characteristics associated with Burnout syndrome.
Keywords:Burnout, psychologicalCritical careHealth personnelIntensive care unitsStress, psychologicalSee moreViews0Abstract
Original ArticleBurnout syndrome among healthcare professionals in intensive care units: a cross-sectional population-based study
Rev Bras Ter Intensiva. 2020;32(2):251-260
DOI 10.5935/0103-507X.20200036
- Maria Emília Miranda Alvares,
- Erika Barbara Abreu Fonseca Thomaz,
- Zeni Carvalho Lamy,
- Rachel Vilela de Abreu Haickel Nina,
- Marina Uchoa Lopes Pereira ,
- João Batista Santos Garcia
Views0ABSTRACT
Objective:
To assess the prevalence of and factors associated with Burnout syndrome among intensive care unit professionals.
Methods:
In this cross-sectional population-based study, a questionnaire assessing sociodemographic, behavioral, and occupational data was administered to 241 nurses and physicians working in 17 public intensive care units in São Luis (MA), Brazil. The Maslach Burnout Inventory – Human Services Survey was used to identify Burnout syndrome based on Maslach’s and Grunfeld’s criteria. The prevalence of each dimension of the syndrome was estimated with a 95% confidence interval. Associations were estimated by the odds ratios via multiple logistic regression analyses (α = 5%).
Results:
The prevalence of Burnout syndrome was 0.41% (0.01 – 2.29) according to Maslach’s criteria and 36.9% (30.82 – 43.36) according to Grunfeld’s criteria. Infant intensive care unit professionals were more likely to develop emotional exhaustion than other intensive care professionals (OR = 3.16). Respondents over the age of 35 were less likely to develop emotional exhaustion (OR = 0.32) and depersonalization (OR = 0.06). Longer working hours in intensive care units were associated with a reduced sense of personal accomplishment (OR = 1.13). Among nurses, males had a lower sense of professional accomplishment, and not exercising regularly was associated with more emotional exhaustion and less depersonalization. Among physicians, working in infant and cardiology intensive care units made them less likely to have a reduced sense of personal accomplishment, and physicians without a postgraduate degree who worked in intensive care units had a higher chance of having a lower sense of personal accomplishment.
Conclusion:
This study demonstrated the low prevalence of Burnout syndrome. Most of the professionals reported low levels for each dimension of Burnout, including low levels of emotional exhaustion, low levels of depersonalization, and a lower likelihood of having a reduced sense of personal accomplishment. Nurses and physicians have different characteristics associated with Burnout syndrome.
Keywords:Burnout, psychologicalCritical careHealth personnelIntensive care unitsStress, psychologicalSee more -
Original Article
Functional deficit in children with congenital heart disease undergoing surgical correction after intensive care unit discharge
- Eloisa da Rosa Schunck ,
- Camila Wohlgemuth Schaan ,
- Gabriela Alves Pereira ,
- Nathália Vieira Rosa ,
- Tatiana Coser Normann , [ … ],
- Janice Luisa Lukrafka
Abstract
Original ArticleFunctional deficit in children with congenital heart disease undergoing surgical correction after intensive care unit discharge
Rev Bras Ter Intensiva. 2020;32(2):261-267
DOI 10.5935/0103-507X.20200042
- Eloisa da Rosa Schunck ,
- Camila Wohlgemuth Schaan ,
- Gabriela Alves Pereira ,
- Nathália Vieira Rosa ,
- Tatiana Coser Normann ,
- Claudia Pires Ricachinevsky ,
- Caroline Tozzi Reppold ,
- Renata Salatti Ferrari ,
- Janice Luisa Lukrafka
Views0See moreAbstract
Objective:
To evaluate the functional status of pediatric patients undergoing congenital heart surgery after discharge from the intensive care unit, and to evaluate the correlations among clinical variables, functional status and surgical risk.
Methods:
Cross-sectional study including patients aged 1 month to less than 18 years undergoing congenital heart surgery between October 2017 and May 2018. Functional outcome was assessed by the Functional Status Scale, surgical risk classification was determined using the Risk Adjustment for Congenital Heart Surgery-1 (RACHS-1), and clinical variables were collected from electronic medical records.
Results:
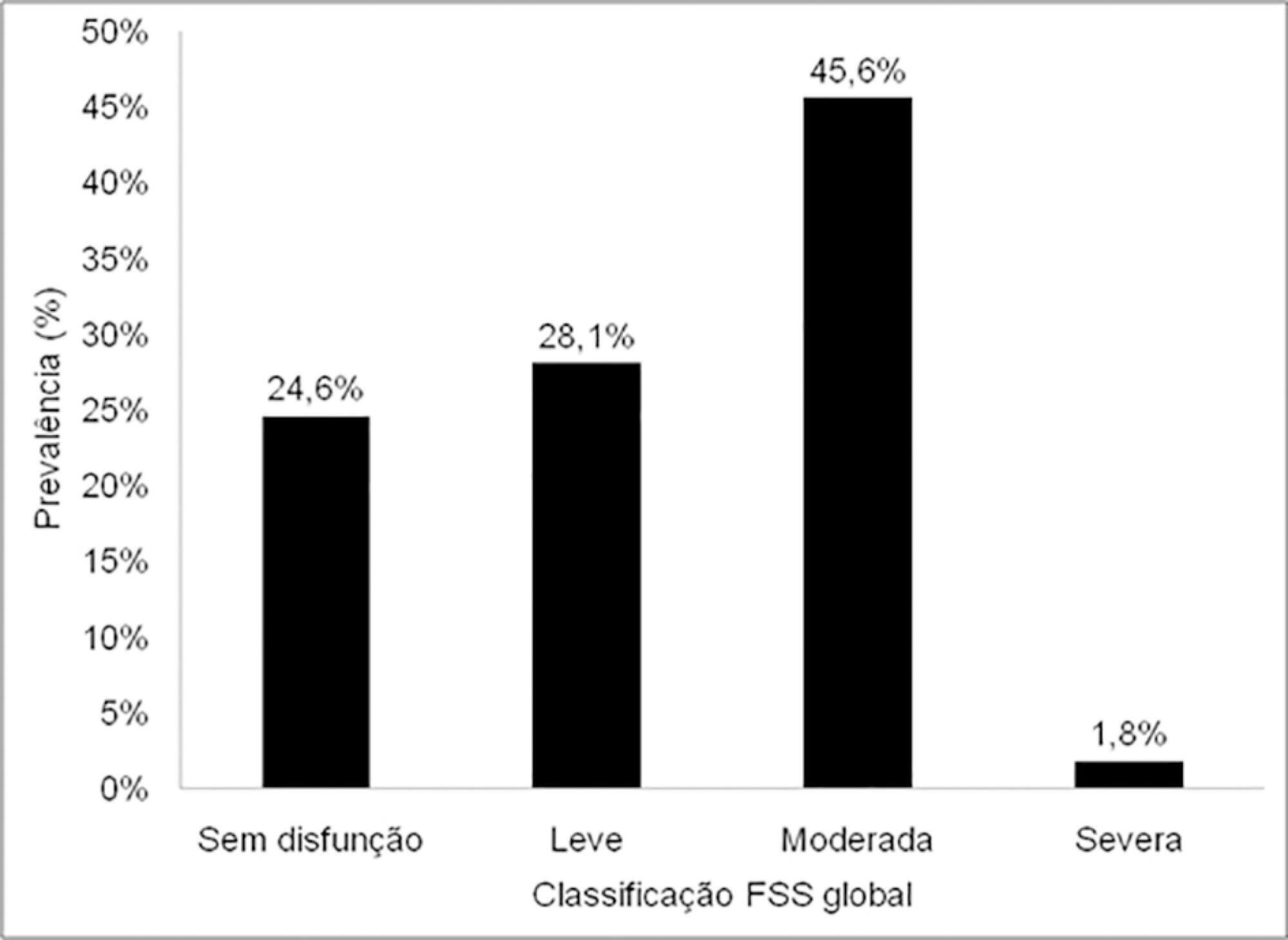
The sample comprised 57 patients with a median age of 7 months (2 – 17); 54.4% were male, and 75.5% showed dysfunction, which was moderate in 45.6% of the cases. RACHS-1 category > 3 was observed in 47% of the sample, indicating higher surgical risk. There was a correlation between functional deficit and younger age, longer duration of invasive mechanical ventilation and longer intensive care unit stay. Moreover, greater functional deficit was observed among patients classified as RACHS-1 category > 3.
Conclusion:
The prevalence of functional deficit was high among children and adolescents with congenital heart disease after cardiac surgery. Higher surgical risk, longer duration of invasive mechanical ventilation, longer intensive care unit stay and younger age were correlated with worse functional status.
Views0Abstract
Original ArticleFunctional deficit in children with congenital heart disease undergoing surgical correction after intensive care unit discharge
Rev Bras Ter Intensiva. 2020;32(2):261-267
DOI 10.5935/0103-507X.20200042
- Eloisa da Rosa Schunck ,
- Camila Wohlgemuth Schaan ,
- Gabriela Alves Pereira ,
- Nathália Vieira Rosa ,
- Tatiana Coser Normann ,
- Claudia Pires Ricachinevsky ,
- Caroline Tozzi Reppold ,
- Renata Salatti Ferrari ,
- Janice Luisa Lukrafka
Views0See moreAbstract
Objective:
To evaluate the functional status of pediatric patients undergoing congenital heart surgery after discharge from the intensive care unit, and to evaluate the correlations among clinical variables, functional status and surgical risk.
Methods:
Cross-sectional study including patients aged 1 month to less than 18 years undergoing congenital heart surgery between October 2017 and May 2018. Functional outcome was assessed by the Functional Status Scale, surgical risk classification was determined using the Risk Adjustment for Congenital Heart Surgery-1 (RACHS-1), and clinical variables were collected from electronic medical records.
