Infections Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2022;34(3):327-334
DOI 10.5935/0103-507X.20220070-en
To describe the implementation and results of the collaborative PROADI-SUS project by the Brazilian Ministry of Health to reduce healthcare-associated infections: ventilator-associated pneumonia, primary central line-associated bloodstream infection and catheter-associated urinary tract infections.
This was a prospective observational study that investigated the implementation stages and outcomes during 18 months in five intensive care units in the city of Recife. Reductions in healthcare-associated infections in each unit were calculated using previous medians compared to those of the study period.
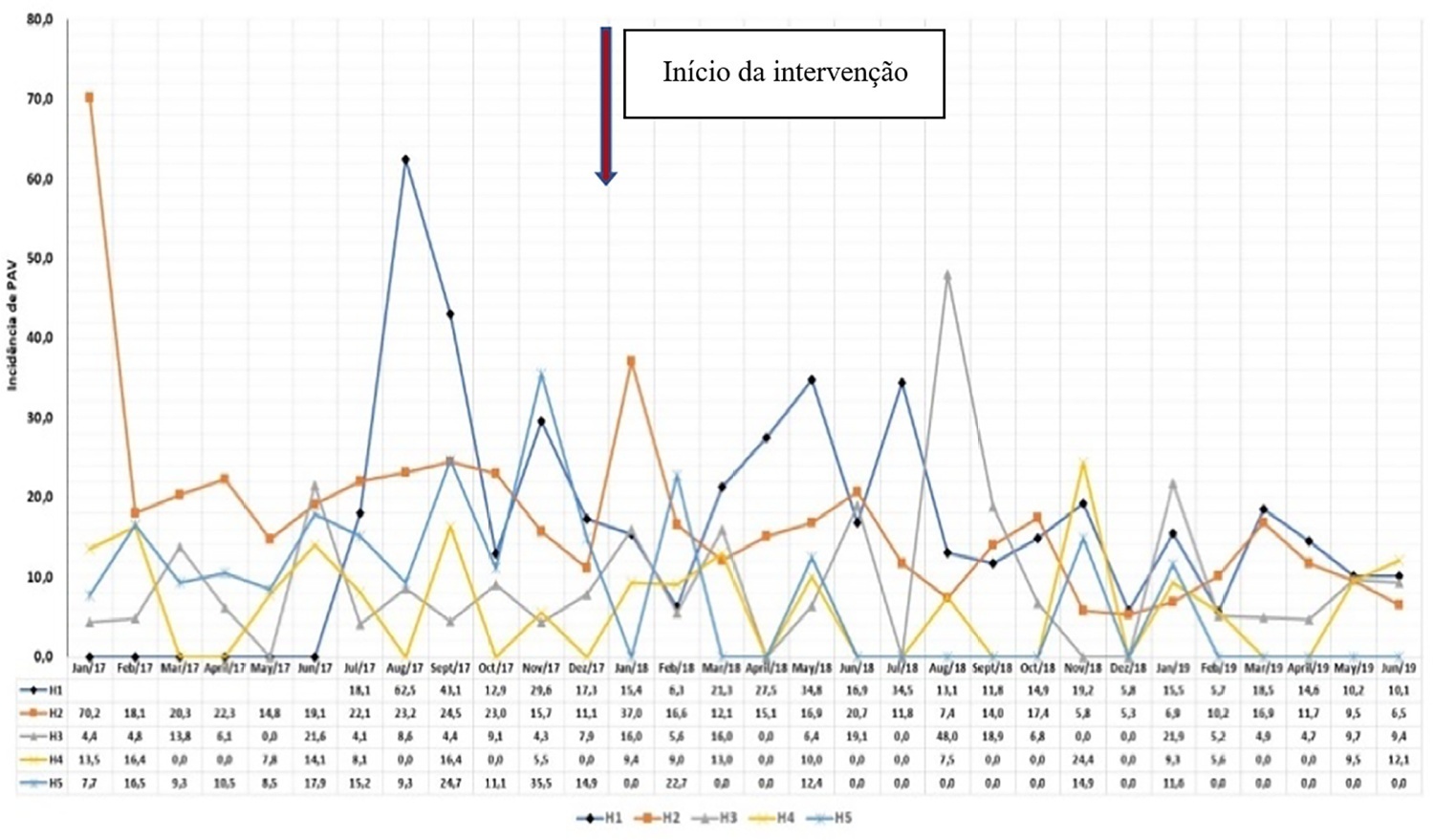
The goal of reducing the three healthcare-associated infections, i.e., 30% in 18 months, was achieved in at least one of the healthcare-associated infections and was also achieved for two healthcare-associated infections in two hospitals and three healthcare-associated infections in just one hospital; the latter reached the target of 36 months. Implementing the bundles and monitoring the results by the professionals were considered essential actions by the local management teams. In addition, the acquisition of supplies and their availability alongside the beds, signage, checklists, staff awareness, adaptation, team building, training and celebration of achievements were assessed as being relevant for reducing healthcare-associated infections.
