Shock, septic/drug therapy Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2019;31(4):586-591
DOI 10.5935/0103-507X.20190068
Among the infections caused by Streptococcus β hemolyticus from the Lancefield serogroup A, toxic shock syndrome is perhaps the most severe, and its mortality rate is high. Its clinical similarity to other forms of shock, especially septic shock, can often confuse the evaluator and interfere with the selection of the most appropriate therapy. This report aims to inform readers of the need to add this syndrome as a differential diagnosis in cases of shock, especially those with no well-defined clinical manifestations. For this purpose, we present the case of an infant with common flu-like symptoms who progressed rapidly with a rash, a reduced level of consciousness and clinical and laboratory signs of shock that required intensive support. In addition to cultures indicating the etiological agent, the appearance of exanthema and necrotizing fasciitis led to the diagnosis. However, less than 50% of cases present classic clinical signs of this entity. Penicillins combined with aminoglycosides are still the therapy of choice and are supported by a high level of evidence. Despite the severity of this patient's presentation, the progression was satisfactory.
Abstract
Rev Bras Ter Intensiva. 2019;31(4):586-591
DOI 10.5935/0103-507X.20190068
Among the infections caused by Streptococcus β hemolyticus from the Lancefield serogroup A, toxic shock syndrome is perhaps the most severe, and its mortality rate is high. Its clinical similarity to other forms of shock, especially septic shock, can often confuse the evaluator and interfere with the selection of the most appropriate therapy. This report aims to inform readers of the need to add this syndrome as a differential diagnosis in cases of shock, especially those with no well-defined clinical manifestations. For this purpose, we present the case of an infant with common flu-like symptoms who progressed rapidly with a rash, a reduced level of consciousness and clinical and laboratory signs of shock that required intensive support. In addition to cultures indicating the etiological agent, the appearance of exanthema and necrotizing fasciitis led to the diagnosis. However, less than 50% of cases present classic clinical signs of this entity. Penicillins combined with aminoglycosides are still the therapy of choice and are supported by a high level of evidence. Despite the severity of this patient's presentation, the progression was satisfactory.

Abstract
Rev Bras Ter Intensiva. 2016;28(3):315-322
DOI 10.5935/0103-507X.20160044
To evaluate the prevalence of antibiotic de-escalation in patients diagnosed with severe sepsis or septic shock at a public academic tertiary hospital and to evaluate antibiotic adequacy and culture positivity.