Results:
The sample comprised 57 patients with a median age of 7 months (2 – 17); 54.4% were male, and 75.5% showed dysfunction, which was moderate in 45.6% of the cases. RACHS-1 category > 3 was observed in 47% of the sample, indicating higher surgical risk. There was a correlation between functional deficit and younger age, longer duration of invasive mechanical ventilation and longer intensive care unit stay. Moreover, greater functional deficit was observed among patients classified as RACHS-1 category > 3.
Conclusion:
The prevalence of functional deficit was high among children and adolescents with congenital heart disease after cardiac surgery. Higher surgical risk, longer duration of invasive mechanical ventilation, longer intensive care unit stay and younger age were correlated with worse functional status.
- Eloisa da Rosa Schunck
-
Original Article
Practices for promoting sleep in intensive care units in Brazil: a national survey
Rev Bras Ter Intensiva. 2020;32(2):268-276
Abstract
Original ArticlePractices for promoting sleep in intensive care units in Brazil: a national survey
Rev Bras Ter Intensiva. 2020;32(2):268-276
DOI 10.5935/0103-507X.20200043
Views0See moreABSTRACT
Objective:
To conduct a national survey of intensive care professionals to identify the practices for promoting sleep in adult intensive care units in Brazil and describe the professionals’ perceptions of the importance of sleep for patients.
Methods:
An electronic questionnaire was distributed by the clinical research cooperation network of the Associação de Medicina Intensiva Brasileira and by the Brazilian Research in Intensive Care Network to physicians and nurses registered with the association. The questionnaire evaluated the profile of the respondents, the profile of their intensive care units, whether protocols for promoting sleep were present, the pharmacological and nonpharmacological measures typically employed in the unit, and the professionals’ perceptions regarding sleep in critically ill patients.
Results:
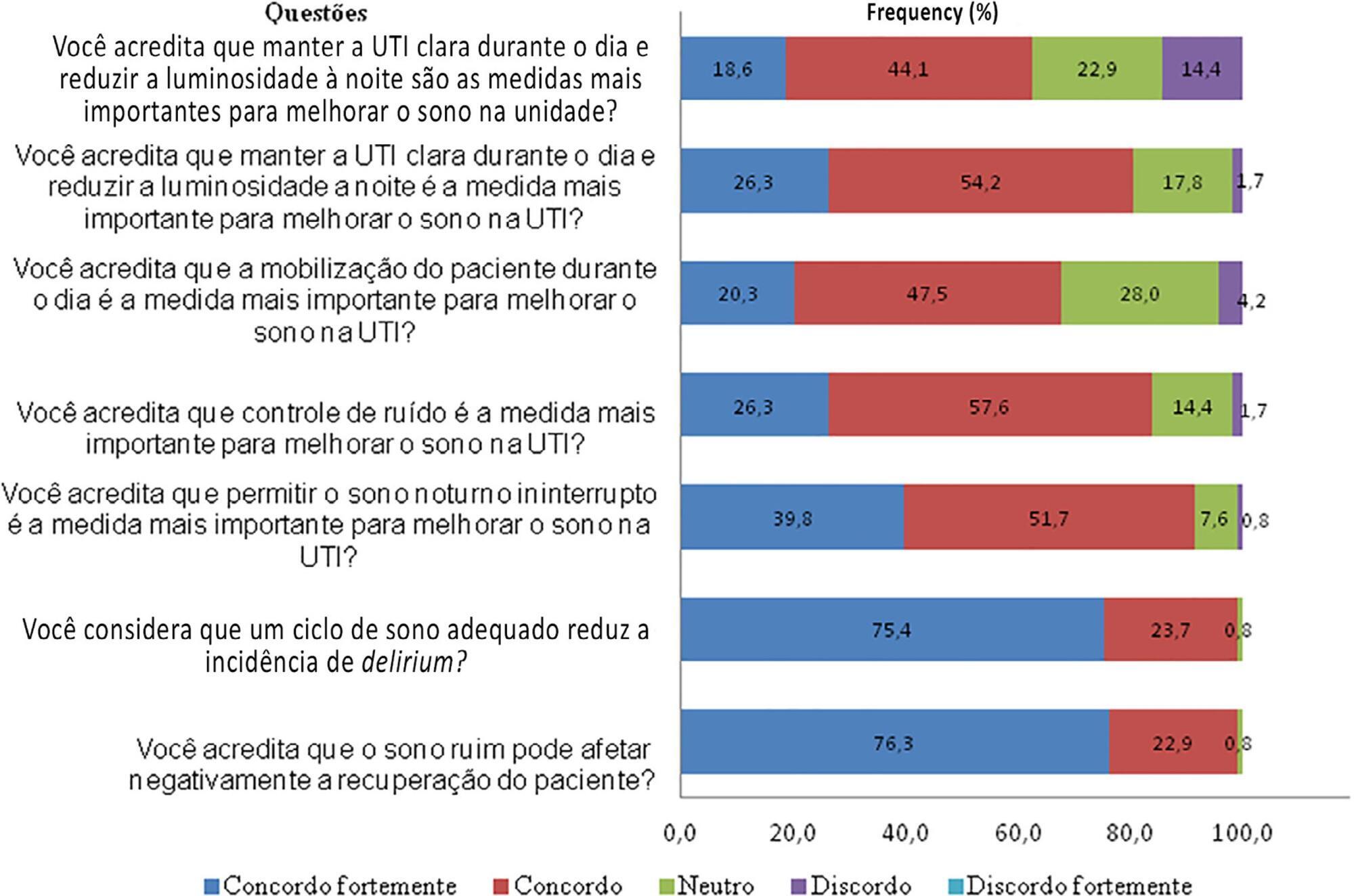
A total of 118 questionnaires were evaluated. The Southeast region of the country was the most represented (50 questionnaires, 42.4%). The majority of units had a clinical-surgical profile (93 questionnaires; 78.8%), and 26 had a continuous visitation policy (22.0%). Only 18 intensive care units (15.3%) reported having protocols for promoting sleep. The most cited measure for sleep promotion was reducing light during the night (95 questionnaires; 80.5%), which was more often performed in private intensive care units. Almost all of the responders (99%) believed that poor-quality sleep has a negative impact on patient recovery.
Conclusion:
The responses to this Brazilian survey revealed that few intensive care units had a program for promoting sleep, although almost all participants recognized the importance of sleep in patient recovery.
Views0Abstract
Original ArticlePractices for promoting sleep in intensive care units in Brazil: a national survey
Rev Bras Ter Intensiva. 2020;32(2):268-276
DOI 10.5935/0103-507X.20200043
Views0See moreABSTRACT
Objective:
To conduct a national survey of intensive care professionals to identify the practices for promoting sleep in adult intensive care units in Brazil and describe the professionals’ perceptions of the importance of sleep for patients.
Methods:
An electronic questionnaire was distributed by the clinical research cooperation network of the Associação de Medicina Intensiva Brasileira and by the Brazilian Research in Intensive Care Network to physicians and nurses registered with the association. The questionnaire evaluated the profile of the respondents, the profile of their intensive care units, whether protocols for promoting sleep were present, the pharmacological and nonpharmacological measures typically employed in the unit, and the professionals’ perceptions regarding sleep in critically ill patients.
Results:
A total of 118 questionnaires were evaluated. The Southeast region of the country was the most represented (50 questionnaires, 42.4%). The majority of units had a clinical-surgical profile (93 questionnaires; 78.8%), and 26 had a continuous visitation policy (22.0%). Only 18 intensive care units (15.3%) reported having protocols for promoting sleep. The most cited measure for sleep promotion was reducing light during the night (95 questionnaires; 80.5%), which was more often performed in private intensive care units. Almost all of the responders (99%) believed that poor-quality sleep has a negative impact on patient recovery.
Conclusion:
The responses to this Brazilian survey revealed that few intensive care units had a program for promoting sleep, although almost all participants recognized the importance of sleep in patient recovery.
-
Original Article
Pharmacokinetics of micafungin in patients treated with extracorporeal membrane oxygenation: an observational prospective study
- Marta López-Sánchez ,
- Ignacio Moreno-Puigdollers,
- Maria Isabel Rubio-López,
- Iratxe Zarragoikoetxea-Jauregui,
- Rosario Vicente-Guillén, [ … ],
- Maria Pilar Argente-Navarro
Abstract
Original ArticlePharmacokinetics of micafungin in patients treated with extracorporeal membrane oxygenation: an observational prospective study
Rev Bras Ter Intensiva. 2020;32(2):277-283
DOI 10.5935/0103-507X.20200044
- Marta López-Sánchez ,
- Ignacio Moreno-Puigdollers,
- Maria Isabel Rubio-López,
- Iratxe Zarragoikoetxea-Jauregui,
- Rosario Vicente-Guillén,
- Maria Pilar Argente-Navarro
Views0See moreABSTRACT
Objective:
To determine micafungin plasma levels and pharmacokinetic behavior in patients treated with extracorporeal membrane oxygenation.