The collaborative approach reduced healthcare-associated infections, despite partial adherence to the bundles. The hypothesis is that success is related to the project methodology and motivated multidisciplinary teams, especially nursing teams.
Abstract
Rev Bras Ter Intensiva. 2022;34(3):327-334
DOI 10.5935/0103-507X.20220070-en
To describe the implementation and results of the collaborative PROADI-SUS project by the Brazilian Ministry of Health to reduce healthcare-associated infections: ventilator-associated pneumonia, primary central line-associated bloodstream infection and catheter-associated urinary tract infections.
This was a prospective observational study that investigated the implementation stages and outcomes during 18 months in five intensive care units in the city of Recife. Reductions in healthcare-associated infections in each unit were calculated using previous medians compared to those of the study period.
The goal of reducing the three healthcare-associated infections, i.e., 30% in 18 months, was achieved in at least one of the healthcare-associated infections and was also achieved for two healthcare-associated infections in two hospitals and three healthcare-associated infections in just one hospital; the latter reached the target of 36 months. Implementing the bundles and monitoring the results by the professionals were considered essential actions by the local management teams. In addition, the acquisition of supplies and their availability alongside the beds, signage, checklists, staff awareness, adaptation, team building, training and celebration of achievements were assessed as being relevant for reducing healthcare-associated infections.
The collaborative approach reduced healthcare-associated infections, despite partial adherence to the bundles. The hypothesis is that success is related to the project methodology and motivated multidisciplinary teams, especially nursing teams.
Abstract
Rev Bras Ter Intensiva. 2022;34(1):154-162
DOI 10.5935/0103-507X.20220010-en
To evaluate the influence of patient characteristics on hyperlactatemia in an infected population admitted to intensive care units and the influence of hyperlactatemia severity on hospital mortality.
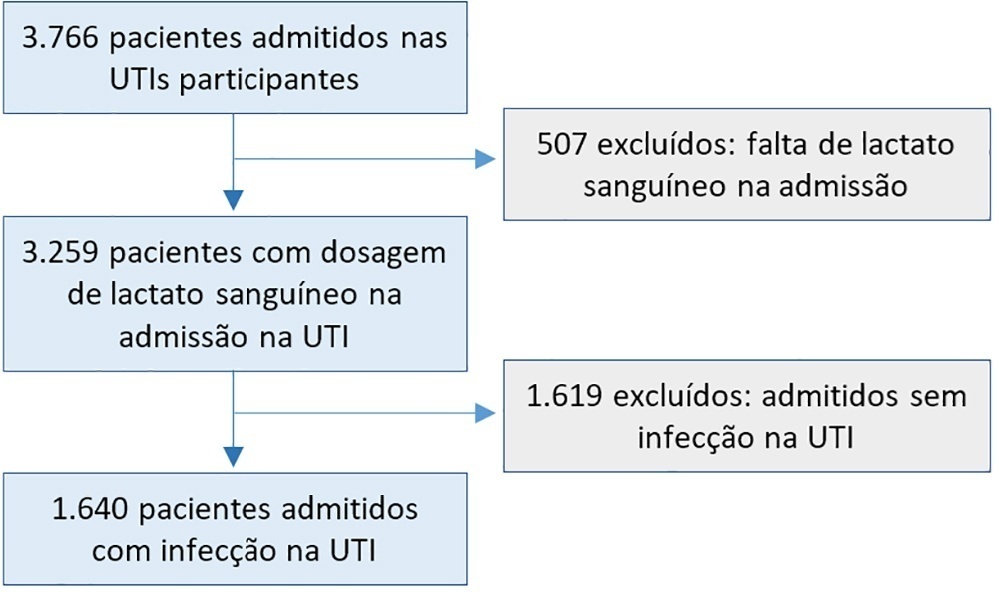
A post hoc analysis of hyperlactatemia in the INFAUCI study, a national prospective, observational, multicenter study, was conducted in 14 Portuguese intensive care units. Infected patients admitted to intensive care units with a lactate measurement in the first 12 hours of admission were selected. Sepsis was identified according to the Sepsis-2 definition accepted at the time of data collection. The severity of hyperlactatemia was classified as mild (2 - 3.9mmol/L), moderate (4.0 - 9.9mmol/L) or severe (> 10mmol/L).