The prevalence of antibiotic de-escalation, the adequacy of antibiotic treatment and the rates of culture positivity were analyzed in patients with severe sepsis and septic shock between April and December 2013 at an intensive care unit in a tertiary university hospital.
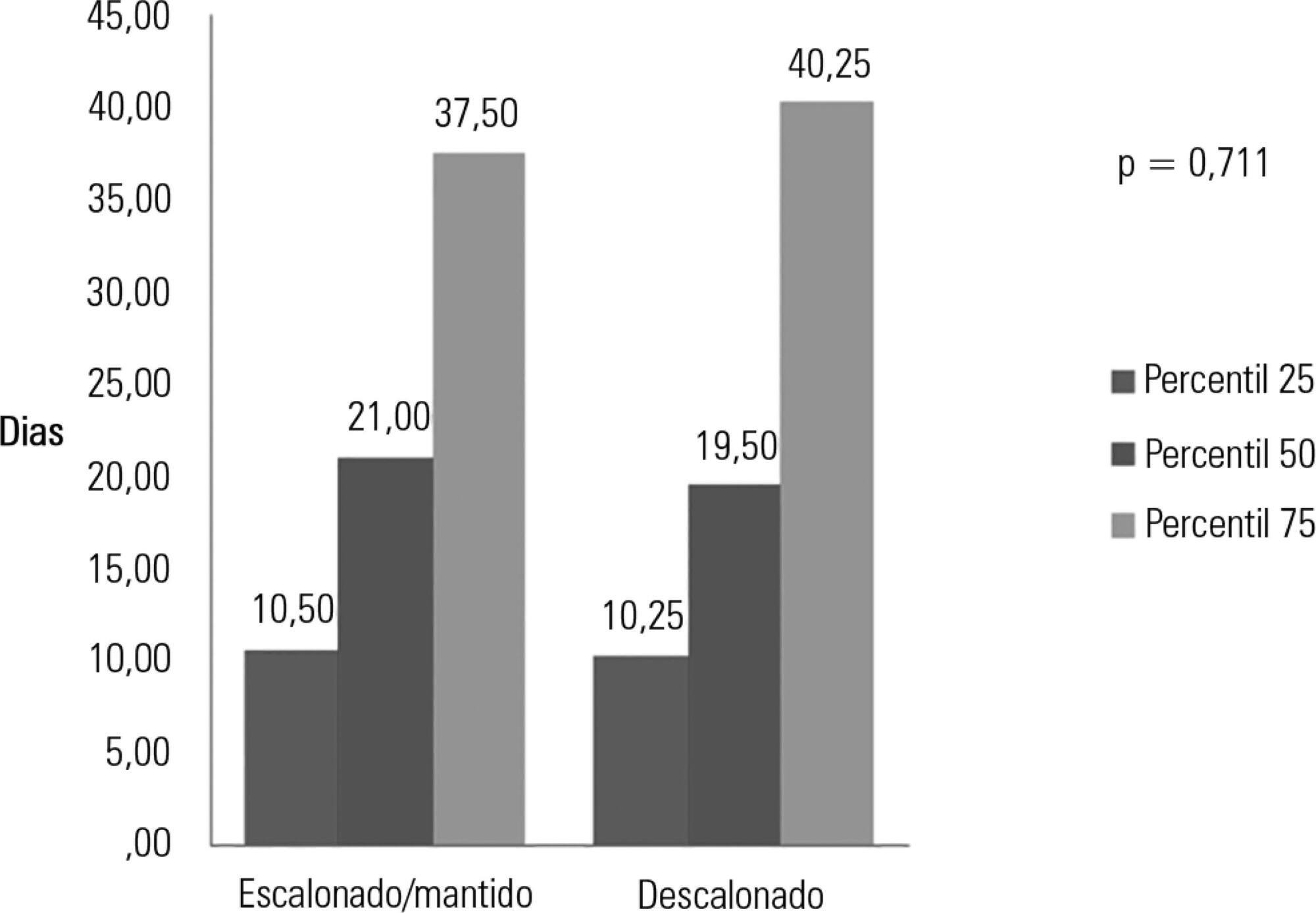
Among the 224 patients included in the study, de-escalation was appropriate in 66 patients (29.4%) but was implemented in 44 patients (19.6%). Among the patients who underwent de-escalation, half experienced narrowing of the antimicrobial spectrum. The mortality rate was 56.3%, with no differences between the patients with or without de-escalation (56.8% versus 56.1%; p = 0.999) nor in the length of hospital stay. Empirical antibiotic therapy was appropriate in 89% of cases. Microorganisms were isolated from total cultures in 30% of cases and from blood cultures in 26.3% of cases.
The adequacy rate of empirical antibiotic therapy was high, reflecting an active institutional policy of monitoring epidemiological profiles and institutional protocols on antimicrobial use. However, antibiotic de-escalation could have been implemented in a greater number of patients. De-escalation did not affect mortality rates.
Abstract
Rev Bras Ter Intensiva. 2016;28(3):315-322
DOI 10.5935/0103-507X.20160044
To evaluate the prevalence of antibiotic de-escalation in patients diagnosed with severe sepsis or septic shock at a public academic tertiary hospital and to evaluate antibiotic adequacy and culture positivity.
The prevalence of antibiotic de-escalation, the adequacy of antibiotic treatment and the rates of culture positivity were analyzed in patients with severe sepsis and septic shock between April and December 2013 at an intensive care unit in a tertiary university hospital.
Among the 224 patients included in the study, de-escalation was appropriate in 66 patients (29.4%) but was implemented in 44 patients (19.6%). Among the patients who underwent de-escalation, half experienced narrowing of the antimicrobial spectrum. The mortality rate was 56.3%, with no differences between the patients with or without de-escalation (56.8% versus 56.1%; p = 0.999) nor in the length of hospital stay. Empirical antibiotic therapy was appropriate in 89% of cases. Microorganisms were isolated from total cultures in 30% of cases and from blood cultures in 26.3% of cases.
The adequacy rate of empirical antibiotic therapy was high, reflecting an active institutional policy of monitoring epidemiological profiles and institutional protocols on antimicrobial use. However, antibiotic de-escalation could have been implemented in a greater number of patients. De-escalation did not affect mortality rates.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (116) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)