Methods:
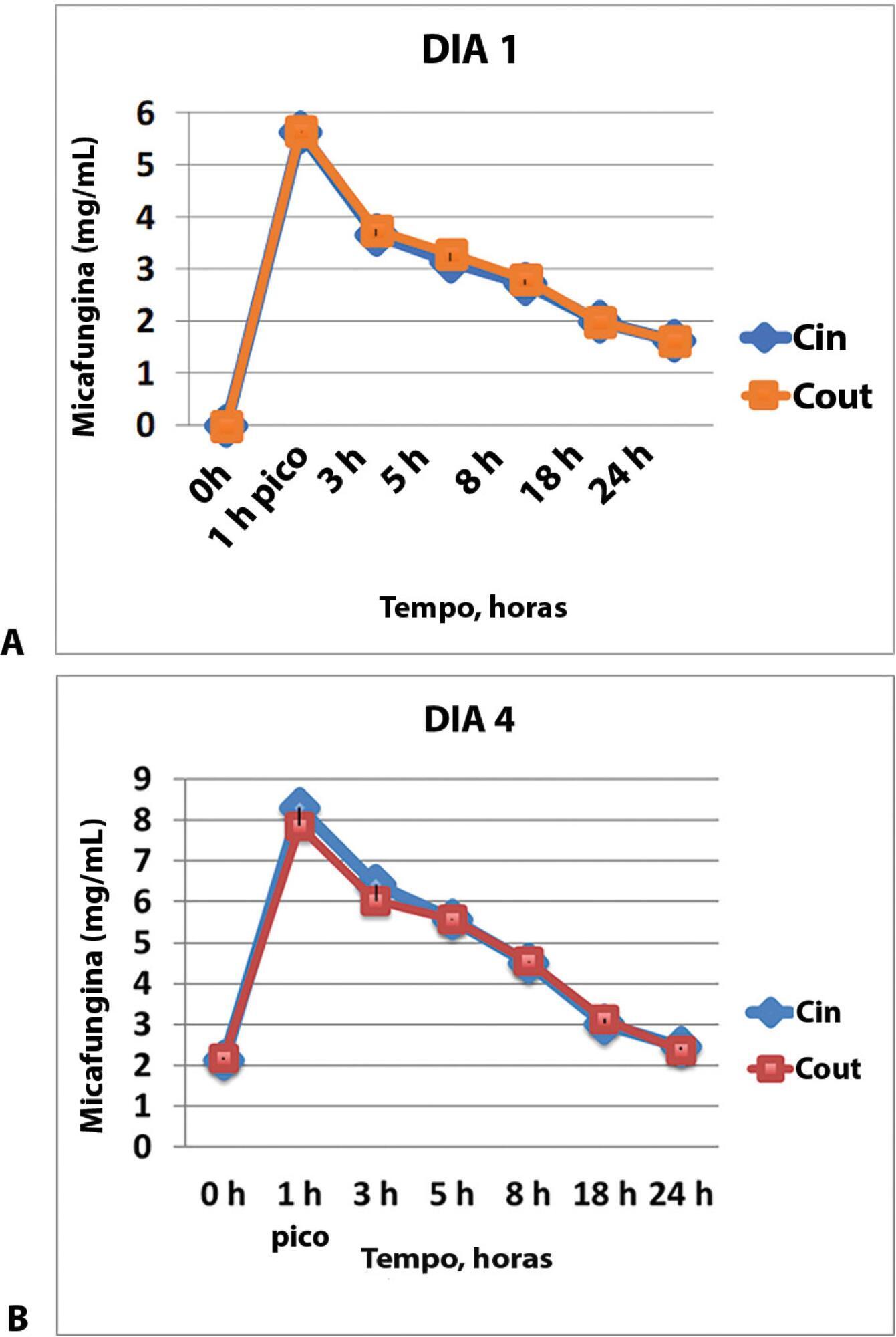
The samples were taken through an access point before and after the membrane in two tertiary hospitals in Spain. The times for the calculation of pharmacokinetic curves were before the administration of the drug and 1, 3, 5, 8, 18 and 24 hours after the beginning of the infusion on days one and four. The area under the curve, drug clearance, volume of distribution and plasma half-life time with a noncompartmental pharmacokinetic data analysis were calculated.
Results:
The pharmacokinetics of the values analyzed on the first and fourth day of treatment did not show any concentration difference between the samples taken before the membrane (Cin) and those taken after the membrane (Cout), and the pharmacokinetic behavior was similar with different organ failures. The area under the curve (AUC) before the membrane on day 1 was 62.1 (95%CI 52.8 – 73.4) and the AUC after the membrane on this day was 63.4 (95%CI 52.4 – 76.7), p = 0.625. The AUC before the membrane on day 4 was 102.4 (95%CI 84.7 – 142.8) and the AUC was 100.9 (95%CI 78.2 – 138.8), p = 0.843.
Conclusion:
The pharmacokinetic parameters of micafungin were not significantly altered.
Views0Abstract
Original ArticlePharmacokinetics of micafungin in patients treated with extracorporeal membrane oxygenation: an observational prospective study
Rev Bras Ter Intensiva. 2020;32(2):277-283
DOI 10.5935/0103-507X.20200044
- Marta López-Sánchez ,
- Ignacio Moreno-Puigdollers,
- Maria Isabel Rubio-López,
- Iratxe Zarragoikoetxea-Jauregui,
- Rosario Vicente-Guillén,
- Maria Pilar Argente-Navarro
Views0See moreABSTRACT
Objective:
To determine micafungin plasma levels and pharmacokinetic behavior in patients treated with extracorporeal membrane oxygenation.
Methods:
The samples were taken through an access point before and after the membrane in two tertiary hospitals in Spain. The times for the calculation of pharmacokinetic curves were before the administration of the drug and 1, 3, 5, 8, 18 and 24 hours after the beginning of the infusion on days one and four. The area under the curve, drug clearance, volume of distribution and plasma half-life time with a noncompartmental pharmacokinetic data analysis were calculated.
Results:
The pharmacokinetics of the values analyzed on the first and fourth day of treatment did not show any concentration difference between the samples taken before the membrane (Cin) and those taken after the membrane (Cout), and the pharmacokinetic behavior was similar with different organ failures. The area under the curve (AUC) before the membrane on day 1 was 62.1 (95%CI 52.8 – 73.4) and the AUC after the membrane on this day was 63.4 (95%CI 52.4 – 76.7), p = 0.625. The AUC before the membrane on day 4 was 102.4 (95%CI 84.7 – 142.8) and the AUC was 100.9 (95%CI 78.2 – 138.8), p = 0.843.
Conclusion:
The pharmacokinetic parameters of micafungin were not significantly altered.
- Marta López-Sánchez
-
Original Article
Outcomes of ventilatory asynchrony in patients with inspiratory effort
- Frank Daniel Martos-Benítez ,
- Yairén Domínguez-Valdés,
- Dailé Burgos-Aragüez,
- Hilev Larrondo-Muguercia,
- Versis Orama-Requejo, [ … ],
- Iraida González-Martínez
Abstract
Original ArticleOutcomes of ventilatory asynchrony in patients with inspiratory effort
Rev Bras Ter Intensiva. 2020;32(2):284-294
DOI 10.5935/0103-507X.20200045
- Frank Daniel Martos-Benítez ,
- Yairén Domínguez-Valdés,
- Dailé Burgos-Aragüez,
- Hilev Larrondo-Muguercia,
- Versis Orama-Requejo,
- Karla Ximena Lara-Ponce,
- Iraida González-Martínez
Views0Abstract
Objective:
To identify the relationship of patient-ventilator asynchrony with the level of sedation and hemogasometric and clinical results.
Methods:
This was a prospective study of 122 patients admitted to the intensive care unit who underwent > 24 hours of invasive mechanical ventilation with inspiratory effort. In the first 7 days of ventilation, patient-ventilator asynchrony was evaluated daily for 30 minutes. Severe patient-ventilator asynchrony was defined as an asynchrony index > 10%.
Results:
A total of 339,652 respiratory cycles were evaluated in 504 observations. The mean asynchrony index was 37.8% (standard deviation 14.1 – 61.5%). The prevalence of severe patient-ventilator asynchrony was 46.6%. The most frequent patient-ventilator asynchronies were ineffective trigger (13.3%), autotrigger (15.3%), insufficient flow (13.5%), and delayed cycling (13.7%). Severe patient-ventilator asynchrony was related to the level of sedation (ineffective trigger: p = 0.020; insufficient flow: p = 0.016; premature cycling: p = 0.023) and the use of midazolam (p = 0.020). Severe patient-ventilator asynchrony was also associated with hemogasometric changes. The persistence of severe patient-ventilator asynchrony was an independent risk factor for failure of the spontaneous breathing test, ventilation time, ventilator-associated pneumonia, organ dysfunction, mortality in the intensive care unit, and length of stay in the intensive care unit.
Conclusion:
Patient-ventilator asynchrony is a frequent disorder in critically ill patients with inspiratory effort. The patient’s interaction with the ventilator should be optimized to improve hemogasometric parameters and clinical results. Further studies are required to confirm these results.
Keywords:Intensive care unitsInteractive ventilatory supportMortalityPhysiological monitoringRespiration, artificial/methodsSee moreViews0Abstract
Original ArticleOutcomes of ventilatory asynchrony in patients with inspiratory effort
Rev Bras Ter Intensiva. 2020;32(2):284-294
DOI 10.5935/0103-507X.20200045
- Frank Daniel Martos-Benítez ,
- Yairén Domínguez-Valdés,
- Dailé Burgos-Aragüez,
- Hilev Larrondo-Muguercia,
- Versis Orama-Requejo,
- Karla Ximena Lara-Ponce,
- Iraida González-Martínez
Views0Abstract
Objective:
To identify the relationship of patient-ventilator asynchrony with the level of sedation and hemogasometric and clinical results.
Methods:
This was a prospective study of 122 patients admitted to the intensive care unit who underwent > 24 hours of invasive mechanical ventilation with inspiratory effort. In the first 7 days of ventilation, patient-ventilator asynchrony was evaluated daily for 30 minutes. Severe patient-ventilator asynchrony was defined as an asynchrony index > 10%.