In a total of 1,640 patients infected on admission, hyperlactatemia occurred in 934 patients (57%), classified as mild, moderate and severe in 57.0%, 34.4% and 8.7% of patients, respectively. The presence of hyperlactatemia and a higher degree of hyperlactatemia were both associated with a higher Simplified Acute Physiology Score II, a higher Charlson Comorbidity Index and the presence of septic shock. The lactate Receiver Operating Characteristic curve for hospital mortality had an area under the curve of 0.64 (95%CI 0.61 - 0.72), which increased to 0.71 (95%CI 0.68 - 0.74) when combined with Sequential Organ Failure Assessment score. In-hospital mortality with other covariates adjusted by Simplified Acute Physiology Score II was associated with moderate and severe hyperlactatemia, with odds ratio of 1.95 (95%CI 1.4 - 2.7; p < 0.001) and 4.54 (95%CI 2.4 - 8.5; p < 0.001), respectively.
Blood lactate levels correlate independently with in-hospital mortality for moderate and severe degrees of hyperlactatemia.
Abstract
Rev Bras Ter Intensiva. 2022;34(1):154-162
DOI 10.5935/0103-507X.20220010-en
To evaluate the influence of patient characteristics on hyperlactatemia in an infected population admitted to intensive care units and the influence of hyperlactatemia severity on hospital mortality.
A post hoc analysis of hyperlactatemia in the INFAUCI study, a national prospective, observational, multicenter study, was conducted in 14 Portuguese intensive care units. Infected patients admitted to intensive care units with a lactate measurement in the first 12 hours of admission were selected. Sepsis was identified according to the Sepsis-2 definition accepted at the time of data collection. The severity of hyperlactatemia was classified as mild (2 - 3.9mmol/L), moderate (4.0 - 9.9mmol/L) or severe (> 10mmol/L).
In a total of 1,640 patients infected on admission, hyperlactatemia occurred in 934 patients (57%), classified as mild, moderate and severe in 57.0%, 34.4% and 8.7% of patients, respectively. The presence of hyperlactatemia and a higher degree of hyperlactatemia were both associated with a higher Simplified Acute Physiology Score II, a higher Charlson Comorbidity Index and the presence of septic shock. The lactate Receiver Operating Characteristic curve for hospital mortality had an area under the curve of 0.64 (95%CI 0.61 - 0.72), which increased to 0.71 (95%CI 0.68 - 0.74) when combined with Sequential Organ Failure Assessment score. In-hospital mortality with other covariates adjusted by Simplified Acute Physiology Score II was associated with moderate and severe hyperlactatemia, with odds ratio of 1.95 (95%CI 1.4 - 2.7; p < 0.001) and 4.54 (95%CI 2.4 - 8.5; p < 0.001), respectively.
Blood lactate levels correlate independently with in-hospital mortality for moderate and severe degrees of hyperlactatemia.
Abstract
Rev Bras Ter Intensiva. 2021;33(3):346-352
DOI 10.5935/0103-507X.20210053
To assess pulmonary embolism incidence, its relationship with D-dimer levels and other possible associated factors in addition to anticoagulation and contrast medium adverse effects.