Results:
A total of 339,652 respiratory cycles were evaluated in 504 observations. The mean asynchrony index was 37.8% (standard deviation 14.1 – 61.5%). The prevalence of severe patient-ventilator asynchrony was 46.6%. The most frequent patient-ventilator asynchronies were ineffective trigger (13.3%), autotrigger (15.3%), insufficient flow (13.5%), and delayed cycling (13.7%). Severe patient-ventilator asynchrony was related to the level of sedation (ineffective trigger: p = 0.020; insufficient flow: p = 0.016; premature cycling: p = 0.023) and the use of midazolam (p = 0.020). Severe patient-ventilator asynchrony was also associated with hemogasometric changes. The persistence of severe patient-ventilator asynchrony was an independent risk factor for failure of the spontaneous breathing test, ventilation time, ventilator-associated pneumonia, organ dysfunction, mortality in the intensive care unit, and length of stay in the intensive care unit.
Conclusion:
Patient-ventilator asynchrony is a frequent disorder in critically ill patients with inspiratory effort. The patient’s interaction with the ventilator should be optimized to improve hemogasometric parameters and clinical results. Further studies are required to confirm these results.
Keywords:Intensive care unitsInteractive ventilatory supportMortalityPhysiological monitoringRespiration, artificial/methodsSee more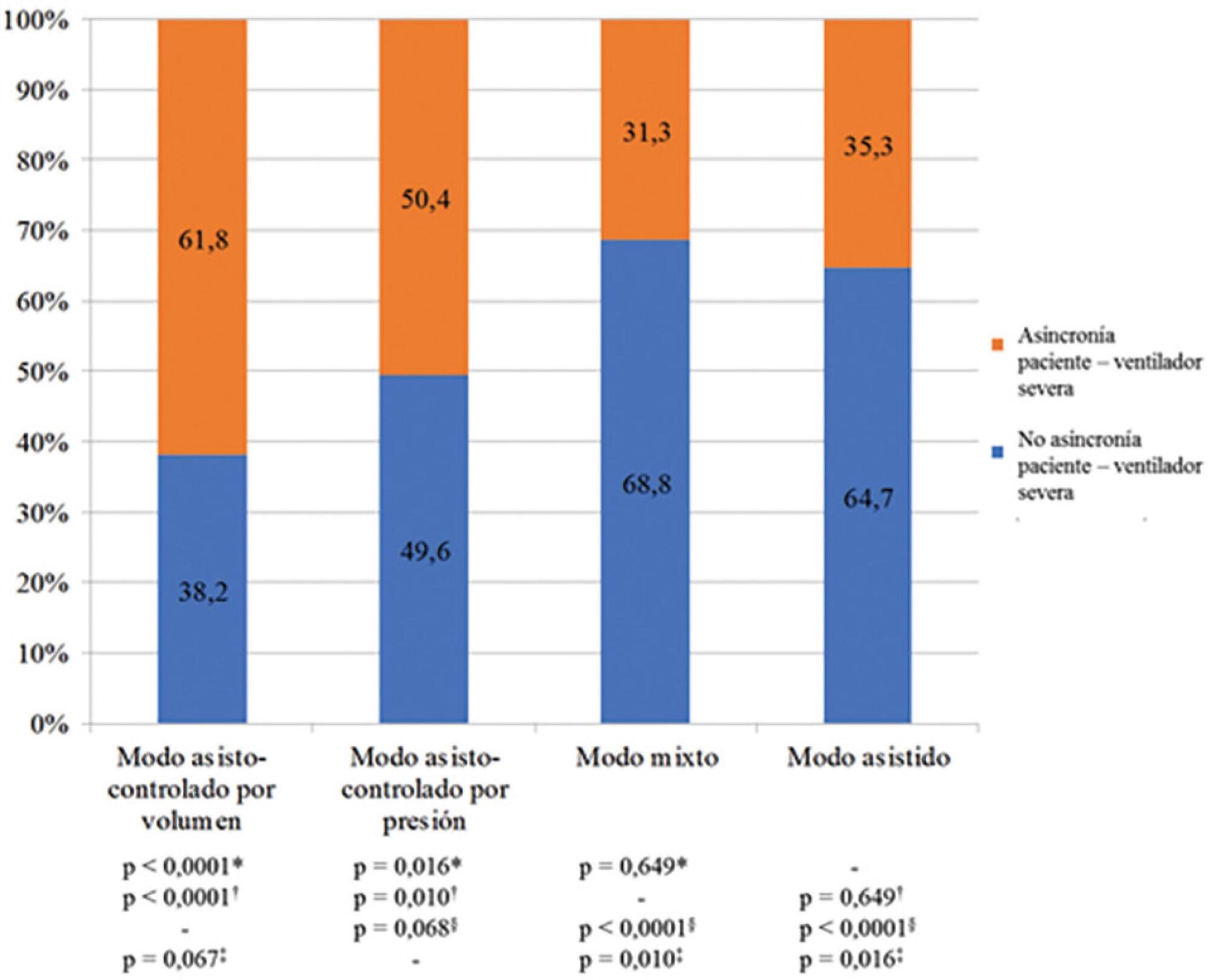
- Frank Daniel Martos-Benítez
-
Original Article
Does the endotracheal tube insertion depth predicted by formulas in children have a good concordance with the ideal position observed by X-ray?
- Dayanna Letícia Silva Santos ,
- Paulo Douglas de Oliveira Andrade,
- Evelim Leal de Freitas Dantas Gomes
Abstract
Original ArticleDoes the endotracheal tube insertion depth predicted by formulas in children have a good concordance with the ideal position observed by X-ray?
Rev Bras Ter Intensiva. 2020;32(2):295-300
DOI 10.5935/0103-507X.20200046
- Dayanna Letícia Silva Santos ,
- Paulo Douglas de Oliveira Andrade,
- Evelim Leal de Freitas Dantas Gomes
Views0ABSTRACT
Objective:
To evaluate the effectiveness of the different formulas for estimating the insertion depth of an endotracheal tube in children.
Methods:
This was an observational and cross-sectional study that included children between 29 days and 2 years of age who were hospitalized in a pediatric intensive care unit and mechanically ventilated. The formulas based on height [(height/10) + 5], the inner diameter of the tube (endotracheal tube × 3), and weight (weight + 6) were evaluated to determine which of them showed better concordance with the ideal insertion depth of the endotracheal tube as evaluated by X-ray.
Results:
The correlation between the height-based calculation and the ideal depth observed on X-ray was strong, with r = 0.88, p < 0.05, and a concordance correlation coefficient of 0.88; the correlation between the weight-based calculation and depth on X-ray was r = 0.75, p < 0.05, and concordance correlation coefficient 0.43; and the correlation between endotracheal tube diameter-based calculation and depth on X-ray was r = 0.80, p < 0.05, and concordance correlation coefficient 0.78. Lin’s concordance correlation analysis indicated that the measurements showed weak concordance (< 0.90).
Conclusion:
The formulas that estimate the insertion depth of the endotracheal tube in children were not accurate and were discordant with the gold-standard method of X-ray evaluation. There is a need for a new method based on anthropometric variables (weight and height) and age that is effective in guiding health professionals of pediatric intensive care units at the time of intubation.
Keywords:ChildInfantIntensive care units, pediatricIntubation, intratrachealThorax/imaging diagnosisSee moreViews0Abstract
Original ArticleDoes the endotracheal tube insertion depth predicted by formulas in children have a good concordance with the ideal position observed by X-ray?
Rev Bras Ter Intensiva. 2020;32(2):295-300
DOI 10.5935/0103-507X.20200046
- Dayanna Letícia Silva Santos ,
- Paulo Douglas de Oliveira Andrade,
- Evelim Leal de Freitas Dantas Gomes
Views0ABSTRACT
Objective:
To evaluate the effectiveness of the different formulas for estimating the insertion depth of an endotracheal tube in children.
Methods:
This was an observational and cross-sectional study that included children between 29 days and 2 years of age who were hospitalized in a pediatric intensive care unit and mechanically ventilated. The formulas based on height [(height/10) + 5], the inner diameter of the tube (endotracheal tube × 3), and weight (weight + 6) were evaluated to determine which of them showed better concordance with the ideal insertion depth of the endotracheal tube as evaluated by X-ray.
Results:
The correlation between the height-based calculation and the ideal depth observed on X-ray was strong, with r = 0.88, p < 0.05, and a concordance correlation coefficient of 0.88; the correlation between the weight-based calculation and depth on X-ray was r = 0.75, p < 0.05, and concordance correlation coefficient 0.43; and the correlation between endotracheal tube diameter-based calculation and depth on X-ray was r = 0.80, p < 0.05, and concordance correlation coefficient 0.78. Lin’s concordance correlation analysis indicated that the measurements showed weak concordance (< 0.90).
Conclusion:
The formulas that estimate the insertion depth of the endotracheal tube in children were not accurate and were discordant with the gold-standard method of X-ray evaluation. There is a need for a new method based on anthropometric variables (weight and height) and age that is effective in guiding health professionals of pediatric intensive care units at the time of intubation.
Keywords:ChildInfantIntensive care units, pediatricIntubation, intratrachealThorax/imaging diagnosisSee more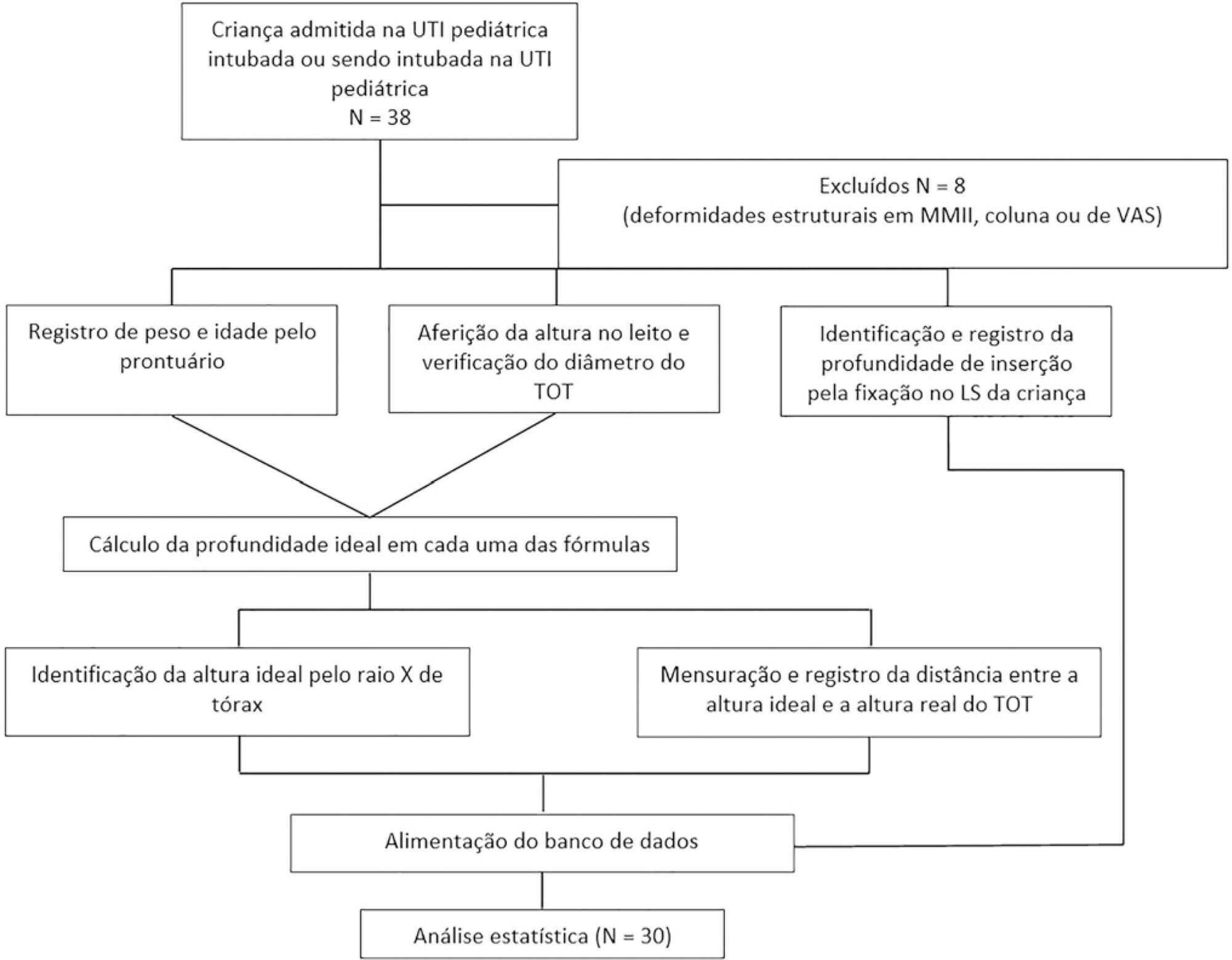
- Dayanna Letícia Silva Santos
-
Original Article
Modified Early Warning Score as a predictor of intensive care unit readmission within 48 hours: a retrospective observational study
- Ahmed Naji Balshi,
- Basim Mohammed Huwait,
- Alfateh Sayed Nasr Noor,
- Abdulrahman Mishaal Alharthy,
- Ahmed Fouad Madi, [ … ],
- Waleed Tharwat Aletreby
Abstract
Original ArticleModified Early Warning Score as a predictor of intensive care unit readmission within 48 hours: a retrospective observational study
Rev Bras Ter Intensiva. 2020;32(2):301-307
DOI 10.5935/0103-507X.20200047
- Ahmed Naji Balshi,
- Basim Mohammed Huwait,
- Alfateh Sayed Nasr Noor,
- Abdulrahman Mishaal Alharthy,
- Ahmed Fouad Madi,
- Omar Elsayed Ramadan,
- Abdullah balahmar,
- Huda A. Mhawish,
- Bobby Rose Marasigan,
- Alva Minette Alcazar,
- Muhammad Asim Rana,
- Waleed Tharwat Aletreby
Views1See moreABSTRACT
Objective:
To evaluate the hypothesis that the Modified Early Warning Score (MEWS) at the time of intensive care unit discharge is associated with readmission and to identify the MEWS that most reliably predicts intensive care unit readmission within 48 hours of discharge.
Methods:
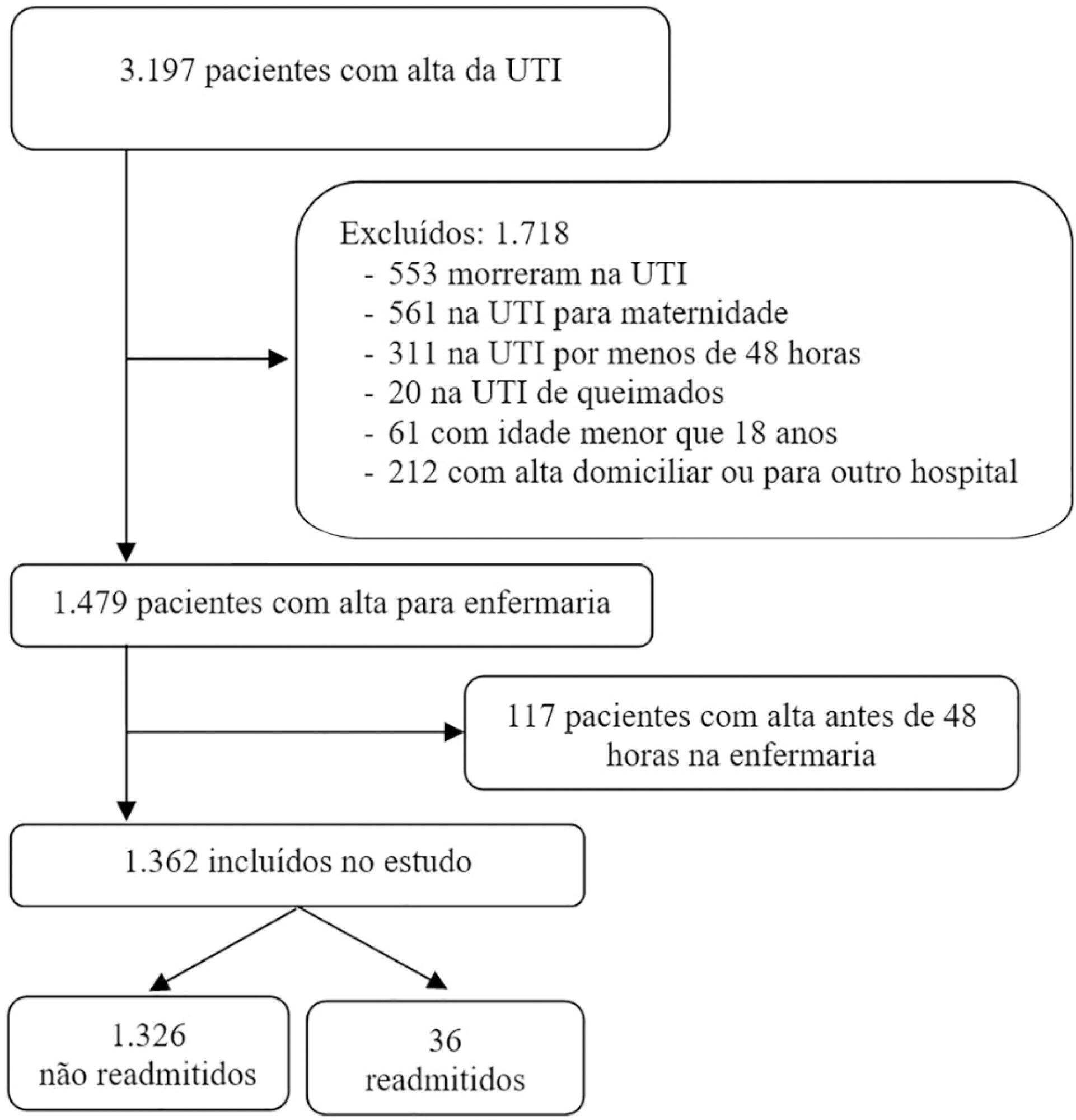
This was a retrospective observational study of the MEWSs of discharged patients from the intensive care unit. We compared the demographics, severity scores, critical illness characteristics, and MEWSs of readmitted and non-readmitted patients, identified factors associated with readmission in a logistic regression model, constructed a Receiver Operating Characteristic (ROC) curve of the MEWS in predicting the probability of readmission, and presented the optimum criterion with the highest sensitivity and specificity.
Results:
The readmission rate was 2.6%, and the MEWS was a significant predictor of readmission, along with intensive care unit length of stay > 10 days and tracheostomy. The ROC curve of the MEWS in predicting the readmission probability had an AUC of 0.82, and a MEWS > 6 carried a sensitivity of 0.78 (95%CI 0.66 – 0.9) and specificity of 0.9 (95%CI 0.87 – 0.93).
Conclusion:
The MEWS is associated with intensive care unit readmission, and a score > 6 has excellent accuracy as a prognostic predictor.