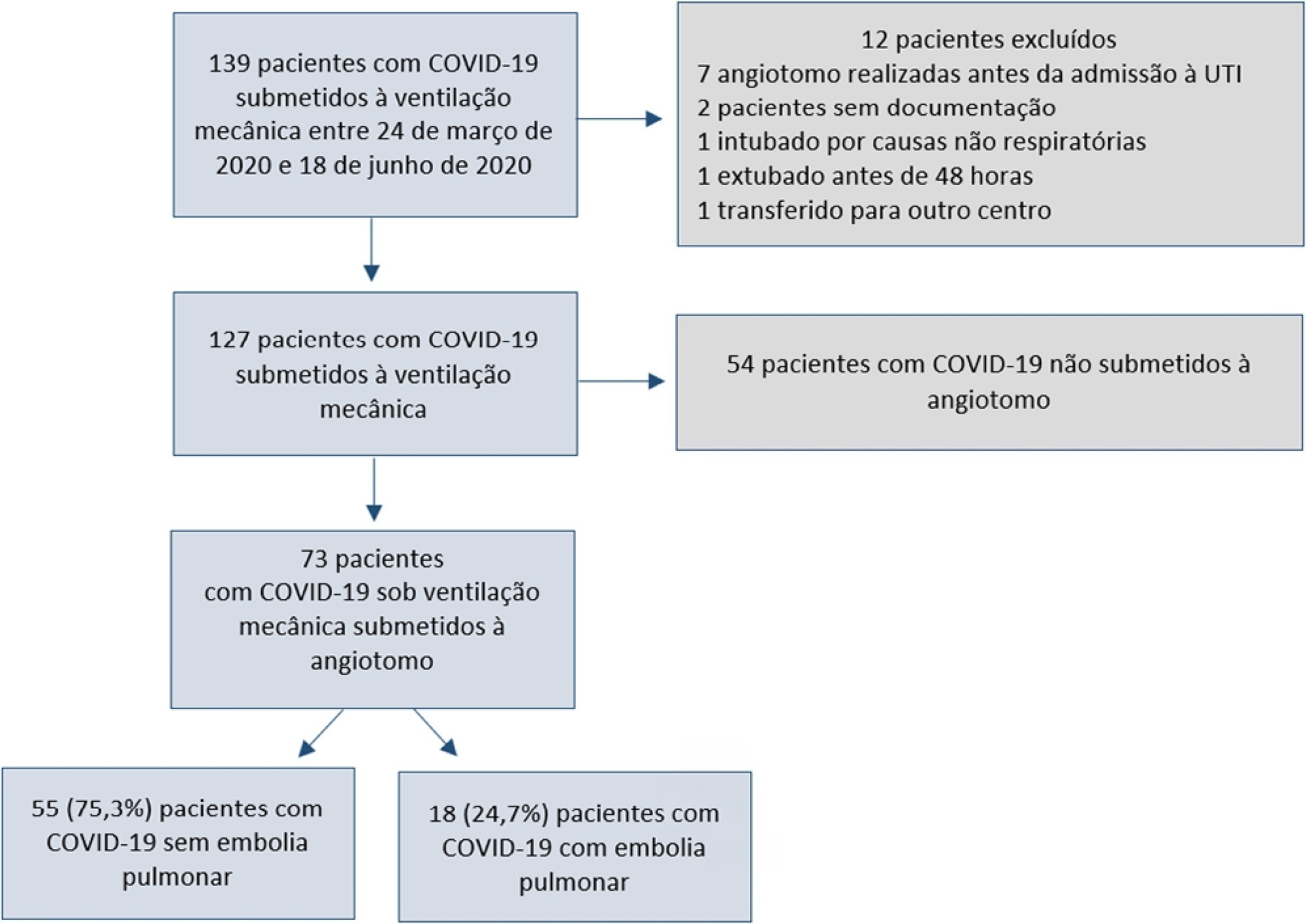
A retrospective observational cohort study at a Chilean public hospital was performed. Intensive care unit mechanically ventilated COVID-19 patients older than 18 years old between March and June 2020 were included. All patients received heparin thromboprophylaxis, which was increased to the anticoagulation dose with D-dimer greater than 3µg/mL.