Views1Abstract
Original ArticleModified Early Warning Score as a predictor of intensive care unit readmission within 48 hours: a retrospective observational study
Rev Bras Ter Intensiva. 2020;32(2):301-307
DOI 10.5935/0103-507X.20200047
- Ahmed Naji Balshi,
- Basim Mohammed Huwait,
- Alfateh Sayed Nasr Noor,
- Abdulrahman Mishaal Alharthy,
- Ahmed Fouad Madi,
- Omar Elsayed Ramadan,
- Abdullah balahmar,
- Huda A. Mhawish,
- Bobby Rose Marasigan,
- Alva Minette Alcazar,
- Muhammad Asim Rana,
- Waleed Tharwat Aletreby
Views1See moreABSTRACT
Objective:
To evaluate the hypothesis that the Modified Early Warning Score (MEWS) at the time of intensive care unit discharge is associated with readmission and to identify the MEWS that most reliably predicts intensive care unit readmission within 48 hours of discharge.
Methods:
This was a retrospective observational study of the MEWSs of discharged patients from the intensive care unit. We compared the demographics, severity scores, critical illness characteristics, and MEWSs of readmitted and non-readmitted patients, identified factors associated with readmission in a logistic regression model, constructed a Receiver Operating Characteristic (ROC) curve of the MEWS in predicting the probability of readmission, and presented the optimum criterion with the highest sensitivity and specificity.
Results:
The readmission rate was 2.6%, and the MEWS was a significant predictor of readmission, along with intensive care unit length of stay > 10 days and tracheostomy. The ROC curve of the MEWS in predicting the readmission probability had an AUC of 0.82, and a MEWS > 6 carried a sensitivity of 0.78 (95%CI 0.66 – 0.9) and specificity of 0.9 (95%CI 0.87 – 0.93).
Conclusion:
The MEWS is associated with intensive care unit readmission, and a score > 6 has excellent accuracy as a prognostic predictor.
-
Review Article
The medical decision-making process in the time of the coronavirus pandemic
- Cassiano Teixeira ,
- Regis Goulart Rosa ,
- Edison Moraes Rodrigues Filho,
- Eduardo de Oliveira Fernandes
Abstract
Review ArticleThe medical decision-making process in the time of the coronavirus pandemic
Rev Bras Ter Intensiva. 2020;32(2):308-311
DOI 10.5935/0103-507X.20200033
- Cassiano Teixeira ,
- Regis Goulart Rosa ,
- Edison Moraes Rodrigues Filho,
- Eduardo de Oliveira Fernandes
Views0ABSTRACT
The disease pandemic caused by the novel coronavirus has triggered significant changes in the medical decision-making process relating to critically ill patients. Admissions to intensive care units have suddenly increased, but many of these patients do not present with clinical manifestations related to the viral infection but rather exacerbation of preexisting diseases. In this context, we must prevent intuitive decision-making and insecurity from leading us to exhaust the available critical-care beds before they are truly necessary, while still recognizing the importance of rapid decision-making in emergency situations. One of the best ways to achieve this goal may be by practicing metacognition and establishing ways for regular feedback to be provided to professionals engaged in inherently rapid decision-making processes.
Keywords:BetacoronavirusCatastrophic illnessClinical decision-makingCoronavirusCoronavirus infectiousFeedbackIntensive care unitsMetacognitionPandemicsSee moreViews0Abstract
Review ArticleThe medical decision-making process in the time of the coronavirus pandemic
Rev Bras Ter Intensiva. 2020;32(2):308-311
DOI 10.5935/0103-507X.20200033
- Cassiano Teixeira ,
- Regis Goulart Rosa ,
- Edison Moraes Rodrigues Filho,
- Eduardo de Oliveira Fernandes
Views0ABSTRACT
The disease pandemic caused by the novel coronavirus has triggered significant changes in the medical decision-making process relating to critically ill patients. Admissions to intensive care units have suddenly increased, but many of these patients do not present with clinical manifestations related to the viral infection but rather exacerbation of preexisting diseases. In this context, we must prevent intuitive decision-making and insecurity from leading us to exhaust the available critical-care beds before they are truly necessary, while still recognizing the importance of rapid decision-making in emergency situations. One of the best ways to achieve this goal may be by practicing metacognition and establishing ways for regular feedback to be provided to professionals engaged in inherently rapid decision-making processes.
Keywords:BetacoronavirusCatastrophic illnessClinical decision-makingCoronavirusCoronavirus infectiousFeedbackIntensive care unitsMetacognitionPandemicsSee more - Cassiano Teixeira
-
Review Article
Apnea test for brain death diagnosis in adults on extracorporeal membrane oxygenation: a review
- Erica Regina Ribeiro Sady ,
- Lígia Junqueira,
- Viviane Cordeiro Veiga ,
- Salomón Soriano Ordinola Rojas
Abstract
Review ArticleApnea test for brain death diagnosis in adults on extracorporeal membrane oxygenation: a review
Rev Bras Ter Intensiva. 2020;32(2):312-318
DOI 10.5935/0103-507X.20200048
- Erica Regina Ribeiro Sady ,
- Lígia Junqueira,
- Viviane Cordeiro Veiga ,
- Salomón Soriano Ordinola Rojas
Views0Abstract
Among the potential complications of extracorporeal membrane oxygenation, neurological dysfunctions, including brain death, are not negligible. In Brazil, the diagnostic process of brain death is regulated by Federal Council of Medicine resolution 2,173 of 2017. Diagnostic tests for brain death include the apnea test, which assesses the presence of a ventilatory response to hypercapnic stimulus. However, gas exchange, including carbon dioxide removal, is maintained under extracorporeal membrane oxygenation, making the test challenging. In addition to the fact that the aforementioned resolution does not consider the specificities of the diagnostic process under extracorporeal membrane oxygenation, studies on the subject are scarce. This review aims to identify case studies (and/or case series) published in the PubMed® and Cochrane databases describing the process of brain death diagnosis. A total of 17 publications (2011 – 2019) were identified. The practical strategies described were to provide pretest supplemental oxygenation via mechanical ventilation and extracorporeal membrane oxygenation (fraction of inspired oxygen = 1.0) and, at the beginning of the test, titrate the sweep flow (0.5 – 1.0L/minute) to minimize carbon dioxide removal. It is also recommended to increase blood flow and/or sweep flow in the presence of hypoxemia and/or hypotension, which may be combined with fluid infusion and/or the escalation of inotropic/vasoactive drugs. If the partial pressure of carbon dioxide threshold is not reached, repeating the test under supplementation of carbon dioxide exogenous to the circuit is an alternative. Last, in cases of venoarterial extracorporeal membrane oxygenation, to measure gas variation and exclude differential hypoxia, blood samples of the native and extracorporeal (post-oxygenator) circulations are recommended.
Keywords:Brain death/diagnosisExtracorporeal membrane oxygenationIntensive care unitsPoint-of-care testingSee moreViews0Abstract
Review ArticleApnea test for brain death diagnosis in adults on extracorporeal membrane oxygenation: a review
Rev Bras Ter Intensiva. 2020;32(2):312-318
DOI 10.5935/0103-507X.20200048
- Erica Regina Ribeiro Sady ,
- Lígia Junqueira,
- Viviane Cordeiro Veiga ,
- Salomón Soriano Ordinola Rojas
Views0Abstract
Among the potential complications of extracorporeal membrane oxygenation, neurological dysfunctions, including brain death, are not negligible. In Brazil, the diagnostic process of brain death is regulated by Federal Council of Medicine resolution 2,173 of 2017. Diagnostic tests for brain death include the apnea test, which assesses the presence of a ventilatory response to hypercapnic stimulus. However, gas exchange, including carbon dioxide removal, is maintained under extracorporeal membrane oxygenation, making the test challenging. In addition to the fact that the aforementioned resolution does not consider the specificities of the diagnostic process under extracorporeal membrane oxygenation, studies on the subject are scarce. This review aims to identify case studies (and/or case series) published in the PubMed® and Cochrane databases describing the process of brain death diagnosis. A total of 17 publications (2011 – 2019) were identified. The practical strategies described were to provide pretest supplemental oxygenation via mechanical ventilation and extracorporeal membrane oxygenation (fraction of inspired oxygen = 1.0) and, at the beginning of the test, titrate the sweep flow (0.5 – 1.0L/minute) to minimize carbon dioxide removal. It is also recommended to increase blood flow and/or sweep flow in the presence of hypoxemia and/or hypotension, which may be combined with fluid infusion and/or the escalation of inotropic/vasoactive drugs. If the partial pressure of carbon dioxide threshold is not reached, repeating the test under supplementation of carbon dioxide exogenous to the circuit is an alternative. Last, in cases of venoarterial extracorporeal membrane oxygenation, to measure gas variation and exclude differential hypoxia, blood samples of the native and extracorporeal (post-oxygenator) circulations are recommended.
Keywords:Brain death/diagnosisExtracorporeal membrane oxygenationIntensive care unitsPoint-of-care testingSee more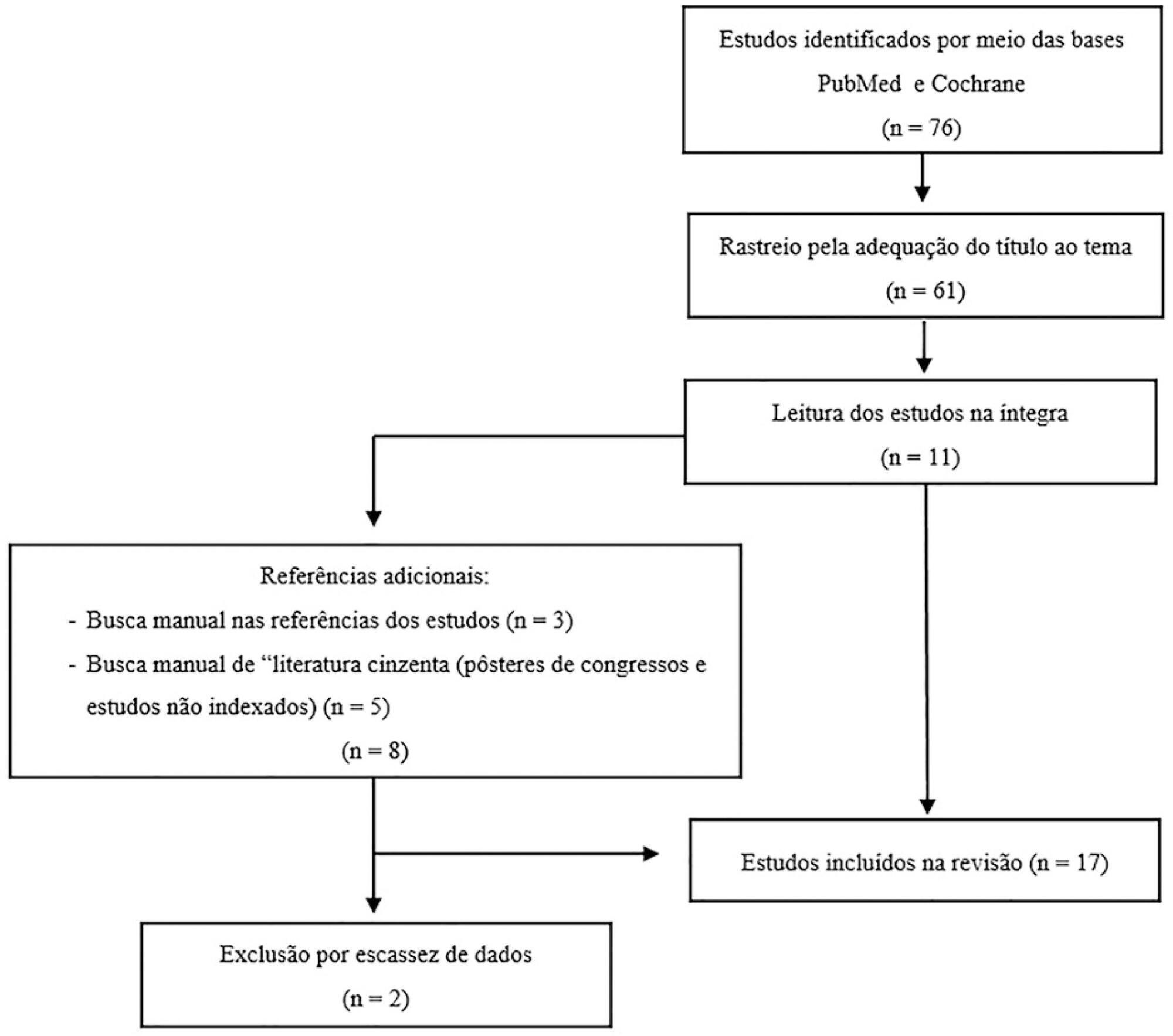
- Erica Regina Ribeiro Sady
-
Case Report
Use of CPAP as an alternative to the apnea test during the determination of brain death in hypoxemic patients. Report of two cases
- Glauco Adrieno Westphal ,
- Veviani Fernandes ,
- Verônica Westphal,
- Jessica Cangussu Fonseca,
- Luciano Rodrigues da Silva, [ … ],
- Jorge Luis dos Santos Valiatti
Abstract
Case ReportUse of CPAP as an alternative to the apnea test during the determination of brain death in hypoxemic patients. Report of two cases
Rev Bras Ter Intensiva. 2020;32(2):319-325
DOI 10.5935/0103-507X.20200032
- Glauco Adrieno Westphal ,
- Veviani Fernandes ,
- Verônica Westphal,
- Jessica Cangussu Fonseca,
- Luciano Rodrigues da Silva,
- Jorge Luis dos Santos Valiatti
Views0ABSTRACT
The apnea test, which involves disconnection from the mechanical ventilator, presents risks during the determination of brain death, especially in hypoxemic patients. We describe the performance of the apnea test without disconnection from the mechanical ventilator in two patients. The first case involved an 8-year-old boy admitted with severe hypoxemia due to pneumonia. He presented with cardiorespiratory arrest, followed by unresponsive coma due to hypoxic-ischemic encephalopathy. Two clinical exams revealed the absence of brainstem reflexes, and transcranial Doppler ultrasound revealed brain circulatory arrest. Three attempts were made to perform the apnea test, which were interrupted by hypoxemia; therefore, the apnea test was performed without disconnection from the mechanical ventilator, adjusting the continuous airway pressure to 10cmH2O and the inspired fraction of oxygen to 100%. The oxygen saturation was maintained at 100% for 10 minutes. Posttest blood gas analysis results were as follows: pH, 6.90; partial pressure of oxygen, 284.0mmHg; partial pressure of carbon dioxide, 94.0mmHg; and oxygen saturation, 100%. The second case involved a 43-year-old woman admitted with subarachnoid hemorrhage (Hunt-Hess V and Fisher IV). Two clinical exams revealed unresponsive coma and absence of all brainstem reflexes. Brain scintigraphy showed no radioisotope uptake into the brain parenchyma. The first attempt at the apnea test was stopped after 5 minutes due to hypothermia (34.9°C). After rewarming, the apnea test was repeated without disconnection from the mechanical ventilator, showing maintenance of the functional residual volume with electrical bioimpedance. Posttest blood gas analysis results were as follows: pH, 7.01; partial pressure of oxygen, 232.0mmHg; partial pressure of carbon dioxide, 66.9mmHg; and oxygen saturation, 99.0%. The apnea test without disconnection from the mechanical ventilator allowed the preservation of oxygenation in both cases. The use of continuous airway pressure during the apnea test seems to be a safe alternative in order to maintain alveolar recruitment and oxygenation during brain death determination.
Keywords:ApneaApnea testingbrain deathContinuous positive airway pressureElectrical impedanceHypoxiaRespiratory insufficiencySleep apnea syndromesTomography/methodsSee moreViews0Abstract
Case ReportUse of CPAP as an alternative to the apnea test during the determination of brain death in hypoxemic patients. Report of two cases
Rev Bras Ter Intensiva. 2020;32(2):319-325
DOI 10.5935/0103-507X.20200032
- Glauco Adrieno Westphal ,
- Veviani Fernandes ,
- Verônica Westphal,
- Jessica Cangussu Fonseca,
- Luciano Rodrigues da Silva,
- Jorge Luis dos Santos Valiatti
Views0ABSTRACT
The apnea test, which involves disconnection from the mechanical ventilator, presents risks during the determination of brain death, especially in hypoxemic patients. We describe the performance of the apnea test without disconnection from the mechanical ventilator in two patients. The first case involved an 8-year-old boy admitted with severe hypoxemia due to pneumonia. He presented with cardiorespiratory arrest, followed by unresponsive coma due to hypoxic-ischemic encephalopathy. Two clinical exams revealed the absence of brainstem reflexes, and transcranial Doppler ultrasound revealed brain circulatory arrest. Three attempts were made to perform the apnea test, which were interrupted by hypoxemia; therefore, the apnea test was performed without disconnection from the mechanical ventilator, adjusting the continuous airway pressure to 10cmH2O and the inspired fraction of oxygen to 100%. The oxygen saturation was maintained at 100% for 10 minutes. Posttest blood gas analysis results were as follows: pH, 6.90; partial pressure of oxygen, 284.0mmHg; partial pressure of carbon dioxide, 94.0mmHg; and oxygen saturation, 100%. The second case involved a 43-year-old woman admitted with subarachnoid hemorrhage (Hunt-Hess V and Fisher IV). Two clinical exams revealed unresponsive coma and absence of all brainstem reflexes. Brain scintigraphy showed no radioisotope uptake into the brain parenchyma. The first attempt at the apnea test was stopped after 5 minutes due to hypothermia (34.9°C). After rewarming, the apnea test was repeated without disconnection from the mechanical ventilator, showing maintenance of the functional residual volume with electrical bioimpedance. Posttest blood gas analysis results were as follows: pH, 7.01; partial pressure of oxygen, 232.0mmHg; partial pressure of carbon dioxide, 66.9mmHg; and oxygen saturation, 99.0%. The apnea test without disconnection from the mechanical ventilator allowed the preservation of oxygenation in both cases. The use of continuous airway pressure during the apnea test seems to be a safe alternative in order to maintain alveolar recruitment and oxygenation during brain death determination.