A total of 127 patients were followed up, of whom 73 underwent pulmonary computed tomography angiography (mean age, 54 ± 12 years; 49 men). Sixty-two of the 73 patients (84.9%) received full anticoagulation before computed tomography angiography. In addition, 18 of the 73 patients had pulmonary embolism (24.7%). When comparing patients with and without pulmonary embolism, no significant differences were observed in age, sex, obesity, smoking, Wells and revised Geneva scores, D-dimer or mortality. Anticoagulant use was similar in both groups. Days from the start of anticoagulation until computed tomography angiography were significantly lower in the pulmonary embolism group (p = 0.002). Three patients presented post contrast-acute kidney injury (4.1%), and one patient had major bleeding.
Despite anticoagulation, one in four COVID-19 patients connected to mechanical ventilation and evaluated with pulmonary computed tomography angiography had pulmonary embolism. With a longer the delay in performing computed tomography angiography once empirical anticoagulation was started, significantly less pulmonary embolism was identified.
Abstract
Rev Bras Ter Intensiva. 2021;33(3):346-352
DOI 10.5935/0103-507X.20210053
To assess pulmonary embolism incidence, its relationship with D-dimer levels and other possible associated factors in addition to anticoagulation and contrast medium adverse effects.
A retrospective observational cohort study at a Chilean public hospital was performed. Intensive care unit mechanically ventilated COVID-19 patients older than 18 years old between March and June 2020 were included. All patients received heparin thromboprophylaxis, which was increased to the anticoagulation dose with D-dimer greater than 3µg/mL.
A total of 127 patients were followed up, of whom 73 underwent pulmonary computed tomography angiography (mean age, 54 ± 12 years; 49 men). Sixty-two of the 73 patients (84.9%) received full anticoagulation before computed tomography angiography. In addition, 18 of the 73 patients had pulmonary embolism (24.7%). When comparing patients with and without pulmonary embolism, no significant differences were observed in age, sex, obesity, smoking, Wells and revised Geneva scores, D-dimer or mortality. Anticoagulant use was similar in both groups. Days from the start of anticoagulation until computed tomography angiography were significantly lower in the pulmonary embolism group (p = 0.002). Three patients presented post contrast-acute kidney injury (4.1%), and one patient had major bleeding.
Despite anticoagulation, one in four COVID-19 patients connected to mechanical ventilation and evaluated with pulmonary computed tomography angiography had pulmonary embolism. With a longer the delay in performing computed tomography angiography once empirical anticoagulation was started, significantly less pulmonary embolism was identified.
Abstract
Rev Bras Ter Intensiva. 2020;32(2):245-250
DOI 10.5935/0103-507X.20200029
To assess the relationship between time to focus clearance and hospital mortality in patients with sepsis and septic shock.