Keywords:ApneaApnea testingbrain deathContinuous positive airway pressureElectrical impedanceHypoxiaRespiratory insufficiencySleep apnea syndromesTomography/methodsSee more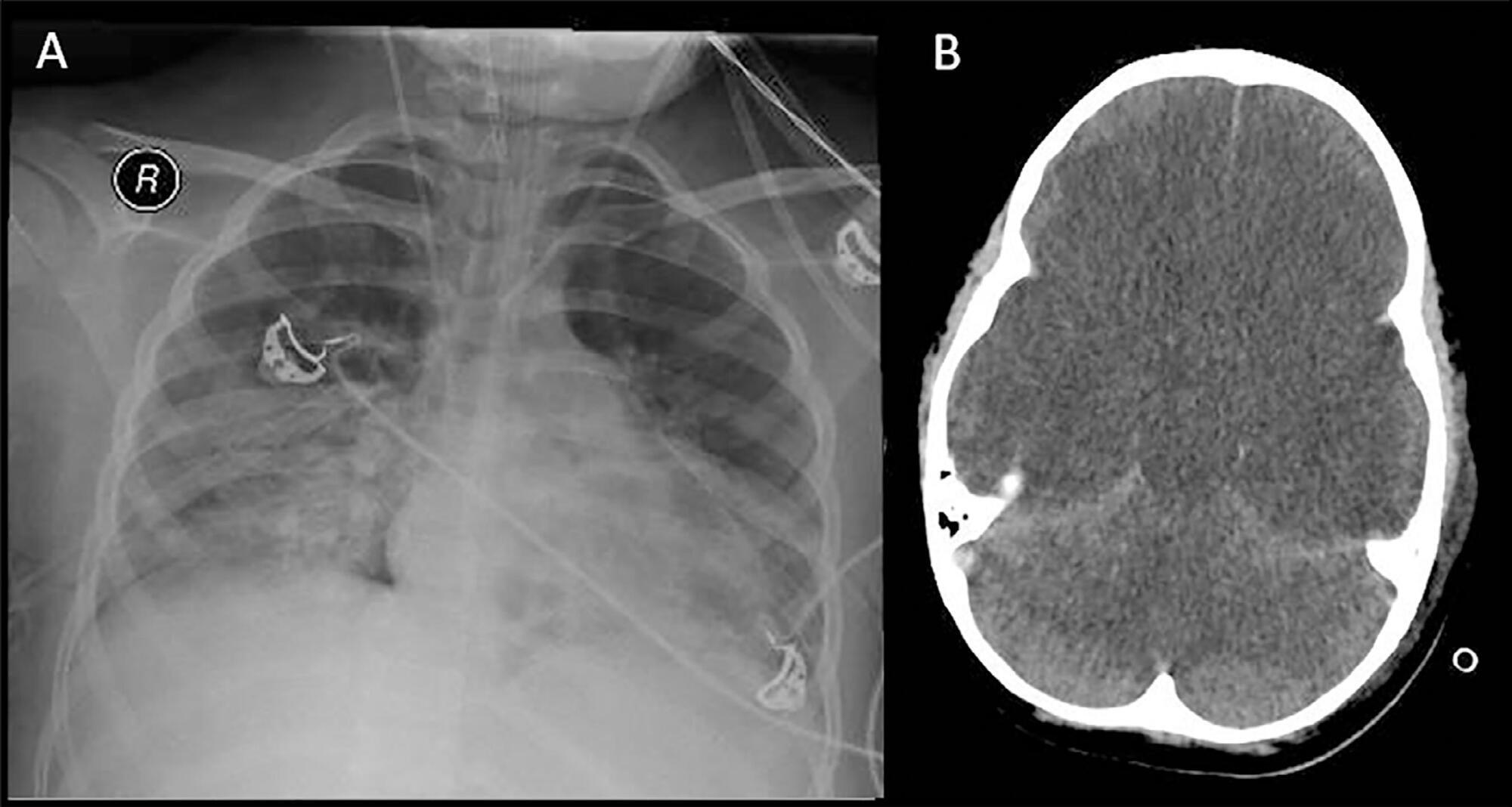
- Glauco Adrieno Westphal
-
Letter to the Editor
Time to positivity: a useful parameter to evaluate intensive care unit blood stream infections?
Rev Bras Ter Intensiva. 2020;32(2):326-329
Abstract
Letter to the EditorTime to positivity: a useful parameter to evaluate intensive care unit blood stream infections?
Rev Bras Ter Intensiva. 2020;32(2):326-329
DOI 10.5935/0103-507X.20200049
Views0Dear editor, Bloodstream infections (BSI) are frequent and serious complications in intensive care units (ICU) and are associated with high morbidity and mortality rates, increased hospital stay and healthcare-related costs.(–)[…]See moreViews0Abstract
Letter to the EditorTime to positivity: a useful parameter to evaluate intensive care unit blood stream infections?
Rev Bras Ter Intensiva. 2020;32(2):326-329
DOI 10.5935/0103-507X.20200049
Views0Dear editor, Bloodstream infections (BSI) are frequent and serious complications in intensive care units (ICU) and are associated with high morbidity and mortality rates, increased hospital stay and healthcare-related costs.(–)[…]See more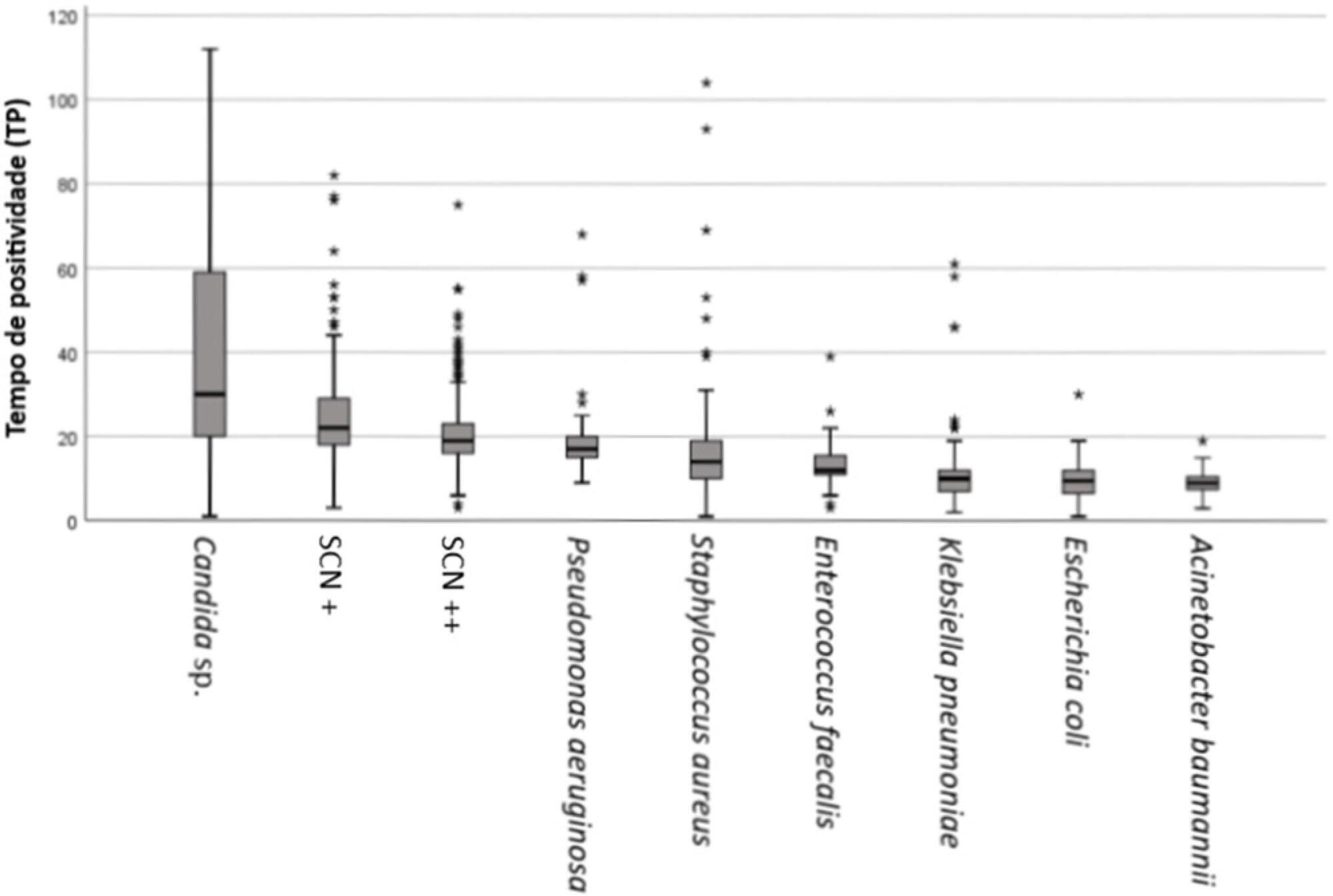
-
Author’s Response
Reply to: Efficacy and safety of high-flow nasal cannula oxygen therapy in moderate acute hypercapnic respiratory failure
Rev Bras Ter Intensiva. 2020;32(2):330-331
Abstract
Author’s ResponseReply to: Efficacy and safety of high-flow nasal cannula oxygen therapy in moderate acute hypercapnic respiratory failure
Rev Bras Ter Intensiva. 2020;32(2):330-331
DOI 10.5935/0103-507X.20200035
Views0To the Editor We thank Dr. Esquinas and Reazaul for their interest in our study and their thoughtful commentaries about some aspects of the methodology and the generalizability of the results.[…]See moreViews0Abstract
Author’s ResponseReply to: Efficacy and safety of high-flow nasal cannula oxygen therapy in moderate acute hypercapnic respiratory failure
Rev Bras Ter Intensiva. 2020;32(2):330-331
DOI 10.5935/0103-507X.20200035
Views0To the Editor We thank Dr. Esquinas and Reazaul for their interest in our study and their thoughtful commentaries about some aspects of the methodology and the generalizability of the results.[…]See more -
Erratum
Erratum
Rev Bras Ter Intensiva. 2020;32(2):332-332
Abstract
ErratumErratum
Rev Bras Ter Intensiva. 2020;32(2):332-332
DOI 10.5935/0103-507X.20200050
Views0In the article Impact of fast track on adult cardiac surgery: clinical and hospital outcomes, with DOI number: 10.5935/0103-507X.20190059, published in the journal Revista Brasileira de Terapia Intensiva, 31(3):361-7, on page 361: Where it read: […]See moreViews0Abstract
ErratumErratum
Rev Bras Ter Intensiva. 2020;32(2):332-332
DOI 10.5935/0103-507X.20200050
Views0In the article Impact of fast track on adult cardiac surgery: clinical and hospital outcomes, with DOI number: 10.5935/0103-507X.20190059, published in the journal Revista Brasileira de Terapia Intensiva, 31(3):361-7, on page 361: Where it read: […]See more
Volume Articles - Critical Care Science (CCS)