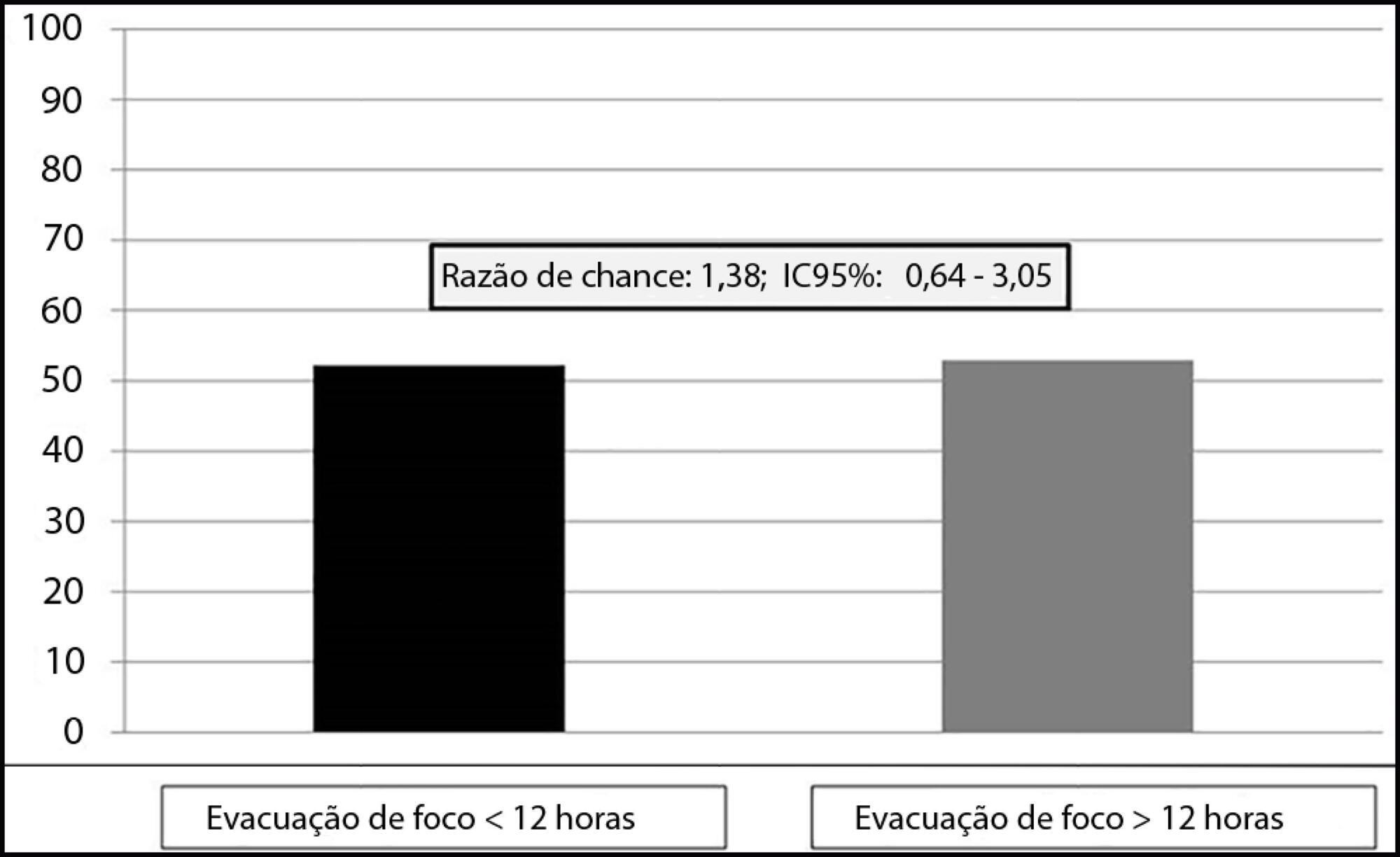
This was an observational, single-center study with a retrospective analysis of the time to clearance of abdominal septic focus. Patients were classified according to the time to focus clearance into an early (≤ 12 hours) or delayed (> 12 hours) group.
A total of 135 patients were evaluated. There was no association between time to focus clearance and hospital mortality (≤ 12 hours versus > 12 hours): 52.3% versus 52.9%, with p = 0.137.
There was no difference in hospital mortality among patients with sepsis or septic shock who had an infectious focus evacuated before or after 12 hours after the diagnosis of sepsis.
Abstract
Rev Bras Ter Intensiva. 2020;32(2):245-250
DOI 10.5935/0103-507X.20200029
To assess the relationship between time to focus clearance and hospital mortality in patients with sepsis and septic shock.
This was an observational, single-center study with a retrospective analysis of the time to clearance of abdominal septic focus. Patients were classified according to the time to focus clearance into an early (≤ 12 hours) or delayed (> 12 hours) group.
A total of 135 patients were evaluated. There was no association between time to focus clearance and hospital mortality (≤ 12 hours versus > 12 hours): 52.3% versus 52.9%, with p = 0.137.
There was no difference in hospital mortality among patients with sepsis or septic shock who had an infectious focus evacuated before or after 12 hours after the diagnosis of sepsis.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (116) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)